
Antibiotic Resistance in Long Term Care Facilities: existing and upcoming challenges Robert A....
34
Antibiotic Resistance in Long Term Care Facilities: existing and upcoming challenges Robert A. Bonomo, MD VISN 10 GRECC VAMC Cleveland, Ohio Professor of Medicine, Case Western Reserve University School of Medicine
-
Upload
bertram-melton -
Category
Documents
-
view
213 -
download
0
Transcript of Antibiotic Resistance in Long Term Care Facilities: existing and upcoming challenges Robert A....
Antibiotic Resistance in Long Term Care Facilities: existing
and upcoming challenges
Robert A. Bonomo, MD
VISN 10 GRECC
VAMC Cleveland, Ohio
Professor of Medicine,
Case Western Reserve University School of Medicine

Objectives
• Describe the demographics of a global aging population and the burden of infection
• Describe the Immunology of Aging and its role in Infection
• Understand the role of LTCF and reservoirs of resistance; impact of resistant infections; transmission dynamics
• Discuss the existing and upcoming challenges; can we understand this and can we mount an effective response ?

Demographic ImperativeDemographic Imperative

Introduction
• By 2030, the population > 65 yo will 2x and > 85 yo will 3x
• Aging and functional limitations increase with each ensuing decade.
• More than 40% of elderly will spend at least some time in a LTCF.
Capitano and Nicolau, JAMDA, 2003; Strausbaugh and Joseph, 2000, ICHE
The challenge of infections in the elderly-I
• Mean age of residents with ID syndromes is > 80 years.
• Risk is 32.7% ; 4-10 infections per 1000 patient days; 1 infection per year (1 course of antibiotics)
• Up to 40% mortality with certain infections admitted to hospital
The challenge of infections in the elderly-II
• Unique living situations exist among the elderly (socialization)
• Functional outcomes change with age and underlying diseases
– DM
– Ca
– Frailty : Dementia, instability, falls, CVA and swallowing, BPH and E2 depletion

Common Infections in the elderly-I
• Pneumonia – CAP-pneumococcal– NH or HCAP – aspiration – Influenza, RSV, other viruses
• UTI-catheter
• Skin and soft tissue infections – VZV and pressure ulcers

Common Infections in the elderly-II
• Gastrointestinnal: Intra abdominal abscess– Cholecystitis, diverticulitis, appendicitis, – C. difficile colitis (a)symptomatic
• Endocarditis
• Meningitis not pneumococcal!!
• Tuberculosis
• Sepsis –the most feared! CV resiliency

“New Infections” in the Elderly
• HIV : one in eleven cases of HIV is reported in patients older than 50 (Ohio is 1 in 10)
• HCV ; STDs
• Surgical infections (vascular revisions)
• Travel associated infections
• WNV
CDC JAMA 1998 279 575-576
WHAT HAPPENS TO THE IMMUNE SYSTEM WITH
ADVANCED AGE?
WHAT HAPPENS TO THE IMMUNE SYSTEM WITH
ADVANCED AGE?

Immunology of Aging
• Elderly individuals are the largest group of “immuno-compromised” patients that physicians are asked to treat
• Immunology of aging is still poorly understood
High KP. CID 2003 37 196-200

Immunosenescence-I
• Impairments of adaptive and innate immunity; T and B lymphocytes? – cellular immune responses and antibody
production– surface expression or function of toll like
receptor (TLR1/2) that may relate to increased risk of disease due to specific pathogens (Listeria, Mtb, VZV) and impaired response to ag challenge

Immunosenescence-II
increase age, increase IL-6- multifunctional cytokine- mediator of the acute phase response (chronic inflammation)
decreased IL-2 and soluble IL-2 receptor
decreased interferon
increased IL-4 and -1
increased TNF
LTCFs AS RESEVOIRS of
RESISTANCE; IMPACT OF RESISTANT
INFECTIONS
LTCFs AS RESEVOIRS of
RESISTANCE; IMPACT OF RESISTANT
INFECTIONS

LTCFs as “reservoirs of resistance”-I
• Since 1975, reports identified ATBR pathogens in LTCFs:
– MRSA , MRSE, VRE, PRP
– Mupirocin resistance
– TMP/SMX resistant GNRs
– AGR enterococci and Gram negatives
Shlaes et al; 1986 Loeb et al., American Journal of Epidemiology, 157, 2003; Weiner et al. JAMA 1999, 281, 517-523; Terpenning et al
LTCFs as “reservoirs of resistance”-I
– Quinolone resistant P. aeruginosa
– Amox/clav R E. coli*
– TAZ R E. coli , K. pneumoniae
• ESBLs of the TEM (TEM-12, -26), SHV (SHV-7) varieties
• plasmid borne AmpCs
• Non TEM, non SHV ESBLs
Bonomo et al JAGS, Bonomo et al, Clin Lab Med. 2004 , Rice et al, AAC, 1990; Bradford 1995, AAC,
Neuhauser, JAMA, 2003, Pitout, et al, Shlaes et al,

Resistant GPCs in LTCFs
• Rates of colonization and infection range from 25-50% and 3 % of residents colonized, get infected.
• Colonization by MRSA is often a hallmark of significant short-term disability. In a study by Niclaes et al., the RR of dying within 6 months was greater for MRSA carriers than that for non-carriers
Bradley SF,. Ann Intern Med 1991; Niclase, 1999 EI

CeftazidimeR in LTCFs
• The 1st outbreak of ESBLs in the US occurred in a LTCF in Ma. in 1990 (TEM-26 and TEM-12);
• SHV-7 from E. coli UTI from LTCF in NY• Outbreak in Cleveland (TEM-6)• In a study of ceftazidime-resistant E. coli
and K. pneumoniae in Chicago, 31 of 35 patients from 8 nursing facilities harbored an ESBL-producing enteric pathogen.
Rice AAC 1990, Bradford AAC 1995, Rice CID 1996, Weiner JAMA 1999
Cefotaxime-Resistant Bacteria Colonizing Older People
Admitted to an Acute Care Hospital
• Of the 190 surveillance cultures obtained from 143 patients, 26 cefotaxime-resistant gram-negative isolates from 22 patients were recovered.
• The prevalence rate of cefotaxime-resistant isolates on admission was 13.3% (19/143).
• A logistic regression model using cefotaxime colonization as the dependent variable found that multiple co-morbidities, admission to a surgical service, and having a diagnosis of infection on presentation and a transfusion history were factors associated with the presence of colonization. These four clinical items accurately classified 74% of patients colonized.
Bonomo 2003 JAGS
• ATB use and NH residence were not associated with the presence of colonization by cefotaxime-resistant organisms.
• CONCLUSION: These data raise awareness that there are community- and LTCF-dwelling older patients colonized with gram-negative enteric bacilli resistant to third-generation cephalosporins on admission to the hospital. The "reservoir of resistant bacteria" in older people is no longer confined to LTCFs.
CTX GNRs Colonizing Older People Admitted to an Acute
Care Hospital
Bonomo 2003 JAGS
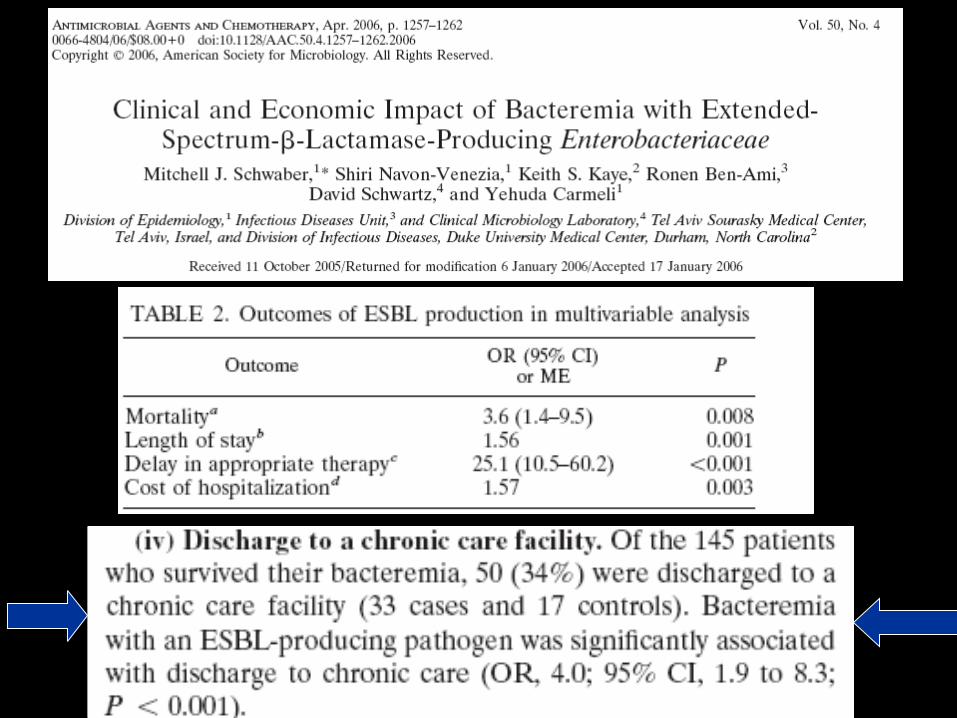
Spread of E. coli with high levels of cefotaxime resistance between
community, LTCF and Hospital institutions
• Prospective surveillance study; 151 E. coli isolates resistant to taz and tax
• 3 hospitals, 8 LTCFs, and day care center• Co resistance to cipro, gent, tobra, cefepime, a/c and
tmp/smx• CTX-M-15, -14, -32; linked to ISEcp1 and IS26 elements• Other clusters of mobile resistance genes (tetA, aac6’1b,
dfrA, sul, aac3IIb; virulence genes• The greatest cluster of isolates were from UTIs in
elderly adults
Oteo et al, JCM, 2006

Spread of K. pneumoniae strain producing a plasmid mediated ACC-1 AmpC beta-lactamase in a teaching
hospital admitting debilitated patients
• 57 cases acquired from a 26 yo patient with tetraplegia with a Kp UTI bearing blaAAC-1
• PMR and other departments; 28 days to acquire the pathogen
• First report of plasmid mediated AmpC outbreak
Ohana AAC 2005
Why AtbR pathogens are found in the elderly LTCFs?
• Transfer of Patients from tertiary and quaternary Care institutions; lapses in IC
• Excess use of broad spectrum antibiotics that select for resistant strains
• Risk factors associated with recovery of resistant strains (percutaneous endoscopic gastrostomy feeding tubes, pressure ulcers, malnutrition, immunosuppression [age- and medication-related], prior antibiotic use)
• Cycle of institutionalization and hospitalization
Bonomo CID, 2000

Hospital
CommunityLTCF
***LTAC***PM&R
DAYCARE
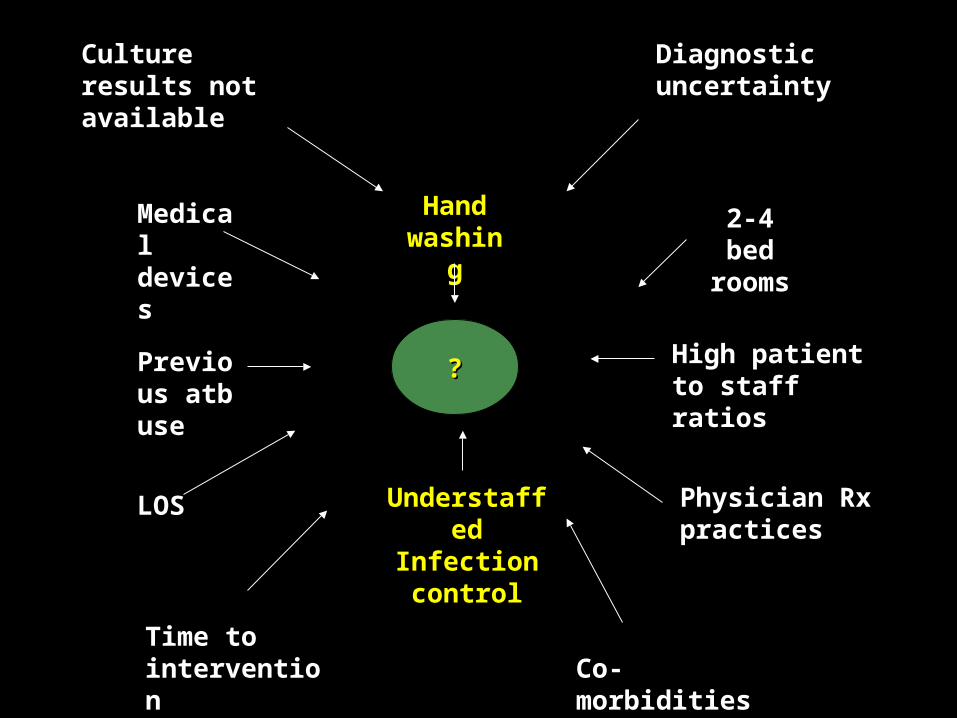
??
Medical devices
Previous atb use
LOS
2-4 bed rooms
High patient to staff ratios
Hand washing
Understaffed Infection control
Physician Rx practices
Culture results not available
Diagnostic uncertainty
Co-morbiditiesTime to intervention


Barrier precautions?
• Do they really work? We are learning from the recent flu epidemic that there is significant controversy regarding their use
• Intensity of barrier precautions, isolation or cohorting, or environmental cleaning does not decrease the likelihood of transmission of MRSA or VRE.
Barrier precautions?
• Additional precautions are recommended for patients colonized with these microorganisms only when the patients are a documented source of transmission to other patients (e.g., MRSA patients with extensive skin lesions that cannot be covered or VRE patients with diarrhea and incontinence)

Unresolved Questions!
• What is freq of cross transmission?
• Is there evolution from previously susceptible organisms?
• If cross transmission, best methods to limit horizontal spread? Targeted or generalized surveillance ? Identify unrecognized reservoirs?
• If evolution, antibiotic restriction policies?

Personal comment
From an analysis of this data it is clear that atbR in LTCFs approach prevalence
rates comparable to ICU!!
Therefore, the clinical and economic impact of infections due to MRSA and
MDR GNRs is substantial and will present one of the greatest challenges
to the institutionalized elderly .
Critical Questions
• Should we continue to rely on empirical antibiotic treatment in LTCF residents, given limited diagnostic capabilities vs. increasing antibiotic resistance (MRSA, C. difficile, VRE)?
• How do we approach, manage and control infectious disease outbreaks in LTCFs?
Opportunities in LTCFs
Deficiencies in ID in LTCFs
1. Transmission of infections (Infection Control)
2. What makes physicians use antibiotics?
3. How much resistance is present and what is the origin?
4. Antibiotic (mis)use
Opportunities and challenges
1. Infection control programs directed to LTCFs
2. Physicians trained in ID in LTCFS (recognition)
3. Regional programs characterizing resistance
4. Programs to optimize antibiotic use in LTCFs
We have implemented a new program to provide on site education and service to geriatricians in our affiliated program to answer some of these needs

Contact
• For questions about this audio conference please contact Dr. Robert Bonomo at [email protected]
• For any questions about the monthly GRECC Audio Conference Series please contact Tim Foley at [email protected] or call (734) 222-4328
• To evaluate this conference for CE credit please obtain a ‘Satellite Registration’ form and a ‘Faculty Evaluation’ form from the Satellite Coordinator at you facility. The forms must be mailed to EES within 2 weeks of the broadcast


















