Anticipatory Care Planning – what does it offer? · Anticipatory Care Planning – what does it...
14
Anticipatory Care Planning – what does it offer? Karen J Hogg Glasgow Royal Infirmary & Golden Jubilee National Hospital
Transcript of Anticipatory Care Planning – what does it offer? · Anticipatory Care Planning – what does it...
Anticipatory Care Planning – what does it offer?
Karen J Hogg
Glasgow Royal Infirmary & Golden Jubilee National Hospital
Karen
Stamp
What is anticipatory care planning?
• Process designed to support patients living with a chronic long-term condition to help plan for an expected change at some time in the future
• Voluntary progressive process of discussion
– Patient at a time where they have capacity to make healthcare decisions, family, and healthcare providers
• Patient held and led document – Prompt patients and clinicians to “think ahead” – Details patients’ current & future priorities of care
• Not legally binding – Can result in legal documentation
• DNACPR • Wills • Power of attorney
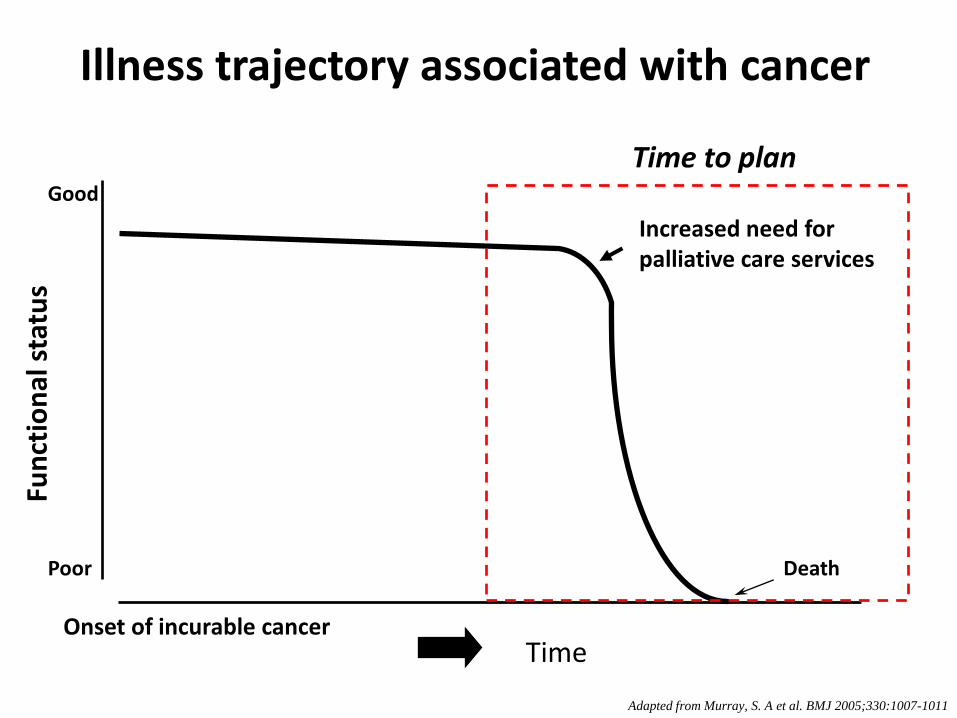
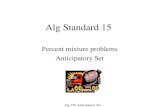
Time Onset of incurable cancer
Illness trajectory associated with cancer F
un
ctio
nal
sta
tus
Death
Good
Poor
Cancer Increased need for palliative care services
Adapted from Murray, S. A et al. BMJ 2005;330:1007-1011
Time to plan
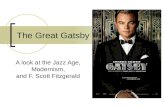
Time
Fu
nct
ion
al
statu
s
Death
Good
Poor
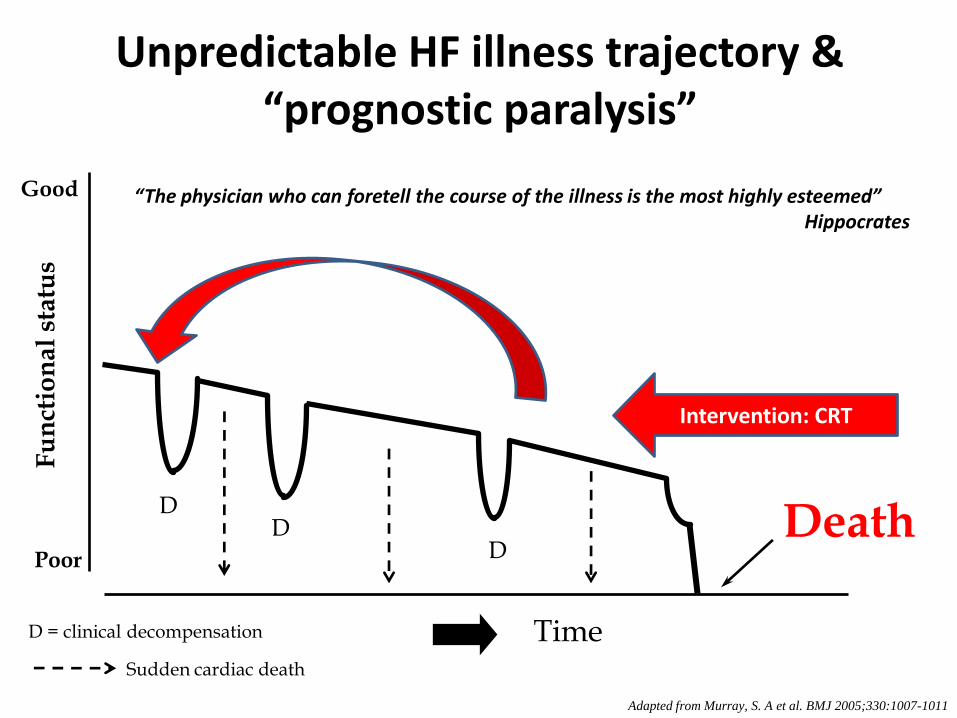
Heart Failure
Unpredictable HF illness trajectory & “prognostic paralysis”
D D
D
D = clinical decompensation
Sudden cardiac death
Adapted from Murray, S. A et al. BMJ 2005;330:1007-1011
Intervention: CRT
“The physician who can foretell the course of the illness is the most highly esteemed” Hippocrates
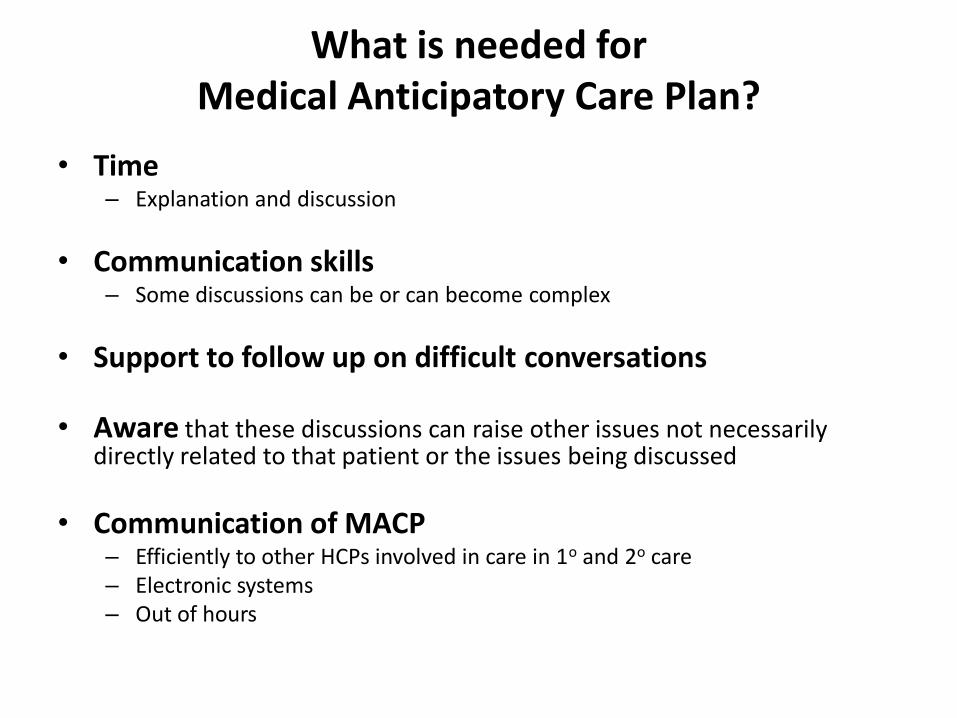
What is needed for Medical Anticipatory Care Plan?
• Time – Explanation and discussion
• Communication skills – Some discussions can be or can become complex
• Support to follow up on difficult conversations
• Aware that these discussions can raise other issues not necessarily directly related to that patient or the issues being discussed
• Communication of MACP – Efficiently to other HCPs involved in care in 1o and 2o care – Electronic systems – Out of hours
Who should complete the Medical Anticipatory Care Plan?
• Healthcare professional – Relationship with the patient to facilitate the
appropriate conversations
– Who knows most about their condition
• May need to involve others where there are multiple co-morbidities or specific circumstances
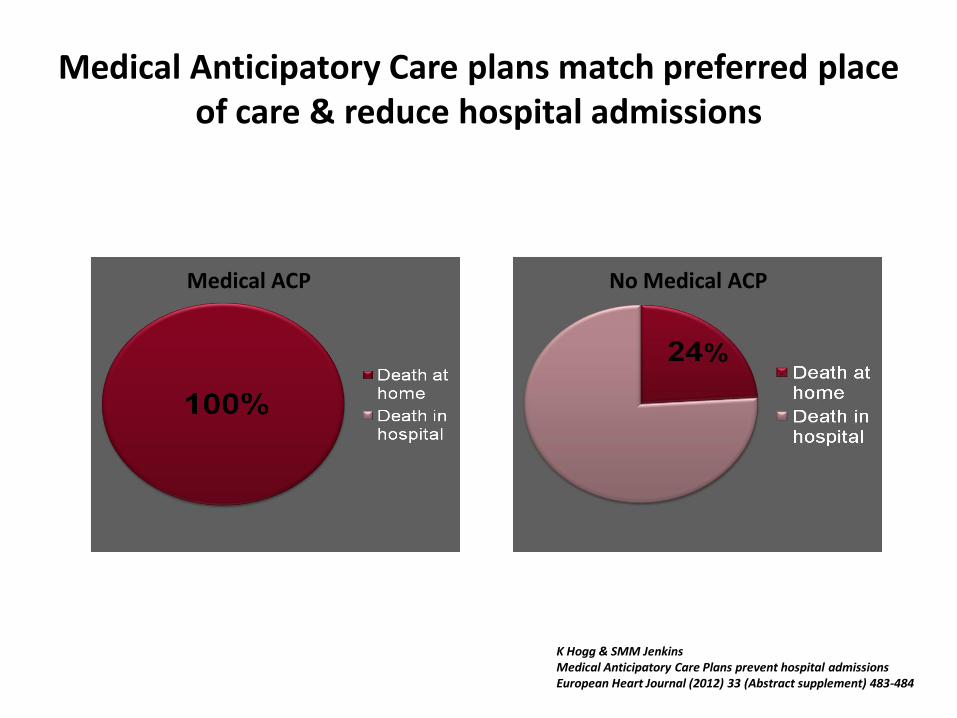
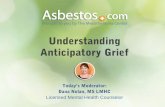
Medical Anticipatory Care plans match preferred place of care & reduce hospital admissions
K Hogg & SMM Jenkins Medical Anticipatory Care Plans prevent hospital admissions European Heart Journal (2012) 33 (Abstract supplement) 483-484
Medical ACP No Medical ACP
Medical Anticipatory Care Plan in Practice
• 70yr old male – Chronic heart failure with severe LVSD (QRSd 118ms) – Secondary prevention ICD – Multiple co-morbidities (DM, Arthritis, COPD, CKD, AF, anaemia)
• 5 Admissions over 6 months various reasons (86 bed days)
– Pulmonary oedema & ascites – Painful cellulitic legs 2o peripheral oedema – Appropriate discharge from defibrillator – Acute on chronic renal impairment – Falls secondary to postural hypotension
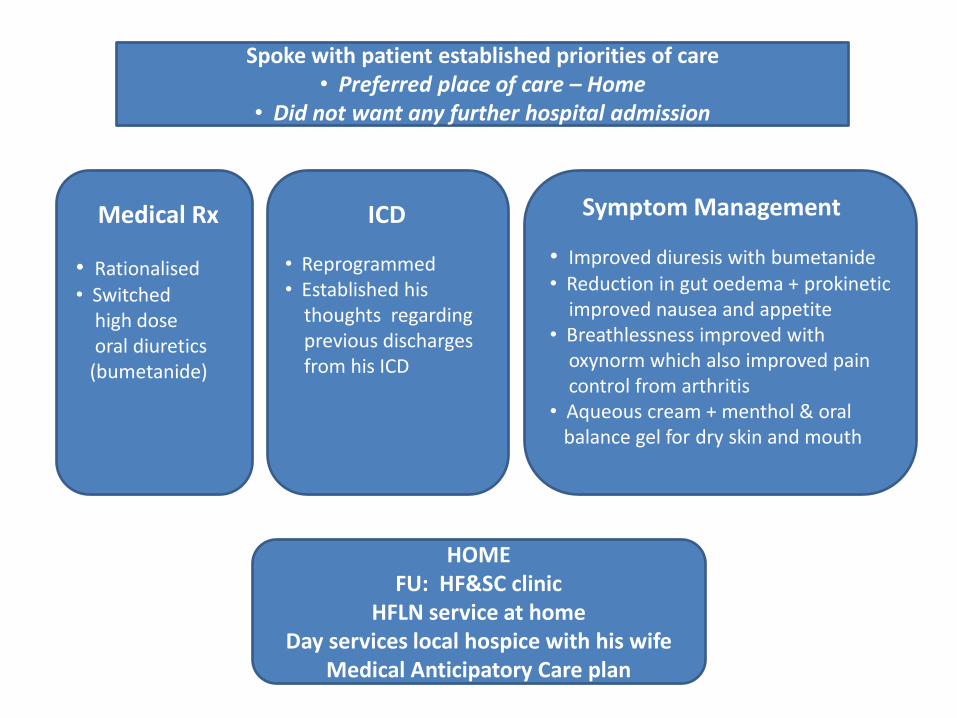
Spoke with patient established priorities of care • Preferred place of care – Home
• Did not want any further hospital admission
• Rationalised • Switched high dose oral diuretics (bumetanide)
• Improved diuresis with bumetanide • Reduction in gut oedema + prokinetic improved nausea and appetite • Breathlessness improved with oxynorm which also improved pain control from arthritis • Aqueous cream + menthol & oral balance gel for dry skin and mouth
HOME FU: HF&SC clinic
HFLN service at home Day services local hospice with his wife
Medical Anticipatory Care plan
ICD Symptom Management Medical Rx
• Reprogrammed • Established his thoughts regarding previous discharges from his ICD

Outcome
• 4 months following discharge from hospital – Primarily home care with help of GP/DN and HFLN
service guided by medical ACP – Attended HF&SC clinic at GRI
• Optimised heart failure medication • Managed cardiac & non-cardiac symptoms • Ongoing discussions re timing of device deactivation • Made alterations to MACP
– Attended and benefited from day services at local hospice
– No hospital admissions – No discharges from ICD
Outcome
• 5 months following discharge from hospital
– Losing weight & developing cahexia
– Increasing symptom burden
– Spending more time in bed
– ICD was deactivated electively as planned
– Developed resistant painful ascites despite high dose oral diuretics
– Short admission to local hospice to allow for some ascitic fluid to be drained to relieve symptoms
Outcome
• 6.5 months following discharge from hospital (Hospital bed days = 0) – Died comfortably at home with family supported by
HFLN service, community palliative care and GP
– No further hospital admissions
– No further discharges from device
– Death was not a surprise and the family felt supported
– GP provided bereavement care
– Wife continued to attend local hospice for support for several months following his death
Karen
Stamp