Antibiotic and Anti-Inflammatory Therapies for Cystic...
18
Antibiotic and Anti-Inflammatory Therapies for Cystic Fibrosis James F. Chmiel 1 , Michael W. Konstan 1 , and J. Stuart Elborn 2 1 Department of Pediatrics, Case Western Reserve University School of Medicine, Rainbow Babies and Children’s Hospital, Cleveland, Ohio 44106 2 Medicine and Surgery, Queens University Belfast, Belfast City Hospital, Belfast BT9 7AB, Northern Ireland, United Kingdom Correspondence: [email protected] Cystic fibrosis (CF) lung disease is characterized by chronic bacterial infection and an unre- mitting inflammatory response, which are responsible for most of CF morbidityand mortality. The median expected survival has increased from ,6 mo in 1940 to .38 yr now. This dramatic improvement, although not great enough, is due to the development of therapies directed at secondary disease pathologies, especially antibiotics. The importance of devel- oping treatments directed against the vigorous inflammatory response was realized in the 1990s. New therapies directed toward the basic defect are now visible on the horizon. However, the impact of these drugs on downstream pathological consequences is unknown. It is likely that antibiotics and anti-inflammatory drugs will remain an important part of the maintenance regimen for CF in the foreseeable future. Current and future antibiotic and anti- inflammatory therapies for CF are reviewed. A lthough cystic fibrosis (CF) impacts many organ systems, lung disease accounts for most of the morbidity and mortality (Davis et al. 1996). Abnormal or insufficient cystic fi- brosis transmembrane conductance regulator (CFTR) leads from the defective gene and pro- tein to an abnormal surface environment to a vicious cycle of obstruction, chronic infection, and inflammation (Chmiel et al. 2002a). Reliev- ing obstruction with mucolytics and airway clearance, controlling infection with antibiotics, and reducing inflammation with anti-inflam- matory drugs have been the cornerstones of a comprehensive pulmonary treatment program in CF. INFECTION AND INFLAMMATION IN THE CF AIRWAY CF airways are most susceptible to chronic in- fection with Staphylococcus aureus, Hemophilus influenzae, Pseudomonas aeruginosa, Burkhol- deria cepacia complex organisms, Stenotropho- monas maltophilia, and Achromobacter xylosox- idans. Most of these microbes form biofilms, thus serving as persistent inflammatory stimuli (Chmiel and Davis 2003). When local host de- fense mechanisms are challenged by intercurrent viral or bacterial infections, massive numbers of neutrophils are recruited into the airway. Al- though inflammation is meant to eradicate in- fection, this ultimately fails, and the exaggerated Editors: John R. Riordan, Richard C. Boucher, and Paul M. Quinton Additional Perspectives on Cystic Fibrosis available at www.perspectivesinmedicine.org Copyright # 2013 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a009779 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 1 www.perspectivesinmedicine.org Press on December 18, 2020 - Published by Cold Spring Harbor Laboratory http://perspectivesinmedicine.cshlp.org/ Downloaded from
Transcript of Antibiotic and Anti-Inflammatory Therapies for Cystic...

Antibiotic and Anti-Inflammatory Therapiesfor Cystic Fibrosis
James F. Chmiel1, Michael W. Konstan1, and J. Stuart Elborn2
1Department of Pediatrics, Case Western Reserve University School of Medicine, Rainbow Babiesand Children’s Hospital, Cleveland, Ohio 44106
2Medicine and Surgery, Queens University Belfast, Belfast City Hospital, Belfast BT9 7AB,Northern Ireland, United Kingdom
Correspondence: [email protected]
Cystic fibrosis (CF) lung disease is characterized by chronic bacterial infection and an unre-mitting inflammatory response, which are responsible for most of CF morbidityand mortality.The median expected survival has increased from ,6 mo in 1940 to .38 yr now. Thisdramatic improvement, although not great enough, is due to the development of therapiesdirected at secondary disease pathologies, especially antibiotics. The importance of devel-oping treatments directed against the vigorous inflammatory response was realized in the1990s. New therapies directed toward the basic defect are now visible on the horizon.However, the impact of these drugs on downstream pathological consequences is unknown.It is likely that antibiotics and anti-inflammatory drugs will remain an important part of themaintenance regimen for CF in the foreseeable future. Current and future antibiotic and anti-inflammatory therapies for CF are reviewed.
Although cystic fibrosis (CF) impacts manyorgan systems, lung disease accounts for
most of the morbidity and mortality (Daviset al. 1996). Abnormal or insufficient cystic fi-brosis transmembrane conductance regulator(CFTR) leads from the defective gene and pro-tein to an abnormal surface environment to avicious cycle of obstruction, chronic infection,and inflammation (Chmiel et al. 2002a). Reliev-ing obstruction with mucolytics and airwayclearance, controlling infection with antibiotics,and reducing inflammation with anti-inflam-matory drugs have been the cornerstones of acomprehensive pulmonary treatment programin CF.
INFECTION AND INFLAMMATIONIN THE CF AIRWAYCF airways are most susceptible to chronic in-fection with Staphylococcus aureus, Hemophilusinfluenzae, Pseudomonas aeruginosa, Burkhol-deria cepacia complex organisms, Stenotropho-monas maltophilia, and Achromobacter xylosox-idans. Most of these microbes form biofilms,thus serving as persistent inflammatory stimuli(Chmiel and Davis 2003). When local host de-fense mechanisms are challenged by intercurrentviral or bacterial infections, massive numbers ofneutrophils are recruited into the airway. Al-though inflammation is meant to eradicate in-fection, this ultimately fails, and the exaggerated
Editors: John R. Riordan, Richard C. Boucher, and Paul M. Quinton
Additional Perspectives on Cystic Fibrosis available at www.perspectivesinmedicine.org
Copyright # 2013 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a009779
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

inflammatory response that ensues is responsi-ble for much of the lung’s pathology.
The CF inflammatory response begins earlyin life, becomes persistent, and is often excessiverelative to the burden of infection. Bronchoal-veolar lavage (BAL) fluid from CF patients, in-cluding infants and patients with mild disease,contains large concentrations of inflammatorymediators and cells, particularly neutrophils(Konstan et al. 1993, 1994; Birrer et al. 1994;Armstrong et al. 1995, 1997; Balough et al. 1995;Bonfield et al. 1995a; Khan et al. 1995; Kirchneret al. 1996). The presence of large concentrationsof inflammatory mediators in the absence of de-tectable pathogens suggests either that the in-flammatory response operates independentlyof infection or that there is failure to terminatethe inflammatory response once the incitingstimulus has been removed (Khan et al. 1995).The inflammatory response could be triggeredby a transient viral or bacterial infection thatthen cannot be stopped. In addition, BAL studiesshow that infected CF infants have more in-flammation than do similarly infected non-CFinfants (Noah et al. 1997; Muhlebach et al. 1999).
Neutrophils, present in massive quantities,release actin, DNA, proinflammatory cytokinesand chemokines, oxidants, and proteases. B cellsand T cells, particularly TH-17 cells, also con-tribute to CF lung disease (Dubin et al. 2007).The continued presence of bacteria triggers anunrelenting inflammatory response that drivesthe persistent generation of proinflammatorymediators including neutrophil chemoattrac-tants IL-8 and LTB4, which recruit more neutro-phils into the airways, fueling the vicious cycleof inflammation that leads to lung destruction(Konstan and Berger 1997; Chmiel et al. 2002a).Because the neutrophil plays a central role in CFairway pathophysiology, any anti-inflammatorydrug developed for CF must, either directly orindirectly, address the neutrophil and its prod-ucts (Table 1).
Airway surface fluid from CF patients con-tains large concentrations of inflammatorymediators including TNF-a, IL-1b, IL-6, IL-8,IL-17, and GM-CSF (Bonfield et al. 1995a;McAllister et al. 2005). The synthesis of thesemediators is promoted by a few transcription
factors including AP-1, NF-kB, and MAPK. Inaddition to a heightened proinflammatory arm,there appears to be inappropriately decreasedcounter-regulatory pathways, particularly thoseinvolving IL-10 and nitric oxide (NO) (Bonfieldet al. 1995b, 1999; Balfour-Lynn et al. 1996;Grasemann et al. 1997). When counter-regula-tory controls are abnormal, an imbalance oc-curs, resulting in prolonged and excessive in-flammatory mediator production. It is possiblethat a combination of these mechanisms fuelsthe destructive inflammatory cascade. It is un-likely that asingle defect in one pathwayaccountsfor the entirety of the exaggerated inflammatoryresponse. Multiple pathways are probably up-regulated (i.e., pathways that activate the inflam-matory response) or down-regulated (i.e., path-ways that terminate the inflammatory response)in response to the cell’s attempt to correct theunderlying physiological abnormality due to ab-normal CFTR. The end result is that the delicatebalance between the pro- and anti-inflammato-ry arms is disrupted, and pathways promotingthe activation and perpetuation of the inflam-matory response are favored. A schematic of theCF airway is seen in Figure 1.
THERAPIES DIRECTED AT BACTERIALINFECTION
The range of microorganisms, particularly bac-teria that have been identified in the CF airway,is much wider than previously appreciated
Table 1. Neutrophil chemoattractants andproducts targeted by anti-inflammatory drugs
I. Neutrophil chemoattractantsA. IL-8B. LTB4
C. Complement components: C5a, C5a-des-ArgD. Bacterial products: N-formyl-Met-Leu-Phe
II. Neutrophil productsA. Proteases (elastase)B. DNAC. Oxidants (H2O2 and O2
2)D. IL-8E. LTB4
J.F. Chmiel et al.
2 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

(Tunney et al. 2008, 2011). Using moleculartechniques, organisms that were previously un-culturable, particularly microaerophilic and an-aerobic bacteria, have been identified (Lipuma2012). The virulence of these organisms andtheir complex interaction as an airway micro-biome has yet to be fully established. However,there are some studies to suggest that the diver-sity or the lack of diversity in sputum and BAL
from people with CF is associated with moresevere and chronic disease, and this may inpart be driven by antibiotic therapy (Tunneyet al. 2011; Zhao et al. 2012)
Antimicrobial therapy in CF has a long his-tory, and effective treatment of infection isthought to be one of the key advances that haveresulted in improved outcomes over the past 50years for people with CF (Doring et al. 2012).
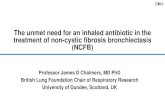
Blood vessel
Bronchiectatic airwayTNF-α, IL-1β, IL-6
IL-8, GM-CSF
IL-6, IL-8, GM-CSFElastaseoxidants
IL-8LTB4
TNF-αIL-1b
IL-17
Key
Activated macrophage
Neutrophil
Lymphocyte (T, B)
Dendritic cell
P. aeruginosa
S. aureus
DNA
Adhesins(selectins, ICAM-1)
Figure 1. Infection and inflammation in the CF lung. CF lung disease is essentially an endobronchial/peribron-chial process. The alveoli do not become involved until late in the disease course. In CF, the gene defect leads toan abnormal airway surface environment and then to airway obstruction with mucus (represented as anamorphous gray area in the center of the airway), chronic bacterial infection, and persistent inflammation.Although there are several different types of bacteria that infect the CF airway, S. aureus predominates early in lifebut typically yields to P. aeruginosa. However, most patients have polymicrobic infections, thus making selectionof appropriate antibiotics for treatment of a pulmonary exacerbation difficult. The bacterial infection is asso-ciated with a vigorous inflammatory response that is characterized by a large neutrophilic infiltration. Otherinflammatory cells are also involved in the inflammatory response including epithelial cells, macrophages,dendritic cells, B lymphocytes, and T lymphocytes. These cells release many inflammatory cytokines andmediators that further promote the inflammatory response. The inflammatory response is ineffectual in elim-inating bacteria from the airway, but the excess inflammatory mediators released into the endobronchial andperibronchial spaces damage the airway wall architecture and ultimately lead to bronchiectasis. This figurefocuses on the proinflammatory aspects of CF airway inflammation. The abnormalities in the counter-regula-tory mechanisms in CF are not depicted.
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

S. aureus was identified in 1949 as the predomi-nant pathogen in cultures taken from youngchildren with CF. Subsequently, P. aeruginosawas identified as an organism associated withbronchiectasis and chronicity. From the late1950s, P. aeruginosa was reported with increas-ing frequency from children with CF, and themucoid phenotype for P. aeruginosa was firstdescribed in 1966 (J Littlewood; www.cfmedi-cine.com). Specific antimicrobial therapy in CFhas, therefore, been directed against these or-ganisms. Over the subsequent decades, a rangeof other dominant organisms has presentedchallenges for antibiotic therapy. These includemembers of the B. cepacia complex, S. malto-philia, Achromobacter species, and other Gram-negative infections. Nontuberculous mycobac-terial infection is also emerging as a new chal-lenge for antibiotic treatment for people withCF.
ANTIBIOTIC PROPHYLAXIS
The presence of S. aureus in airway secretionsfrom people with CF prompted early cliniciansto consider the use of prophylactic antibiotics toprevent and control Staphylococcal infection inthe early years (Smyth and Walters 2012). Thistype of treatment has been and, in some coun-tries, remains controversial. In some small stud-ies, prophylactic treatment from diagnosis withflucloxacillin has been associated with a reduc-tion in the frequency of positive Staphylococcalairway sample cultures and a reduction in ad-mission to hospital, but no long-term improve-ments have been shown in lung function. Theseobservations were followed up with a clinicaltrial of cephalexin, a more broad-spectrum an-tibiotic, which did not show any efficacy. But inpatients treated with long-term prophylaxis,there was an increase in the frequency of newinfections with P. aeruginosa.
These observations have been supportedby several registry studies. In a recent updatedCochrane Review, a meta-analysis of four studiesincluding 401 patients under the age of sevenwas reported (Smyth and Walters 2012). In thisanalysis, no significant increase in the numberof isolates of P. aeruginosa was shown between
treated and untreated groups from reportedstudies, although there was a trend toward alower cumulative isolation rate of P. aeruginosain the patients treated with long-term antibiot-ics at 2–3 yr and a higher isolation rate from 4to 6 yr. These studies used a range of antibioticsincluding flucloxacillin, co-trimoxazole, cefa-droxil, and cephalexin. It is unclear what theclinical benefits of simply reducing the frequen-cy of culture of S. aureus might be.
Antibiotic Therapy for S. aureus
S. aureus is avery common infecting organism inpeople with CF. This is most commonly methi-cillin-sensitive S. aureus (MSSA), but methicil-lin-resistant S. aureus (MRSA) is becoming in-creasingly common in the sputum of peoplewith CF. The increased incidence of MRSA in-fection in people with CF is particularly con-cerning because it is associated with a more rap-id rate of decline in lung function and worsesurvival (Dasenbrook et al. 2008, 2010). Wheneither MSSA or MRSA is identified in sputum, itmakes sense to attempt eradication. For MSSA,cephalexin, flucloxacillin, co-trimoxazole, and,additionally, in adults, tetracyclines can be usedto do this. MRSA similarly may be eradicatedwith a combination of drugs used by cliniciansincluding vancomycin, linezolid, rifampin, ri-fampicin, fusidic acid, tetracycline, and co-trimoxazole-based regimes. Several studies arecurrently trying to determine the best regimeto treat this organism. Similarly, antibiotic ap-proaches can be used to treat exacerbations inindividuals who are chronically infected withthis organism.
ANTIBIOTIC THERAPY FOR INFECTIONWITH P. aeruginosa ERADICATIONTHERAPY
In contrast to the debate around antibioticprophylaxis for S. aureus, there is currently nodebate for antibiotic prophylaxis against P.aeruginosa in people with CF (Doring et al.2012). There is currently a clinical trial in Europeusing avian immunoglobulin Y antibodies,which are gargled, to explore if this novel inter-
J.F. Chmiel et al.
4 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

vention of treating the oropharynx might pre-vent P. aeruginosa acquisition in the lower air-ways (EUDRACT-2011-000801-39).
There is, however, a compelling rationale forantibiotic eradication therapy for P. aeruginosain CF. This approach was championed by theCopenhagen Centre, who in early studies ofthis intervention using a historical comparativecohort, showed that there was a strong indica-tion that the combination of inhaled colistinand oral ciprofloxacin resulted in approximate-ly an 80% success in P. aeruginosa eradication(Valerius et al. 1991). Subsequent studies, suchas the ELITE and EPIC studies, have shown thatinhaled tobramycin for 4 wk is also an effectiveantibiotic eradication therapy (Ratjen et al.2010; Treggiari et al. 2011). In two small stud-ies, no difference was identified between thesetwo regimes with a comparable eradication rate(Taccetti et al. 2012; Proesmans 2013).
Early intervention is now a recommendedpart of most guidelines for the treatment ofnew or repeated infection with P. aeruginosa(Doring et al. 2012). It is less clear what thebest treatment for failure to eradicate using ei-ther the colistin/ciprofloxacin or inhaled to-bramycin regimes should be. A recent recom-mendation from a consensus group was thatafter two attempts at eradication using inhaledand oral therapy, intravenous antipseudomo-nal antibiotics should be considered. A clinicaltrial (Torpedo; www.torpedo-cf.org.uk/index.html) comparing colistin/ciprofloxacin and in-travenous antibiotics is currently under way inthe United Kingdom.
Treatment of Chronic P. aeruginosa Infection
In �75% of people with CF, P. aeruginosa even-tually cannot be eradicated and chronic infec-tion ensues (Doring et al. 2012). When thisoccurs, the bacteria frequently have a mucoidphenotype and exist in a biofilm. This and otherimportant adaptions reduce the effectiveness ofinnate host defense and make treatment withantibiotics less effective (Williams and Davies2012). When chronic infection has developed,treatment with long-term aerosolized antibiot-ics is an important and effective intervention.
Tobramycin (TOBI, Bramitob) and aztreonamlysine (Cayston) are approved therapies bymost regulators throughout the world. Both ofthese treatments have shown superiority overplacebo for measurements of lung function,quality of life, and reduction in pulmonaryexacerbations (Doring et al. 2012). Colistin isalso used in chronic suppressive therapy in itsnebulized form. Tobramycin and colistin haverecently been developed into dry-powder in-haled antibiotics. Tobramycin inhalation pow-der (TobiPodhaler) is approved by the EMAand also is under review by the FDA, and colis-tin inhalation powder (Colobreathe) has beenapproved by the EMA for treatment (Konstanet al. 2011; Schuster et al. 2012). Both of thesedrugs have shown noninferiority for key clinicaloutcomes to tobramycin delivered by nebulizer,and have increased cough as a common sideeffect.
In general, inhaled antipseudomonal anti-biotics decrease bacterial burden (measured inCFU/g of sputum), improve lung functionand quality of life, and reduce the frequency ofpulmonary exacerbations (Doring et al. 2012).Colistin is given every day, whereas tobramy-cin is licensed for administration as an alter-nate-month therapy. Many patients describeincreased symptoms and reduced FEV1 duringthe month off tobramycin. Therefore, manypatients cycle between two different inhaled an-tibiotics. The optimal regime for aerosolizedantibiotic therapy as long-term suppressivetherapy has yet to be determined. It is unlikelythat a randomized controlled trial will allow anyfurther direct comparisons between regimes oranswer the challenging question of whethercontinuous nebulized antibiotics using alter-nate regimes, for example, alternating tobramy-cin, aztreonam lysine, and colistin, would besuperior to the current recommended month-off month-on regimes.
Several other inhaled antibiotic therapiesagainst P. aeruginosa are in development. Twoformulations of levofloxacin, ciprofloxacin as adry powder inhaler, and ciprofloxacin and ami-kacin as liposomal formulations are in variousstages of development and may become avail-able in the near future (Doring et al. 2012).
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Treating Exacerbations in Patients withChronic P. aeruginosa Infection
Pulmonary exacerbations (PEs) are significantevents in people with CF. These events are asso-ciated with an increase in pulmonarysymptoms,systemic symptoms including weight loss, some-times newclinical signs, physiological changes inlung function, and often evidence of local andsystemic inflammation. Frequency of pulmo-naryexacerbations is associated with a more rap-id decline in FEV1 and reduced survival (Smythand Elborn 2008; Doring et al. 2012). Preventionof pulmonary exacerbations is, therefore, a keyintervention, and there is good evidence thatlong-term suppressive antibiotic therapy, con-comitant human DNase (Pulmozyme), azithro-mycin, and inhaled hypertonic saline reduce thetime to the next exacerbation in clinical trials,and, by extrapolation, probably reduce the fre-quency of these events in people with CF. Opti-mizing long-term treatment to reduce theseevents and the inflammatory injury impactthey have on the lungs in people with CF is acritically important intervention (Stenbit andFlume 2011).
Optimizing the antibiotic therapy and du-ration of treatment is important in treating pul-monary exacerbations. There is some evidencethat �25% of pulmonary exacerbations resultin a failure to return to baseline lung functionand/or rapid relapse (Sanders et al. 2010; Sten-bit and Flume 2011; Parkins et al. 2012). Selec-tion of antibiotics for treatment of such ex-acerbations is largely empirical. Using currenttechniques to determine in vitro antimicrobialsusceptibility does not appear to improve theoutcomes (Doring et al. 2012). This is a partic-ular problem with P. aeruginosa because withrepeated antibiotic therapy, these organismsdevelop resistance. However, response to anti-biotics does not appear to relate directly to invitro susceptibility as currently determined inmicrobiology laboratories. The choice of ini-tial antibiotics to treat a pulmonary exacerba-tion is often based on antibiotic susceptibilitytesting and is affected by patient tolerability. Ifclinical response is suboptimal, changes in an-tibiotic regimen are often made based on clin-
ical experience irrespective of susceptibilitytesting.
There is a good historical and current ra-tionale for the use of a combination of an ex-tended-action penicillin and an aminoglyco-side. Conventionally, this therapy has been for14 d, although in a recent registry-based study,10 d may be a sufficient period of time for themajority of patients (Van Devanter et al. 2010).However, this approach has not been subjectedto a prospective study.
ANTIBIOTIC TREATMENT FOR OTHERBACTERIAL PATHOGENS IN CF
S. maltophilia and Achromobacter Species
S. maltophilia and Achromobacter species arecommonly isolated in CF sputum, althoughtheir prevalences are variable. Single centershave reported up to 25% prevalence of eitherorganism. The clinical significance of theseorganisms is hard to determine, although it isclear that individual patients with either of thesebacteria as their predominant pathogen canhave progressive deterioration in lung functionand pulmonary exacerbations. A range of anti-biotics can be useful against these bacteria in-cluding tetracyclines, co-trimoxazole, colistin,and piperacillin/tazobactam. There are no erad-ication studies in the people infected with thesebacteria, but it is logical to attempt to clearthese organisms if possible. Inhaled colistincan be used for S. maltophilia infection, andcombinations of the above antibiotics can beused for treatment of exacerbations (Doringet al. 2012).
B. cepacia Complex Strains
Treatment of B. cepacia complex strains is quiteproblematic. In general, members of this com-plex have intrinsic antibiotic resistance, andBurkholderia cenocepacia, which historicallyhas been the most common Burkholderia inpeople with CF, is almost universally pan-resis-tant. There are no long-term antibiotics recom-mended for treatment of patients with chronicinfection with B. cepacia complex strains, and a
J.F. Chmiel et al.
6 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

recent study of inhaled aztreonam lysine showedno benefit. Intravenous antibiotic treatment isbased on several studies that would suggest thattetracycline, co-trimoxazole, chloramphenicol,colistin, ceftazidime, meropenem, and pipera-cillin/tazobactam combinations may have clin-ical efficacy (Doring et al. 2012).
Nontuberculous Mycobacterial Infection
Nontuberculous mycobacterial infection is acurrently emerging area that is causing diag-nostic and therapeutic challenges. Several non-tuberculous mycobacteria have been isolatedfrom people with CF, although the predominantgroups are the Mycobacterium avium complexand Mycobacterium abscessus organisms. M. ab-scessus infection in CF and in other chroniclung conditions is associated with particularchallenges (Doring et al. 2012). Treatment forboth organisms requires long-term therapy withcombinations of oral, intravenous and/or in-haled antimycobacterial agents. Mycobacteriumavium complex organisms are typically treatedwith combinations of ethambutol, rifampin,macrolides, and inhaled amikacin. For Myco-bacterium abscessus, combinations of amikacin,linezolid, macrolides, cefoxitin, tigicycline, and/or meropenem are utilized. Currently, interna-tional guidelines are being developed to helpfurther guide treatment of this difficult groupof bacteria.
Other Bacterial Species
Many other bacterial species are being identifiedin the airway microbiota in people with CF.Treatment of organisms such as Streptococcusspecies and anaerobic bacteria such as Prevo-tella, Veillonella, Rothia, and Actinomyces spe-cies is not clear (Tunney et al. 2011; Zhaoet al. 2012). There may be changes in how weperceive treatment with antibiotics over thenext several years because second-generation se-quencing provides more insight into the com-plex microbiota of the airways in people withCF. Antimicrobial therapy remains a key corner-stone for the modulation of infection and in-flammation in CF.
THERAPIES DIRECTED AT THEINFLAMMATORY RESPONSE OF THECF AIRWAY
Addressing the inflammatory response is war-ranted because it is the major process leadingto lung destruction. Several steps in the patho-physiological cascade could be targeted. How-ever, efficacy at any step may be beneficial. Earlyanti-inflammatory drug studies focused onsystemic and inhaled corticosteroids, ibupro-fen, and other nonsteroidal anti-inflammatorydrugs (NSAIDs). Many anti-inflammatory drugshave been studied in CF since 1990. Althoughmany have been translated from the bench to aclinical trial, precious few are recommended forclinical use (Table 2). The length of this reviewprecludes a detailed discussion of all of thesedrugs. This review focuses on drugs that haveundergone in-depth evaluation or more recentdevelopments. Corticosteroids and ibuprofenare reviewed first, followed by cytokines and an-ticytokines, modulators of intracellular signal-ing, antioxidants, protease inhibitors, and otheranti-inflammatory therapies.
CORTICOSTEROIDS
Corticosteroids were the first anti-inflammatorydrugs studied in CF. They reduce the formationof mucus and edema; inhibit chemotaxis, adhe-sion, and activation of leukocytes; inhibit NF-kB activation; and interfere with the synthesisor actions of inflammatory mediators. Severalstudies evaluated corticosteroids as a chronictherapy for attenuating CF airway inflamma-tion. Two 4-yr, double-blind, placebo-con-trolled studies of oral corticosteroids laid thefoundation for future anti-inflammatory trials(Auerbach et al. 1985; Eigen et al. 1995). In thesestudies, alternate-day corticosteroids were asso-ciated with better lung function, improvedweight gain, and fewer hospital admissions. Inone trial, beneficial effects on lung function wereobserved primarily in patients infected withP. aeruginosa (Eigen et al. 1995). Adverse effects,including glucose intolerance, growth impair-ment, and cataract formation, limit the long-term practical application of alternate-day oral
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

corticosteroids. In a follow-up study, growthdeficits persisted after therapy discontinua-tion (Lai et al. 2000). In view of these resultsand other known toxicities of corticosteroidsincluding osteopenia, osteoporosis, and skeletalmuscle weakness, the long-term use of systemiccorticosteroids for slowing lung function de-cline is not advocated (Flume et al. 2007).
Adverse effects associated with systemic cor-ticosteroids prompted investigations of inhaledcorticosteroids (ICS). The inhaled route might
afford benefit with less risk than systemic ad-ministration, but systemic administration maybe necessary to affect neutrophil migration.Consistent ICS use was associated with a slowerrate of decline of lung function. However, ICSuse also was associated with decreased weightand height for age, and increased use of insulinand oral hypoglycemic agents in one large ob-servational study (Ren et al. 2008). In anotherobservational study, ICSs were associated withslower FEV1 decline in children with CF age
Table 2. Anti-inflammatory therapies evaluated in CF
Therapy Target
Evaluated only in preclinical studiesAnti-ICAM-1 Leukocyte adhesion moleculesAnti-IL-8 CytokinesAnti-IL-17 CytokinesIL-10 Intracellular signaling and cytokinesInterferon-g Intracellular signalingp38 Mitogen-activated protein
kinase inhibitorsIntracellular signaling
Evaluated in clinical trialsa1-Protease inhibitor ProteasesCorticosteroids Intracellular signaling, eiscosanoids,
cytokinesCXCR2 antagonist Neutrophil chemotaxis/activationCyclosporine-A Intracellular signalingDHA Eicosanoid modulatorEPI-hNE4 ProteasesGlutathione OxidantsHydroxychloroquine UnknownL-Arginine Intracellular signalingLTB4 receptor antagonist (BIIL 284 BS) Leukotriene receptors, eicosanoidsMethotrexate Adhesion molecules, cytokines, transmethylation
reactions, increases adenosine releaseMonocyte/neutrophil elastase inhibitor ProteasesMontelukast Leukotriene receptorsN-Acetyl cysteine Intracellular signaling, oxidantsOmega-3-fatty acids EicosanoidsSecretory leukoprotease inhibitor ProteasesSimvastatin Intracellular signalingThiazolidinediones/pioglitazone Intracellular signalingVitamins C, E, and b-carotene OxidantsVitamin D Bacteria and cytokines
Therapies recommended for clinical useAntibiotics Bacteria (inflammatory stimuli)Azithromycin UnknownDornase-alfa DNAIbuprofen Intracellular signaling, eicosanoids, cytokines
J.F. Chmiel et al.
8 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

6–12 yr but not other age groups (De Boecket al. 2011). A benefit of ICS has not been shownin randomized placebo-clinical trials. None ofthe trials of ICS in CF showed convincing effectson lung function or airway inflammatory mark-ers (Ross et al. 2009). Small study populationsand short observation periods hampered thesetrials. In a large, prospective, multicenter study,withdrawal of ICS for a 6-mo period was notassociated with significant worsening of CFlung disease (Balfour-Lynn et al. 2006). Patientsin whom steroids were discontinued did nothave worsening of lung function, an increasedneed for oral or intravenous antibiotics, or ashorter time to pulmonary exacerbation. Thus,although inhaled steroids may be of benefit inpatients with coexisting asthma, their use as ananti-inflammatory agent in CF has not beensubstantiated. Potential long-term complica-tions of ICS have not been adequately evalu-ated in CF. Caution should be heeded whenprescribing ICS to patients with CF. A CysticFibrosis Foundation expert panel advisedagainst the long-term use of ICS in patientswith CF older than 6 yr who did not have coex-istent asthma or allergic bronchopulmonaryaspergillosis (ABPA) (Flume et al. 2007).
IBUPROFEN
NSAIDs possess properties similar to cortico-steroids but have fewer adverse effects. Ibupro-fen has received the most attention in CF, largelybecause it has specific activity against neutro-phils. Neutrophil chemotaxis to mucosal epi-thelium is significantly decreased with oral dosesof ibuprofen that result in a peak plasma con-centration .50 mg/mL (Konstan et al. 2003). Ina 4-yr, double-blind, placebo-controlled clini-cal trial in the United States in patients withCF, twice-daily high-dose ibuprofen was associ-ated with a slower rate of decline in pulmonaryfunction measures, better preservation of bodyweight, fewer hospital admissions, and betterBrasfield chest radiograph scores, with no sig-nificant adverse effects (Konstan et al. 1995).The beneficial effects were most pronounced inthe youngest patients (5–13 yr old). A 2-yr pla-cebo-controlled multicenter trial in Canada in
145 CF children also showed a beneficial effect ofibuprofen on lung function (Lands et al. 2007).Results from an analysis of observational datafrom the CF Foundation Patient Registry re-vealed that “real world” clinical use of ibuprofenin 1365 CF children treated on average for 4 yrreduced the annual rate of FEV1 decline by 29%compared with those not treated with ibuprofen(Konstan et al. 2007).
Nonetheless, ibuprofen has not been widelyadopted, largely because of the logistic chal-lenges associated with the need to establish thedose in each patient with a 3-h pharmacoki-netic test and to concerns related to adverse ef-fects of the drug (Konstan 2008). Based on U.S.CF Foundation Patient Registry data, ibuprofenuse is associated with gastrointestinal bleeding,but the occurrence is rare (annual incidence0.37% vs. 0.14% in those not treated with ibu-profen [Konstan et al. 2007]). Concomitant useof antacids, proton pump inhibitors, or miso-prostol (a PGE1 analog) would likely limit thisadverse event. Renal failure associated with ibu-profen therapy has been the subject of a few casereports, but CF Foundation Registry data sug-gest that the incidence of renal failure is not in-creased among CF patients treated with ibupro-fen (Konstan et al. 2007). Thus, the benefits ofthis therapy appear to outweigh the associatedrisks. An expert panel recommended high-doseibuprofen for CF patients with mild lung disease(Flume et al. 2007). ACochrane Review also con-cluded that “high-dose ibuprofen can slow theprogression of lung disease in people with CF,especially in children, and this suggests thatstrategies to modulate lung inflammation canbe beneficial for people with CF” (Lands andStanojevic 2007).
CYTOKINES AND ANTICYTOKINES
Since the first trial of corticosteroids, many newanti-inflammatory drugs have been introducedfor the treatment of other diseases. Anti-in-flammatory cytokines and antibodies to proin-flammatory cytokines may have efficacy in CF.Most cytokines are pleiomorphic, and althoughsome show a preponderance of proinflamma-tory effects, others show a preponderance of
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

anti-inflammatory effects. IL-10 possesses manyanti-inflammatory properties. It inhibits theproduction of many proinflammatory cyto-kines, inhibits NF-kB activation, induces neu-trophil apoptosis, and decreases antigen presen-tation and T-cell stimulation. Because IL-10terminates the inflammatory response, its defi-ciency, as shown in CF (Bonfield et al. 1999),might result in persistent inflammation even af-ter stimulus removal. IL-10 deficiency worsensendobronchial inflammation in P. aeruginosa-infected mice (Chmiel et al. 2002b). Administra-tion of IL-10 to infected mice showed beneficialeffects on airway inflammation (Chmiel et al.1999). A planned clinical trial of the drug wasabandoned for reasons unrelated to CF, but thisremains an interesting therapeutic option. Inter-feron-g, another cytokine with anti-inflamma-tory effects, did not improve pulmonary func-tion or alter sputum inflammatory mediators ina multicenter clinical trial despite its ability torestore counter-regulatory functions in CF cellmodels (Moss et al. 2005).
An alternative approach to administeringanti-inflammatory cytokines would be to inhib-it specific proinflammatory mediators. Anti-bodies to ICAM-1 and IL-8 have been evaluatedin preclinical studies but never came to fruitionin clinical trials. IL-17, a proinflammatory cyto-kine involved in TH-17 cell signaling, is elevatedin CF lungs (McAllister et al. 2005; Dubin andKolls 2007) and plays an important role in re-cruiting neutrophils to the airway in response toinfectious stimuli. Anti-IL-17 antibodies re-duced airway neutrophilia in mice exposed tolipopolysaccharide (LPS) (Ferretti et al. 2003).Clinical trials of anti-IL-17 in rheumatoid ar-thritis and psoriasis recently have been complet-ed. Given the similarities between CF lung in-flammation and these hyperinflammatory con-ditions, anti-IL-17 could be considered for CF.
EICOSANOID MODULATORS
LTB4, a potent neutrophil chemoattractant, ispresent in high concentrations in the CF airway(Konstan et al. 1993). BIIL 284 BS (amelubant),a specific LTB4 receptor antagonist, was studiedin CF, but the trial was terminated early because
of a statistically significant increase in pulmo-nary-related serious adverse events in adults re-ceiving BIIL 284 BS (Konstan et al. 2005). Onepossible explanation is that LTB4 has some otherpreviously unrecognized beneficial effect in CF,and its inhibition is detrimental. A more plau-sible explanation might be that the inhibitoryeffect of BIIL 284 BS on the LTB4 pathway wastoo potent, resulting in impaired antimicrobialdefenses and increasing the risk of an exacerba-tion. Regardless, the results of this study showthat care must be taken when selecting an anti-inflammatory agent for future clinical trials.
Deficiencies in some fatty acids may contrib-ute to CF pulmonary inflammation. There is anincrease in arachidonic acid and a decrease indocosahexaenoic acid (DHA) in cftr2/2 mice(Freedman et al. 1999). Investigators have shownthat oral administration of DHA to cftr2/2 micecorrected the lipid imbalance and reversed theobserved pathological manifestations (Freed-man et al. 2002; Beharry et al. 2007). There havebeen a handful of studies of DHA supplementa-tion in CF patients (Van Biervliet et al. 2008;Aldamiz-Echevarria et al. 2009). Unfortunately,the dose of DHA, study size, duration of treat-ment, and outcome measures vary widely. Feware placebo-controlled, and some do not show aclinical effect on lung function, possibly becauseof short observational periods. Despite thesedrawbacks, the cumulative data from these stud-ies indicate that DHA oral supplementation mayeffectively increase serum and phospholipid con-centrations of this essential fatty acid, and thatthis may have beneficial health effects, includingimproved pulmonary function. To validate thisclaim, larger, placebo-controlled trials with anadequate observation period are necessary.
MODULATORS OF INTRACELLULARSIGNALING
Because cytokines contribute to the excessiveinflammatory response in CF, it seems logicalto target signaling pathways responsible for up-regulating their production. Unfortunately,there is no consensus as to what these pathwaysare and how they may interact with the basicdefect in CF. High-dose ibuprofen and IL-10
J.F. Chmiel et al.
10 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

inhibit NF-kB activation, thereby down-regu-lating the inflammatory response at the tran-scriptional level. Other drugs that limit pro-inflammatory molecule transcription may beuseful in CF. Another mechanism of inhibitingNF-kB activity occurs via up-regulation of per-oxisome proliferator activating receptor (PPAR)with the thiazolidinediones or glitazones (Ruanet al. 2003; Vanden Berghe et al. 2003; Zingarelliet al. 2003). CF tissues appear to be deficient inPPAR (Ollero et al. 2004; Perez et al. 2008).Decreased PPAR expression leads to an im-balance between IkB and NF-kB and favors in-creased inflammation. Activation of PPAR mayquell the CF inflammatory response. One of themechanisms by which ibuprofen may work inCF is through the inhibition of NF-kB by acti-vating PPARg (Jaradat et al. 2001; Davis et al.2003). Troglitazone and ciglitazone activatePPAR in primary CF airway epithelial cells andCF epithelial cell lines, and reduce productionof proinflammatory mediators in response toP. aeruginosa (Perez et al. 2008). A 28-d clinicaltrial of pioglitazone did not show a benefi-cial effect on sputum inflammatory mediators(Konstan et al. 2009). However, this may haveoccurred because the dose of pioglitazone wasnot adequate to inhibit inflammation, the du-ration of the study was too short, the number ofsubjects was too small (N ¼ 20), or sputummeasures may not have been sensitive enoughto detect subtle changes. Although this studydid not show a beneficial effect, further evalua-tion of the glitazones in CF is warranted.
Multiple studies show decreased NO in ex-haled air (eNO) from patients with CF (Balfour-Lynn et al. 1996; Grasemann et al. 1997). NO is ahighly reactive molecule with important antimi-crobial and anti-inflammatory properties. Theloss of NO production from the airways maycontribute to bacterial infection and overzeal-ous inflammation (Kelley and Drumm 1998;Meng et al. 1998). One potential cause of de-creased eNO in CF is up-regulation of RhoGT-Pase, a signaling molecule that reduces NOS2expression (Kraynacket al. 2002). Up-regulationof RhoGTPase may also contribute to the in-flammatory response by increasing IL-8 pro-duction. RhoGTPase can be inhibited by block-
ing 3-hydroxy-3-methylglutaryl-CoA reductase(HMG-CoAR) with the commercially availablestatins (e.g., simvastatin) (Kraynack et al. 2002).The statins have other anti-inflammatory effectsincluding the ability to inhibit neutrophil mi-gration, decrease proinflammatory cytokineproduction, and increase transcriptional activa-tion of PPAR (Dunzendorfer et al. 1997; Rezaie-Majd et al. 2002; Zelvyte et al. 2002). A clinicaltrial of simvastatin showed a trend toward in-creased eNO, but no effect was seen on sputuminflammatory markers. This may be for the samereasons cited above for pioglitazone (Kraynacket al. 2008). Other agents that increase NO pro-duction have also been studied. Arginase activityis increased in blood and sputum of CF patientsand may further decrease NO by degradingL-arginine, an NO substrate (Grasemann et al.2005a). In a rodent model, L-arginine was as-sociated with reduced tissue damage, decreas-ed neutrophil recruitment, and reduced IL-1b(Hopkins et al. 2006). A small study of L-argi-nine in CF was associated with increased eNO(Grasemann et al. 2005b). L-Arginine has poten-tial, but large prospective clinical trials have notbeen performed.
Synthetic triterpenoids are small-moleculederivatives of naturally occurring compoundsthat increase Nrf2 activity. Nrf2, a transcriptionfactor active in respiratory epithelia and pivotalto mitigating the acute inflammatory response,is deficient in CF cells (Chen et al. 2008; Nicholset al. 2009). Small molecules like the synthetictriterpenoids that target proinflammatory sig-naling abnormalities in CF cells may be candi-dates for clinical trials. Preclinical studies showthe ability of 2-cyano-3,12-dioxooleana-1,9-dien-28-oic acid (CDDO) to reduce the inflam-matory response (Nichols et al. 2009). Muchresearch is still needed to determine their utility,but early data suggest the theory that com-pounds affecting transcriptional regulators ofinflammation (both pro- and anti-inflammato-ry) are promising therapeutic agents.
ANTIOXIDANTS
Neutrophils release oxygen radicals that con-tribute to local tissue damage and perpetuate
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

inflammation. Elevated concentrations of oxi-dants have been detected in the airways of CFmice and patients (Hull et al. 1997; Velsor etal. 2001). The oxidant–antioxidant imbalancecontributes to the exaggerated and damaginginflammatory response. Some biochemical ab-normalities in CF can be reversed by antioxi-dants. N-Acetyl cysteine, initially developed asa mucolytic, is receiving renewed interest as anantioxidant that both inhibits H2O2 and in-creases glutathione. In a pilot study, oral N-acetyl cysteine was associated with increasedglutathione levels in whole blood and decreasedsputum neutrophils, IL-8, and elastase activity(Tirouvanziam et al. 2006). The study was ofshort duration and not powered to detectchanges in pulmonary function or other clinicaloutcome measures. A large randomized double-blind placebo-controlled trial of N-acetyl cys-teine is ongoing in patients with CF.
The oxidant–antioxidant imbalance maybe exacerbated by abnormalities in CFTR. Ifglutathione is transported by CFTR (Linsdelland Hanrahan 1998), then CFTR abnormalitieswould decrease the concentrations of this im-portant antioxidant on epithelial surfaces, thusleaving the airway vulnerable to even ordinarylevels of oxidative stress. Because decreased lungconcentrations of glutathione have been shownin CF mice and patients (Roum et al. 1993; Vel-sor et al. 2001), it seems logical to augmentits concentration in the CF lung. Glutathionein epithelial lining fluid may be increased bytwice-daily treatment with aerosolized glutathi-one. This treatment also reduced superoxideproduction by inflammatory cells (Roum et al.1993). However, subjects treated with inhaledglutathione had no detectable change in BALmarkers of oxidative stress (Bishop et al. 2005;Hartl 2005). Inhaled glutathione therapy for CFhas attracted much attention, but its therapeuticbenefit has not been adequately studied.
PROTEASE INHIBITORS
Early in life, neutrophils infiltrate the CF airwayand release massive amounts of proteases thatoverwhelm antiproteases, including alpha-1-protease inhibitor (a1-PI) and secretory leuko-
cyte protease inhibitor (SLPI). The concentra-tion of a1-PI in BAL fluid from CF patients isseveral-fold higher than in healthy subjects, buteven in mild patients there is a several hundredto several thousand fold excess of elastase andother neutrophil proteases, which vastly exceedsthe capacity of the inhibitors (Birrer et al. 1994;Konstan et al. 1994; Chmiel et al. 2002a). Theimbalance between the proteases and their in-hibitors becomes worse during exacerbationsand undoubtedly results in airway injury.Antiproteases have been under investigation inCF since 1990. Aerosol delivery of a1-antitryp-sin suppressed inflammatory markers includingfree neutrophil elastase, proinflammatory cyto-kines, and neutrophils (McElvaney et al. 1991;Berger et al. 1995; Bilton et al. 1999; Griese et al.2007). Other inhibitors of neutrophil elastasestudied in CF include rSLPI and the small-mol-ecule drug EPI-hNE4 (McElvaney et al. 1993;Grimbert et al. 2003). Although these inhibitorsshowed positive effects in CF, further trialshave not been conducted with these inhibitors.Data regarding antiprotease therapy suggest thatantiprotease therapy possesses the potential toimpact CF inflammation. Of the antiproteasetherapies studied in CF, inhalation of plasma-derived a1-antitrypsin appears closest to possi-ble clinical use.
OTHER THERAPIES THAT IMPACTINFLAMMATION IN THE CF AIRWAY
Hydroxychloroquine, a dihydrofolate reductaseinhibitor that increases intracellular pH andpossesses anecdotal efficacy in some rare inter-stitial lung diseases, was evaluated in a small28-d study in CF (Williams et al. 2008). Thedrug was well tolerated, but there was no changein sputum inflammatory markers (Williamset al. 2008). CXCR2 is an important receptorin neutrophil chemotaxis. Clinical and preclin-ical studies have evaluated the effects of CXCR2antagonists in many lung diseases includingCOPD, asthma, and ozone-induced airway in-flammation (Lazaar et al. 2011). A clinical trialin CF of SB-656933, a CXCR2 antagonist, wasrecently completed and shows some promise inmodulating airway inflammation (Moss et al.
J.F. Chmiel et al.
12 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

2012). Although chemotherapeutics have beenstudied in refractory asthma, there have been fewstudies in CF. Low-dose cyclosporin A decreasedthe need for systemic corticosteroids in onesmall case series (Bhal et al. 2001). In a smallpilot study, methotrexate increased FEV1 anddecreased total serum immunoglobulins in fiveCF patients after 1 yr of treatment (Ballmannet al. 2003). However, in a more recent study,methotrexate was not well tolerated and was as-sociated with an increased need for IVantibiot-ics (Oermann et al. 2007). Its routine use cannotbe advocated. Because of toxicities, chemother-apeutics should be studied first in animal mod-els. However, even if toxic, some agents may havea favorable risk/benefit profile.
CONCLUSION
CF lung disease begins early in infancy and con-tinues unabated. Persistent infection and exces-sive inflammation are key contributors to theprogression of CF lung disease. Studies showedthat judicious use of antibiotics and anti-in-flammatory drugs is beneficial. The develop-ment of both systemic and inhaled antibioticshas greatly improved survival and remains acornerstone therapy. With the wider range ofantibiotics now available, it is important thatthe most effective regimes for chronic therapy,which reduce pulmonary exacerbations, be de-termined. It is also critical that pulmonary exac-erbations be identified early and treated withappropriate antibiotic combinations.
Anti-inflammatory drugs are another im-portant weapon in the fight against CF. Al-though ICSs are the most frequently prescribedanti-inflammatory therapy in CF, their benefits,like their risks, have not been fully establish-ed. Thus far, high-dose chronic ibuprofen treat-ment is the best-proven anti-inflammatorydrug, although its use in the CF communityhas been surprisingly low. Newer anti-inflam-matory agents will probably come to clinicaltrial over the next few years. More studies ofanti-inflammatory agents are necessary to fullyelucidate their mechanisms of action, to deter-mine which would provide the most benefit toCF patients, and to establish the optimal patient
age and stage of lung disease for initiation oftreatment.
Drugs designed to target abnormal CFTRmay not fully ameliorate the relentless progres-sion of CF lung disease in patients with es-tablished bronchiectasis. Therefore, vigorousresearch and development into anti-infectiveand anti-inflammatory therapeutics that ad-dress secondary disease pathology must contin-ue. Improved antibacterial and anti-inflamma-tory therapies should lessen morbidity, improvequality of life, and prolong survival.
ACKNOWLEDGMENTS
Grant support from the National Institutes ofHealth (Grant P30-DK27651) and the U.S. Cys-tic Fibrosis Foundation is gratefully acknowl-edged. We gratefully acknowledge the editorialassistance of Robert C. Stern, M.D.
REFERENCES
Aldamiz-Echevarrıa L, Prieto JA, Andrade F, Elorz J, Sojo A,Lage S, Sanjurjo P, Vazquez C, Rodrıguez-Soriano J. 2009.Persistence of essential fatty acid deficiency in cystic fi-brosis despite nutritional therapy. Pediatr Res 66: 585–589.
Armstrong DS, Grimwood K, Carzino R, Carlin JB, Olin-sky A, Phelan PD. 1995. Lower respiratory infection andinflammation in infants with newly diagnosed cystic fi-brosis. BMJ 310: 1571–1572.
Armstrong DS, Grimwood K, Carlin JB, Armstrong DS,Grimwood K, Carlin JB, Carzino R, Gutierrez JP, Hull J,Olinsky A, et al. 1997. Lower airway inflammation ininfants and young children with cystic fibrosis. Am JRespir Crit Care Med 156: 1197–1204.
Auerbach HS, Williams M, Kirkpatrick JA, Colten HR. 1985.Alternate-day prednisone reduces morbidity and im-proves pulmonary function in cystic fibrosis. Lancet 2:686–688.
Balfour-Lynn IM, Laverty A, Dinwiddie R. 1996. Reducedupper airway nitric oxide in cystic fibrosis. Arch Dis Child75: 319–322.
Balfour-Lynn IM, Lees B, Hall P, Phillips G, Khan M, Fla-ther M, Elborn JS, CF WISE (Withdrawal of InhaledSteroids Evaluation) Investigators. 2006. Multicenterrandomized controlled trial of withdrawal of inhaled cor-ticosteroids in cystic fibrosis. Am J Respir Crit Care Med173: 1356–1362.
Ballmann M, Junge S, von der Hardt H. 2003. Low-dosemethotrexate for advanced pulmonary disease in patientswith cystic fibrosis. Respir Med 97: 498–500.
Balough K, McCubbin M, Weinberger M, Smits W, Ah-rens R, Fick R. 1995. The relationship between infection
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

and inflammation in the early stages of lung disease fromcystic fibrosis. Pediatr Pulmonol 20: 63–70.
Beharry S, Ackerley C, Corey M, Kent G, Heng YM, Chris-tensen H, Luk C, Yantiss RK, Nasser IA, Zaman M, et al.2007. Long-term docosahexaenoic acid therapy in a con-genic murine model of cystic fibrosis. Am J Physiol Gas-trointest Liver Physiol 292: G839–G848.
Berger M, Konstan MW, Hilliard JB. 1995. Aerosolized pro-lastin (a1-protease inhibitor) in CF. Pediatr Pulmonol 20:421.
Bhal GK, Maguire SA, Bowler IM. 2001. Use of cyclosporinA as a steroid sparing agent in cystic fibrosis. Arch DisChild 84: 89.
Bilton D, Elborn S, Conway S, Edgar J, Redmond A. 1999.Phase II trial to assess the clinical efficacy of transgenica-1-antitrypsin (tg-hAAT) as an effective treatment of cys-tic fibrosis. Pediatr Pulmonol 28 (Suppl 19): 246.
Birrer P, McElvaney NG, Rudeberg A, Sommer CW, Liechti-Gallati S, Kraemer R, Hubbard R, Crystal RG. 1994. Pro-tease–antiprotease imbalance in the lungs of childrenwith cystic fibrosis. Am J Respir Crit Care Med 150: 207–213.
Bishop C, Hudson VM, Hilton SC, Wilde C. 2005. A pilotstudy of the effects of inhaled buffered reduced glutathi-one on the clinical status of patients with cystic fibrosis.Chest 127: 308–317.
Bonfield TL, Panuska JR, Konstan MW, Hilliard KA, Hil-liard JB, Ghnaim H, Berger M. 1995a. Inflammatory cy-tokines in cystic fibrosis lungs. Am J Respir Crit Care Med152: 2111–2118.
Bonfield TL, Konstan MW, Burfeind P, Panuska JR, Hilli-ard JB, Berger M. 1995b. Normal bronchial epithelial cellsconstitutively produce the anti-inflammatory cytokineinterleukin-10, which is downregulated in cystic fibrosis.Am J Respir Cell Mol Biol 13: 257–261.
Bonfield TL, Konstan MW, Berger M. 1999. Altered respira-tory epithelial cell cytokine production in cystic fibrosis.J Allergy Clin Immunol 104: 72–78.
Chen J, Kinter M, Shank S, Cotton C, Kelley TJ, Ziady AG.2008. Dysfunction of Nrf-2 in CF epithelia leads to excessintracellular H2O2 and inflammatory cytokine produc-tion. PLoS ONE 3: e3367.
Chmiel JF, Davis PB. 2003. State of the art: Why do the lungsof patients with cystic fibrosis become infected and whycan’t they clear the infection? Respir Res 4: 8–21.
Chmiel JF, Konstan MW, Knesebeck JE, Hilliard JB, Bon-field TL, Dawson DV, Berger M. 1999. IL-10 attenuatesexcessive inflammation in chronic Pseudomonas in-fection in mice. Am J Respir Crit Care Med 160: 2040–2047.
Chmiel JF, Konstan MW, Berger M. 2002a. The role of in-flammation in the pathophysiology of CF lung disease.Clin Review Allergy Immunol 23: 5–27.
Chmiel JF, Konstan MW, Saadane A, Krenicky JE, LesterKirchner H, Berger M. 2002b. Prolonged inflammatoryresponse to acute Pseudomonas challenge in interleukin-10 knockout mice. Am J Respir Crit Care Med 165: 1176–1181.
Dasenbrook EC, Merlo CA, Diener-West M, Lechtzin N,Boyle MP. 2008. Persistent methicillin-resistant Staphylo-
coccus aureus and rate of FEV1 decline in cystic fibrosis.Am J Respir Crit Care Med 178: 814–821.
Dasenbrook EC, Checkley W, Merlo CA, Konstan MW,Lechtzin N, Boyle MP. 2010. Association between respi-ratory tract methicillin-resistant Staphylococcus aureusand survival in cystic fibrosis. JAMA 303: 2386–2392.
Davis PB, Drumm M, Konstan MW. 1996. Cystic fibrosis.State of the art. Am J Resp Crit Care Med 154: 1229–1256.
Davis PB, Gupta S, Eastman J, Konstan MW. 2003. Inhibi-tion of proinflammatory cytokine production by PPARgagonists in airway epithelial cells. Pediatr Pulmonol 36(Suppl 25): 268–269.
De Boeck K, Vermeulen F, Wanyama S, Thomas M, Mem-bers of the Belgian CF Registry. 2011. Inhaled corticoste-roids and lower lung function decline in young childrenwith cystic fibrosis. Eur Respir J 37: 1091–1095.
Doring G, Flume P, Heijerman H, Elborn JS, ConsensusStudy Group. 2012. Treatment of lung infection in pa-tients with cystic fibrosis: Current and future strategies. JCyst Fibros 2012 11: 461–479.
Dubin PJ, Kolls JK. 2007. IL-23 mediates inflammatory re-sponses to mucoid Pseudomonas aeruginosa lung infec-tion in mice. Am J Physiol Lung Cell Mol Physiol 292:L519–L528.
Dubin PJ, McAllister F, Kolls JK. 2007. Is cystic fibrosis aTH17 disease? Inflamm Res 56: 221–227.
Dunzendorfer S, Rothbucher D, Schratzberger P, ReinischN, Kahler CM, Wiedermann CJ. 1997. Mevalonate-de-pendent inhibition of transendothelial migration andchemotaxis of human peripheral blood neutrophils bypravastatin. Circ Res 81: 963–969.
Eigen H, Rosenstein BJ, FitzSimmons S, Schidlow DV. 1995.A multicenter study of alternate-day prednisone therapyin patients with cystic fibrosis. Cystic Fibrosis FoundationPrednisone Trial Group. J Pediatr 126: 515–523.
Ferretti S, Bonneau O, Dubois GR, Jones CE, Trifilieff A.2003. IL-17, produced by lymphocytes and neutrophils,is necessary for lipopolysaccharide-induced airway neu-trophilia: IL-15 as a possible trigger. J Immunol 170:2106–2112.
Flume PA, O’Sullivan BP, Robinson KA, Goss CH, Mogay-zel PJ Jr, Willey-Courand DB, Bujan J, Finder J, Lester M,Quittell L, et al. 2007. Cystic fibrosis pulmonary guide-lines. Am J Respir Crit Care Med 176: 957–969.
Freedman SD, Katz MH, Parker EM, Laposata M, Ur-man MY, Alvarez JG. 1999. A membrane lipid imbal-ance plays a role in the phenotypic expression of cysticfibrosis in cftr2/2 mice. Proc Natl Acad Sci 96: 13995–14000.
Freedman SD, Weinstein D, Blanco PG, Martinez-Clark P,Urman S, Zaman M, Morrow JD, Alvarez JG. 2002. Char-acterization of LPS-induced lung inflammation incftr2/2 mice and the effect of docosahexaenoic acid. JAppl Physiol 92: 2169–2176.
Grasemann H, Michler E, Wallot M, Ratjen F. 1997. De-creased concentration of exhaled nitric oxide (NO) inpatients with cystic fibrosis. Pediatr Pulmonol 24: 173–177.
Grasemann H, Schwiertz R, Matthiesen S, Racke K, Ratjen F.2005a. Increased arginase activity in cystic fibrosis air-ways. Am J Respir Crit Care Med 172: 1523–1528.
J.F. Chmiel et al.
14 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Grasemann H, Grasemann C, Kurtz F, Tietze-Schillings G,Vester U, Ratjen F. 2005b. Oral L-arginine supplementa-tion in cystic fibrosis patients: A placebo-controlledstudy. Eur Respir J 25: 62–68.
Griese M, Latzin P, Kappler M, Weckerle K, Heinzlmaier T,Bernhardt T, Hartl D. 2007. a1-Antitrypsin inhalationreduces airway inflammation in cystic fibrosis patients.Eur Respir J 29: 240–250.
Grimbert D, Vecellio L, Delepine P, Attucci S, Boissinot E,Poncin A, Gauthier F, Valat C, Saudubray F, Antonioz P,et al. 2003. Characteristics of EPI-hNE4 aerosol: A newelastase inhibitor for treatment of cystic fibrosis. J AerosolMed 16: 121–129.
Hartl D, Starosta V, Maier K, Beck-Speier I, Rebhan C,Becker BF, Latzin P, Fischer R, Ratjen F, Huber RM,et al. 2005. Inhaled glutathione decreases PGE2 and in-creases lymphocytes in cystic fibrosis lungs. Free RadicBiol Med 39: 463–472.
Hopkins N, Gunning Y, O’Croinin DF, Laffey JG, Mc-Loughlin P. 2006. Anti-inflammatory effect of augment-ed nitric oxide production in chronic lung infection. JPathol 209: 198–205.
Hull J, Vervaart P, Grimwood K, Phelan P. 1997. Pulmonaryoxidative stress response in young children with cysticfibrosis. Thorax 52: 557–560.
Jaradat MS, Wongsud B, Phornchirasilp S, Rangwala SM,Shams G, Sutton M, Romstedt KJ, Noonan DJ, Feller DR.2001. Activation of peroxisome proliferators-activatedreceptor isoforms and inhibition of prostaglandin H2
synthases by ibuprofen, naproxen, and indomethacin.Biochem Pharmacol 62: 1587–1595.
Kelley TJ, Drumm ML. 1998. Inducible nitric oxide synthaseexpression is reduced in cystic fibrosis murine and hu-man airway epithelial cells. J Clin Invest 102: 1200–1207.
Khan TZ, Wagener JS, Bost T, Martinez J, Accurso FJ,Riches DW. 1995. Early pulmonary inflammation in in-fants with cystic fibrosis. Am J Respir Crit Care Med 151:1075–1082.
Kirchner KK, Wagener JS, Khan TZ, Copenhaver SC,Accurso FJ. 1996. Increased DNA levels in bronchoalveo-lar lavage fluid obtained from infants with cystic fibrosis.Am J Respir Crit Care Med 154: 1426–1429.
Konstan MW. 2008. Ibuprofen therapy for cystic fibrosislung disease: Revisited. Curr Opin Pulm Med 14: 567–573.
Konstan MW, Berger M. 1997. Current understanding of theinflammatory process in cystic fibrosis—Onset and eti-ology. Pediatr Pulmonol 24: 137–142.
Konstan MW, Walenga RW, Hilliard KA, Hilliard JB. 1993.Leukotriene B4 is markedly elevated in the epithelial lin-ing fluid of patients with cystic fibrosis. Am Rev Respir Dis148: 896–901.
Konstan MW, Hilliard KA, Norvell TM, Berger M. 1994.Bronchoalveolar lavage findings in cystic fibrosis patientswith stable, clinically mild lung disease suggest ongoinginfection and inflammation. Am J Respir Crit Care Med150: 448–454.
Konstan MW, Byard PJ, Hoppel CL, Davis PB. 1995. Effect ofhigh-dose ibuprofen in patients with cystic fibrosis. NEngl J Med 332: 848–854.
Konstan MW, Krenicky JE, Finney MR, Kirchner HL,Hilliard KA, Hilliard JB, Davis PB, Hoppel CL. 2003.Effect of ibuprofen on neutrophil migration in vivo incystic fibrosis. J Pharmacol Exp Ther 306: 1086–1091.
Konstan MW, Doring G, Lands LC, Hilliard KA, Koker P,Bhattacharya S, Staab A, Hamilton AL. 2005. Results of aphase II clinical trial of BIIL 284 BS (a LTB4 receptorantagonist) for the treatment of CF lung disease. PediatrPulmonol 40 (Suppl 28): 125–127.
Konstan MW, Schluchter MD, Xue W, Davis PB. 2007. Clin-ical use of ibuprofen is associated with slower FEV1 de-cline in children with cystic fibrosis. Am J Respir Crit CareMed 176: 1084–1089.
Konstan M, Krenicky J, Hilliard K, Hilliard J. 2009. A pilotstudy evaluating the effect of pioglitazone, simvastatin,and ibuprofen on neutrophil migration in vivo in healthysubjects. Pediatr Pulmonol 44 (Suppl 32): 289–290.
Konstan MW, Geller DE, Minic P, Brockhaus F, Zhang J,Angyalosi G. 2011. Tobramycin inhalation powder forP. aeruginosa infection in cystic fibrosis: The EVOLVEtrial. Pediatr Pulmonol 46: 230–238.
Kraynack NC, Corey DA, Elmer HL, Kelley TJ. 2002. Mech-anisms of NOS2 regulation by Rho GTPase signaling inairway epithelial cells. Am J Physiol Lung Cell Mol Physiol283: L604–L611.
Kraynack NC, Chmiel JF, Xue W, Schluchter MD, Gib-son RL, Kelley TJ, Hilliard JB, Konstan MW. 2008. Effectof simvastatin on exhaled nitric oxide and inflammatorymarkers in sputum in patients with cystic fibrosis. PediatrPulmonol 43 (Suppl 31): 300.
Lai H-C, FitzSimmons SC, Allen DB, Kosorok MR, Ro-senstein BJ, Campbell PW, Farrell PM. 2000. Risk of per-sistent growth impairment after alternate-day prednisonetreatment in children with cystic fibrosis. N Engl J Med342: 851–859.
Lands L, Stanojevic S. 2007. Oral non-steroidal anti-inflam-matory drug therapy for cystic fibrosis. Cochrane Data-base Syst Rev 17: CD001505.
Lands LC, Milner R, Cantin AM, Manson D, Corey M. 2007.High-dose ibuprofen in cystic fibrosis: Canadian safetyand effectiveness trial. J Pediatr 151: 228–230.
Lazaar AL, Sweeney LE, MacDonald AJ, Alexis NE, Chen C,Tal-Singer R. 2011. SB-656933, a novel CXCR2 selectiveantagonist, inhibits ex vivo neutrophil activation andozone-induced airway inflammation in humans. Br JClin Pharmacol 72: 282–293.
Linsdell P, Hanrahan JW. 1998. Glutathione permeability ofCFTR. Am J Physiol 275 (Pt 1): C323–C326.
LiPuma J. 2010. The changing microbial epidemiology inCF. Clin Microbiol Rev 23: 299–323.
LiPuma J. 2012. The new microbiology of cystic fibrosis: Ittakes a community. Thorax 67: 851–852.
McAllister F, Henry A, Kreindler JL, Dubin PJ, Ulrich L,Steele C, Finder JD, Pilewski JM, Carreno BM, Gold-man SJ, et al. 2005. Role of IL-17A, IL-17F, and the IL-17 receptor in regulating growth related oncogene-a andgranulocyte colony-stimulating factor in bronchial epi-thelium: Implications for airway inflammation in cysticfibrosis. J Immunol 175: 404–412.
McElvaney NG, Hubbard RC, Birrer P, Chernick MS,Caplan DB, Frank MM, Crystal RG. 1991. Aerosol a1-
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

antitrypsin treatment for cystic fibrosis. Lancet 337:392–394.
McElvaney NG, Doujaiji B, Moan MJ, Burnham MR, WuMC, Crystal RG. 1993. Pharmacokinetics of recombinantsecretory leukoprotease inhibitor aerosolized to normalsand individuals with cystic fibrosis. Am Rev Respir Dis148 (Pt 1): 1056–1060.
Meng QH, Springall DR, Bishop AE, Morgan K, EvansTJ, Habib S, Gruenert DC, Gyi KM, Hodson ME, Ya-coub MH, et al. 1998. Lack of inducible nitric oxide syn-thase in bronchial epithelium: A possible mechanism ofsusceptibility to infection in cystic fibrosis. J Pathol 184:323–331.
Moss RB, Mayer-Hamblett N, Wagener J, Daines C, Hale K,Ahrens R, Gibson RL, Anderson P, Retsch-Bogart G,Nasr SZ, et al. 2005. Randomized, double-blind, place-bo-controlled, dose-escalating study of aerosolized inter-feron g-1b in patients with mild to moderate cystic fibro-sis lung disease. Pediatr Pulmonol 39: 209–218.
Moss RB, Mistry SJ, Konstan MW, Pilewski JM, Kerem E,Tal-Singer R, Lazaar AL, for the CF2110399 Investigators.2012. Safety and early treatment effects of the CXCR2antagonist SB-656933 in patients with cystic fibrosis. JCyst Fibros pii: S1569-1993(12)00155-5
Muhlebach MS, PW Stewart, Leigh MW, Noah TL. 1999.Quantitation of inflammatory response to bacteria inyoung cystic fibrosis and control patients. Am J RespirCrit Care Med 160: 186–191.
Nichols DP, Ziady AG, Shank SL, Eastman JF, Davis PB.2009. The triterpenoid CDDO limits inflammation inpreclinical models of cystic fibrosis lung disease. Am JPhysiol Lung Cell Mol Physiol 297: L828–L836.
Noah TL, Black HR, Cheng PW, Wood RE, Leigh MW. 1997.Nasal and bronchoalveolar lavage fluid cytokines in earlycystic fibrosis. J Infect Dis 175: 638–647.
Oermann CM, Katz M, Wheeler C, Cumming S. 2007. Apilot study evaluating the potential use of low-dose meth-otrexate as an anti-inflammatory therapy for cystic fibro-sis lung disease. Pediatr Pulmonol 42 (Suppl 30): 292–293.
Ollero M, Junaidi O, Zaman MM, Tzameli I, Ferrando AA,Andersson C, Blanco PG, Bialecki E, Freedman SD. 2004.Decreased expression of peroxisome proliferators activat-ed receptor g in cftr2/2 mice. J Cell Physiol 200: 235–244.
Parkins MD, Rendall JC, Elborn JS. 2012. Incidence and riskfactors for pulmonary exacerbation treatment failures incystic fibrosis patients chronically infected with Pseudo-monas aeruginosa. Chest 141: 485–493.
Perez A, van Heeckeren AM, Nichols D, Gupta S, Eastman JF,Davis PB. 2008. Peroxisome proliferator–activated re-ceptor-g in cystic fibrosis lung epithelium. Am J PhysiolLung Cell Mol Physiol 295: L303–L313.
Proesmans M. 2013. Comparison of two treatment regimensfor eradication of P. aeruginosa infection in children withcystic fibrosis. J Cyst Fibros 12: 29–34.
Ratjen F, Munck A, Kho P, Angyalosi G, ELITE Study Group.2010. Treatment of early Pseudomonas aeruginosa infec-tion in patients with cystic fibrosis: The ELITE trial. Tho-rax 65: 286–291.
Ren CL, Pasta DJ, Rasouliyan L, Wagener JS, Konstan MW,Morgan WJ, Scientific Advisory Group the Investigators
and Coordinators of the Epidemiologic Study of CysticFibrosis. 2008. Relationship between inhaled corticoste-roid therapy and rate of lung function decline in childrenwith cystic fibrosis. J Pediatr 153: 746–751.
Rezaie-Majd A, Maca T, Bucek RA, Valent P, Muller MR,Husslein P, Kashanipour A, Minar E, Baghestanian M.2002. Simvastatin reduces expression of cytokines inter-leukin-6, interleukin-8, and monocyte chemoattractantprotein-1 in circulating monocytes from hypercholester-olemic patients. Arterioscler Thromb Vasc Biol 22: 1194–1199.
Ross KR, Chmiel JF, Konstan MW. 2009. The role of inhaledcorticosteroids in the management of cystic fibrosis. Pae-diatr Drugs 11: 101–113.
Roum JH, Buhl R, McElvaney NG, Borok Z, Crystal RG.1993. Systemic deficiency of glutathione in cystic fibrosis.J Appl Physiol 75: 2419–2424.
Ruan H, Pownall HJ, Lodish HF. 2003. Troglitazone antag-onizes tumor necrosis factor-a-induced reprogrammingof adipocyte gene expression by inhibiting the transcrip-tional regulatory functions of NF-kB. J Biol Chem 278:28181–28192.
Sanders DB, Bittner RC, Rosenfeld M, Hoffman LR, Red-ding GJ, Goss CH. 2010. Failure to recover to baselinepulmonary function after cystic fibrosis pulmonary exac-erbation. Am J Respir Crit Care Med 182: 627–632.
Schuster A, Haliburn C, Doring G, Goldman MH, for theFreedom Study Group. 2012. Safety, efficacy and conve-nience of colistimethate sodium dry powder for inhala-tion (Colobreathe DPI) in cystic fibrosis patients: A rand-omised study. Thorax 68: 344–350.
Smyth A, Elborn JS. 2008. Exacerbations in cystic fibrosis:3—Management. Thorax 63: 180–184.
Smyth AR, Walters S. 2012. Prophylactic anti-staphylococ-cal antibiotics for cystic fibrosis. Cochrane Database SystRev 12: CD001912. 23235585.
Stenbit AE, Flume PA. 2011. Pulmonary exacerbations incystic fibrosis. Curr Opin Pulm Med 17: 442–447.
Taccetti G, Bianchini E, Cariani L, Buzzetti R, Costantini D,Trevisan F. 2012. Early antibiotic treatment for Pseudo-monas aeruginosa eradication in patients with cystic fi-brosis: A randomised multicentre study comparing twodifferent protocols. Thorax 67: 853–859.
Tirouvanziam R, Conrad CK, Bottiglieri T, Herzenberg LA,Moss RB, Herzenberg LA. 2006. High-dose oral N-ace-tylcysteine, a glutathione prodrug, modulates inflamma-tion in cystic fibrosis. Proc Natl Acad Sci 103: 4628–4633.
Treggiari MM, Retsch-Bogart G, Mayer-Hamblett N, KhanU, Kulich M, Kronmal R, Williams J, Hiatt P, Gibson RL,Spencer T, et al. 2011. Comparative efficacy and safety of 4randomized regimens to treat early Pseudomonas aerugi-nosa infection in children with cystic fibrosis. Arch PediatrAdolesc Med 165: 847–856.
Tunney MM, Field TR, Moriarty TF, Patrick S, Doering G,Muhlebach MS, Wolfgang MC, Boucher R, Gilpin DF,McDowell A, et al. 2008. Detection of anaerobic bacteriain high numbers in sputum from patients with cysticfibrosis. Am J Respir Crit Care Med 177: 995–1001.
Tunney MM, Klem ER, Fodor AA, Gilpin DF, Moriarty TF,McGrath SJ, Muhlebach MS, Boucher RC, Cardwell C,Doering G, et al. 2011. Use of culture and molecularanalysis to determine the effect of antibiotic treatment
J.F. Chmiel et al.
16 Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

on microbial community diversity and abundance dur-ing exacerbation in patients with cystic fibrosis. Thorax66: 579–584.
Valerius NH, Koch C, Høiby N. 1991. Prevention of chronicPseudomonas aeruginosa colonisation in cystic fibrosis byearly treatment. Lancet 338: 725–726.
Van Biervliet S, Devos M, Delhaye T, Van Biervliet JP,Robberecht E, Christophe A. 2008. Oral DHA supple-mentation in DF508 homozygous cystic fibrosis patients.Prostaglandins Leukot Essent Fatty Acids 78: 109–115.
Vanden Berghe W, Vermeulen L, Delerive P, De Bosscher K,Staels B, Haegeman G. 2003. A paradigm for gene regu-lation: Inflammation, NF-kB, and PPAR. Adv Exp MedBiol 544: 181–196.
VanDevanter DR, O’Riordan MA, Blumer JL, Konstan MW.2010. Assessing time to pulmonary function benefit fol-lowing antibiotic treatment of acute cystic fibrosis exac-erbations. Respir Res 11: 137.
Velsor LW, van Heeckeren A, Day BJ. 2001. Antioxidantimbalance in the lungs of cystic fibrosis transmembraneconductance regulator protein mutant mice. Am J PhysiolLung Cell Mol Physiol 281: L31–L38.
Williams HD, Davies JC. 2012. Basic science for the chestphysician: Pseudomonas aeruginosa and the cystic fibrosisairway. Thorax 67: 465–467.
Williams B, Robinette M, Slovis B, Deretci V, Perkett E. 2008.Hydroxychloroquine—Pilot study of anti-inflammatoryeffects in cystic fibrosis. Pediatr Pulmonol 43 (Suppl 31):314.
Zelvyte I, Dominaitiene R, Crisby M, Janciauskiene S. 2002.Modulation of inflammatory mediators and PPARg andNFkB expression by pravastatin in response to lipopro-teins in human monocytes in vitro. Pharmacol Res 45:147–154.
Zhao J, Schloss PD, Kalikin LM, Carmody LA, Foster BK,Petrosino JF, Cavalcoli JD, VanDevanter DR, Murray S,Li JZ, et al. 2012. Decade-long bacterial community dy-namics in cystic fibrosis airways. Proc Natl Acad Sci 109:5809–5814.
Zingarelli B, Sheehan M, Hake PW, O’Connor M, Denen-berg A, Cook JA. 2003. Peroxisome proliferator activatorreceptor-g ligands, 15-deoxy-D12,14-prostaglandin J2 andciglitazone, reduce systemic inflammation in polymicor-bial sepsis by modulation of signal transduction path-ways. J Immunol 171: 6827–6837.
Antibiotics and Anti-Inflammatories in CF
Cite this article as Cold Spring Harb Perspect Med 2013;3:a009779 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

23, 20132013; doi: 10.1101/cshperspect.a009779 originally published online JulyCold Spring Harb Perspect Med
James F. Chmiel, Michael W. Konstan and J. Stuart Elborn Antibiotic and Anti-Inflammatory Therapies for Cystic Fibrosis
Subject Collection Cystic Fibrosis
Cystic FibrosisAntibiotic and Anti-Inflammatory Therapies for
ElbornJames F. Chmiel, Michael W. Konstan and J. Stuart
The Cystic Fibrosis IntestineRobert C. De Lisle and Drucy Borowitz
System of the LungStructure and Function of the Mucus Clearance
Brenda M. Button and Brian ButtonCorrectors and PotentiatorsCystic Fibrosis Transmembrane Regulator
Steven M. Rowe and Alan S. Verkman
Other than CFTRNew Pulmonary Therapies Directed at Targets
Scott H. Donaldson and Luis Galietta
The Cystic Fibrosis of Exocrine PancreasMichael Wilschanski and Ivana Novak
The Cystic Fibrosis Airway MicrobiomeSusan V. Lynch and Kenneth D. Bruce
and StabilityFunctionTransmembrane Conductance Regulator
Dynamics Intrinsic to Cystic Fibrosis
Dokholyan, et al.P. Andrew Chong, Pradeep Kota, Nikolay V.
Regulator (ABCC7) StructureCystic Fibrosis Transmembrane Conductance
John F. Hunt, Chi Wang and Robert C. FordPerspectiveThe Cystic Fibrosis Gene: A Molecular Genetic
Lap-Chee Tsui and Ruslan Dorfman
Cystic FibrosisStatus of Fluid and Electrolyte Absorption in
M.M. Reddy and M. Jackson StuttsAnion PermeationThe CFTR Ion Channel: Gating, Regulation, and
Tzyh-Chang Hwang and Kevin L. Kirk
PhenotypesThe Influence of Genetics on Cystic Fibrosis
Michael R. Knowles and Mitchell DrummCFTRAssessing the Disease-Liability of Mutations in
Claude Ferec and Garry R. Cutting
Lessons from the Biochemical World−−Perspectives on Mucus Properties and Formation
Gustafsson, et al.Daniel Ambort, Malin E.V. Johansson, Jenny K.
Supramolecular Dynamics of MucusPedro Verdugo
http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see
Copyright © 2013 Cold Spring Harbor Laboratory Press; all rights reserved
Press on December 18, 2020 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from