ANTRAL GASTRITIS AND SPASM:
8
ANTRAL GASTRITIS AND SPASM: THEIR CLINICAL AND SURGICAL SIGNIFICANCE JAMES W. R. RENNIE, F.R.C.S. (ED.) WINNIPEG, MAN. DURING THE PAST TEN YEARS on the North American continent with the use of the "spot-film device" for the study of the mucosal patterns of the stomach by radiography, and with the extended use of the flexible gastroscope, due to the efforts of Schindler, the diagnosis of gastritis has become a problem to the radiologist and the surgeon especially in those cases where there is ulceration or hypertrophic processes which may simulate neoplasm of the stomach. Apart from a type of hypertrophic gastritis which produces giant rugae on the greater curvature of the stomach, and which may be mistaken for a neoplastic defect,3' the most difficulty to the surgeon from a clinical and surgical point of view is caused by the variety labelled "antral gastritis"5 or "hypertrophic antrum gastritis."' Although spasm or inflammation may involve any part of the stomach, they are more commonly observed in the antrum. As this part of the stomach is a common site of carcinoma, antral gastritis and spasm are of particular importance to the surgeon because of the difficulties that arise in differential diagnosis. The internist on the other hand is mainly interested in those cases which fit mainly into the classification of gastritis developed by Schindler who differentiates: (i) Superficial gastritis; (2) atrophic gastritis; (3) hypertrophic gastritis; and (4) gastritis of the postoperative stomach. This classification does not greatly assist the radiologist who is able usually to distinguish only the hypertrophic type, and referring as it does to the mucosal lesions as seen by the gastroscopist it does not distin- guish the variety of inflammatory lesions that are seen in the antrum. There is also serious doubt that the first type, superficial gastritis, is always clearlv dis- tinguishable, as the reddening and congestion described in this type are known to occur normally during periods of emotion such as anger. Nevertheless, it is generally agreed that the gastroscopist, particularly in the body of the stomach, can more easily and with more certainty make a diagnosis of gas- tritis than the radiologist. Because it is the radiologist who, after perhaps a test meal, makes the initial examination of the stomach of a patient with gastric complaints, a great deal of responsibility devolves on him to correctly assess the amount of spasm in the antrum or any disturbance of antral systole5 which he may see during the fluoroscopic examination, because it is his judgment of this spasm which deter- mines largely the diagnosis of antral spasm. If the spasm is marked or per- sistent then the radiographs may show this persistent spasm in serial films as an elongation and narrowing of the antrum, giving a picture that is very similar to that of some cases of antral gastritis. Also during fluoroscopic examination, and assisted by radiographic studies of the imucosal pattern of the antrum, he Imutist estimate any rigidity or abnormality of the normal mucosal folds before 402
-
Upload
nguyentuong -
Category
Documents
-
view
238 -
download
0
Transcript of ANTRAL GASTRITIS AND SPASM:

ANTRAL GASTRITIS AND SPASM:THEIR CLINICAL AND SURGICAL SIGNIFICANCE
JAMES W. R. RENNIE, F.R.C.S. (ED.)WINNIPEG, MAN.
DURING THE PAST TEN YEARS on the North American continent with theuse of the "spot-film device" for the study of the mucosal patterns of thestomach by radiography, and with the extended use of the flexible gastroscope,due to the efforts of Schindler, the diagnosis of gastritis has become a problemto the radiologist and the surgeon especially in those cases where there isulceration or hypertrophic processes which may simulate neoplasm of thestomach. Apart from a type of hypertrophic gastritis which produces giantrugae on the greater curvature of the stomach, and which may be mistaken fora neoplastic defect,3' the most difficulty to the surgeon from a clinical andsurgical point of view is caused by the variety labelled "antral gastritis"5 or"hypertrophic antrum gastritis."' Although spasm or inflammation mayinvolve any part of the stomach, they are more commonly observed in theantrum. As this part of the stomach is a common site of carcinoma, antralgastritis and spasm are of particular importance to the surgeon because ofthe difficulties that arise in differential diagnosis. The internist on the otherhand is mainly interested in those cases which fit mainly into the classificationof gastritis developed by Schindler who differentiates: (i) Superficial gastritis;(2) atrophic gastritis; (3) hypertrophic gastritis; and (4) gastritis of thepostoperative stomach. This classification does not greatly assist the radiologistwho is able usually to distinguish only the hypertrophic type, and referring asit does to the mucosal lesions as seen by the gastroscopist it does not distin-guish the variety of inflammatory lesions that are seen in the antrum. There isalso serious doubt that the first type, superficial gastritis, is always clearlv dis-tinguishable, as the reddening and congestion described in this type are knownto occur normally during periods of emotion such as anger. Nevertheless, it isgenerally agreed that the gastroscopist, particularly in the body of thestomach, can more easily and with more certainty make a diagnosis of gas-tritis than the radiologist.
Because it is the radiologist who, after perhaps a test meal, makes the initialexamination of the stomach of a patient with gastric complaints, a great dealof responsibility devolves on him to correctly assess the amount of spasm inthe antrum or any disturbance of antral systole5 which he may see during thefluoroscopic examination, because it is his judgment of this spasm which deter-mines largely the diagnosis of antral spasm. If the spasm is marked or per-sistent then the radiographs may show this persistent spasm in serial films as anelongation and narrowing of the antrum, giving a picture that is very similarto that of some cases of antral gastritis. Also during fluoroscopic examination,and assisted by radiographic studies of the imucosal pattern of the antrum, heImutist estimate any rigidity or abnormality of the normal mucosal folds before
402

Volume 124Number 2 ANTRAL GASTRITIS AND SPASM
making a diagnosis of antral gastritis. In our experience, a diagnosis of local-ized prepyloric hypertrophic gastritis has been made too frequently by radiolo-gists in patients showing some degree of antral spasm with radiographicevidence of marked folds when on gastroscopic examination no evidence of anyinflammatory process could be seen, and even the folds were obliterated by thedistention necessary to the examination. This difficulty was foreseen by Gor-sell,4 in I923, when he stated that: "Great experience and thorough compara-tive investigation are necessary before we are able to distinguish the pathologictypes of the relief from the normal ones, and to separate the outlines formedby the defects or infiltrations of the intestinal wall from the relief of a con-tracted mucous membrane." And, more particularly, the fervent hope of
~~1(_.... . ...,
~~~~~~~~~~~~~~~~~~~~~F I G*.2
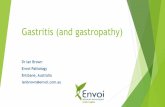
FIG. I.-Case i Antral spasm, slight indentation of duodenal cap Normal folds.FIG. 2.-Case I Normal stomach one year later. Border folds of Chaoul clearly seen.
Kirklin,8 in I937, "further I hope that neither the roentgenologic and thegastroscopic diagnosis of gastritis will become common until the morbid anat-omy of the disease, its right to be considered a pathologic entity and its clinicalsignificance become better understood and more firmly established," still holdsa great deal of truth today. Therefore, it is desirable that the diagnosis ofantral gastritis be made only in those cases where there is demonstrable stiffen-ing and irregularity of the antral mucosal folds or presence of an inflammatoryfilling defect, or where definite signs of inflammation are seen on gastroscopicexamination. The degree of corelation between the roentgenologic and gastro-scopic diagnosis of gastritis is stated by Renshaw13 to be 93 per cent. In 842cases, a positive diagnosis of gastritis was made in 17.7 per cent where therewas a negative roentgenologic examiniation, and in 7.9 per cent of cases diseasewas excluded whlere a positive diagnosis of gastritis had been made by theradiologist.
403

JAMES W. R. RENNIE Annals of SurgeryW. R.RENNIE ~~August, 1946
The symptomatology of antral spasm and gastritis, unfortunately, presentsno classical pattern such as is usually stated for peptic ulcer, carcinoma of thestomach or gallbladder disease, but is a peculiar combination of the symptomsof all three conditions. Pain in the epigastrium is the outstanding symptom.The pain bears no constant relation to food, being sometimes relieved, but moreoften made worse by eating. Anorexia with weight loss is common, and distastefor fats and heavy fried foods is common. In antral gastritis, hemorrhage issaid to occur in I9.7 per cent of cases (Benedict).2 In reviewing 34 cases ofantral spasm found during 487 consecutive roentgenologic examinations of thestomach, it was found that these cases had an amazing similarity in their
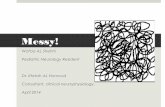
FIG. 3.-Case 2: Hypertrophic antral gastritis. Elongation and narrowing of anitrum.Kirklin's sign present. Thickened antral folds.
FIG. 4.-Case 2: Progressive improvement six months later.
symptoms, and it is of further interest that these symptoms do not vary sig-nificantly from those cases of antral gastritis which we have seen.
Physical examination yields little information. Schindler has described atender area to the left of the navel in some cases.1
Gastric acidity tends to be normal or high in cases of antral gastritis, but inantral spasm we have found that the free acid is low or absent with anordinary test meal.
As has been mentioned, antral spasm is best estimiated by the radiologistduring fluoroscopy and with serial films which show the constant spasm with-out derangement of the normal folds of the antrum during contraction of theantrum. A detailed discussion of the mechanism of the production of thesefolds is without the scope of this paper. A roentgenologic diagnosis of antral
404

Volume 124Number 2 ANTRAL GASTRITIS AND SPASM
gastritis can be made during fluoroscopy in the presence of a deranged antralsystole coupled with the finding of stiff unnatural folds which cannot be oblit-erated by pressure. The radiographs characteristically show persistent spasmwith elongation and funnel-shaped narrowing of the antrum. Sometimes thereis indentation of the duodenal cap said to be due to the stiffened mucosa beingsqueezed through the pyloric ring. This sign, "Kirklin's sign," is seen mostcharacteristically in the type of case called pyloric stenosis" in adults, andwhich according to Stout are associated with histologic evidence of gastritis.
FIG. 5.-Case 3: Extreme hypertrophic antralgastritis, simulating carcinoma.
This extrusion of the mucosa through the pyloric ring may also be extreme ingastritis, without hypertrophy of the pylorus, and is recently reported12 as"extrusion of the mucosa through the pyloric ring." The mucosal pattern,although enlarged and stiffened, is not usually disrupted, and the folds on reliefcan be seen both fluoroscopically and radiographically to run through theantrum. Even in the extreme hypertrophic forms, the complete normal archi-tecture is not always disturbed, and the border folds of Chaoul can often beidentified.
As yet no pathologic classification seems complete to cover all the types ofinflammation in the antrum of the stomach seen rocntgenologically, at oper-ation, or in the pathology laboratory after gastric resection. Schindler's classi-fication covers those seen gastroscopically and refers mainly to the changes inthe mucosae as does the classification given by Vaughn,'5 in which he dividesthe gross pathology into three types-(i) acute edematous; (2) ulcerative;
405

JAMES W. R. RENNIE Annals of SurgeryAugust. 1946
and (3) chronic inflammatory, with hypertrophy, which lhe correlates with thegastroscopic pictures of-(a) reddening with edema; (b) reddening witlulceration, and chronic hypertrophic gastritis or the cobble stone appearance.Neither Schindler's or Vaughn's classification appear to include a type of hyper-trophic antral gastritis of which the three cases described by Konjetzny10 aresimilar to Case 3 presented in this paper. Also, the above classification seemsto indicate that the process begins in the mucosa and submucosa and mayspread to the deeper tissues. Particularly in the extreme hypertrophic formsit may be that the process is an interstitial gastritis, and the mucosal changesand the ulceration may be secondary.
Unexplained, also, is the relation of spasm which is always present. If anianalogy holds to the rest of the gastro-intestinal tract, it may be that a dis-turbance in function exhibited as spasm is the underlying factor, and that themucosal, and submucosal or interstitial inflammation or hypertrophic changes,are secondary to the spasm.
The differential diagnosis is of interest to the surgeon mainly in those caseswith a defect in the antrum which simulates carcinoma. Attention to mucosarelief patterns will provide the diagnosis in many cases aided by gastroscopicexamination. However, there are some cases6 in which a definite differentialdiagnosis cannot be made between inflammatory infiltration of the antrumii,ulceration, hypertrophic defects, and carcinoma. These doubtful cases may beobserved for short periods, and with repeated examinations, but if after thisbrief period of observation a definite diagnosis cannot be ma(le, then explora-tion should be carried out. It should be emphasized that even at operation itstill may not be possible to rule out carcinoma, and even biopsy is not infal-lible. If any doubt as to exact nature of a lesion in the antrum exists at celiot-omy, gastric resection should be done without further delay. With the presentreasonably low mortality for gastric resection, delay in operation, with its riskof permitting an operable carcinoma to develop into an inoperable one, isunjustified.
CASE REPORTS
Case I.-P. D., a 47-year-old white male, with stomach trouble for one year.Attacks of epigastric distress present for one month. Pain comes on four hours aftereating. Gas on stomach troublesome. Loss of I4 lbs. weight in one year. No freeacid (I9 units in one hour). Roentgenologic examination: Localized prepyloricgastritis. Gastroscopic examination: Mucosa of antrum normal orange-red color. Somefolds in antrum but these neither stiffened or nodular. Diagnosis: Antral spasm. Patientput on a bland diet and antispasmodics. One year later roentgenologic examination-normal stomach and antrum.
This is a case in which the correct diagnosis is antral spasm.
Case 2.-A. C., a 54-year-old white male, with gaseous dyspepsia for one year.Gas causes dyspnea. Distress after meals but no relation to any particular food. Acid-fasting 55/92; one hour 52/84. Roentgenologic examinations: First films showed adefect in prepyloric region which suggested carcinoma. Examination repeated in twoweeks after treatment showed improvement, so further observation decided. After six
406

Volume 124 ANTRAL GASTRITIS AND SPASMNumber 2
months defect had disappeared, and only spasm with thickened antral folds present.Symptoms relieved. Patient has remained well. Diagnzosis: Antral gastritis.
This is a case of antral gastritis in which progressive improvement tookplace under observation.
Case 3.-T. M., a 46-year-old white male. Epigastric discomfort after meals,vomiting occasionally for one year. Anorexia and weight loss 15 lbs. one year. Severepain on day of admission, with blood in stools. Low acid with test meal. Clinicalimpression: Ulcer or gastritis. Roentgenologic examination: Annular filling defectin antrum practically occluding pylorus, with appearance of new growth. OperativeFindings: Large firm mass in antrum of stomach. Serosa white and infiltrated withsmall excrescences resembling peritoneal implants. Subpyloric and lower nodes alonglesser curvature enlarged. Gross appearance resembled carcinoma, so gastric resection
Fi ( Fr 7FIG. 6 Case 4 Carcinoma of the pylorus simulating antral gastritis. Gastrostomy
negative.FIG. 7.-Case 4: Carcinoma of the pylorus six months later. Frozen-section negative.
Paraffin section-adenocarcinoma of pylorus.
proceeded with on this basis. Anterior P6lya resection, antecolic anastomosis. Unevent-ful recovery.
Pathologic Report: Resected stomach. Large mass in antrum. Stomach openedshows an ulcer, Y4 inches in diameter on anterior wall near lesser curvature, three inchesfrom pylorus. Ulcer is shallow with a necrotic base. Mucosa of antrum is red andedematous and thrown into large folds. The wall of the antrum is thickened, measur-ing 2 cm. The muscular coat is not interrupted and can be traced through the mass.
Microscopically: All coats show edema, with infiltration by large and smalllymphocytes, plasma cells and many eosinophils. The reaction is most severe in thesubmucosa. There is also a diffuse fibrosis throughout the muscular layers.
This is a case of extremie hiypertrophic gastritis, wvhich by roentgenologicexamination and at operationi could not be distinguished fromi carcinoma.
407

JAMES W. R. RENNIE Analgof Surgery
Treated by gastric resection, with uneventful recovery and relief of symptomssix months after operation.
Case 4.-A. R., a 57-year-old white female. Epigastric distress of one year'sduration with anorexia. Distress made worse by food. Vomiting recently. No weightloss. No free acid, but moderate amounts of free and combined acid on serial sampleswith ordinary test meal. Roentgenologic examination: localized prepyloric gastritiswith spasm, with 25%, retention in five hours. This did not improve on a short medicalregimem.
Operative Findinigs: At the pyloric end of the stomach, and invaginating theduodenum was a rubbery induration and thickening of the antrum of the stomach. Nodiscrete mass. Gastrotomy performed. Mucosa normal. Pylorus normal. Impression-antral gastritis. Abdomen closed.
Patient made an uneventful recovery anid was well for six months, when vomitingrecurred, accompanied by a small loss of weight. No aniemia. Roentgenologic examina-tion now showed prepyloric spasm with some narrowing of the pylorus. Peristalsisseen to pass through the antrum to the pylorus.
Gastroscopic Examination: Persistent spasm in the antrum. Mucosa of angulusanid body of stomach normal. Pylorus not seen due to spasm.
Operative Findings: Grossly, the stomach was, essentially the same as before.Gastrotomy was performed. Mucosa again appeared normal in the antrum. No ulcera-tion. The pylorus was now narrowed and almost occluded by a ring of firm tissue.Biopsy of the pyloric ring was taken in two places. Frozen-section reported as "chronicinflammatory reaction." Because it was felt that with an apparently normal stomachwith a high grade pyloric obstruction that a posterior gastro-enterostomy would be ade-quate to relieve her symptoms, this was done. Report on paraffin sections: Infiltratingadenocarcinoma of the pylorus. Patient made an uneventful recovery.
This is probably an early case of linitis plastica which on two occasions atoperation, even with biopsy, was mistaken for antral gastritis. Resection isnow contemplated due to apparent low grade of tumor without any knownmetastases.
CONCLUSIONS
(i) Antral spasm and antral gastritis are a fairly common cause of gastriccomplaints and present a not dissimilar clinical picture.
(2) Antral spasm must be differentiated from antral gastritis by roent-genologic and gastroscopic examination.
(3) Pathogenesis of antral gastritis is obscure and present classificationsare incomplete.
(4) Certain types of antral gastritis are indistinguishable from carcinomaof the stomach; exploration and biopsy are not infallible and gastric resectionshould be undertaken unless a positive diagnosis can be made.
REFERENCES1 Arendt, Juliani: ANNALS OF SURGERY, 122, 235, August, 1945.2 Benedict, E. B.: Am. Jr. Roentgenol., 47, 254, February, I942.Crohn, Burrell B.: Chronic Gastritis: Clinical Aspects. Bulletin of the New YorkAcademy of Medicine, 15, 293, June, I939.
Forsell, G.: Am. Jr. Roentgenol., 35, 204, February, 1936.
408

Volume 124 ANTRAL GASTRITIS AND SPASMNumber 2
F Golden, R.: J. A. M. A., I09, 1497, November, 1937.e Harris, Charles M.: Am. Jr. of Surgery, 68, 26T, May, I941.7 Kantor, J. L.: Am. J. Roentgenol., 35, 204, February, I936.8 Kirklin, B. R.: Radiology, 29, 493, 1937.9 Kirklin, B. R., and Harris, Milo T.: Am. Jr. Roentgenol., 29, 437, April, 1933.
"0 Konjetzny, G. E.: Der Chirug., 10, 260, April I5, I938." McClure, C. C.: Surg., Gynec. & Obst., 52, 945, May, I93I.12 Norgore, Martin, and Shuler, Ivan J. D.: Surgery, I8, 452, October, 1945.13 Renshaw, R. J. F.: Am. Jr. Roentgenol., 47, 254, February, I942."I Schindler, Rudolph: Rocky Mountain Medical Journal, 37, 570, August, 1940.lb Vaughn, Walter: Radiology, 44, 53I, June, 1945.
409