Anything new in diabetes care? · 2014-05-09 · antibodies shortly after diagnosis of diabetes....
36
Anything New in Diabetes Care? OAFP Spring CME Weekend April 25, 2014 Josh Reagan MD
Transcript of Anything new in diabetes care? · 2014-05-09 · antibodies shortly after diagnosis of diabetes....

Anything New in Diabetes Care?
OAFP Spring CME Weekend
April 25, 2014
Josh Reagan MD
Objectives
• Review 2014 changes to ADA guidelines • Review blood pressure and cholesterol goals for
patients with diabetes • Discuss “newish” medications for diabetes
management • Discuss role of bariatric surgery in diabetes care • Review new technology for diabetes
management • Where the rubber hits the road: any changes in
billing for diabetes with ICD 10 and PCMH?

ADA Revisions to the 2014 Clinical Practice Recommendations 1:
• Acceptance of both 1- or 2-step testing for GDM; using either 1-step fasting 75 mg oral gtt or original 2-step 50 gm glucose 1 hr GTT followed by 100 gm 3 hr GTT, if needed.
• Simplification of Nephropathy terminology: microalbuminuria renamed albuminuria 30-299 mg/24 hr and macroalbuminuria renamed albuminuria > 300 mg/24h.
• For painful diabetic neuropathy, treatment options of duloxetine and pregabalin added to prior treatment options venlafaxine, amitriptyline, gabapentin, valproate, opioids.
• Liberalization of blood glucose monitoring recommendations, with intent of easing acquisition of multiple cbg strips per day from insurance companies.
ADA Revisions to the 2014 Clinical Practice Recommendations 2:
• Shorten course of non-insulin monotherapy from 3-6 month trial to 3 month trial.
• New standards for thyroid and celiac disease screening in type 1 diabetes. Recommendation to screen with celiac antibodies shortly after diagnosis of diabetes. For thyroid screening, plan TSH testing shortly after metabolic control is obtained, and then every 1-2 years.
• Discourage use of sliding scale alone for management alone of hyperglycemia in hospital. Preference is for use of basal-bolus insulin with correction dose insulin for vast majority of patients.
• NO CHANGES TO GUIDELINES REGARDING TREATMENT OF CHOLESTEROL OR HYPERTENSION.
New blood pressure guidelines?
• In 2013, ADA reduced goals for blood pressure for patients with DM to 140/80 (from 130 systolic), although they acknowledged lower goals may be appropriate in younger pts with DM.
• Meanwhile, the JNC 8, the American Society of Hypertension and the International Society of Hypertension (ASH/ISH) released new guidelines in December 2013 that suggested that the BP target for patients with DM should be < 140/90, rather than <140/80.
• RCTs demonstrate reduced mortality and improved cardiovascular and cerebrovascular outcomes with treatment goal SBP <150 mm Hg, less so with SBP < 140. More intensively managed DM w/ HTN have minor decrease in CVA, but no change in mortality. There may be fewer microvascular complications. But there are more med-related adverse events and an increase in creatinine to over 1.5.
New Cholesterol Guidelines?
• Current treatment guidelines are to aim for LDL < 100 on all patients w/ DM and <70 if established CVD.
• New recommendations put out by AHA/ACC are to just start a mid potency statin on every diabetic aged 40-75 years. If a diabetic in this age range falls in ASCVD category >7.5%, they recommend high intensity statin therapy.
• Moderate intensity statin refers to atorvastatin 10 mg, rosuvastatin 5-10 mg, simvastatin 20-40 mg, pravastatin 40 mg, lovastatin 40 mg, fluvastatin 40 mg.
• High intensity refers to atorvastatin 40-80 mg and rosuvastatin 20-40 mg.
• A cost & convenience advantage of this scenario would be less frequent lipid checks.
Newish Drugs
But first, a review of the old… METFORMIN
• Metformin is the first drug to offer to patients with diabetes.
• Black box for heart failure was removed, it actually reduces mortality in heart failure by 31%.
• It also reduces likelihood of MI.
• It may help with weight loss, or at least avoidance of weight gain in patients taking insulin.
• We still don’t really understand how it works.
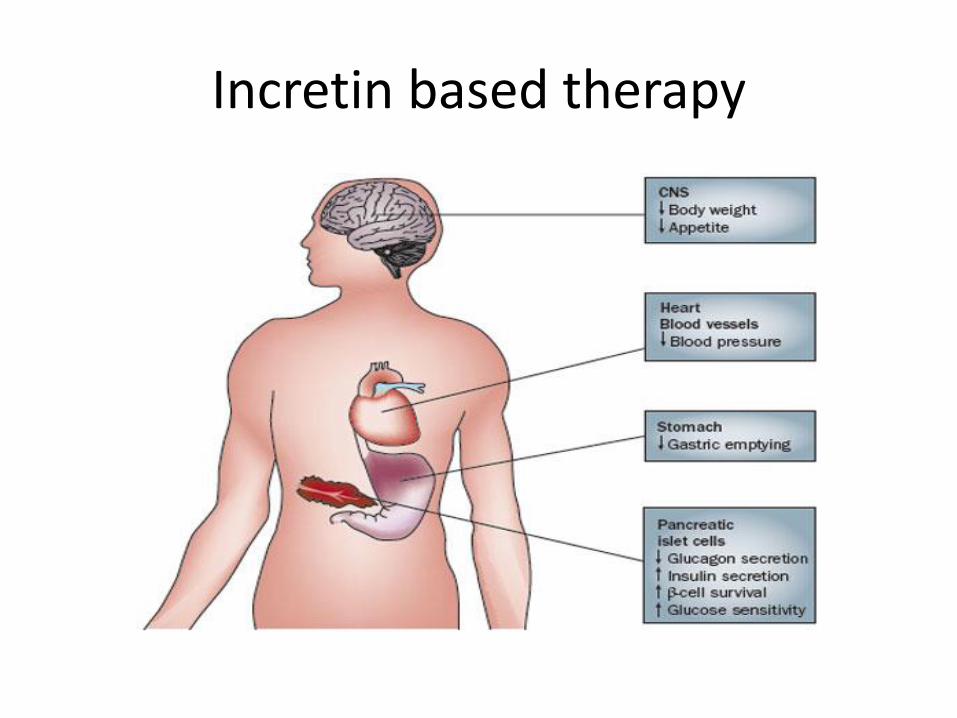
Incretin based therapy
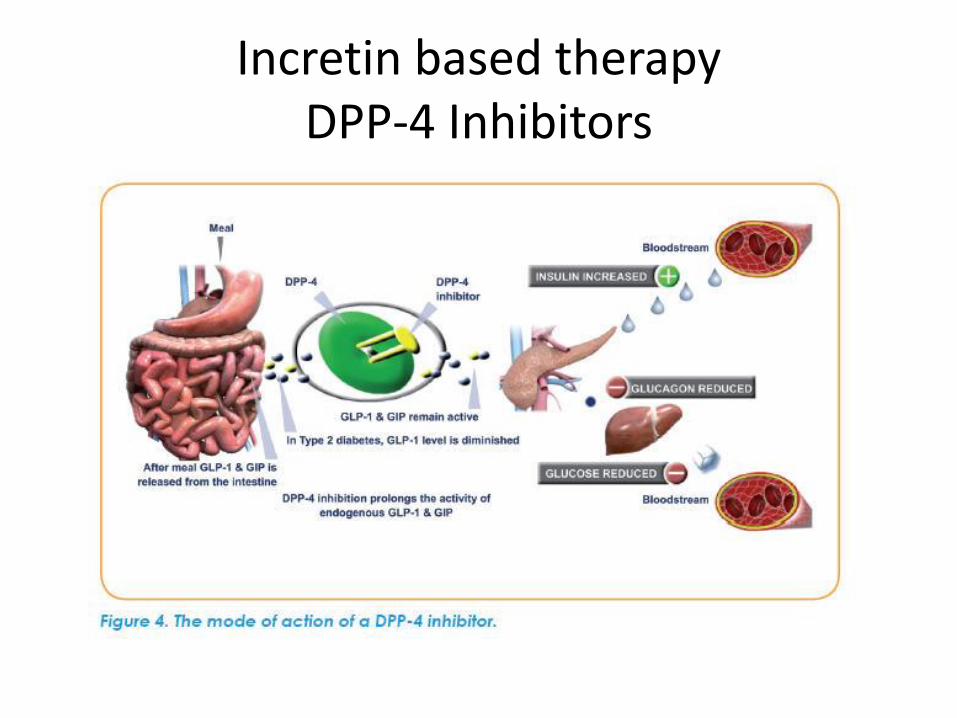
Incretin based therapy DPP-4 Inhibitors

DPP-4 Inhibitors 1
• Inhibit an adenosine-deaminase binding protein that is quite widespread in the body.
• Function by increasing endogenous GLP-1 levels. • Examples available in the United States include sitagliptin,
saxagliptin, linagliptin and alogliptin. • Functions as a weak insulin secretagogue. Less of an effect
on gastric emptying. • Tend to drop A1c by 0.4 to 0.8 percent. Has a greater effect
on postprandial glucose levels. • Tend to be weight neutral. • Excreted renally, thus dosage adjustment needed in CKD.
DPP-4 Inhibitors 2
• Do not appear to have any cardiovascular outcomes, positive or negative, in current short term trials.
• Other side effects:
• A) Rare GI side effects.
• B) Increase in nasopharyngitis symptoms (RR 1.2).
• C) Increase in UTI symptoms (RR 1.5).
• D) Increase in HA (RR 1.4).
• Rare skin hypersensitivity and elevated transaminases.
• No increase in pancreatitis.
• $$$
The Story of Gila Monster Spit
• Discovered by John Eng in the early 1990s, from desiccated Gila Monster (Heloderma suspectum) saliva.
• Drawn to the Gila Monster because he was aware that its venom caused swelling of pancreas. The Gila Monster can also go for extended periods of time by slowing down its own metabolism and maintaining a constant glucose level during an extended fast.
• Developed a chemical assay to ferret out new hormones in animals. Stumbled upon a hormone in the venom of the Mexican beaded lizard that was vasoactive. But in the Gila Monster venom he found a compound he called Exendin-4 that was similar to GLP-1 (glucagon like peptide) which had recently been discovered to regulate glucose and satiety.
• The advantage over GLP-1 was that it lasted 12 hours, while GLP-1 was quite short-lived.
GLP-1 Agonists 1
• Mechanism: Appear to stimulate insulin secretion (even in people who already failed oral medications). May inhibit glucagon secretion. Do not change insulin resistance. Inhibits food intake and slows gastric emptying. Primarily, actions seem mediated by effects on weight, insulin, glucagon and possibly oral intake.
• Benefits: Lower postprandial glucose levels. Reduce weight by about 2.5 to 4 kg (compared to trial looking at glargine therapy, which raised weight by 1.4 kg).
• Efficacy: • A) Short acting GLP 1 agonists ie twice-daily exenatide, appear to
drop a1c by about 0.8%. • B) Long acting GLP 1 agonists ie once-weekly exenatide, daily
liraglutide, may drop a1c by almost 1.1 to 1.4%.
GLP-1 Agonists 2
• Frequent side effects: nausea, vomiting, diarrhea (10-40%), injection site pruritus. Nausea often declines with time.
• Discontinuation rates vary from 5-10% in studies. Primarily due to nausea. • Safety? • There is a question of pancreatitis and pancreatic cancer, however data at
this time unconvincing. Diabetics at baseline higher risk of pancreatitis (two-fold). The study that looked at pancreatitis did not compare diabetes severity, obesity, or use of other diabetes medications.
• There may be slight increase in hospitalization for heart failure. • There are no comparative trials looking at long term outcomes such as
diabetic complications. • There is also a link between liraglutide and thyroid C-cell tumors in lab
mice and rats, currently relevance to humans is unknown. Should counsel on possible increased risk of medullary thyroid cancer.
• Bottom line: We don’t have years of experience with it yet. • $$$$
SGLT-2 Inhibitors 1
• Newest class of drugs for diabetes, aimed at a novel target.
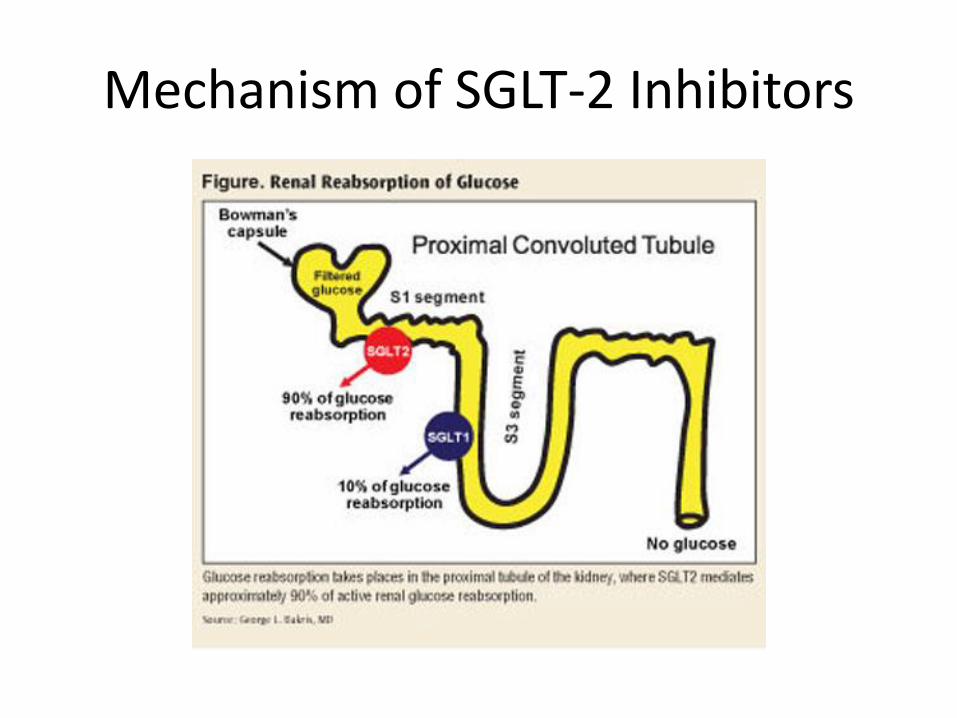
• Mechanism: SGLT2 is a channel in the proximal convoluted tubules that reabsorb approximately 160 gm of glucose per day. The SGLT2co-transports sodium and glucose into proximal convoluted tubule cells. It is inhibited by the SGLT2 inhibitors: canagliflozin and dapagliflozin.
• Causes excretion of 80-100 gm glucose per day.
Mechanism of SGLT-2 Inhibitors
SGLT-2 Inhibitors 2
• Efficacy: Reduces a1c by about 0.5% to 1% (for 100 mg and 300 mg canagliflozin). However a subset of more newly diagnosed diabetics dropped A1c by 2 to 2.5%.
• It has a greater effect on postprandial glucose levels. • Associated with weight loss: at about 26 weeks patients
typically exhibit an average loss of 2.5% body weight. Corresponds to average of 2-3 kg loss.
• Reduction of BP: 1.3 to 7.3 mm Hg. • No hypoglycemia. • Studied in combination with metformin, insulin and
sulfonylureas. • No data on CV or microvascular outcomes.
SGLT-2 Inhibitors 3
• Appears well tolerated, in studies discontinuation rates were higher with glimepiride.
• Safety? • Increases in female genital mycotic infections (10-15% compared to
3%), UTI, hypotension, renal insufficiency, hyperkalemia. No increase in severe UTI, hospitalization for dehydration. Increase in LDL also noted. Uncircumcised men also at greater risk of mycotic infection (5% v 1%). Increase in urination was noted in 5% of patients (compared to 0.8%).
• Dapagliflozin has been associated with an increase in bladder cancer.
• NO canagliflozin if GFR < 45 (and only 100 mg dose if GFR 45-60). Limit dapagliflozin to GFR > 60.
• May need to reduce dose of insulin or sulfonylurea to reduce hypoglycemia.
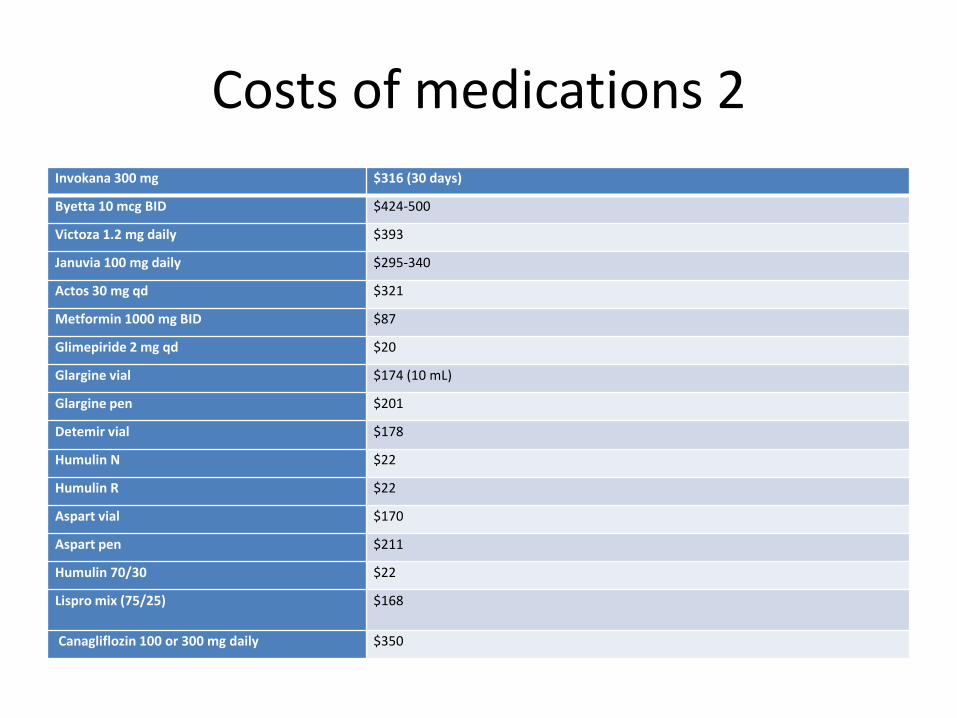
Costs of medications 2
Invokana 300 mg $316 (30 days)
Byetta 10 mcg BID $424-500
Victoza 1.2 mg daily $393
Januvia 100 mg daily $295-340
Actos 30 mg qd $321
Metformin 1000 mg BID $87
Glimepiride 2 mg qd $20
Glargine vial $174 (10 mL)
Glargine pen $201
Detemir vial $178
Humulin N $22
Humulin R $22
Aspart vial $170
Aspart pen $211
Humulin 70/30 $22
Lispro mix (75/25) $168
Canagliflozin 100 or 300 mg daily $350
Bariatric Surgery for Diabetes
• 3 main types:
• 1. Restrictive: can’t ingest the same number of calories. Examples: vertical sleeve gastrectomy, gastric banding
• 2. Malabsorptive: disable intestines to worsen absorption. Examples: Biliopancreatic diversion with duodenal switch (not done much)
• 3. Restrictive and Malabsorptive. Example:Roux-en-Y Gastric Bypass. 91% of these are now performed by laparoscopy.
Bariatric Surgery vs Medical Management

Gastric Banding
• Safe, mortality 1/1200 • Simple operation • Tremendous range of
weight loss, but there is often a failure to lose significant weight; or dramatic weight gain after initial loss (soda/ice cream can slide right by band!).
• Occasionally esophageal dilatation occurs.
Vertical Sleeve Gastrectomy
• New kid on the block.
• No long term data yet. No experience over 5 years.
• Weight loss appears to be 50-60% over first 3-5 years.
• Risks: leak (2%), bleeding (2%), stricture (0.6%), death (0.19%).
• 37% of patients achieved A1c of 6%.

Roux-en-Y Gastric Bypass
Gastric Bypass
• Gold standard
• Creates small divided gastric pouch.
• Wt loss at 1 year averages 112 lbs.
• Results fairly consistent.
• Complications: 0.28% mortality, leak 0.5-0.2%, bleeding 0.5%, PE 0.5%, Stricture 3-7%, macro and micro nutrient deficiencies 15%, EWL 70-80% at 10 years, durable.
• Often curative of diabetes. 42% of patients achieved A1c of 6%, in individuals who began at 9% A1c.
Other issues around surgery
• Estimated that cost of surgery is recouped in 2-3 years of medical treatment. Cost around $25,000-30,000.
• Tailor to the correct patient. Avoid malabsorptive surgery in patients with malabsorption or nutrient deficiency.
• Not appropriate in people with uncontrolled mental illness or poor self control.
• For gastric bypass request extensive dietary change prior to surgery with goal of shrinking liver.
• Blood sugar improvement occurs much more rapidly than the weight loss.
• Often leads to reduction in hypertension.
Unstudied Bariatric Surgery Techniques
• There are many “rogue” procedures that are being performed in a variety of locations, most of these have been inadequately studied.
New Technologies
• Continuous glucose monitors
• Pump/CGM combinations with low glucose suspend function
• Smart phone/glucometer
• Diabetes apps
• Ultra long lasting insulin (degludec)
• Inhaled insulin- second attempt
• Implantible PAQ insulin pump

CGM 1
• Measure glucose content of interstitial fluid using electrochemical enzymatic sensor.
• Sensor inserted subcutaneously, for 6-7 days (officially). • Reduce a1c in type 1 DM by about 0.3%. • Largest benefit with hypoglycemia unawareness: reduces
frequency and enables earlier detection. • In DM2, has also been shown to drop a1c by about 0.7%. • Useful in motivated patients. Initial studies on children w/DM1
demonstrated no benefit, however when study populations were broken down into those who used it and those who didn’t, it was effective at lowering a1c in device users.
• Fairly accurate, within 20% cbg about 75% of the time. Need to be calibrated, usually twice daily. Accuracy worse when hypoglycemic.
• Combine with pump, with automated shut-off for hypoglycemia.
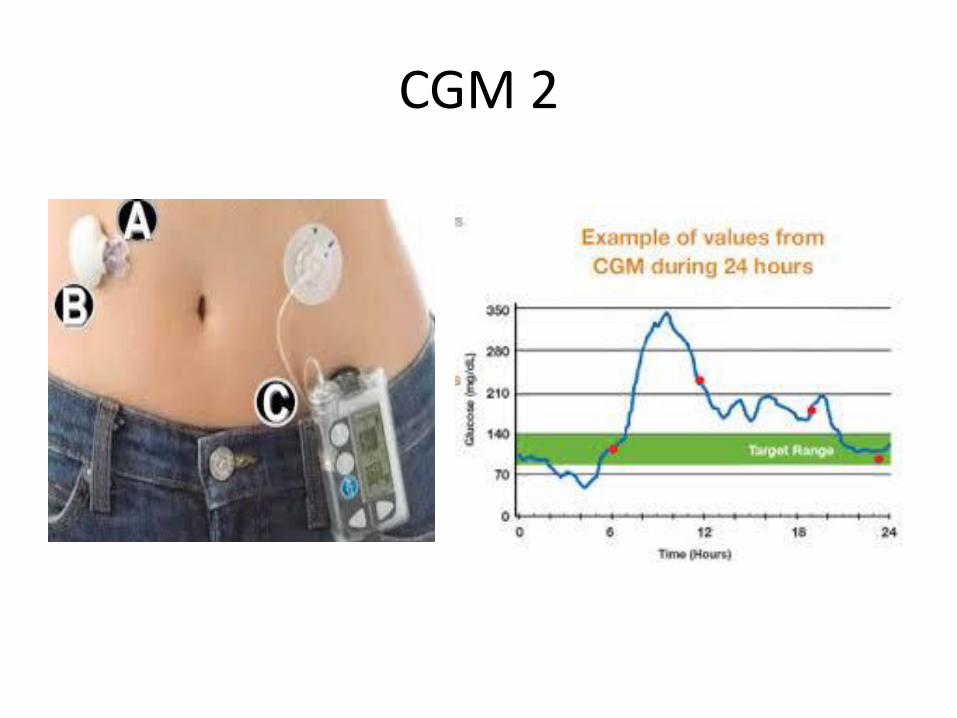
CGM 2
Ultra long acting insulin- degludec
Lifestyle Apps
• Calculate BMI • Give 7 minute exercise
routines • Provide calorie content of
foods • Calculator to inform you of
necessary calorie intake/expenditure to lose weight
• App that tracks when you go to gym, allows you to make or lose money based on gym attendance

Improving Reimbursement for Providing Diabetes Care
• Two main categories of achieving this goal:
• A) Improve Patient Centered Medical Home status to tier 2 or 3 and receive age-adjusted per-member per-month incentives.
• B) Assign patients with appropriate ICD codes to reflect complexity of care, which will be translated to reimbursement.

Bibliography 1
• Diabetes Care January 2014 37:Supplement 1 S14-S80; doi:10.2337/dc14-S014
• Diabetes Care January 2013 36:Supplement 1 S11-S66; doi:10.2337/dc13-S011
• James PA et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA Dec 18; [e-pub ahead of print]. (http://dx.doi.org/10.1001/jama.2013.284427)
• The ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010 Mar 14; [e-pub ahead of print]. (http://dx.doi.org/10.1056/NEJMoa1001286)
• http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437738.63853.7a.citation
Bibliography 2
• Dalla Man C, et al. Diabetes Care January 2009 vol. 32 no. 1 14-18.
• De Fronzo RA, et al. Diabetes Care. 2005:28 (5): 1092-1100. • Scirica, BM, et al. N Engl J Med 2013; 369:1317-1326. • Singh, S et al. JAMA Intern Med. 2013;173(7):534-539. • Stenlof, K et al. Diabetes Obes Metab. 2013 Apr;15(4):372-
82. • Vasilakou, D, et al. Ann Intern Med. 2013;159(4):262-274. • Schauer, PR, et al. Bariatric Surgery versus Intensive
Medical Therapy in Obese Patients with Diabetes. N Engl J Med 2012; 366:1567-1576.