ANXIETY - Universitas Padjadjaranblogs.unpad.ac.id/tatyhernawaty/files/2010/12/ANXIETY1.pdf ·...
34
ANXIETY Taty Hernawaty, S.K.p., M.Kep Bagian Keperawatan Klinik http://blogs.unpad.ac.id/tatyhernawaty email: [email protected]
Transcript of ANXIETY - Universitas Padjadjaranblogs.unpad.ac.id/tatyhernawaty/files/2010/12/ANXIETY1.pdf ·...

ANXIETY
Taty Hernawaty, S.K.p., M.Kep
Bagian Keperawatan Klinik
http://blogs.unpad.ac.id/tatyhernawaty
email: [email protected]
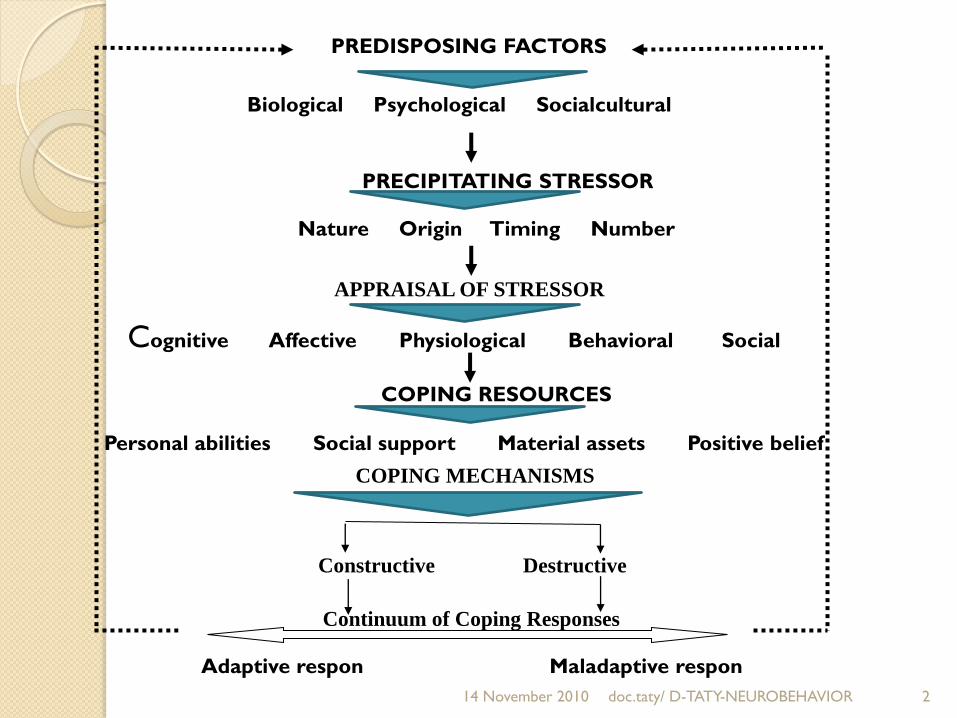
PREDISPOSING FACTORS
Biological Psychological Socialcultural
PRECIPITATING STRESSOR
Nature Origin Timing Number
APPRAISAL OF STRESSOR
Cognitive Affective Physiological Behavioral Social
COPING RESOURCES
Personal abilities Social support Material assets Positive belief
COPING MECHANISMS
Constructive Destructive
Continuum of Coping Responses
Adaptive respon Maladaptive respon
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 2

14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 3
Respon
Respon
Respon
Soc
Bio
Psycho
Psycho
Bio
Soc
Psycho
Bio
SocSoc-Cul
PsychoBio

Definition
Taylor (1953) : Suatu perasaan subyektif
mengenai ketegangan mental yang
menggelisahkan sbg reaksi umum dari
ketidakmampuan mengatasi suatu masalah
atau tidak adanya rasa aman.
Stuart and Sundeen (1998) is an emotion
and a subjective experience.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 4

Predisposing Factors
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 5
Anxiety is a prime factor in the
development of the personality and
formation of individual character traits
PhychoanaliticView
• Freud believed that unexpressed sexual energy was
converted into anxiety therefore alleviation of
anxiety merely required improved sexual technique.

Predisposing…
Interpersonal View
Sullivan believed that…
Anxiety could not arise until the organism had some
awareness of its environment.
Originated in the early bond between the infant and
mother through this close emotional bond,
anxiety is first conveyed by the mother to the infant.
The anxiety in later life arises when a person
perceives that he/she will be viewed unfavorably or
will lose the love of a person he/she values.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 6

Predisposing…
Behavioral View
Anxiety is a product frustation caused by anything
that interferes with attaining a desire goal, ex: the
loss of a job (external frustation), the young college
graduates who set unrealistically goal (internal
frustation)
Anxiety as a drive that is learned because of an
innate desire to avoid pain.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 7
Predisposing…
Biological Basis
The anxiety is helped by benzodiazepines, the spesific
receptors in the brain.
This is related to the activity of the neurotransmitter
gammaaminobutyric acid (GABA).
the antianxiety class of drugs is reduced firing rate
of cells in areas implicated in anxiety disorders, the
clinical result is that the person becomes less
anxious.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 8

Precipitating Factors
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 9
Clearly, experiencing or wtnessing a
source of trauma of any kind has been
associated with a variety of anxiety
disorders, particularly PTSD
Threats to Physical Integrity
• Internal sources may include the failure of
physiological mechanism such as the heart, immune
system, or temperature regulation.

Precipitating…
External sources may include exposure to viral
and bacterial infection, enviromental pollutants, safety
hazards, lack of adequate housing, food, or clothing,
and traumatic injury.
Threats to self-system
Internal sources may include interpersonal
difficulties at home or at work or assuming a new
role, such as parent, student, or employee.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 10

Precipitating…
External sources may include the loss of a valued
person through death, divorce, or relocation, a
change in job status, an ethical dillema, and social or
cultural group pressure.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 11

Coping Mechanisms
Task-Oriented Reactions
In attack behavior : a person attempts to remove or overcome obstacles to satisfy a need.
Withdrawl behavior : involves removing oneself from source of the threat. Biological such as smoke-filled rooms, exposure to irradiation, or contact with contagious diseases. Phychologicalsuch as by admitting defeat, becoming apathetic, or lowering aspirations.
Compromise : is necessary in situations that cannot be resolved through attack or withdrawl.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 12

Coping…
Ego-Oriented Reactions
Not always successful in coping with
stressful situations (mild and moderate
level)
Also called ego defence mechanisms,
are the first line of psychic defence.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 13

Ego…
Compensation : process by which a person makes up for a perceived deficiency by strongly emphasizing a feature that he/she regards as an asset.
Denial : avoidance of disagreeable realities by ignoring or refusing to recognize them; the simplest and most primitive of all defense mechanisms.
Displacement : shift of emotion from a person or object to another, usually neutral or less dangerous or object.
Dissociation : the separation of group of mental or behavioral processes from the rest of the person’s consciousness or identity.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 14

Ego …
Identification : process by which a person tries to
become like someone he/she admires by taking on
thoughts, mannerisms, or tastes of that person.
Intellectualization : excessive reasioning or logic is
used to avoid experiencing disturbing feelings.
Introjection : intense identification in which a person
incorporates qualities or values of another person or
group into his/he own ego structure. It is one of the
earliest mechanisms of the child, important in
formation of conscience.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 15

Ego …
Isolation : splitting off of emotional components of a
thought, which may be temporary or long term.
Projection : attributing one’s thoughts or impulses to
another person. Through this process one can
attribute intolerable wishes, emotional feelings, or
motivations to another person.
Rationalization : offering a socially acceptable or
apparently logical explanation to justify or make
acceptable otherwise unacceptable impulses, feelings,
behaviors, and motives.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 16

Ego …
Reaction formation : development of conscious
attitudes and behavior patterns that are opposite
to what one really feels or would like to do.
Reggresion : retreat to behavior characteristic of
an earlier level of development.
Repression : involuntary exclusion of a painful or
conflictual thought, impulse, or memory from
awareness. It is the primary ego defence, and
other mechanisms tend to reinforce it.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 17
Ego …
Splitting : viewing people and situations as either all good or all bad. Failure to integrate the positive and negative qualities of oneself.
Sublimation : acceptance od a socially approved substitute goal for a drive whose normal channel of expression is blocked.
Suppression : a process often listed as a defencemechanism buat really a conscious counterpart of repression. It is intentional exclusion of material from consciousness. At time, it may lead to repression.
Undoing : act or communication that partially negates a previous one; a primitive defence mechanisms.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 18

Levels of Anxiety
Peplau identified four levels :
Mild anxiety
Associated with the tension of day-to-day living
alert
Perceptual field is increased
The person sees, hears, and graps more than before
Can motivate learning
Produce growth and creativity
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 19
Levels …
Moderate anxiety
The person focuses only on immediate concerns
Involves the narrowing of the perceptual field
The person sees, hears, and graps less
The person blocks out selected areas but can attend
to more if directed to do so
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 20

Levels …
Severe anxiety
Marked by a significant reduction in perceptual field
The person tends to focus on a specific detail and
not think about anything else
All behavior is aimed at relieving anxiety
Much direction needed to focus on another area
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 21

Levels …
Panic
Associated with awe, dread, and teror
Blown out of proportion
Unable to do things even with direction
Involves the disorganization of personalitry
A person can no longer function as an organized human being
Motor activity is increased
Decreased ability to relate to others
Distorted perceptions
Loss of rational thought
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 22
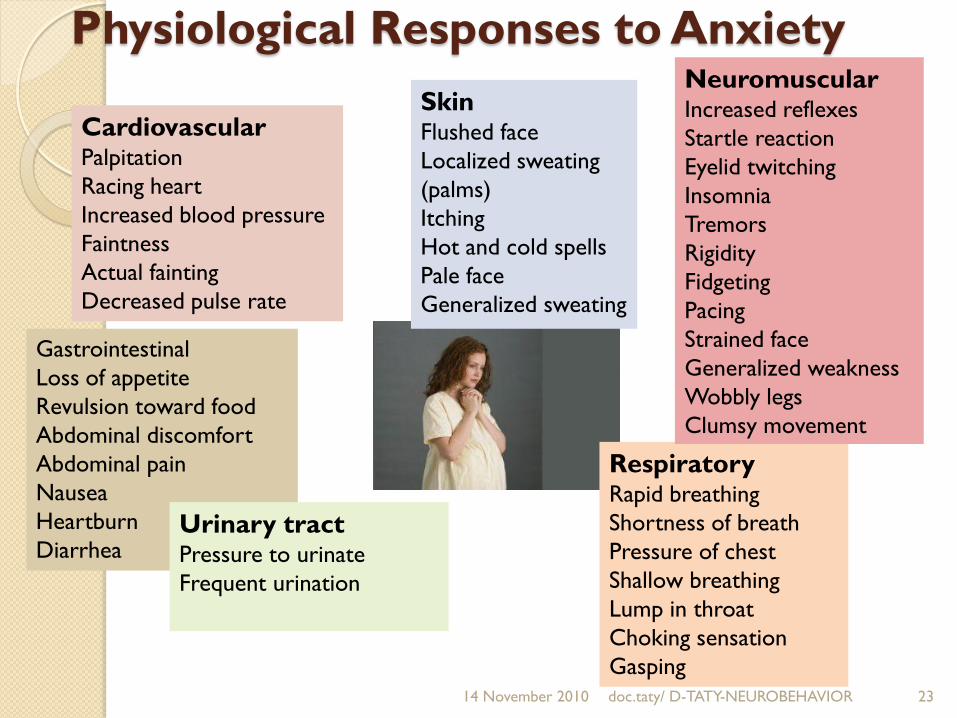
Physiological Responses to Anxiety
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 23
CardiovascularPalpitation
Racing heart
Increased blood pressure
Faintness
Actual fainting
Decreased pulse rate
RespiratoryRapid breathing
Shortness of breath
Pressure of chest
Shallow breathing
Lump in throat
Choking sensation
Gasping
Gastrointestinal
Loss of appetite
Revulsion toward food
Abdominal discomfort
Abdominal pain
Nausea
Heartburn
Diarrhea
NeuromuscularIncreased reflexes
Startle reaction
Eyelid twitching
Insomnia
Tremors
Rigidity
Fidgeting
Pacing
Strained face
Generalized weakness
Wobbly legs
Clumsy movement
Urinary tractPressure to urinate
Frequent urination
SkinFlushed face
Localized sweating
(palms)
Itching
Hot and cold spells
Pale face
Generalized sweating

The Responses…
BEHAVIORAL
Restlessness
Physical tension
Tremors
Startle reaction
Hypervigilance
Rapid speech
Lack of coordination
Accident proneness
Interpersonal withdrawl
Inhibition
Flight
Avoidance
Hyperventilation
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 24
COGNITIVE
Impaired attention
Poor concentration
Forgetfulness
Errors in judgment
Preoccupation
Blocking of thoughts
Decreased perceptual field
Reduced creativity
Diminished productivity
Confusion
Self-consciousness
Loss of objectivity
Fear of losing control
Frightening visual images
Fear of injury or death
Flashbacks
Nightmares
AFFECTIVEEdginess
Impatience
Uneasiness
Tension
Nervousness
Fear
Fright
Alarm
Terror
Jitteriness
Jumpiness
Numbing
Guilt
Shame

InterventionExpected outcome: the patient will demonstrate
adaptive ways of coping with stress
Short-term goal:
The patient will identify and describe feelings of
anxiety
The patient will identify antecedents of anxiety
The patient will describe adaptive and maladaptive
coping responses
The patient will implement two adaptive responses for
coping with anxiety
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 25

Intervention… Help the patient identify and describe underlying
feelings
Link the patient’s behavior with such feelings
Validate all inferences and assumptions with the
patient
Use open questions to move from nonthreatening
topics to issues of conflict.
Vary the amount of anxiety to enhance the patient’s
motivation.
In time, supportive confrontation may be used
judiciously.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 26

Intervention… Help the patient describe the situations and
interactions that immediately precede anxiety.
Review the patient’s appraisal of the stressor, values
being threatened, and the way in which the conflict
developed.
Relate the patient’s present experiences with
relevant ones from the past.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 27

Intervention… Explored how the patient reduced anxiety in the
past and what kinds of actions produced relief.
Point out the maladapative and destructive effects
of present coping responses.
Encourage the patient to use adaptive coping
responses that were effective in the past.
Focus responsibility for change on the patient.
Actively help the patient correlate cause-and –effect
relationships while maintaining anxiety within
appropriate limits.
Help the patient reappraise the value, nature, and
meaning of the stressor when appropriate.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 28

Intervention… Help the patient identify ways to restructure
thoughts, modify behavior, use resources, and test
new coping responses.
Encourage physical activity to discharge energy.
Include significant others as resources and social
supports in helping the patients learn new coping
responses.
Teach the patient relaxation exercises to increase
control and self-reliance and reduce stress.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 29

For severe/panic level of anxietyExpected outcome : the patient will reduce anxiety to a
moderate or mild level.
Short-term goals :
- The patient will be protected from harm
- The patient will experience fewer anxiety provoking
situations.
- The patient will engage in a daily schedule of
activities.
- The patient will experience relief from the
symptoms of severe anxiety.
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 30

Antianxiety drugs
Benzodiazepines
Alprazolam (Xanax)
Chlordiazepoxide
(Librium)
Clorazepate (Tranxene)
Clonazepam (Klonopin)
Diazepam (Valium)
Halazepam (Paxipam)
Lorazepam (Ativan)
Oxazepam (Serax)
Prazepam (Centrax)14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 31
Antihistamines
Diphenhydramine (Benadryl)
Hydroxyzine (Atarax)
Beta-adrenergic Blocker
Propanolol (Inderal)
Antidepressant
Anxiolytic
Buspirone (BuSpar)

Antidepresant drugs
14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 32
Clomipramine (Anafranil)
Fluoxetine (Prozac)
Setraline (Zoloft)
Paroxetine (Paxil)
Fluvoxamine (Luvox)
Venlafaxine (Effexor)
Nefazodone (Serzone)
Phenelzine (Nardil)
The scales for anxiety Beck Anxiety Inventory (BAI)
Covi Anxiety Scale
Dissociative Experience Scale
Dissociative Disorders Interview Schedule (DDIS)
Hamilton Rating Scale for Anxiety (Ham-A)
Maudsley Obsessional Compulsive Inventory
Panic Disorder Outcomes Module (PDOM)
Spielberger Anxiety State-Trait
Taylor Anxiety Scale
Yale-Brown Obsessive Compulsive Scale (YBOCS)
Zung Anxiety Scale14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 33

14 November 2010 doc.taty/ D-TATY-NEUROBEHAVIOR 34