Antiphospholipid antibodies associated with clozapine treatment
2
166 Letters and Correspondence REFERENCES I. Endo Y, Yokota T, Tsutamoto Y, Kodma M: lo6 depletion of WBC with CF-2, a new leucocyte removal filter. Am J Haematol44:3841, 1993. 2. Sivakumaran M, Tan L. Revill JA, Hutchinson RM, Norfolk DR, Major K, Wood JK: Evaluation of the ‘handling capacity’ of Pall R C l W leucocyte removal filters and the effect of air introduction on its performance. (Submitted). 3. Sivakumaran M, Norfolk DR, Major KG, Revill JA, Hutchinson RM, Wood JK: A new method to study the efficiency of third generation blood filters. Br J Haematol 84:175-177, 1993. 4. Sivakumaran M, Hutchinson RM, Wood JK, Revill JA, Ghosh K, Myint S: Removal of cytomegalovirus (CMV) infected leucocytes from CMV seropositive blood units by bedside filtration. Br J Haematol 135, 1993. TABLE 1. Laboratory Profile’ Antiphospholipid Antibodies Associated With Clozapine Treatment To rhe Editor: “Lupus” anticoagulants were originally described in patients with systemic lupus erythematous (SLE). Subsequently these inhibitors were demonstrated in a variety of other diseases, and with the administra- tion of drugs, especially chlorpromazine (CPZ) [ 11. It is now believed that these coagulation inhibitors are a heterogenous group of antibodies directed to epitopes of proteins complexed with negatively charged phospholipids 121. These antibodies are termed lupus anticoagulants (LA) and anticardio- lipin antibodies (ACLA); collectively, they are called antiphospholipid antibodies (APLA) [3]. It is believed that LA activity can be separated from APLA and that the activity can be discordant [4]. Clozapine is a dibenzodiazepine-derivative antipsychotic effective in the treatment of patients with refractory schizophrenia. The drug has a pipera- zine-substituted tricyclic structure that primarily differs from phenothi- azines by the presence of a 7- rather than a 6-membered central ring. Clozapine was approved for distribution in February 1990 with recommen- dations for strict monitoring of white cell counts because of the risk of agranulocytosis. In this report, a patient with chronic schizophrenia on long-term clozapine is shown to have developed asymptomatic APLA. The adverse drug reaction files of Sandoz Laboratories (the manufacturer) do not contain a previously reported case of this association. The patient is a 54-year-old Caucasian male who was referred in June 1993 for an elevated prothrombin time (PT) and activated partial thrombo- plastin (apTT) time. The patient was scheduled for elective surgery for urethral obstruction and bladder neck obstruction. Symptoms included uri- nary frequency and nocturia without gross hematuria. The patient is a known chronic schizophrenic who was placed on clozapine in October 1983. In 1983 and 1990, the patient had a normal aPTT and PT (data obtained from pre-operative screens at other institutes). No bleeding or thrombosis was reported during or following these previous operations. Laboratory data in June 1993 are shown in Table I. The hematologic profile confirmed the presence of APLAs with inhibition studies similar to those seen in patients treated with CPZ. Without discontinuing clozapine the patient underwent direct vision urethrotomy. The patient was dis- charged in 3 days without excessive bleeding. However, 2 days later he returned to the emergency room with a single episode of gross hematuria; he was not hospitalized. Three days later the patient was readmitted to the hospital for gross hematuria. Continuous bladder irrigation (CBI) failed to control gross hematuria totally. After 4 days of CBI epsilon-aminocaproic acid was prescribed by i.v. continuous infusion; gross hematuria disap- peared within 48 hours. Since discharge, there has not been any local or systemic bleeding Although found in normal healthy people, the greatest clinical signifi- cance of APLAs is their association with SLE and other conditions in which thrombosis, thrombocytopenia, and fetal loss are the predominant manifes- tations, i.e., an antiphospholipid syndrome [3]. APLAs can be of the IgG, Parameter Count Bleeding time (3-8 min) 6 &TI (< 32 sec) 45.2 tT (INR 0.761 25) 1.38 Thrombin time (5-15 sec) 5 Fibrinogen (200-400 mg%) 382 D-diamer (negative) Negative Factors V (50-150%)a 84 VII 93 VIII 24 IX 24 X 92 XI 11 XI1 16 ANA (< 1:W) Negative ds-DNA, Fan (< 3.5 unitsiml) 1.3 Serum IgG (565-1,765 mg%) 80 1 IgA (85-385 mg%) 101 IgM (45-250 mg%) 36 I < 30 < 23 Rheumatoid factor (0-35 IU/ml) Anticardiolipin IgG (< 23 GPL) IgM (< 11 MPL) 22 Lupus anticogulant (negative) Positive RPR (negative) Nonreactive *Numbers in parentheses are normal range. ‘Single-stage assays, 1.5 dilution. IgM, or IgA classes; those of the IgM class arise after CMZ administration and are rarely associated with arterial and venous thrombosis [5]. This was clearly the case with our patient, who had elevated serum anticardiolipin (IgM positive), LA, and an absence of thrombotic events. Patients ingesting CMZ for more than 2% years develop increased serum concentrations of IgM and circulating anticoagulants. Greater than 40% have positive ANA and/or antibody to native DNA. The IT is usually normal or slightly prolonged, and the thrombin time and serum fibrinogen are within normal levels. The levels of factors IX, XI, and XI1 are reduced, whereas factor VIII activity is infrequently positive (< 10%) [5,6]. These data are essentially identical to the data obtained in our patient treated for 10 years with clozapine. Because of the increasing use of clozapine and the development of APLAs, it is recommended that physicians and patients treated with cloza- pine be aware of the association with asymptomatic APLAs. Surgery should not be affected by this association. STEPHEN DAVIS HOWARD 0. KERN RENGASWAMY ASOKAN Department of Medicine and Urology, Chilton Memorial Hospital, Pompton Plains, New Jersey REFERENCES I. Schleider MA, Nachman RL, Jaffe EA, et al.: A clinical study of the lupus anticoagulant. Blood 48:499, 1976. 2. Bevers EM, Galli M: B2-glycoprotein I for binding of anticardiolipin antibodies to cardiolipin antibodies to cardiolipin. Lancet 2:952, 1990. 3. Feinstein DI, Francis RB: The lupus anticoagulant and anticardiolipin antibodies. In Wallace DJ, Hahn BH (eds): “Systemic Lupus Erythematosus,” Ed 2. Philadel- phia: Lea & Febiger, 1992, p 246. 4. Bevers EM, Galli M, Barbini T, et al.: Lupus anticoagulant IgGs (LA) are not directed to phospholipid only, but to a complex of lipid-bound human prothrombin Thromb Haemost 66:129, 1991.
-
Upload
stephen-davis -
Category
Documents
-
view
215 -
download
3
Transcript of Antiphospholipid antibodies associated with clozapine treatment
166 Letters and Correspondence
REFERENCES I . Endo Y, Yokota T, Tsutamoto Y, Kodma M: lo6 depletion of WBC with CF-2, a
new leucocyte removal filter. Am J Haematol44:3841, 1993. 2. Sivakumaran M, Tan L. Revill JA, Hutchinson RM, Norfolk DR, Major K, Wood
JK: Evaluation of the ‘handling capacity’ of Pall R C l W leucocyte removal filters and the effect of air introduction on its performance. (Submitted).
3. Sivakumaran M, Norfolk DR, Major KG, Revill JA, Hutchinson RM, Wood JK: A new method to study the efficiency of third generation blood filters. Br J Haematol 84:175-177, 1993.
4. Sivakumaran M, Hutchinson RM, Wood JK, Revill JA, Ghosh K, Myint S: Removal of cytomegalovirus (CMV) infected leucocytes from CMV seropositive blood units by bedside filtration. Br J Haematol 135, 1993.
TABLE 1. Laboratory Profile’
Antiphospholipid Antibodies Associated With Clozapine Treatment
To rhe Editor: “Lupus” anticoagulants were originally described in patients with systemic lupus erythematous (SLE). Subsequently these inhibitors were demonstrated in a variety of other diseases, and with the administra- tion of drugs, especially chlorpromazine (CPZ) [ 11. It is now believed that these coagulation inhibitors are a heterogenous group of antibodies directed to epitopes of proteins complexed with negatively charged phospholipids 121. These antibodies are termed lupus anticoagulants (LA) and anticardio- lipin antibodies (ACLA); collectively, they are called antiphospholipid antibodies (APLA) [3]. It is believed that LA activity can be separated from APLA and that the activity can be discordant [4].
Clozapine is a dibenzodiazepine-derivative antipsychotic effective in the treatment of patients with refractory schizophrenia. The drug has a pipera- zine-substituted tricyclic structure that primarily differs from phenothi- azines by the presence of a 7- rather than a 6-membered central ring. Clozapine was approved for distribution in February 1990 with recommen- dations for strict monitoring of white cell counts because of the risk of agranulocytosis. In this report, a patient with chronic schizophrenia on long-term clozapine is shown to have developed asymptomatic APLA. The adverse drug reaction files of Sandoz Laboratories (the manufacturer) do not contain a previously reported case of this association.
The patient is a 54-year-old Caucasian male who was referred in June 1993 for an elevated prothrombin time (PT) and activated partial thrombo- plastin (apTT) time. The patient was scheduled for elective surgery for urethral obstruction and bladder neck obstruction. Symptoms included uri- nary frequency and nocturia without gross hematuria. The patient is a known chronic schizophrenic who was placed on clozapine in October 1983. In 1983 and 1990, the patient had a normal aPTT and PT (data obtained from pre-operative screens at other institutes). No bleeding or thrombosis was reported during or following these previous operations.
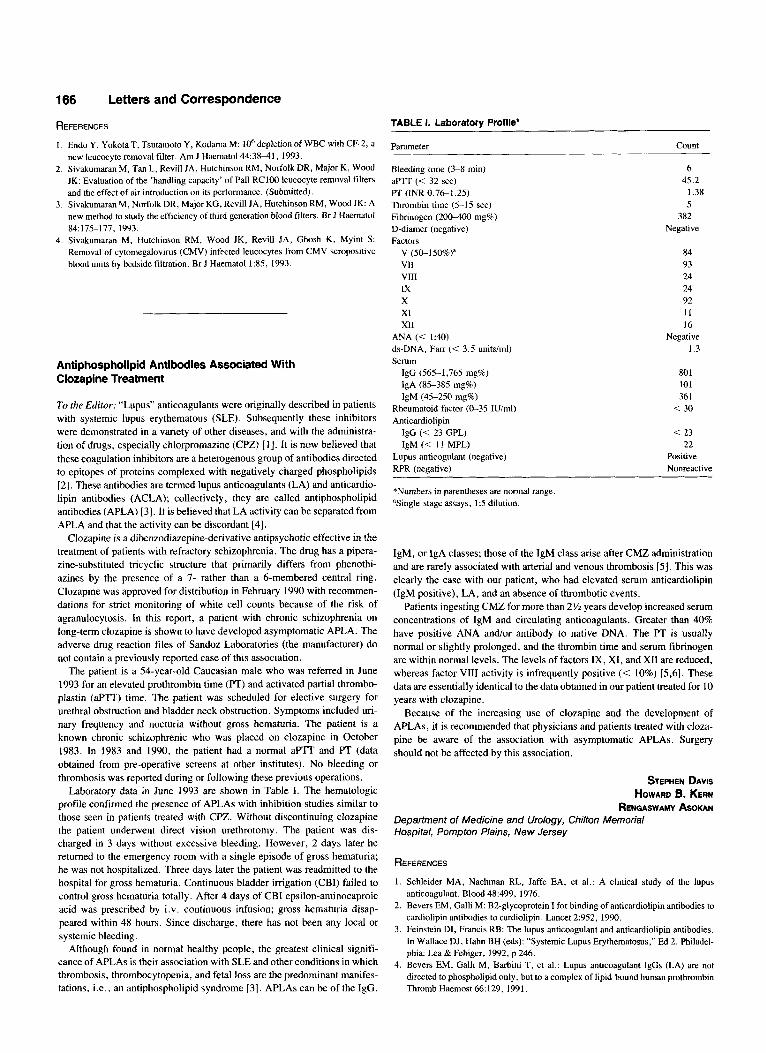
Laboratory data in June 1993 are shown in Table I. The hematologic profile confirmed the presence of APLAs with inhibition studies similar to those seen in patients treated with CPZ. Without discontinuing clozapine the patient underwent direct vision urethrotomy. The patient was dis- charged in 3 days without excessive bleeding. However, 2 days later he returned to the emergency room with a single episode of gross hematuria; he was not hospitalized. Three days later the patient was readmitted to the hospital for gross hematuria. Continuous bladder irrigation (CBI) failed to control gross hematuria totally. After 4 days of CBI epsilon-aminocaproic acid was prescribed by i.v. continuous infusion; gross hematuria disap- peared within 48 hours. Since discharge, there has not been any local or systemic bleeding
Although found in normal healthy people, the greatest clinical signifi- cance of APLAs is their association with SLE and other conditions in which thrombosis, thrombocytopenia, and fetal loss are the predominant manifes- tations, i.e., an antiphospholipid syndrome [3]. APLAs can be of the IgG,
Parameter Count
Bleeding time (3-8 min) 6 &TI (< 32 sec) 45.2 tT (INR 0.761 2 5 ) 1.38 Thrombin time (5-15 sec) 5 Fibrinogen (200-400 mg%) 382 D-diamer (negative) Negative Factors
V (50-150%)a 84 VII 93 VIII 24 IX 24 X 92 XI 11 XI1 16
ANA (< 1:W) Negative ds-DNA, Fan (< 3.5 unitsiml) 1.3 Serum
IgG (565-1,765 mg%) 80 1 IgA (85-385 mg%) 101 IgM (45-250 mg%) 36 I
< 30
< 23
Rheumatoid factor (0-35 IU/ml) Anticardiolipin
IgG (< 23 GPL) IgM (< 11 MPL) 22
Lupus anticogulant (negative) Positive RPR (negative) Nonreactive
*Numbers in parentheses are normal range. ‘Single-stage assays, 1.5 dilution.
IgM, or IgA classes; those of the IgM class arise after CMZ administration and are rarely associated with arterial and venous thrombosis [5] . This was clearly the case with our patient, who had elevated serum anticardiolipin (IgM positive), LA, and an absence of thrombotic events.
Patients ingesting CMZ for more than 2% years develop increased serum concentrations of IgM and circulating anticoagulants. Greater than 40% have positive ANA and/or antibody to native DNA. The IT is usually normal or slightly prolonged, and the thrombin time and serum fibrinogen are within normal levels. The levels of factors IX, XI, and XI1 are reduced, whereas factor VIII activity is infrequently positive (< 10%) [5 ,6] . These data are essentially identical to the data obtained in our patient treated for 10 years with clozapine.
Because of the increasing use of clozapine and the development of APLAs, it is recommended that physicians and patients treated with cloza- pine be aware of the association with asymptomatic APLAs. Surgery should not be affected by this association.
STEPHEN DAVIS HOWARD 0. KERN
RENGASWAMY ASOKAN Department of Medicine and Urology, Chilton Memorial Hospital, Pompton Plains, New Jersey
REFERENCES
I . Schleider MA, Nachman RL, Jaffe EA, et al.: A clinical study of the lupus anticoagulant. Blood 48:499, 1976.
2. Bevers EM, Galli M: B2-glycoprotein I for binding of anticardiolipin antibodies to cardiolipin antibodies to cardiolipin. Lancet 2:952, 1990.
3. Feinstein DI, Francis RB: The lupus anticoagulant and anticardiolipin antibodies. In Wallace DJ, Hahn BH (eds): “Systemic Lupus Erythematosus,” Ed 2. Philadel- phia: Lea & Febiger, 1992, p 246.
4. Bevers EM, Galli M, Barbini T, et al.: Lupus anticoagulant IgGs (LA) are not directed to phospholipid only, but to a complex of lipid-bound human prothrombin Thromb Haemost 66:129, 1991.

Letters and Correspondence 167
examined patients with AML and found leukaemic thrombi or aggregates in 40% of autopsy specimens. Thrombosis of major vessels was uncommon, with only 4 of 82 patients demonstrating coronary artery or internal carotid artery occlusion. Thrombosis of peripheral arteries was not reported.
Macrovascular occlusion in the absence of the hyperleukocytosis syn- drome has not been reported. Our patient had a claudication history sugges- tive of superficial femoral artery stenosis and a subacute deterioration over several weeks, culminating in clinically critical ischaemia. Cytotoxic ther- apy with reduction in WCC coincided with resolution of symptoms and signs of ischaemia over several days. We propose that hyperleukocytosis developed in this patient, producing leukostasis at the site of an atheroscle- rotic stenosis. Chemotherapy then reduced the WCC and reversed the luminal stenosis, allowing recovery of tissue perfusion. Angiography was not performed on admission because of dehydration, hypercalcaemia, and the perceived urgency to initiate chemotherapy.
While the risk of development of the hyperleukocytosis syndrome in- creases with the absolute WCC (31, the kinetics of blast cell turnover are important, as leukostasis occurs particularly when the doubling time is short [4]. While the kinetics of cell turnover were unknown, symptoms had been present for several weeks, suggesting the blast count had been ele- vated for some time. The patient’s observed leukocrit at presentation was 14 ml/dl [ S ] . The erythrocnt was 45 mlidl and hence the minimum apparent viscosity was > 4.5 centipoise (51. Dehydration induced by vomiting and hypercalcaemia may have contributed to this increased blood viscosity, particularly at the site of a pre-existing femoral artery stenosis, resulting in local vascular insufficiency without clinical evidence of leukostasis else- where.
5. Zucker S , Farrabi MH, Gail S , et al.: IgM inhibitors of the contact activation phase of coagulation in chlorpromazine treated patients. Br J Haematol40447, 1978.
6. Zarrabi MH, Zucker S, Miller F, et al.: Immunologic and coagulation disorders in chlorpromazine treated patients. Ann Intern Med 91: 194, 1979.
Acute Leg lschaemia as a Manifestation of the Hyperleukocytosis Syndrome in Acute Myeloid Leukaemia
To the Editor: Hyperleukocytosis is a recognised cause of morbidity and mortality in acute leukaemias [I]. The clinical syndrome is a consequence of leukostasis in the pulmonary and cerebral circulations [2]. Major periph- eral vessel occlusion has not been reported.
A 74 year old smoker was admitted for management of a critically ischaemic left leg. He had a history of stable claudication of the left calf but complained of decreasing claudication distance over 3 weeks, with concur- rent development of rest pain and leg weakness. He also reported 2 weeks of anorexia, bilateral upper abdominal pain, nausea, and vomiting. Exami- nation revealed an unwell, moderately dehydrated man with tender he- patosplenomegaly. The left leg was cold below the knee and dusky with absent popliteal and pedal pulses and poor capillary return. Neuromuscular examination of the leg was normal.
Full blood examination revealed haemoglobin 14.4 g/dL, WCC 225 X 109/L (blasts 186 X 109/L, neutrophils 11.98 x lo9& lympho- cytes 2.4 X 109/L, monocytes 6.7 X 109/L, eosinophils 4.5 X 109/L, bands 2.25 X 109/L, myelocytes 4.5 X 109/L, eosinophils 4.5 X 109/L, bands 2.25 X 109/L, myelocytes 4.5 X 109/L, promyelocytes 6.7 X lo9/ L), platelets 75 X 109/L. The serum albumin was 34 g/L and serum cal- cium 2.88 mmol/L (2.15-2.6 mmol/L). Bone marrow examination con- firmed the diagnosis of acute myeloid leukaemia (AML) M2. Intravenous mitoxantrone (10 mg/mZ DI-3) and cytosine arabinoside (100 mg/m’ D1-7) were commenced, with reduction in the WCC to < SO X 109/L within 3 days.
On D7 the left leg was warm and well perfused although there were two areas of infarction on the left heel. On D17 the patient was ambulating up to 50 metres without claudication. Bone marrow examination on D20 demon- strated persistent leukaemia. Accordingly, reinduction chemotherapy was initiated (daunorubicin SO mg/mz D1-3, etoposide 75 mg/m2 D1-7, cy- tosine arabinoside 100 mg/m’ D1-7).
Postmortem examination of patients with AML has shown that leu- kaemic thrombi or intravascular aggregates are common. McKee et al. [3]
JANINE CAMPBELL CHRISTINA A. MITCHELL
Department of Medicine, Monash University, Box Hill Hospital, Melbourne. Australia
REFERENCES
1. Dutcher JP, Schiffer CA, Wiernik PH: Hyperleukocytosis in adult acute nonlym- phocytic leukaemia: Impact on remission rate and duration, and survival. 1 Clin Oncol5:13641372, 1987.
2. Lichtman MA, Gregory A, Keamey E: Rheology of leukocytes, leukocyte suspen- sions and blood in leukaemia. J Clin Invest 52:35&358, 1973.
3. McKee LC, Collins RD: Intravascularleukocyte thrombi and aggregates as a cause of morbidity and mortality. Medicine 53:463, 1974.
4. Vemant JP, Brun B, Mannoni P, Dreyfus B: Respiratory distress of hyperleuko- cytic granulocytic leukaemias. Cancer 44:264-268, 1979.
5. Lichtman MA, Rowe JM: Hyperleukocytic leukaemias: Rheological, clinical and therapeutic considerations. Blood 60:279-283, 1982.