
Antimicrobials in the Pediatric ICU February 24, 2015 Ashley Casper, Pharm.D.
51
Antimicrobials in the Pediatric ICU February 24, 2015 Ashley Casper, Pharm.D.
-
Upload
solomon-roland-johns -
Category
Documents
-
view
213 -
download
0
Transcript of Antimicrobials in the Pediatric ICU February 24, 2015 Ashley Casper, Pharm.D.

Antimicrobials in the Pediatric ICU
February 24, 2015Ashley Casper, Pharm.D.

Objectives• Evaluate general aspects of microbiology including
bacterial differentiation, microbial terminology, and classes of antibiotics.
• Explain the mechanism of action, spectrum of activity, and toxicities of the most commonly used antimicrobials in the PICU setting.
• Use patient, culture results, and location of infection to select appropriate antimicrobial coverage.
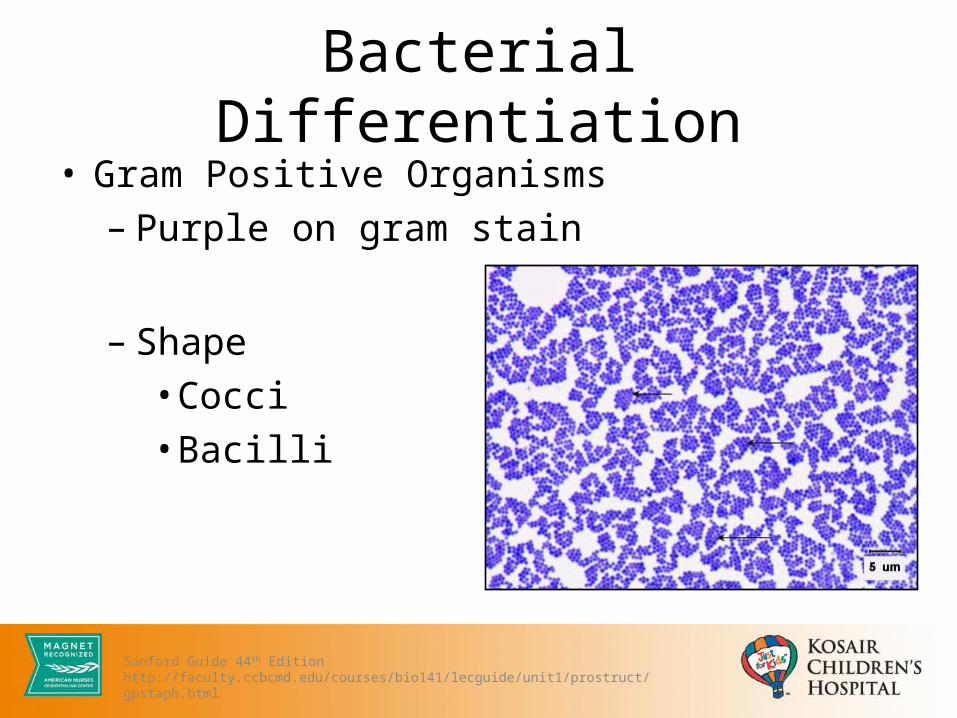
Bacterial Differentiation• Gram Positive Organisms– Purple on gram stain
– Shape• Cocci• Bacilli
Sanford Guide 44th Editionhttp://faculty.ccbcmd.edu/courses/bio141/lecguide/unit1/prostruct/gpstaph.html

Gram Positive Organisms
Sanford Guide 44th Edition

Gram Positive Organisms
• Staphylococcus aureus• Staphylococcus
epidermis• Streptococcus
pneumoniae• Enterococcus faecalis• Enterococcus faecium
• Bacillus• Corynebacterium• Clostridium• Actinobacteria• Listeria
Sanford Guide 44th Edition

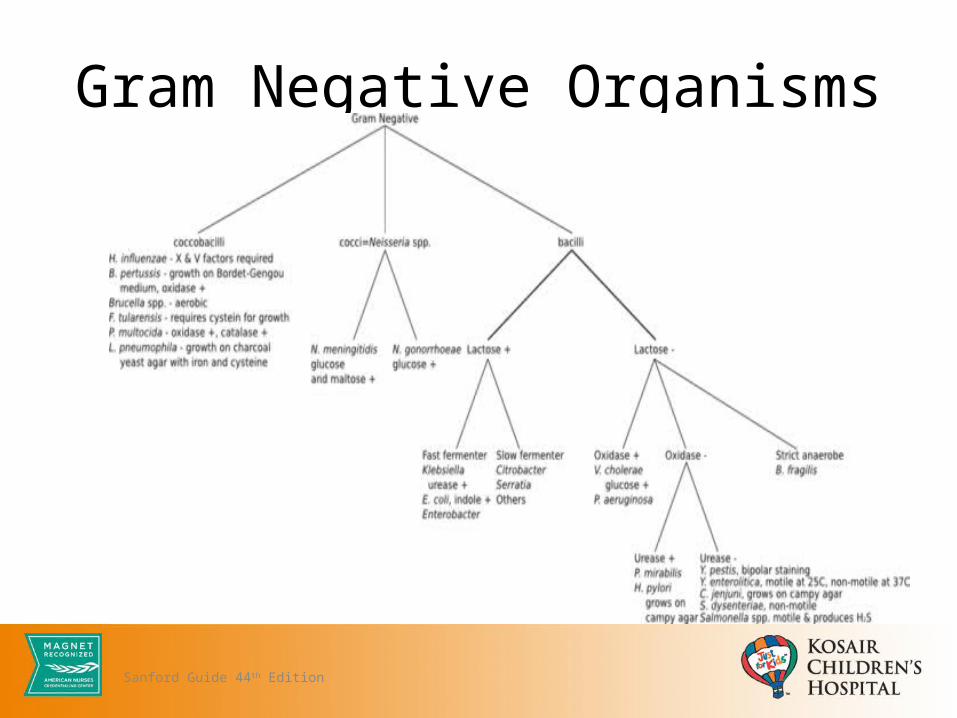
Gram Negative Organisms• Gram Negative Organisms– Pink on gram stain
– Shape• Cocci• Bacilli• Coccobacilli
Sanford Guide 44th Edition
Gram Negative Organisms
Sanford Guide 44th Edition

Gram Negative Organisms
• Acinetobacter spp.• Enterobacter spp. • Escherichia coli• Haemophilus influenzae• Klebsiella pneumoniae• Moraxella catarrhalis• Pseudomonas
aeruginosa
• Proteus spp. • Serratia spp.• Salmonella spp.• Stenotrophomonas
maltophilia• Aeromonas spp.• Neisseria spp.
Sanford Guide 44th Edition
Miscellaneous Organisms
• Anaerobes– Peptostreptococcus
spp.– Bacteroides fragilis– Clostridium spp.
• Atypicals– Chlamydia
pneumoniae– Mycoplasma
pneumoniae– Legionella spp.
Sanford Guide 44th Edition

Fungi• Two groups– Yeast• Solitary rounded form – clusters
– Mold• Branching filaments - hyphae
http://www.doctorfungus.org/imageban/index.htm

Fungi
• Aspergillus spp• Blastomyces dermatitidis• Candida spp.• Coccidioides immitis• Cryptococcus spp.• Histoplasma spp.
• Paracoccidioides brasiliensis
• Sporothrix schenckii • Zygomycetes spp.
Sanford Guide 44th Edition

Viruses
• Adenovirus• Coronavirus• Coxsackievirus• Enterovirus• Hepatitis • Cytomegalovirus• Herpes virus
• Parainfluenza• Parvovirus• Respiratory syncytial
virus• Rhinovirus• Influenza• Rotavirus
Sanford Guide 44th Edition

Definitions• Bactericidal– an antibiotic that kills microorganisms
• Bacteriostatic – an antibiotic that inhibits the growth of
microorganisms
Tortora. Microbiology. 2014

Definitions• Minimum Inhibitory Concentration (MIC)– lowest concentration of an antibiotic that
completely inhibits the growth of a microorganism
• Minimum Bactericidal Concentration (MBC)– lowest concentration of an antibiotic that
completely kills the growth of a microorganism
Tortora. Microbiology. 2014
Definitions• Cpmax
– Serum peak concentration after administration of an antimicrobial agent
• Area under the curve (AUC)– Measures the extent of exposure and time in which antimicrobital
levels remain above the target MIC during a dosing interval
• Post-Antibiotic Effect (PAE)– Continued inhibition of the organism for a period of time after the
concentration of the antimicrobial agent has dropped below the MIC
Tortora. Microbiology. 2014
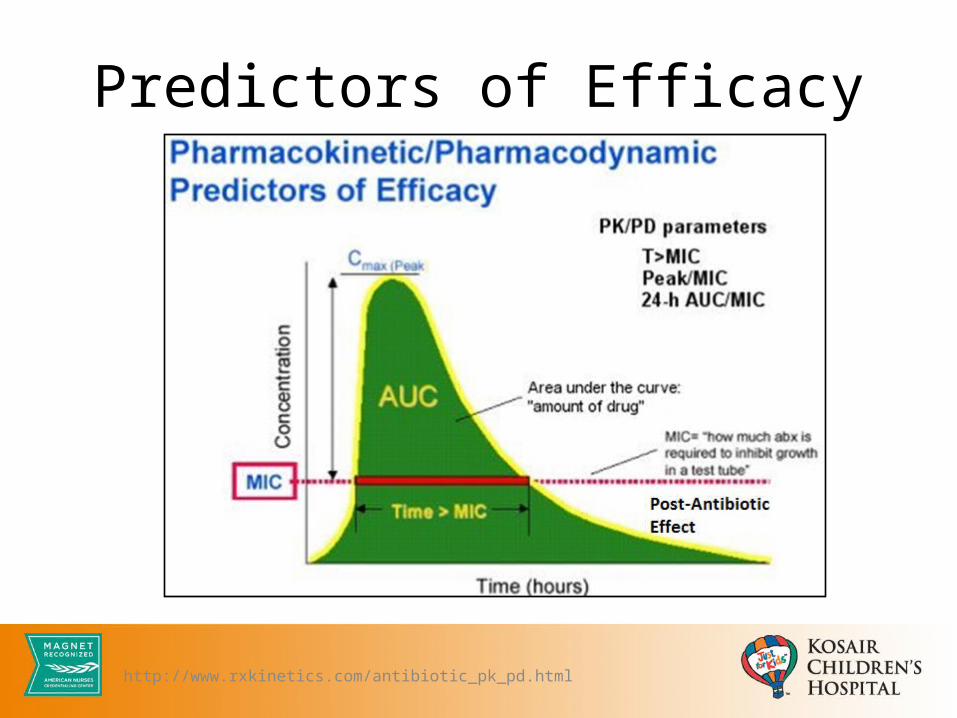
Predictors of Efficacy
http://www.rxkinetics.com/antibiotic_pk_pd.html
Antibiotic Activity• Concentration-Dependent
– Rate and extent of microorganism killing are a function of the antimicrobial concentration
– PD parameter: 24h-AUC/MIC; Peak/MIC
• Time-Dependent– Rate and extent of microorganism killing remain unchanged
regardless of antimicrobial concentration– Killing is dependent on time maintained above the MIC– PD parameter: Time > MIC
Int J Antimicrob Agents 1999;11:7Bradley, JS. Principles and Practice of Infectious Diseases. Ch 292 Antimicrobial Agents. 2015

Antibiotic Activity
Int J Antimicrob Agents 1999;11:7

Antibiotic Activity
Pattern of Activity Antibiotics Goal of Therapy PK/PD Parameter
Concentration-dependent killing
AminoglycosidesDaptomycin
FluoroquinolonesKetolides
Maximize concentrations 24h-AUC/MICPeak/MIC
Time-dependent killing
CarbapenemsCephalosporinsErythromycin
LinezolidPenicillins
Maximize duration of exposure T>MIC
Bradley, JS. Principles and Practice of Infectious Diseases. Ch 292 Antimicrobial Agents. 2015
Commonly Used Antimicrobials in PICU• Antivirals • Aminoglycosides• Antifungals • Carbapenems • Cephalosporins • Penicillins • Vancomycin• Linezolid

Antivirals• Acyclovir
– Mechanism of action: inhibition of DNA synthesis and viral replication by competing with deoxyguanosine triphosphate for viral DNA polymerase and being incorporated into viral DNA.
– Spectrum of activity: HSV 1, HSV 2, and Varicella Zoster Virus (VZV)
Lexi-Comp.http://depts.washington.edu/hivaids/derm/case2/discussion.html#ref
Antivirals• Acyclovir– Dosing: • HSV encephalitis: 10-15 mg/kg/dose Q8H x 14-21 days• VZV treatment: 10 mg/kg IV Q8H x 7-10 days (continue for
> 48h after last lesion has appeared)– Adverse effects/toxicities:• GI: nausea/vomiting• Renal: acute renal failure (increased creatinine or BUN)
Lexi-Comp.Micromedex
Aminoglycosides• Gentamicin/Tobramycin– Mechanism of action: interferes with bacterial protein
synthesis by binding to 30S and 50S ribosomal subunits resulting in a defective bacterial cell membrane
– Spectrum of activity: susceptible gram negative bacilli (Pseudomonas, E. coli, Proteus, Serratia, and syngergy for gram-positive Staphylococcus)
Lexi-Comp.Micromedex
Aminoglycosides• Gentamicin/Tobramycin
– Dosing (several dosing schemes): • KCH – extended interval dosing
– Infants and children: 7.5 mg/kg/dose IV Q24H• Synergy – 3 mg/kg/dose IV Q24H or 1 mg/kg/dose IV Q8H
– Monitoring: 4 and 8 hour levels (calculate PK parameters)– Adverse effects/toxicities:
• Neurologic: Neuromuscular blockade finding• Otic: Ototoxicity• Renal: Nephrotoxicity
Lexi-Comp.Micromedex
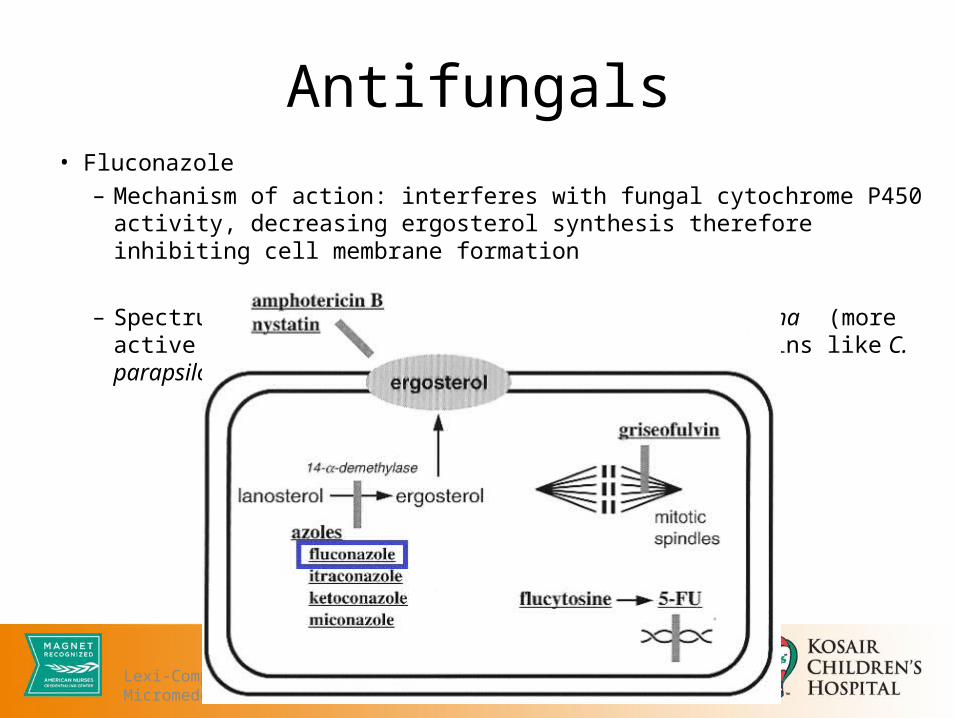
Antifungals• Fluconazole – Mechanism of action: interferes with fungal cytochrome P450 activity,
decreasing ergosterol synthesis therefore inhibiting cell membrane formation
– Spectrum of activity: Candida, Blastomycoses, Histoplasma (more active against C. albicans than other candidal strains like C. parapsilosis, C. glabrata, and C. tropicalis)
Lexi-Comp.Micromedex

Antifungals• Fluconazole
– Dosing: • Treatment: 6-12 mg/kg x 1, followed by 3-12 mg/kg Q24h
– Adverse effects/toxicities:• GI: nausea, vomiting• Neurologic: headache
– Resistance is becoming an issue
Lexi-Comp.Micromedex
Antifungals• Voriconazole (second generation triazole)– Mechanism of action: interferes with fungal cytochrome P450
activity (selectively inhibits 14-alpha-lanosterol demethylation), decreasing ergosterol synthesis (principal sterol in fungal cell membrane) and inhibiting fungal cell membrane formation
– Spectrum of activity: Candida, Aspergillus (drug of choice!)
Lexi-Comp.Micromedex

Antifungals• Voriconazole (second generation triazole)
– Dosing: 9 mg/kg/dose IV or PO Q12H – Monitoring:
• Trough levels after 3-5 days of therapy or change in formulation (PO versus IV)
• Renal function (contraindicated if CrCl < 50)– Adverse effects/toxicities
• CNS: hallucinations• Visual: abnormal vision, color vision change, photophobia• Hepatic: hepatitis, jaundice, cholestasis
Lexi-Comp.Micromedex
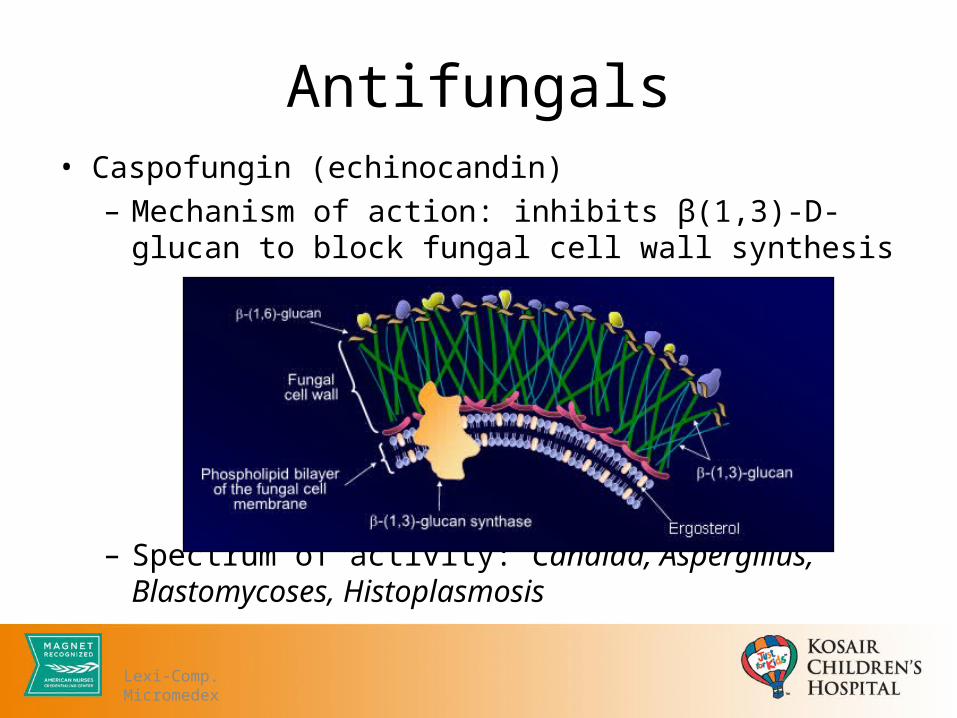
Antifungals• Caspofungin (echinocandin)
– Mechanism of action: inhibits β(1,3)-D-glucan to block fungal cell wall synthesis
– Spectrum of activity: Candida, Aspergillus, Blastomycoses, Histoplasmosis
Lexi-Comp.Micromedex
Antifungals• Caspofungin (echinocandin)
– Dosing: • 70 mg/m2 x 1, followed by 50 mg/m2/dose IV Q24h
– Adverse effects/toxicities:• CV: hypotension• Dermatologic: rash• GI: diarrhea• Hepatic: increased AST/ALT• Other: fever, shivering
Lexi-Comp.Micromedex
Carbapenems• Meropenem– Mechanism of action: inhibits bacterial cell wall synthesis by
binding to penicillin-binding proteins which inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls
– Spectrum of activity: multi-drug resistant infections caused by gram-negative and gram-positive aerobic and anaerobic pathogens
Lexi-Comp.Micromedex

Carbapenems• Meropenem
– Dosing:• 20 mg/kg Q8H - non-CNS infections• 40 mg/kg Q8H – meningitis/concern for multi-drug resistant
organisms (CF population, chronic patients)– Adverse effects/toxicities:
• Dermatologic: rash• GI: diarrhea, nausea, vomiting• Hematologic: anemia• Increased risk for seizures?!
Lexi-Comp.Micromedex
Cephalosporins• Cefazolin (1st generation)– Mechanism of action: inhibits bacterial cell wall synthesis by
binding to penicillin-binding proteins which inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell wall
– Spectrum of activity: treatment of Streptococcus sp, MSSA, E. coli, H. influenzae
Lexi-Comp.Micromedex

Cephalosporins• Cefazolin (1st generation)– Dosing: • 25 mg/kg/dose IV Q6-8H (Max: 1-2 g)
– Adverse effects/toxicities:• Dermatologic: pruritus• GI: diarrhea
Lexi-Comp.Micromedex
Cephalosporins• Ceftriaxone (3rd generation)
– Mechanism of action: inhibits bacterial cell wall synthesis by binding to penicillin-binding proteins which inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls.
– Spectrum of activity: cefazolin activity + additional gram negative coverage including Enterobacter, Serratia, N. meningitidis, Citrobacter
Lexi-Comp.Micromedex

Cephalosporins• Ceftriaxone
– Dosing: • Meningitis: 50 mg/kg/dose IV Q12H• Acute otitis media: 50 mg/kg/dose IM/IV Q24H x 3 doses• All other infections: 75 mg/kg/dose IV Q24H
– Adverse effects/toxicities:• Dermatologic: pruritus• GI: diarrhea
Lexi-Comp.Micromedex

Cephalosporins• Cefepime (4th generation)– Mechanism of action: inhibits bacterial cell wall synthesis by
binding to penicillin-binding proteins which inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls. Activity in the presence of some beta-lactamases
– Spectrum of activity: ceftriaxone activity + Pseudomonas coverage
Lexi-Comp.Micromedex

Cephalosporins• Cefepime (4th generation)
– Dosing:• Mild to moderate infections (UTI, SSSI): 50 mg/kg/dose IV Q12H• Severe infections (meningitis, febrile neutropenia, CF exacerbation):
50 mg/kg/dose IV Q8H
– Adverse effects/toxicities:• Dermatologic: pruritis/rash• GI: diarrhea
Lexi-Comp.Micromedex

Penicillins• Ampicillin
– Mechanism of action: inhibits bacterial cell wall synthesis by binding to penicillin-binding proteins which inhibits the final transpeptidation step of peptidoglycan synthesis in bacterial cell walls
– Spectrum of activity: streptococci, pneumococci, enterococci, nonpenicillinase-producing staphylococci, Listeria, meningococci; some H. flu, P. mirabilis, Salmonella, Shigella, E. coli, Enterobacter, Klebsiella
Lexi-Comp.Micromedex
Penicillins• Ampicillin– Dosing (utilize higher dosing at KCH due to resistance in area)• 100 mg/kg IV Q6H
– Adverse effects/toxicities:• Dermatologic: rash• GI: diarrhea
Lexi-Comp.Micromedex

Vancomycin• Vancomycin
– Mechanism of action: inhibits bacterial cell wall synthesis by blocking glycopeptide polymerization through binding tightly to D-alanyl-D-alanine portion of cell wall precursor
– Spectrum of activity: streptococci, staphylococci (including methicillin-resistant S. aureus, or beta-lactam resistant coagulase negative Staphylococcus.
NO GRAM NEGATIVE ORGANISMS!
Lexi-Comp.Micromedex
Vancomycin• Vancomycin
– Dosing: 20 mg/kg/dose IV Q6-8H (frequency depends on target trough levels)– Monitoring: serum vancomycin trough levels
• Goal 10-20 mcg/mL: bacteremia, skin-soft tissue infection/cellulitis• Goal 15-20 mcg/mL: pneumonia, osteomyelitis, meningitis, MRSA MIC >2
– Adverse effects/toxicities:• CNS: chills, drug fever• Dermatologic: erythematous rash on face and upper body (red man
syndrome)• Renal: nephrotoxicity
Lexi-Comp.Micromedex

Linezolid• Linezolid
– Mechanism of action: inhibits bacterial protein synthesis by binding to bacterial 23S ribosomal RNA of the 50S subunit preventing the formation of a functional 70S complex required for bacterial translation process
– Spectrum of activity: Streptococcus pneumonia, Staphylococcus aureus, Coagulase negative Staph, Enterococcus faecium, Enterococcus faecalis*including multi-drug resistant S. pneumo, methicillin- resistant S. aureus, and vancomycin-resistant Enterococcus
Lexi-Comp.Micromedexhttp://www.antibiotics-info.org/linezolid.html

Linezolid• Linezolid
– Dosing:• <12 years of age: 10 mg/kg/dose IV or PO Q8H• > 12 years: 10 mg/kg/dose IV or PO Q12H
– Adverse effects/toxicities:• GI: diarrhea, nausea, vomiting• Neurologic: headache• Hematologic (less common): myelosuppression,
thrombocytopenia– Serotonin syndrome?
Lexi-Comp.Micromedex

Antimicrobial Summary Mechanism of Action
(Linezolid)
Antimicrobial Clinical Pearls• Antimicrobial stewardship
– Broad spectrum antibiotics…• PCN allergy
– Current data suggest true rate of penicillin-cephalosporin cross-reactivity is less than 1%• Renal dysfunction or hepatic dysfunction
– Lexi-Comp– Renal dosing handbook (https://kdpnet.kdp.louisville.edu/)
• Vancomycin and MIC– For S. aureus infections with MIC of > 2: goal vancomycin trough 15-20 mcg/mL;
consider transition to linezolid
Lexi-Comp.MicromedexHerbert, ME et al. West J Med. 2000Liu, C et al. Clinical Infectious Diseases. 2011
Antimicrobial Clinical Pearls• Other medication pearls to consider:
– Rifampin: increased sedation requirements– Cefdinir: reddish-colored stools– Ciprofloxacin: suspension clogs g-tube– Meropenem and valproic acid: concurrent use is NOT
recommended; consider alternative antibiotic OR add additional anti-seizure medication
– Avoid use of ceftriaxone/sulfonamides in neonates– Fluoroquinolones/TCN are not contraindicated if indication is
correct
Lexi-Comp.Micromedex
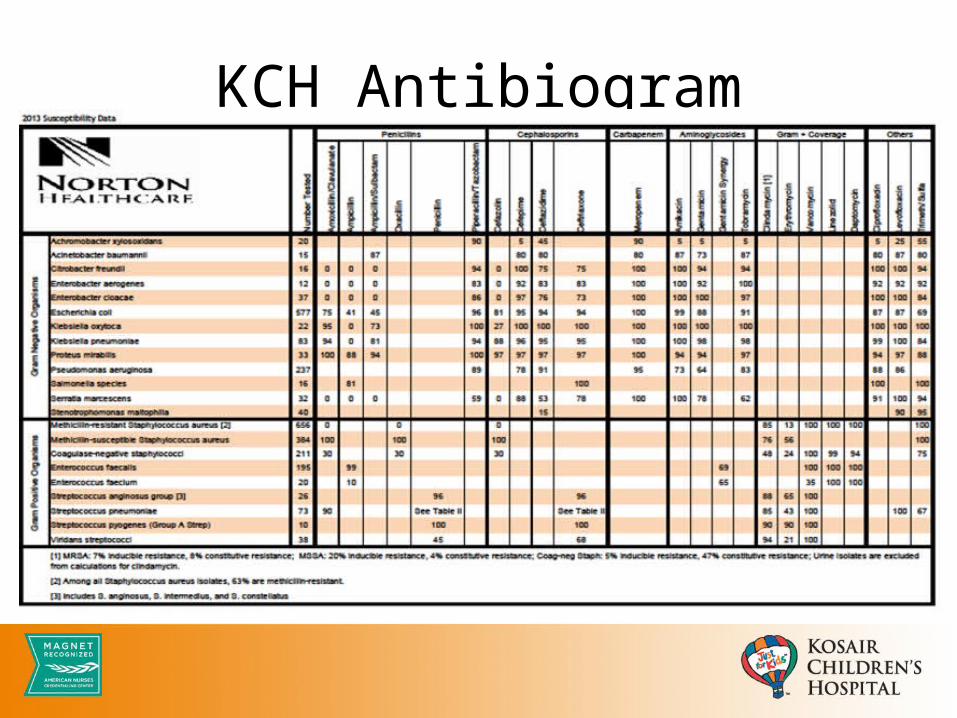
KCH Antibiogram

Patient Case5 week old male (term) presenting with fever and poor feeding noted at home. What drug combination is proper for empiric coverage for meningitis evaluation?
a. vancomycin and cefotaximeb. ampicillin and ceftriaxonec. ampicillin and gentamicind. vancomycin and ceftriaxone

Patient Case7 year old chronically ill female presents after referral from ED due to urine culture which resulted positive for budding yeast (3 days after discharged home on cefdinir). The patient continues to have fever and pain during urination. What is the appropriate empiric regimen for treatment?
a. voriconazoleb. fluconazolec. amphotericin Bd. flucytosine

Antimicrobials in the Pediatric ICU
February 24, 2015Ashley Casper, Pharm.D.


















