Antianginal student222

of 69
Transcript of Antianginal student222
-
8/2/2019 Antianginal student222
1/69
Coronary Vascular
insufficiency
(Ischemic Heart Disease)
-
8/2/2019 Antianginal student222
2/69
Coronary V. Insufficiency
Clinical manifistation:Clinical manifistation:
Disease of coronary artery is almost due to atheroma
and its complications particularly thrombosis.
1. Stable angina
2. Unstable angina
3. Myocardial Infarction M.I.
4. Heart Failure
5. Arrhythmia
-
8/2/2019 Antianginal student222
3/69
Angina Pectoris:
Chest pain due to myocardial ischemia.
Ischemia occurs when there is imbalance between
myocardial oxygen supply ( coronary blood flow) and
myocardial oxygen demand ( myocardial work)
Imbalance between
Decrease oxygen supply
due to fixed atheroscleroticnarrowing
Increase Oxygen Demand due to
increase heart rate, Increase
ventricular contraction, exercise,
emotional stress.
-
8/2/2019 Antianginal student222
4/69
1. Classic, effort, stable angina
present with retrosternal pain, transient 2-5 minprecipitated by exertion andRELIVED BY REST.
2. Unstable angina
Prolonged severe chest pain or pain at rest. It is a rapid
worsening angina that may progress to M.I.
* Myocardial infarction: is due to the death of an area of
myocardium due to prolonged ischemia more than 15 min
induced by coronary thrombosis. Present by severe
prolonged pain pallor, breathlessness, vomiting, collapse,
hypotension and bradycardia ( vagus stimulation).
3. Vasospastic, Variant angina: Transient spasm present with acute
episode of coronary artery spasm with severe chest painAT
REST
Types of Angina
-
8/2/2019 Antianginal student222
5/69
1. Fixed athermatous narrowing of large coronary
vessels (common).
{ Stable (effort) angina, Unstable (resting) angina }
2. Transient spasm of localized portion of
coronary vessels with / without atheroma(less common)
(vasospastic, variant, prinzmetals angina)
Causes of Angina
-
8/2/2019 Antianginal student222
6/69
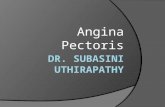
Coronary V. Insufficiency
30% Narrowing 50% Narrowing 70% Narrowing
99% Obstruction 100% Obstruction
No Angina Potential of Angina Stable Angina
Unstable Angina Occlusion M.I.
-
8/2/2019 Antianginal student222
7/69
1.To Increase Oxygen delivery to the
myocardium & increase coronary
perfusion . vasodilators (e.g. nitrates
&nifedipine)
OR
2. To decrease Oxygen demand. By drugs
which depress the cardiac work (e.g CCB
or B-blockers)
General Goals Of Anti anginal
Therapy
-
8/2/2019 Antianginal student222
8/69
Determinants of MyocardialDeterminants of Myocardial
oxygen demandoxygen demand
PreloadDepend and venous tone
After loadABP depends on PVR
Heart rate Cardiac contracti l ity
-
8/2/2019 Antianginal student222
9/69
1. Avoid riskfactors
Smoking,
obesity,
hypertension,diabetes,
increased
cholesterol
level
Management of Angina
3. Invasivemeasures
coronary
bypass, or
angioplasty
2. Drug therapyOrganic
nitrates,
CC blockers,
Blockers,
Aspirin
Heparin
-
8/2/2019 Antianginal student222
10/69
1. Increase
myocardial
oxygen
supply
a. Dilatation of
large
coronary
vessels
b. Redistribution of coronary
flow
c. Dilatation of
collaterals
Organic nitrates
2. Decrease of
oxygen
demand
Decrease ofcardiac work
indirectly.
a. Decrease
preload (veno-
dilators ).
b. Decrease after
load arteriolar
dilators.
3. Antithrombotic
action of
Nitrates.
Decrease
platelets
aggregation by
virtue of
increased
synthesis of (c
GMP)
-
8/2/2019 Antianginal student222
11/69
Mechanism of Action of Nitrates (NO3-)
Nitrites
NO2-
GlutathioneStransferase
Nitric oxide
NO
cGMP
administeredNitrates
Dephosphrylation
of myosin
light chain
Vascular smooth
Muscle
relaxation
-
8/2/2019 Antianginal student222
12/69
1. Rapid acting (acuteattack)
a. Nitroglycerine sublingual
tablets or spray ( onset : 2
min, duration : 25 min)
b. Isosorbid dinitrate
sublingual( onset : 5 min,duration : 1 hour)
Preparations of nitrates
2.Short & Long term
(Prophylaxis)
Nitroglycerine Oral,
sustained release
Isosorbid dinitrate tablets
( onset : 30 min)
(duration : 8 hours)
I. Nitroglycerine Transdermal
Patch
II. Isosorbid mononitrate
( onset : 30 min)
(duration : 8 -14hours)
Used in all types of angina ( treatment and prophylactic)
-
8/2/2019 Antianginal student222
13/69
Pharmacokinetics of nitratesPharmacokinetics of nitrates
NG is well absorbed from GIT butNG is well absorbed from GIT butundergoes extensive first- passundergoes extensive first- passmetabolism in the liver to inactivemetabolism in the liver to inactivemetabolitesmetabolites .So NG is given SL (0.5 mg. ) ,.So NG is given SL (0.5 mg. ) ,
buccal ,Transdermal ,&I.V. ( in acutebuccal ,Transdermal ,&I.V. ( in acuteattack )attack ) Slow release (SR) oral preparations of NGSlow release (SR) oral preparations of NG
(2.5mg-12.5mg ) as prophylactic.(2.5mg-12.5mg ) as prophylactic. Isosorbide dinitrate also has extensive first-Isosorbide dinitrate also has extensive first-
pass metabolismpass metabolism It has relatively longer duration of actionIt has relatively longer duration of action
than NG (it is metabolized to active ISMN )than NG (it is metabolized to active ISMN )
-
8/2/2019 Antianginal student222
14/69
Isosorbid 5-mononitrate is anIsosorbid 5-mononitrate is an
active metabolite of ISD , it isactive metabolite of ISD , it isnot subjected to first-passnot subjected to first-pass
metabolism so used orally.metabolism so used orally.
-
8/2/2019 Antianginal student222
15/69
a)In all types of
Angina.
b)Congestive
heart failure
Therapeuticuses
-
8/2/2019 Antianginal student222
16/69
Precautions:
1. 8-10 hours nitrate free period
2. Never stop nitrate therapy suddenly
3. Do not take double dose
4. Do not use after expiry date.
Side effects:
1. Postural hypotension
&reflex tachycardia .
2. Flushing
3. Throbbing headache
4. Visual disturbance
5. Drug rash
6. Nitrate Tolerance
Side Effects
andPrecaution
s
-
8/2/2019 Antianginal student222
17/69
Drug interaction :Drug interaction :
Sever hypotension if SildenafilSever hypotension if Sildenafil
(a potent PDEI )is given with(a potent PDEI )is given with
nitrates .nitrates .
-
8/2/2019 Antianginal student222
18/69
CALCIUM CHANNELCALCIUM CHANNEL
BLOCKERS:BLOCKERS: 1-Non-dihydropyridines.1-Non-dihydropyridines.
2-Dihydropyridines.2-Dihydropyridines.
-
8/2/2019 Antianginal student222
19/69
Block calcium channels in the
cardiac muscles and smooth muscle
calcium influxdecreasecardiac contractility and VSM
relaxation.
Calcium channel blockersCalcium channel blockers
What is their mechanism ofWhat is their mechanism of
action?action?
-
8/2/2019 Antianginal student222
20/69
non dihydropyridines e.g.non dihydropyridines e.g.
verapamil&diltiazem .verapamil&diltiazem .
1-1- They have mainly cardiac effect.They have mainly cardiac effect. They cause increase of coronary flow asThey cause increase of coronary flow as
they cause coronary dilatation .they cause coronary dilatation .
They decrease myocardial oxygen demandThey decrease myocardial oxygen demandby decreasing cardiac work through their by decreasing cardiac work through their ve inotropic & chronotropic effects .ve inotropic & chronotropic effects .
2-They have reduced vasodilator effect2-They have reduced vasodilator effect( less reflex tachycardia suitable for( less reflex tachycardia suitable forhypotensive patient .hypotensive patient .
-
8/2/2019 Antianginal student222
21/69
The dihydropyridines e.g.The dihydropyridines e.g.
NIEDIPINE (LA) & AMLODIPINE .NIEDIPINE (LA) & AMLODIPINE .
They have mainly vascularThey have mainly vasculareffect :effect :
1- They cause dilation of coronary1- They cause dilation of coronary
artery so prevent or relief coronaryartery so prevent or relief coronary
vasospasm, and improve myocardialvasospasm, and improve myocardialblood flow .blood flow .
2- They cause arteriolar dilation so2- They cause arteriolar dilation so
decreasing PR &cardiac work.decreasing PR &cardiac work.
3-They have reduced ve inotropic &3-They have reduced ve inotropic &
-ve chronotropic effect on the heart .-ve chronotropic effect on the heart .
-
8/2/2019 Antianginal student222
22/69
CCBsCCBs
Mechanism of anti-ischemic actionMechanism of anti-ischemic action
arteriolar vascular resistance afterloadmyocardial contracti l i ty & heart ratewith the use of verapamil and dilt iazem
2.CCBs dilate the large epicardial vessels
3. Prevent focal coronary artery spasmprimary cause of variant angin
-
8/2/2019 Antianginal student222
23/69
-
8/2/2019 Antianginal student222
24/69
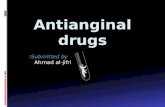
What is the role of CCB in the
treatment of angina?
myocardial oxygen demandarteriolar vascular resistance afterload myocardial contracti l i ty & heart ratewith the use of verapamil and di lt iazem
myocardial oxygen supplycoronary di latation
-
8/2/2019 Antianginal student222
25/69
AMLODIPINE :AMLODIPINE :
1- It is a long acting CCB.1- It is a long acting CCB.
2-It is slowly but completely2-It is slowly but completely
absorbed from GIT .absorbed from GIT .
3-Has very long half life of about3-Has very long half life of about
1 -2-days .1 -2-days .
4- Reduces the ABP gradually &4- Reduces the ABP gradually &causes little reflex tachycardia .causes little reflex tachycardia .
-
8/2/2019 Antianginal student222
26/69
Therapeutic causes of CCB .Therapeutic causes of CCB .
1-Vasospastic angina .1-Vasospastic angina .
2-Stable angina alone or in2-Stable angina alone or in
combination withcombination with blockers .blockers .
-
8/2/2019 Antianginal student222
27/69
BetaBetablocking drugsblocking drugs
Mechanism of anti-ischemic actionMechanism of anti-ischemic action
1. Heart Rate ( resting &
exercise HR)
2. Force of contraction
3. Blood pressure
A.. Myocardial oxygen demands
B. Perfusion of ischemic areas by
prolongation of diastole
-
8/2/2019 Antianginal student222
28/69
-Adrenergic antagonists
Selective (preferred)
Atenolol 50-100 mg / day
Bisoprolol 5-10 mg / day
Metoprolol S.R. 200 mg/
day
Non selective(not used
)due to their B2 action.
propranolol
-
8/2/2019 Antianginal student222
29/69
1- Combination of B Blockers with nitrates and
nifedipine to 1- increase the efficiency 2-decrease the
dose of each drug 3- block the reflex tachycardia that
occurs with theses drugs. (good combination)
2- Combination of B-blockers and verapamil is a bad
combination, as it will potentiate the negative
inotropic effect of verapamil which may lead to heartblock. (bad combination )
COMBINATION OF ANTIANGINAL DRUGS:COMBINATION OF ANTIANGINAL DRUGS:
VD
VD
-
8/2/2019 Antianginal student222
30/69
NitratesCoronary Vessels
(O2 supply)
CCB
Heart
(O2 demand) HR&Contractility
BlockersCCB
BlockersCCB
NitratesNitrates
VD
AfterloadPreload
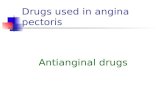
Effect of Anti-anginal drugs on myocardial O2 supply
and work done by the heart (O2 demand)
1. VD epicardial coronaries
2. Redistribution to ischemic areas
3. VD collaterals
VD
-
8/2/2019 Antianginal student222
31/69
Antiplatelet DrugsAntiplatelet Drugs
Aspirin:Aspirin:
AspirinAspirin irreversibly inhibit COXirreversibly inhibit COX (up to(up tothe life-time of the platelets 8-10 days).the life-time of the platelets 8-10 days).
Both PGIBoth PGI22 and TXAand TXA22 synthesis aresynthesis are
inhibited.inhibited.
Aspirin inAspirin in small dose 75-100 mg/daysmall dose 75-100 mg/day
inhibits TXAinhibits TXA22 synthesis withoutsynthesis without
significant effect on the endothelialsignificant effect on the endothelial
PGIPGI22.. A/E: peptic ulcerA/E: peptic ulcerbleeding in patients >bleeding in patients >
60 years.60 years.
U f ti l t l dUses of antiplatele drugs:
-
8/2/2019 Antianginal student222
32/69
Uses of antiplatele drugs:Uses of antiplatele drugs:
They are used in patient at highThey are used in patient at high
risk e.g.risk e.g.
after angina pectoris, MI, atheromaafter angina pectoris, MI, atheroma
oror
prothetic valvesprothetic valves to protect against:to protect against: Stroke,Stroke,
MIMI
or deathor death
-
8/2/2019 Antianginal student222
33/69
ASPIRINASPIRIN
It must be given to all cases ofIt must be given to all cases ofangina . In low doses 70 -150angina . In low doses 70 -150mg /day it will decrease plateletmg /day it will decrease platelet
aggregation .aggregation . N.B. Loading dose is sometimesN.B. Loading dose is sometimes
required for a rapid onset ofrequired for a rapid onset ofeffect ,chewed beforeeffect ,chewed beforeswallowing to aid earlyswallowing to aid earlyabsorption .absorption .
-
8/2/2019 Antianginal student222
34/69
VASOSPASTIC OR VARIENTVASOSPASTIC OR VARIENT
ANGINA .ANGINA .
In vasospastic angina :In vasospastic angina :
Nitates , CCB are the drugs ofNitates , CCB are the drugs ofchoice .choice .
-
8/2/2019 Antianginal student222
35/69
Unstable anginaUnstable angina
-
8/2/2019 Antianginal student222
36/69
UASTABLE ANGINA .UASTABLE ANGINA .
Better transfer to ICU or CCU.Better transfer to ICU or CCU. MMORPHIE-ORPHIE-OOXYGEN-XYGEN-NNG-G-AASPIRINE.SPIRINE. AspirinAspirin as loading dose (150 -300 mg )as loading dose (150 -300 mg )
then small daily dose (75-150 mg/day ) .then small daily dose (75-150 mg/day ) .
The addition of other anti plateletThe addition of other anti platelet e.g.e.g.ClopidogrelClopidogrelto aspirin is moreto aspirin is moreeffectiveeffective ..
Full anticoagulationFull anticoagulation with heparinwith heparinproduces additive benefit .produces additive benefit .
AA adrenergic antagonistadrenergic antagoniste.g.Metoprolol is first choice anti-e.g.Metoprolol is first choice anti-anginl drugs .anginl drugs .
-
8/2/2019 Antianginal student222
37/69
-
8/2/2019 Antianginal student222
38/69
Myocardial infarction .Myocardial infarction .
1-Acute management .1-Acute management .
Aim of therapy :Aim of therapy :
1-Pain relief .1-Pain relief .
2-Reperfusion of occluded artery . So drugs2-Reperfusion of occluded artery . So drugs
will include :will include : Analgesics e.g. Diamorphine 2.5 -5 mg IV .Analgesics e.g. Diamorphine 2.5 -5 mg IV .
SL nitrates (3 doses of nitroglycerine withSL nitrates (3 doses of nitroglycerine with5m intervals) or IV nitrates .5m intervals) or IV nitrates .
Aspirin 150- 300 mg orally (loading dose )Aspirin 150- 300 mg orally (loading dose ) .Continue with Aspirin in small dose 75-150.Continue with Aspirin in small dose 75-150
mg/ day .mg/ day . Oxygen 60% facemask inhalation .Oxygen 60% facemask inhalation .
-
8/2/2019 Antianginal student222
39/69
Thrombolytics :Thrombolytics : to induce clot lysis & restore bloodto induce clot lysis & restore blood
flow e.g. streptokinase .flow e.g. streptokinase .
Anti emetics.as myocardial patient suffer N &VAnti emetics.as myocardial patient suffer N &V
during acute attack of MI. e.g. Metoclopramideduring acute attack of MI. e.g. Metoclopramide
-adrenergic antagonists IV 4-6 h s after MI reduce-adrenergic antagonists IV 4-6 h s after MI reduce
the infarct size & mortality .the infarct size & mortality . If thrombolytics are contraindicated surgery isIf thrombolytics are contraindicated surgery is
indicated .indicated .
-
8/2/2019 Antianginal student222
40/69
Define the initial drug to
start with uponadmission:Morphine
Morphine
Define the initial drug to
start with uponadmission:
a-To alleviate the painPotent opiod analgesic that relives
severe pain.Has anxiolytic effect.Dilates veins leading to decreasedpulmonary venous congestion.
-
8/2/2019 Antianginal student222
41/69
Fibrinolytics Inhibitors (e.g.streptokinase) lyse thrombus occluding arteryleading to revasclarization, since attack is within 1hr.
B-to stop progression ofetiopathological cause
Chewable aspirin 160 mg: because ofits antiplatelet effect .
Oxygen and IV fluids.Nitroglycerine IV infusion.
Anticoagulants, e.g. heparin.
Beta blockers reduce the infarct size.
-
8/2/2019 Antianginal student222
42/69
Myocardial infarction .Myocardial infarction .
Secondary prophylaxis .Secondary prophylaxis .
Aim of therapy is to reduceAim of therapy is to reduce
mortality after MI .mortality after MI .
Stop smoking .Stop smoking .
Low dose aspirin 75-150 mg/Low dose aspirin 75-150 mg/
day reduces re occlusion ofday reduces re occlusion of
the vessels that undergoesthe vessels that undergoes
natural or therapeuticnatural or therapeutic
thrombolysis .thrombolysis .
-
8/2/2019 Antianginal student222
43/69
adrenergic receptor antagonist startedadrenergic receptor antagonist started
orally soon after the MI reduces later deathsorally soon after the MI reduces later deathsand re infarction .and re infarction .
ACEIs should be initiated within 24 hs after MI ,ACEIs should be initiated within 24 hs after MI ,
they prevent HF after MI .they prevent HF after MI . Long term anticoagulant with warfarin reducesLong term anticoagulant with warfarin reduces
mortality & reinfarction .mortality & reinfarction .
Cholesterol reduction .Cholesterol reduction .
-
8/2/2019 Antianginal student222
44/69
Identify whether or notthere is a place for ACE
inhibitors.
To avoid
post MIcardiacremodeli
ng
YES
If the patient is proved to be
-
8/2/2019 Antianginal student222
45/69
If the patient is proved to behypertensive.
Suggest whether there is a place for CCBs. Explain yourreasons.Nondihydropyrines have no placebecause of their negative inotropiceffects.l l dihydropyridines have no place because of theirvasodilatory effect-induced reflex tachycardia.(EXCEPTlong acting e.g. amlodipine which can be used becausebeing long acting they do not induce reflex tachycardia.
When the patient is discharged after
-
8/2/2019 Antianginal student222
46/69
When the patient is discharged afterbeing controlled
Enumerate the drugs that the patienthas to continue on , to preventoccurrence of a second attack.
-
8/2/2019 Antianginal student222
47/69
Oralanticoagulants,e.g.warfarin
Hypocholesterolomic drugs ,e.g.statinsAvoid smoking.
Control diet.
ACEIs orARBsBeta blockers
Nitrates, e.g.isosorbidedinitrateAntiplatelets,e.g.
aspirin
-
8/2/2019 Antianginal student222
48/69
AngioplastyAngioplasty
-
8/2/2019 Antianginal student222
49/69
CABGCABG
-
8/2/2019 Antianginal student222
50/69
Selection
Drug in concomitant diseases
L.N. Nitrates Blockers C.C.Blockers
1. None
2. Recent M.I.
3. Asthma COPD
4. Hypertension
5. Diabetes
x x x x
-
8/2/2019 Antianginal student222
51/69
Case Study 1
1- A 56 year old patient C/O effort chest pain, he is
diagnosed as atherosclerotic angina and prescribed SL NG
for treatment of acute chest pain. Which of the following
adverse effects is likely to be experienced by the patient:
a) Hypertension
c) Bradycardia
b) Throbbing Headache
d) Sexual dysfunction
Correct Answer = b)
NG Causes Throbbing Headache in 30%-60% of Patients
C S d 1 ( C )
-
8/2/2019 Antianginal student222
52/69
Case Study 1. ( Cont.)
The patient is also prescribed metoprolol to prevent
episodes of angina, The B-blocker has the added benefit of
preventing which of the following side effects of SL NG ?
a) Dizziness
c) Throbbing Headache
b) Methemoglobinemia
d) Reflex tachycardia
Correct Answer = d)
NG Causes Reflex tachycardia due to its vasodilatation.
-
8/2/2019 Antianginal student222
53/69
Case Study 2
A 68 year old patient was successfully treated for exercise
induced angina for several years. Recently he has CO of
chest pain at night. Which of the following drugs will be
useful in preventing this patients nocturnal angina?
c) Nitroglycerin (transdermal)
b) Nitroglycerin (SL)
d) Propranolol
a) Hydralazine
Correct Answer = C)
Transdermal NG sustains blood level for 24 hours
MCQ
-
8/2/2019 Antianginal student222
54/69
MCQs:
1- Metoprolol decrease the anginal attacks by the following
mechanisms except:
a) Decrease myocardial contractility
c) Dilates coronary blood vessels
b) Decrease heart rate
d) Decrease the arterial blood pressure
Correct Answer = C)
Metoprolol is not coronary vasodilator
MCQ
-
8/2/2019 Antianginal student222
55/69
MCQs:2- Which of the following drugs is considered to be most
effective in relieving & preventing ischemic episodes inpatients with variant angina?
a)Metoprolol
c) Sodium Nitroprusside
b) Nitroglycerine
d) Amlodepine (Nifedipine)
Amlodepine
-
8/2/2019 Antianginal student222
56/69
I-MENTION
A-Why the combined use of beta blockers
and nitrates can be very effective in
treatment of typical angina?
This combination is a useful combination because:
The two effects of the drugs synergize , allowing lower
doses of each drug to be used. Beta blockers decrease the
rate and force of contraction and nitrates decrease
cardiac preload and afterload ;both . Myocardial O2consumption.
The compensatory sympathetic reflexes produced by
nitrates are inhibited by beta blockers.
-
8/2/2019 Antianginal student222
57/69
I-MENTION c-Drug of choice in treatment of hypertension and
ischemic heart disease
Beta blockers: Treat both hypertension (by its
antihypertensive effects) and IHD( by its antianginal
effects).
-
8/2/2019 Antianginal student222
58/69
5-Match the following antianginals to their
mechanism of action:
1.Glyceryl trinitrate a-By decreasing sympathetic tone to the heart
2. Propranolol. B.By reducing cardiac work load.3. Verapamil. C.By inhibiting uptake of Ca by myocardial cells
1.Glyceryl trinitrate(b) a-By decreasing sympathetic tone to the hear
2. Propranolol. ( a) b.By reducing cardiac work load.
3. Verapamil. (c) c.By inhibiting uptake of Ca by myocardial cel
-
8/2/2019 Antianginal student222
59/69
7.All of the following statements concerning
nitroglycerine are correct EXCEPT:a. It causes elevation of intracellular cGMP.
b. It causes significant first pass metabolism in
the liver.
c. It may cause reflex tachycardia.
d.It significantly decreases AV conduction.
e-It can cause postural hypotension.
-
8/2/2019 Antianginal student222
60/69
V-MARK TRUE (T) OR FALSE (F)and correct the false1. All organic nitrate esters undergo significant
renal excretion which accounts for their short
half lives.
2.Isosorbide dinitrate is a fully nitrated compound,
which can be metabolized to an activ
metabolite.
3.Development of tolerance to the organic nitrates
can be avoided by intermittent therapy.
4.Typical angina is usually not associated with
atherosclerosis.
F undergo significant hepatic metabolism
T
T
Fis usually associated
-
8/2/2019 Antianginal student222
61/69
V-MARK TRUE (T) OR FALSE (F)and correct the false5. The vasodilatory effects of organic nitrates are
greater in arterioles than in veins.
6.Abrupt withdrawal from long term nitrate therapy
can lead to myocardial ischemia, infarction or
death.
7.Beta blockers are especially effective in
vasospastic angina.
8.Organic nitrates decrease oxygen demand of the
heart by their direct negative inotropic and
chronotropic effects .
Fgreater in veins than arteriole
T
Fcontraindicated in vasospastic angi
F decrease oxygen demand of heart by indirect
-
8/2/2019 Antianginal student222
62/69
VI.Choose the correct answer:
1-All of the following statements describing the
cardiovascular effects of organic nitrates are
true EXCEPT :a-They reduce myocardial work by decreasing preload
and afterload.
b.They selectively dilate large epicardial vessels
without impairment of autoregulation in smal
vessels.c.They are effective in relieving all three types of
angina.
d.They directly alter the inotropic and chronotropic
state of the heart.
-
8/2/2019 Antianginal student222
63/69
Choose the correct answer:
2-All of the following are rational drug
combinations for the treatment of typical
angina EXCEPT :a-Nitroglycerine and nifedipine.
b.Verapamil and propranolol.
c.Nitroglycerine and propranolol.
d. Nifedipine and propranolol.
-
8/2/2019 Antianginal student222
64/69
Choose the correct answer:
3-All of the following statements regarding the
mechanism of action of organic nitrates in
vascular smooth muscles are true EXCEPT :a-They lead to generation of nitrous oxide(N2O).
b.Activation of guanylate cyclase eventually occurs.
c.Cellular calcium concentrations are decreased.
d. Concentrations of cGMP are increased.
-
8/2/2019 Antianginal student222
65/69
Choose the correct answer:
4-All of the following statements regarding
antianginal agents are true EXCEPT :a-Calcium channel blockers dilate arterioles more
than veins.
b.Organic nitrates decrease calcium levels in smoothmuscles cells by decreasing their cGMP levels.
c.Beta blockers are effective in treating exertional
angina by decreasing cardiac O2 demand.d. Nifedipine can aggravate angina as a result of its
reflex inotropic & chronotropic effects.
-
8/2/2019 Antianginal student222
66/69
Choose the correct answer:
10-Side effects common to calcium channel
blockers include all of the following EXCEPT :
a-Dizziness and flushing .
b.Worsening of myocardial ischemia.
c.Tachycardia.
d.Excessive vasodilatation.
e.Diarrhoea.
-
8/2/2019 Antianginal student222
67/69
Choose the correct answer:
11-Effective administration route of
nitroglycerine for angina pectoris include all
of the following EXCEPT :
a-Transdermal .
b.Rectal.
c.Sublingual.
d.Intravenous.
e.Oral.
-
8/2/2019 Antianginal student222
68/69
Choose the correct answer:
12-In the treatment of angina pectoris :
a-Beta adrenergic antagonists provide effective
vasodilatation .
b.propranolol is the only beta blocker that is
therapeutically effective.
c. Beta adrenergic antagonists are most effective in
vasospastic angina.
d. Beta adrenergic antagonists withdrawal may causemyocardial infarction.
e.The combination of organic nitrates and beta
adrenergic antagonists is contraindicated.
-
8/2/2019 Antianginal student222
69/69
Good Luck