
Antiandrogen Therapy with Hydroxyflutamide or...
10
Small Molecule Therapeutics Antiandrogen Therapy with Hydroxyflutamide or Androgen Receptor Degradation Enhancer ASC- J9 Enhances BCG Efficacy to Better Suppress Bladder Cancer Progression Zhiqun Shang 1,2 , Yanjun Li 1 , Minghao Zhang 1,3 , Jing Tian 1,2 , Ruifa Han 1 , Chih-Rong Shyr 1 , Edward Messing 2 , Shuyuan Yeh 1,2 , Yuanjie Niu 1,2 , and Chawnshang Chang 1,2,4 Abstract Recent studies suggest that the androgen receptor (AR) might play important roles in influencing bladder cancer progression, yet its clinical application remains unclear. Here, we developed a new combined therapy with Bacillus Calm- ette–Gu erin (BCG) and the AR degradation enhancer ASC-J9 or antiandrogen hydroxyflutamide (HF) to better suppress bladder cancer progression. Mechanism dissection revealed that ASC-J9 treatment enhanced BCG efficacy to suppress bladder cancer cell proliferation via increasing the recruitment of monocytes/macrophages that involved the promotion of BCG attachment/internalization to the bladder cancer cells through increased integrin-a5b1 expression and IL6 release. Such consequences might then enhance BCG-induced bladder cancer cell death via increased TNFa release. Interestingly, we also found that ASC-J9 treatment could directly promote BCG-induced HMGB1 release to enhance the BCG cytotoxic effects for suppression of bladder cancer cell growth. In vivo approaches also concluded that ASC-J9 could enhance the efficacy of BCG to better suppress bladder cancer progression in BBN-induced bladder cancer mouse models. Together, these results suggest that the newly developed therapy combining BCG plus ASC-J9 may become a novel therapy to better suppress bladder cancer progress. Mol Cancer Ther; 14(11); 2586–94. Ó2015 AACR. Introduction Bladder cancer has a high mortality with an estimated 74,690 new cases and 15,580 deaths in United States in 2014 (1). Most bladder cancer patients receive the complete transurethral resec- tion of their tumor followed by intravesical instillation of anti- tumor agents, including Bacillus Calmette–Guerin (BCG) that represents a very successful adjuvant agent for treating noninva- sive bladder cancer (2, 3). However, the BCG therapy still has its limitations: Approximately 30% of patients treated with intrave- sical BCG failed to respond, and for those patients with initial positive response, many suffered the high rate of recurrence (4). Recently, significant progress has been made toward understand- ing the mechanism of BCG antitumor response. With respect to the local response to BCG, accumulating data support a critical role for BCG–tumor interaction in initiating and directing the downstream antitumor response. By the combination of local effects and a systemic immune response, BCG therapy might have a remarkable antitumor effect. Interestingly, a recent study suggested the potential linkage of androgen receptor (AR) with bladder cancer initiation and pro- gression (5), and another study also indicated that androgens might be able to modulate IL6 to alter BCG interaction with bladder cancer cells (6). Here, we found a new potential therapy with combination of BCG and antiandrogen hydroxyflutamide (HF) or AR degradation enhancer ASC-J9 better suppressed bladder cancer progression (7–9). Materials and Methods Reagents The compound ASC-J9 was a gift from AndroScience Corp. BCG, a lyophilized preparation containing 10.5 8.7 10 8 colony-forming units (CFU), was resuspended in PBS. HF was obtained from Sigma. Polyclonal antibodies against F4/80 and integrin-a5b1 were from Abcam and bromodeoxyuridine (BrdUrd) was from BD Biosciences. The liquid DAB þ substrate chromogen system horseradish peroxidase used for immunocy- tochemistry was obtained from Dako Cytomation. Penicillin, 1 Chawnshang Chang Sex Hormone Research Center, Tianjin Institute of Urology, The 2nd Hospital of Tianjin Medical University, Tianjin, China. 2 George Whipple Laboratory for Cancer Research, Depart- ments of Pathology, Urology, Radiation Oncology, and The Wilmot Cancer Center, University of Rochester Medical Center, Rochester, New York. 3 Department of Urology, Tianjin Third Central Hospital, Tianjin, China. 4 Sex Hormone Research Center, China Medical Univer- sity/Hospital, Taichung, Taiwan. Note: Supplementary data for this article are available at Molecular Cancer Therapeutics Online (http://mct.aacrjournals.org/). Corresponding Authors: Chawnshang Chang, University of Rochester Medical Center, 601 Elmwood Avenue, Box 626, Rochester, NY 14642. Phone: 585-275- 9994; Fax: 585-756-4133; E-mail [email protected]; and Yuanjie Niu, Tianjin Institute of Urology, The Second Hospital of Tianjin Medical University, Tianjin, 300211, China, [email protected] doi: 10.1158/1535-7163.MCT-14-1055-T Ó2015 American Association for Cancer Research. Molecular Cancer Therapeutics Mol Cancer Ther; 14(11) November 2015 2586 on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T
Transcript of Antiandrogen Therapy with Hydroxyflutamide or...

Small Molecule Therapeutics
Antiandrogen Therapy with Hydroxyflutamide orAndrogen Receptor Degradation Enhancer ASC-J9 Enhances BCG Efficacy to Better SuppressBladder Cancer ProgressionZhiqun Shang1,2, Yanjun Li1, Minghao Zhang1,3, Jing Tian1,2, Ruifa Han1,Chih-Rong Shyr1, Edward Messing2, Shuyuan Yeh1,2, Yuanjie Niu1,2, andChawnshang Chang1,2,4
Abstract
Recent studies suggest that the androgen receptor (AR)might play important roles in influencing bladder cancerprogression, yet its clinical application remains unclear. Here,we developed a new combined therapy with Bacillus Calm-ette–Gu�erin (BCG) and the AR degradation enhancer ASC-J9or antiandrogen hydroxyflutamide (HF) to better suppressbladder cancer progression. Mechanism dissection revealedthat ASC-J9 treatment enhanced BCG efficacy to suppressbladder cancer cell proliferation via increasing the recruitmentof monocytes/macrophages that involved the promotion ofBCG attachment/internalization to the bladder cancer cellsthrough increased integrin-a5b1 expression and IL6 release.
Such consequences might then enhance BCG-induced bladdercancer cell death via increased TNFa release. Interestingly, wealso found that ASC-J9 treatment could directly promoteBCG-induced HMGB1 release to enhance the BCG cytotoxiceffects for suppression of bladder cancer cell growth. In vivoapproaches also concluded that ASC-J9 could enhance theefficacy of BCG to better suppress bladder cancer progressionin BBN-induced bladder cancer mouse models. Together,these results suggest that the newly developed therapycombining BCG plus ASC-J9 may become a novel therapy tobetter suppress bladder cancer progress. Mol Cancer Ther; 14(11);2586–94. �2015 AACR.
IntroductionBladder cancer has a high mortality with an estimated 74,690
new cases and 15,580 deaths in United States in 2014 (1). Mostbladder cancer patients receive the complete transurethral resec-tion of their tumor followed by intravesical instillation of anti-tumor agents, including Bacillus Calmette–Guerin (BCG) thatrepresents a very successful adjuvant agent for treating noninva-sive bladder cancer (2, 3). However, the BCG therapy still has itslimitations: Approximately 30% of patients treated with intrave-sical BCG failed to respond, and for those patients with initial
positive response, many suffered the high rate of recurrence (4).Recently, significant progress has been made toward understand-ing the mechanism of BCG antitumor response. With respect tothe local response to BCG, accumulating data support a criticalrole for BCG–tumor interaction in initiating and directing thedownstream antitumor response. By the combination of localeffects and a systemic immune response, BCG therapymight havea remarkable antitumor effect.
Interestingly, a recent study suggested the potential linkage ofandrogen receptor (AR) with bladder cancer initiation and pro-gression (5), and another study also indicated that androgensmight be able to modulate IL6 to alter BCG interaction withbladder cancer cells (6).
Here, we found a new potential therapy with combination ofBCGand antiandrogenhydroxyflutamide (HF) or ARdegradationenhancer ASC-J9 better suppressed bladder cancer progression(7–9).
Materials and MethodsReagents
The compound ASC-J9 was a gift from AndroScience Corp.BCG, a lyophilized preparation containing 10.5 � 8.7 � 108
colony-forming units (CFU), was resuspended in PBS. HF wasobtained from Sigma. Polyclonal antibodies against F4/80 andintegrin-a5b1 were from Abcam and bromodeoxyuridine(BrdUrd) was from BD Biosciences. The liquid DABþ substratechromogen system horseradish peroxidase used for immunocy-tochemistry was obtained from Dako Cytomation. Penicillin,
1Chawnshang Chang Sex Hormone Research Center, Tianjin Instituteof Urology, The 2nd Hospital of Tianjin Medical University, Tianjin,China. 2George Whipple Laboratory for Cancer Research, Depart-ments of Pathology, Urology, Radiation Oncology, and The WilmotCancer Center, University of Rochester Medical Center, Rochester,New York. 3Department of Urology, Tianjin Third Central Hospital,Tianjin, China. 4Sex Hormone Research Center, China Medical Univer-sity/Hospital, Taichung, Taiwan.
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Corresponding Authors: Chawnshang Chang, University of Rochester MedicalCenter, 601 Elmwood Avenue, Box 626, Rochester, NY 14642. Phone: 585-275-9994; Fax: 585-756-4133; E-mail [email protected]; and Yuanjie Niu,Tianjin Institute of Urology, The Second Hospital of Tianjin Medical University,Tianjin, 300211, China, [email protected]
doi: 10.1158/1535-7163.MCT-14-1055-T
�2015 American Association for Cancer Research.
MolecularCancerTherapeutics
Mol Cancer Ther; 14(11) November 20152586
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

streptomycin, all media, and FBS were obtained from Invitrogen.Tris, glycine, NaCl, SDS, BSA, and monoclonal antibody againstb-actin were obtained from Sigma.
Cell lines and culture conditionsThe T24 cell line was a gift from Dr. Timothy Ratliff (Depart-
ment of Urology, University of Iowa, Iowa City, IA) in 2009 andcultured in Hyclone McCoy's 5A media supplemented with 10%FBS. The human bladder cancer cell line 253J was generouslyprovided by Dr. Colin P.N. Dinney, The University of Texas(Houston, TX) in 2010 and cultured in T media supplementedwith 10% FBS. The MB49 cell line was a gift from Dr. Ron Wood,University of Rochester Medical Center (Rochester, NY) in 2009.The human THP-1 cell line was obtained from the ATCC inSeptember 10, 2009, and cultured in RPMI-1640 supplementedwith 10% FBS, vitamins, sodium pyruvate, L-glutamine, nones-sential amino acids, and penicillin–streptomycin. All cell lineswere authenticated and tested by PCR when we received them,and then were expanded and frozen down in several aliquots.Each aliquot was thawed and used for no more than 6 months.
AnimalsFVB femalemousewere obtained fromThe Jackson Laboratory.
The animals were housed four per cage in a specific pathogen-freeanimal facility and fed with regular chow diet with water adlibitum. Animal protocols/usage was approved by the Universityof Rochester Committee on Animal Resources, and the mice werekept in a specific pathogen-free environment at the animal facil-ities of the University of Rochester Medical Center.
DNA extraction, RNA extraction, RT-PCR, and quantitative real-time PCR
For RT-PCR, 1 mg of total RNAs was reverse-transcribed usingthe iScript Synthesis Kit (Bio-Rad Laboratories), according to themanufacturer's protocol. The sequence of primers used in the PCRRT-PCR and qPCRwere as followed: Human b-actin: 50-ATC TGGCAC CAC ACC TTC TA-30 (sense) and 50-CGT CAT ACT CCT GCTTGC TG-30 (antisense); human GAPDH: 50-GCT CTC CAG AACATC ATC C-30 (sense) and 50-TGC TTC ACC ACC TTC TTG-30
(antisense); human integrin-a5 50-CCT GGC TGG CTG GTA TTAGC-30 (sense) and 50-GTC GGG GGC TTC AAC TTA GAC-30
(antisense); human integrin-b1: 50-TTA TTG GCC TTG GAT TACTGC T-30 (sense) and 50-CCA CAG TTG TTA CGG CAC TCT-30
(antisense); BCG: 50-CCTGCGAGCGTAGGCGTCGG-30 (sense)and 50-CTC GTC CAG CGC CGC TTC GG-30 (antisense); humanIL6: 50-AAGCCAGAGCTG TGCAGA TGAGTA-30 (sense) and 50-TGT CCT GCA GCC ACT GGT TC-30 (antisense).
MTT assayThe antiproliferative effects of HF and ASC-J9 on BCG against
bladder cancer cell lines 253J and T24 were determined by theMTT dye uptake method.
BCG attachment and internalization assayWe used PCR to detect BCG internalization and attachment to
bladder cancer cells. After incubation and washing out nonat-tached, excess BCG, the cells monolayer was washed twice withHanks BSS (Gibco). Cells were then harvested using Cell Disas-sociation Solution (Sigma). Genomic DNA was extracted accord-ing to procedure of the Dneasy Blood and Tissue Kit (QiaGen).The bladder cancer cell lines were each plated at a density of 105
cells perwell in 6-well plates (Costar) andpretreatedwith 5 mmol/L ASC-J9 orHF, then incubated at 37�C in complete culturemediaovernight. The following day 5� 106 CFUBCGwas added to eachwell, and placed at 37�C for 2 hours. At the time points indicated,the culture media with nonattached BCG was aspirated and thecell monolayer washed twice with Hanks BSS (Gibco). Cells werethenharvested usingCellDisassociation Solution (Sigma). Paren-tal 253J and T24 cells were incubated with a concentration of 50CFU BCG per cell for 2 hours and compared with the negativethreshold. Tests were performed in duplicate and repeated on asubsequent day.
Migration assayA total of 5 � 104 bladder cancer cells were seeded into the
bottom well (5-mm pore size Transwell; Corning Incorporated)treated withHF and ASC-J9 for 12 hours and treated with BCG for2 hours. Then the excess BCG was removed and 4 � 105 THP-1cells placed into the upper Transwell, incubated for 2 hours, thenwe collected the THP-1 cells migrated into the bottom wells forcounting.
N-butyl-N-(4-hydroxybutyl) nitrosamine (BBN)–inducedmouse bladder cancer model
Twelve-weeks-old FVB female mice (The Jackson Laboratory)were supplied ad libitumwith sterile water containing 0.05% BBN(TCI America) in opaque bottles for 12 weeks, and thereafter withsterile water without BBN. The drinking water was prepared freshtwice a week, and consumption was recorded to estimate BBNintake. Then mice were divided into 4 groups (10 mice/group) assoon as urine blood tested positive, and treated with (i) ETOH-control, (ii) BCG (2 � 106 CFU/mouse, intravesical injectionweekly) alone, (iii) ASC-J9 (75 mg/kg body weight, every otherday, IP) alone, and (iv) BCG (2 � 106 CFU/mouse, intravesicalinjection weekly)þASC-J9 (75 mg/kg body weight, every otherday, IP). Mice were then sacrificed 48 hours after the fourthtreatment and bladders were collected for further examination.
Immunohistochemical analysis for F4/80, andBrdUrd in tumortissues
The expressions of F4/80 and BrdUrd were evaluated using animmunohistochemical method described previously (10). Theantibodies used were anti-F4/80 (Abcam) and anti-BrdUrd (BDBiosciences). Results were expressed as the percentage � SE ofpositive cells per �200 magnification field. A total of 5 � 200fields was examined and counted from each group.
Statistical analysisData are presented asmean� SEMof at least three independent
biologic replicates. The values were compared using a Student ttest (two-tailed). We considered a P value inferior to 0.05 assignificant.
ResultsASC-J9 and HF enhance BCG attachment/internalization tobetter suppress bladder cancer cells
Early reports suggested that BCG was able to function throughattachment/internalization into bladder cancer urothelial cellsto alter the immune responses to exert its chemotherapeutic effect(11–13). Other studies also indicated that AR might play impor-tant roles to influence bladder cancer progression (5). We
ASC-J9 with BCG Therapy to Better Suppress Bladder Cancer
www.aacrjournals.org Mol Cancer Ther; 14(11) November 2015 2587
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T
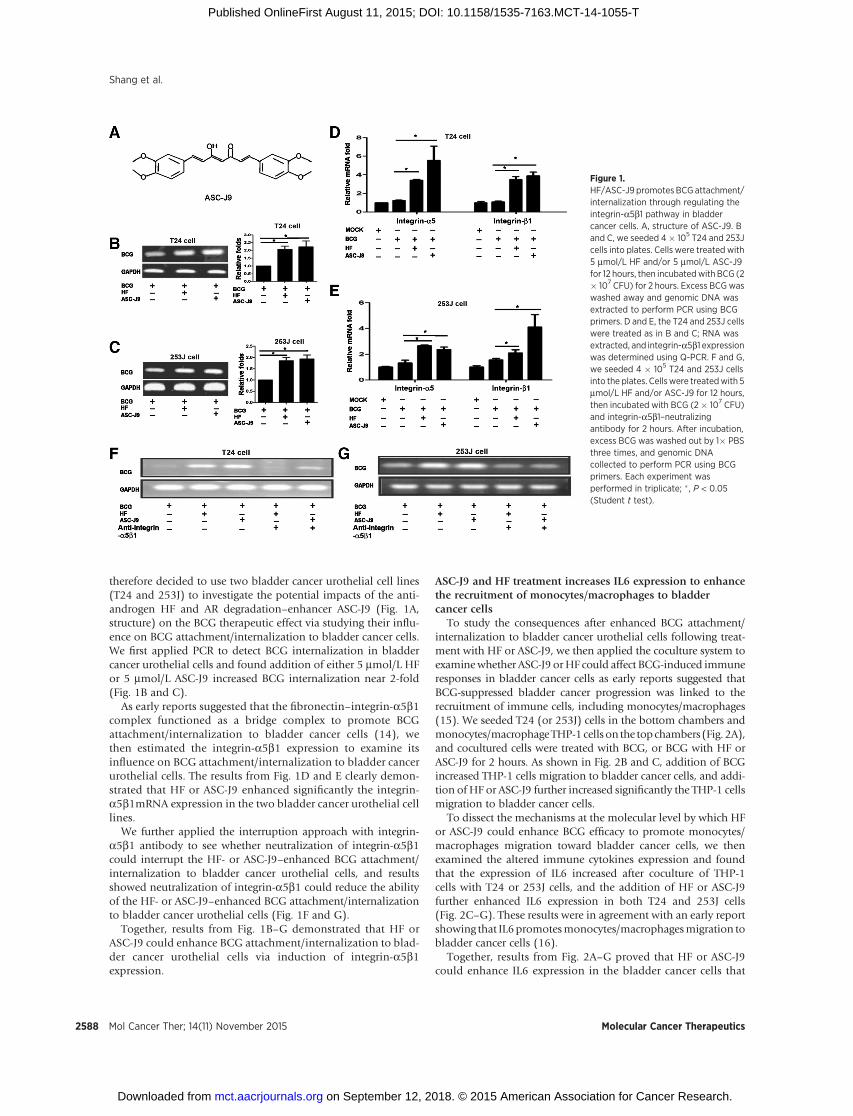
therefore decided to use two bladder cancer urothelial cell lines(T24 and 253J) to investigate the potential impacts of the anti-androgen HF and AR degradation–enhancer ASC-J9 (Fig. 1A,structure) on the BCG therapeutic effect via studying their influ-ence on BCG attachment/internalization to bladder cancer cells.We first applied PCR to detect BCG internalization in bladdercancer urothelial cells and found addition of either 5 mmol/L HFor 5 mmol/L ASC-J9 increased BCG internalization near 2-fold(Fig. 1B and C).
As early reports suggested that the fibronectin–integrin-a5b1complex functioned as a bridge complex to promote BCGattachment/internalization to bladder cancer cells (14), wethen estimated the integrin-a5b1 expression to examine itsinfluence on BCG attachment/internalization to bladder cancerurothelial cells. The results from Fig. 1D and E clearly demon-strated that HF or ASC-J9 enhanced significantly the integrin-a5b1mRNA expression in the two bladder cancer urothelial celllines.
We further applied the interruption approach with integrin-a5b1 antibody to see whether neutralization of integrin-a5b1could interrupt the HF- or ASC-J9–enhanced BCG attachment/internalization to bladder cancer urothelial cells, and resultsshowed neutralization of integrin-a5b1 could reduce the abilityof the HF- or ASC-J9–enhanced BCG attachment/internalizationto bladder cancer urothelial cells (Fig. 1F and G).
Together, results from Fig. 1B–G demonstrated that HF orASC-J9 could enhance BCG attachment/internalization to blad-der cancer urothelial cells via induction of integrin-a5b1expression.
ASC-J9 and HF treatment increases IL6 expression to enhancethe recruitment of monocytes/macrophages to bladdercancer cells
To study the consequences after enhanced BCG attachment/internalization to bladder cancer urothelial cells following treat-ment with HF or ASC-J9, we then applied the coculture system toexaminewhether ASC-J9 orHF could affect BCG-induced immuneresponses in bladder cancer cells as early reports suggested thatBCG-suppressed bladder cancer progression was linked to therecruitment of immune cells, including monocytes/macrophages(15). We seeded T24 (or 253J) cells in the bottom chambers andmonocytes/macrophageTHP-1 cells on the topchambers (Fig. 2A),and cocultured cells were treated with BCG, or BCG with HF orASC-J9 for 2 hours. As shown in Fig. 2B and C, addition of BCGincreased THP-1 cells migration to bladder cancer cells, and addi-tion of HF or ASC-J9 further increased significantly the THP-1 cellsmigration to bladder cancer cells.
To dissect the mechanisms at the molecular level by which HFor ASC-J9 could enhance BCG efficacy to promote monocytes/macrophages migration toward bladder cancer cells, we thenexamined the altered immune cytokines expression and foundthat the expression of IL6 increased after coculture of THP-1cells with T24 or 253J cells, and the addition of HF or ASC-J9further enhanced IL6 expression in both T24 and 253J cells(Fig. 2C–G). These results were in agreement with an early reportshowing that IL6promotesmonocytes/macrophagesmigration tobladder cancer cells (16).
Together, results from Fig. 2A–G proved that HF or ASC-J9could enhance IL6 expression in the bladder cancer cells that
Figure 1.HF/ASC-J9 promotes BCG attachment/internalization through regulating theintegrin-a5b1 pathway in bladdercancer cells. A, structure of ASC-J9. Band C, we seeded 4� 105 T24 and 253Jcells into plates. Cells were treated with5 mmol/L HF and/or 5 mmol/L ASC-J9for 12 hours, then incubatedwith BCG (2� 107 CFU) for 2 hours. Excess BCGwaswashed away and genomic DNA wasextracted to perform PCR using BCGprimers. D and E, the T24 and 253J cellswere treated as in B and C; RNA wasextracted, and integrin-a5b1 expressionwas determined using Q-PCR. F and G,we seeded 4 � 105 T24 and 253J cellsinto the plates. Cellswere treatedwith 5mmol/L HF and/or ASC-J9 for 12 hours,then incubated with BCG (2� 107 CFU)and integrin-a5b1–neutralizingantibody for 2 hours. After incubation,excess BCG was washed out by 1� PBSthree times, and genomic DNAcollected to perform PCR using BCGprimers. Each experiment wasperformed in triplicate; � , P < 0.05(Student t test).
Shang et al.
Mol Cancer Ther; 14(11) November 2015 Molecular Cancer Therapeutics2588
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

recruits more monocytes/macrophages to the bladder cancercells.
More recruitedmonocytes/macrophages to bladder cancer cellsleads to more TNFa secretion to kill more bladder cancer cells
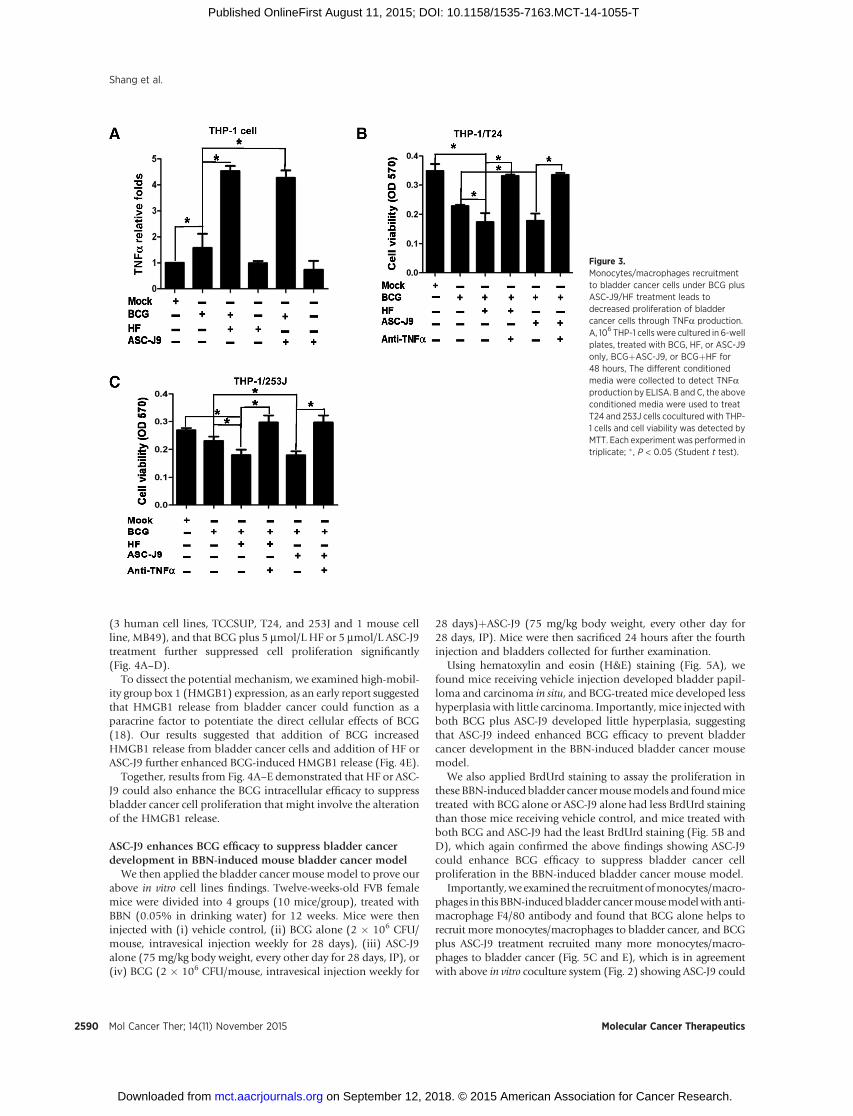
We then asked what are the impacts of recruiting moremonocytes/macrophages to bladder cancer cells. Early studiessuggested that BCG might function through recruitment ofmacrophages to suppress bladder cancer that involved therelease of soluble cytotoxic factors, including TNFa, IFNg , andnitous oxide (17). We first demonstrated that addition of BCGto the THP-1 cells released more TNFa compared with THP-1only and importantly, adding ASC-J9 or HF released even moreTNFa compared with BCG only (Fig. 3A). Importantly, aninterruption approach with addition of anti-TNFa antibodyalso interrupted monocytes/macrophages/BCG/HF– or mono-
cytes/macrophages/BCG/ASC-J9–induced bladder cancer cellviability (Fig. 3B and C).
Together, results from Fig. 3A–C suggest that HF- or ASC-J9–enhanced BCG efficacy to suppress more bladder cancer cellsmight function through recruitingmoremonocytes/macrophagesthat involve the increase of TNFa release.
ASC-J9 or HF enhances BCG efficacy to suppress bladder cancerprogression via high-mobility group box 1 release
In addition to enhancing BCG efficacy via recruitment of moremonocytes/macrophages to suppress bladder cancer cells, we alsoexamined the potential BCG direct intracellular cytotoxic effectafter attachment/internalization to bladder cancer urothelial cells.We first demonstrated that without coculture with THP-1 cells,BCG alone (for 2 hours in every 48 hours) could suppress bladdercancer cell proliferation in four different bladder cancer cell lines
Figure 2.HF/ASC-J9 promotes monocyte migration toward BCG-treated bladder cancer cells. A, a total of 5 � 104 bladdercancer cells were seeded into the bottom chambers ofTranswells and treated with HF or ASC-J9 for 12 hours, thenBCG was added and incubated for additional 2 hours. Afterwashing out excess BCG, 4� 105 THP-1 cells were added intothe top chambers and then coincubated with bladder cancercells for 2 hours. The media of bottom chambers werecollected to count themigrated THP1 cells. B and C, THP-1 cellmigration assays were done in T24 and 253J cells. Eachexperiment was performed in triplicate. D–G, HF and ASC-J9increased BCG-induced IL6 release from bladder cancer cells.We seeded 4 � 105 T24 and 253J cells into the plates. Cellswere treated with 5 mmol/L HF or 5 mmol/L ASC-J9 in thepresence of 10 nmol/L DHT for 12 hours, and then incubatedwith BCG (2 � 107 CFU) for 2 hours. After washing awayexcess BCG, mRNA was extracted from bladder cancer cellsto determine IL6 expression using Q-PCR. Each experimentwas performed in triplicate; � , P < 0.05 (Student t test).
ASC-J9 with BCG Therapy to Better Suppress Bladder Cancer
www.aacrjournals.org Mol Cancer Ther; 14(11) November 2015 2589
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T
(3 human cell lines, TCCSUP, T24, and 253J and 1 mouse cellline, MB49), and that BCG plus 5 mmol/L HF or 5 mmol/L ASC-J9treatment further suppressed cell proliferation significantly(Fig. 4A–D).
To dissect the potential mechanism, we examined high-mobil-ity group box 1 (HMGB1) expression, as an early report suggestedthat HMGB1 release from bladder cancer could function as aparacrine factor to potentiate the direct cellular effects of BCG(18). Our results suggested that addition of BCG increasedHMGB1 release from bladder cancer cells and addition of HF orASC-J9 further enhanced BCG-induced HMGB1 release (Fig. 4E).
Together, results from Fig. 4A–E demonstrated that HF or ASC-J9 could also enhance the BCG intracellular efficacy to suppressbladder cancer cell proliferation that might involve the alterationof the HMGB1 release.
ASC-J9 enhances BCG efficacy to suppress bladder cancerdevelopment in BBN-induced mouse bladder cancer model
We then applied the bladder cancer mouse model to prove ourabove in vitro cell lines findings. Twelve-weeks-old FVB femalemice were divided into 4 groups (10 mice/group), treated withBBN (0.05% in drinking water) for 12 weeks. Mice were theninjected with (i) vehicle control, (ii) BCG alone (2 � 106 CFU/mouse, intravesical injection weekly for 28 days), (iii) ASC-J9alone (75 mg/kg body weight, every other day for 28 days, IP), or(iv) BCG (2 � 106 CFU/mouse, intravesical injection weekly for
28 days)þASC-J9 (75 mg/kg body weight, every other day for28 days, IP). Mice were then sacrificed 24 hours after the fourthinjection and bladders collected for further examination.
Using hematoxylin and eosin (H&E) staining (Fig. 5A), wefound mice receiving vehicle injection developed bladder papil-loma and carcinoma in situ, and BCG-treated mice developed lesshyperplasia with little carcinoma. Importantly, mice injectedwithboth BCG plus ASC-J9 developed little hyperplasia, suggestingthat ASC-J9 indeed enhanced BCG efficacy to prevent bladdercancer development in the BBN-induced bladder cancer mousemodel.
We also applied BrdUrd staining to assay the proliferation inthese BBN-induced bladder cancermousemodels and foundmicetreated with BCG alone or ASC-J9 alone had less BrdUrd stainingthan those mice receiving vehicle control, and mice treated withboth BCG and ASC-J9 had the least BrdUrd staining (Fig. 5B andD), which again confirmed the above findings showing ASC-J9could enhance BCG efficacy to suppress bladder cancer cellproliferation in the BBN-induced bladder cancer mouse model.
Importantly,weexamined the recruitmentofmonocytes/macro-phages in thisBBN-inducedbladder cancermousemodelwith anti-macrophage F4/80 antibody and found that BCG alone helps torecruit more monocytes/macrophages to bladder cancer, and BCGplus ASC-J9 treatment recruited many more monocytes/macro-phages to bladder cancer (Fig. 5C and E), which is in agreementwith above in vitro coculture system (Fig. 2) showing ASC-J9 could
Figure 3.Monocytes/macrophages recruitmentto bladder cancer cells under BCG plusASC-J9/HF treatment leads todecreased proliferation of bladdercancer cells through TNFa production.A, 106 THP-1 cells were cultured in 6-wellplates, treated with BCG, HF, or ASC-J9only, BCGþASC-J9, or BCGþHF for48 hours, The different conditionedmedia were collected to detect TNFaproduction by ELISA. B and C, the aboveconditioned media were used to treatT24 and 253J cells cocultured with THP-1 cells and cell viability was detected byMTT. Each experiment was performed intriplicate; � , P < 0.05 (Student t test).
Shang et al.
Mol Cancer Ther; 14(11) November 2015 Molecular Cancer Therapeutics2590
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

enhance BCG to recruit more monocytes/macrophages to bladdercancer cells.
Together, results from the BBN-induced bladder cancer mousemodel (Fig. 5C–E) clearly demonstrated that ASC-J9 couldenhance BCG efficacy to suppress bladder cancer development.
DiscussionBCG therapy has been used successfully to treat nonmuscle
invasive bladder cancer since 1976 (2, 19, 20). However, eventhough BCG is quite effective, approximately 30% of bladdercancer patients treated with intravesical BCG fail to respond (6),and many patients have higher rates of recurrence and/or pro-gressionwithin 5 years (21, 22). How to improve the BCG efficacyto reduce the recurrence of bladder cancer is, therefore, clinicallyimportant and essential to extend the bladder cancer patientssurvival.
Understanding the mechanism of BCG function is critical forimproving the efficacy of therapy. Presently, it is generallyassumed that the BCG-induced antitumor activity is criticallydominated by a local nonspecific immunologic reaction reflectingthe activity of immunocompetent cells. After instillation, the BCGbinds to fibronectin that is expressed on the urothelium, whichcould then be internalized by the urothelial cells, including cancercells (23). Subsequently, BCG antigens can be presented at the cellsurfaces of urothelial cells in the context of MHC class II, whichmay then stimulate theCD4þT cells and induce aprimary Thelpertype 1 immune response (24). This complex and robust immunereaction evoked by BCG is evidenced by a massive transientsecretion of cytokines in voided urine, including IL1, IL2, IL5,IL6, IL8, IL10, IL12, IL15, and IL18, as well as interference ofinducible protein (IP)-10, TNFa, granulocyte–monocyte colony-stimulating factor (GMCSF), and IFNg (25). The final step in theeradication of bladder cancer cells is the activation of cytotoxic
Figure 4.HF and ASC-J9 potentiate the antitumoreffects of BCG in vitro. A–E, fourdifferent bladder cancer cells wereseeded in the 24-well plates, treatedwithMock, BCG, HF, ASC-J9, or BCGplusHF or ASC-J9 as indicated in the figures.Then the cells were collected for MTTassays (A–D). E, the conditioned mediafrom treated cells were collected andused to detect HMGB1 release by ELISA;� , P < 0.05 (Student t test).
ASC-J9 with BCG Therapy to Better Suppress Bladder Cancer
www.aacrjournals.org Mol Cancer Ther; 14(11) November 2015 2591
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

effector cells, such as the natural killer cells, monocyte/macro-phage cells, and other innate immune cells (26, 27).
The linkage of androgen/AR signals to alter the BCG efficacy,however, remains unclear, and few studies suggest that target-ing AR could be an alternative therapy to suppress bladdercancer progression. Using an ARKO mouse model, Miyamotoand colleagues (5) found that androgen/AR signals mightplay important roles to promote bladder cancer develop-ment/progression, and targeting AR with ASC-J9 suppressedbladder cancer development/progression. See and colleaguesalso reported that one of the cytokines elicited in response toBCG, specifically IL6, upregulates the cellular expression ofintegrin-a5b1, the receptor complex on which BCG adherencedepends (4). They further confirmed that androgen coulddownregulate NF-kB–mediated IL6 expression by human TCClines (6). These studies suggest that alteration of the autocrineIL6 response to BCG via pharmacologic manipulation of theandrogen milieu may have therapeutic value for the BCGantitumor treatment efficacy for transitional carcinoma.
In this article, we used two methods to block androgen/ARsignaling. One is the antiandrogen compound, HF, which is an
active metabolite of flutamide approved by the FDA and inhibitsandrogen/AR signals by blocking androgen binding to AR. On theother hand, we used ASC-J9 to inhibit androgen/AR signaling bydegrading AR in T24 and 253J cells (Supplementary Fig. S1A andS1B). On the basis of the clinical BCG intravesical therapy guide-lines and a previously published article, we used BCG only orcombined with ASC-J9 to treat bladder cancer cells or intravesicaltherapy in the BBN-induced bladder cancermousemodel both for2 hours (28), and the results showed that the combination of BCGand HF or ASC-J9 better suppressed bladder cancer progression.
Importantly, we proved here that ASC-J9 and HF could alsoenhance the BCG therapeutic efficacy to suppress bladder cancercell proliferation in the absence of infiltrating monocytes/macro-phages (Fig. 4). Mechanism dissection suggested that BCG com-bined with HF or ASC-J9 induced more HMGB1 release frombladder cancer cells compared with BCG only. These results are inagreement with recent studies showing that HMGB1 release frombladder cancer after BCG treatment could be one of the directcellular effects of BCG.
Interestingly, in addition to the direct effect, other indirectmechanisms also indicate that BCG could enter into bladder
Figure 5.ASC-J9 potentiates the antitumoreffects of BCG in BBN-induced mousebladder cancer model. Twelve-week-old FVB female mice were divided into4 groups (10 mice/group) and treatedwith 0.05% BBN in drinking water for 12weeks. Mice were then injected with (i)vehicle control, (ii) BCG (2 � 106 CFU/mouse, intravesical injection weekly)alone, (iii) ASC-J9 (75 mg/kg bodyweight, every other day, IP) alone, or(iv) BCG (2 � 106 CFU/mouse,intravesical injection weekly)þASC-J9(75 mg/kg body weight, every otherday, IP). Mice were then sacrificed 48hours after the fourth injection andbladders collected for furtherexamination, including H&E section (A)and BrdUrd stain (B) for the bladdercancer cell proliferation. C, we usedmonocytes/macrophages markerF4/80 antibody to assay monocyte/macrophage cells infiltration. D and E,the positive expression of BrdUrd andF4/80 were quantified in three randomfields. Blue arrows, positive cells;� , P < 0.05 (Student t test).
Mol Cancer Ther; 14(11) November 2015 Molecular Cancer Therapeutics2592
Shang et al.
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

cancer via adherence to the luminal surface of the bladder topromote immunologic responses that involve the recruitment ofthe infiltrating monocytes/macrophages to suppress bladder can-cer (29). Importantly, using qPCR to assay theM1- versusM2-typeof macrophage (30) during BCG treatment, we further found thatBCG could enhance the recruitment of M1-type of macrophagethat led to suppress bladder cancer cell proliferation (Supplemen-tary Fig. S2.). This result is in agreementwith early studies showingthat infiltrated M1-type macrophages may suppress tumor cells(31, 32).
ASC-J9 could enhance BCG immunotherapeutic effects viaalteration of those key factors, including IL6, integrin-a5b1,and TNFa, which is also in agreement with early studiesshowing ASC-J9 had high efficacy to suppress other AR-relatedtumors, including prostate, kidney, and liver (8, 33–37). Wealso found similar effects when we replaced ASC-J9 with HF.This result not only further supports the above findings show-ing that targeting androgen/AR signals can enhance BCG effi-cacy to suppress bladder cancer, but may also provide a mucheasier and quicker therapeutic approach to develop a newcombined therapy of BCG with HF. In contrast, more timeand effort will be needed in the future to see whether ASC-J9can also pass human clinical trials to translate its in vitro and invivo mouse effects into humans.
In summary, our findings showing the combined therapy ofBCGwithHF or ASC-J9 can lead to better therapy than BCG aloneto suppress bladder cancer progressionmayhelp patients to betterbattle bladder cancer in the near future.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: Z. Shang, R. Han, S. Yeh, C. ChangDevelopment of methodology: C-R. ShyrAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): E.M. MessingAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): Z. Shang, C-R. Shyr, S. YehWriting, review, and/or revision of the manuscript: Z. Shang, Y. Li, M. Zhang,J. Tian, E.M. Messing, S. Yeh, Y. Niu, C. ChangStudy supervision: S. Yeh, Y. Niu, C. Chang
AcknowledgmentsASC-J9 was patented by the University of Rochester, University of North
Carolina, and AndroScience, and then licensed to AndroScience. Both theUniversity of Rochester and C.C. own royalties and equity in AndroScience.
Grant SupportThis work was supported by theNIH grant CA156700 andGeorgeWhipple
Professorship Endowment (to C. Chang), the Taiwan Department of HealthClinical Trial and Research Center of Excellence grant DOH99-TD-B-111-004(China Medical University, Taichung, Taiwan; to C. Shyr), and by TianjinNature Science grants 11JCYBJC28400 and 12ZCDZSY16900 (to Z. Shang).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received December 12, 2014; revised June 4, 2015; accepted August 6, 2015;published OnlineFirst August 11, 2015.
References1. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin
2014;64:9–29.2. Morales A, Eidinger D, Bruce AW. Intracavitary bacillus Calmette–
Guerin in the treatment of superficial bladder tumors. J Urol 1976;116:180–3.
3. Huben RP. Intravesical therapeutic versus immunotherapy for superficialbladder cancer. Semin Urol Oncol 1996;14:17–22.
4. Zhang GJ, Crist SA, McKerrow AK, Xu Y, Ladehoff DC, See WA. Auto-crine IL-6 production by human transitional carcinoma cells upregu-lates expression of the alpha5beta1 fibronectin receptor. J Urol 2000;163:1553–9.
5. Miyamoto H, Yang Z, Chen YT, Ishiguro H, Uemura H, Kubota Y, et al.Promotion of bladder cancer development and progression by androgenreceptor signals. J Natl Cancer Inst 2007;99:558–68.
6. Chen F, Langenstroer P, Zhang G, Iwamoto Y, See WA. Androgendependent regulation of bacillus Calmette-Guerin induced interleu-kin-6 expression in human transitional carcinoma cell lines. J Urol2003;170:2009–13.
7. Yang Z, Chang YJ, Yu IC, Miyamoto H, Wu CC, Yeh S, et al. ASC-J9�
ameliorates spinal and bulbar muscular atrophy phenotype via degrada-tion of androgen receptor. Nat Med 2007;13:348–53.
8. Wu MH, Ma WL, Hsu CL, Chen YL, Ou JH, Ryan CK, et al. Androgenreceptor promotes hepatitis B virus-induced hepatocarcinogenesis throughmodulation of hepatitis B virus RNA transcription. Sci Transl Med2010;2:32ra35.
9. Lai JJ, Lai KP, Chuang KH, Chang P, Yu IC, Wen-Jye Lin, et al. Monocyte/macrophage androgen receptor suppresses cutaneous wound healingin mice by enhancing local TNF-a expression. J Clin Invest 2009;119:3739–51.
10. Wu CT, Altuwaijri S, Ricke WA, Huang SP, Yeh S, Zhang C, et al. Increasedprostate cell proliferation and loss of cell differentiation in mice lackingprostate epithelial androgen receptor. Proc Natl Acad Sci U S A 2007;104:12679–84.
11. Bevers RFM, de Boer EC, Kurth K-H, Schamhart DHJ. BCG-inducedinterleukin-6 up-regulation and BCG internalization in well and poorlydifferentiated human bladder cancer cell lines. Eur Cytokine Netw1998;9:181–6.
12. Bevers RFM, de Boer EC, Kurth K-H, Schamhart DHJ. BCG internalizationin human bladder cancer cell lines, especially with regard to cell surface-expressed fibronectin. Aktuelle Urol 2000;31(Suppl 1):31–4.
13. Durek C, Brandau S, Ulmer AJ, Flad HD, Jocham D, Bo€ohle A. Bacillus-Calmette-Gu�erin (BCG) and 3D tumors: an in vitromodel for the study ofadhesion and invasion. J Urol 1999;162:600–5.
14. ZhaoW, Schorey JS, Bong-MastekM, Ritchey J, Brown EJ, Ratliff TL. Role ofa bacillus Calmette-Gu�erin fibronectin attachment protein in BCG-induced antitumor activity. Int J Cancer 2000;86:83–8.
15. Prescott S, James K, Hargreave TB, Chisholm GD, Smyth JF. IntravesicalEvans strain BCG therapy: quantitative immunohistochemical analysisof the immune response within the bladder wall. J Urol 1992;147:1636–42.
16. Eikawa S, Ohue Y, Kitaoka K, Aji T, Uenaka A, Oka M, et al. Enrichment ofFoxp3þ CD4 regulatory T cells in migrated T cells to IL-6– and IL-8–expressing tumors through predominant induction of CXCR1 by IL-6.J Immunol 2010;185:6734–40.
17. Luo Y, Yamada H, Evanoff DP, Chen X. Role of Th1-stimulating cytokinesin bacillus Calmette-Gu�eerin (BCG)-induced macrophage cytotoxicityagainst mouse bladder cancerMBT-2 cells. Clin Exp Immunol 2006;146:181–8.
18. Zhang G, Chen F, Cao Y, Amos JV, Shah G, See WA. HMGB1 release byurothelial carcinoma cells in response to Bacillus Calmette-Gu�erin func-tions as a paracrine factor to potentiate the direct cellular effects of BacillusCalmette-Gu�erin. J Urol 2013;190:1076–82.
19. Sylvester RJ, van der MA, LammDL. Intravesical bacillus Calmette–Guerinreduces the risk of progression in patients with superficial bladder cancer: ameta-analysis of the published results of randomized clinical trials. J Urol2002;168:1964–70.
ASC-J9 with BCG Therapy to Better Suppress Bladder Cancer
www.aacrjournals.org Mol Cancer Ther; 14(11) November 2015 2593
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

20. Bohle A, Bock PR. Intravesical bacillus Calmette–Guerin versus mitomycinC in superficial bladder cancer: formal meta-analysis of comparativestudies on tumor progression. Urology 2004;63:682–6.
21. Hemdan T, Johansson R, Jahnson S, Hellstr€om P, Tasdemir I, Malmstr€omPU; Members of the Urothelial Cancer Group of the Nordic Association ofUrology. 5-Year outcome of a randomized prospective study comparingbacillus Calmette-Gu�erin with epirubicin and interferon-a2b in patientswith T1 bladder cancer. J Urol 2014;191:1244–9.
22. Arends TJ, van der Heijden AG, Witjes JA. Combined chemohyperthermia:10-year single center experience in 160 patients with non-muscle invasivebladder cancer. J Urol 2014;192:708–13.
23. Kavoussi LR, Brown EJ, Ritchey JK, Ratliff TL. Fibronectin-mediatedCalmette-Guerin bacillus attachment to murine bladder mucosa.Requirement for the expression of an antitumor response. J Clin Invest1990;85:62–7.
24. Zuiverloon TC, Nieuweboer AJ, V�ekony H, Kirkels WJ, Bangma CH,Zwarthoff EC. Markers predicting response to bacillus Calmette-Gu�erinimmunotherapy in high-risk bladder cancer patients: a systematic review.Eur Urol 2012;61:128–45.
25. Luo Y, Chen X, O'Donnell MA. Role of Th1 and Th2 cytokines in BCG-induced IFN-g production: cytokine promotion and simulation of BCGeffect. Cytokine 2003;21:17–26.
26. Luo Y, Knudson MJ. Mycobacterium bovis bacillus Calmette–Guerininduced macrophage cytotoxicity against bladder cancer cells. Clin DevImmunol 2010;2010:357591.
27. Naoe M, Ogawa Y, Takeshita K, Morita J, Iwamoto S, Miyazaki A, et al.Bacillus Calmette–Guerin-pulsed dendritic cells stimulate natural killer Tcells and gamma delta T cells. Int J Urol 2007;14:532–8.
28. Hsu JW, Yin PN, Wood R, Messing J, Messing E, Lee YF. 1 alpha, 25-dihydroxylvitamin D3 promotes Bacillus Calmette-Gu�erin immunother-apy of bladder cancer. Oncotarget 2013;4:2397–406.
29. Redelman-Sidi G, GlickmanMS, Bochner BH. The mechanism of action ofBCG therapy for bladder cancer—a current perspective. Nat Rev Urol2014;11:153–62.
30. Martinez FO, Gordon S. The M1 and M2 paradigm of macrophageactivation: time for reassessment. F1000Prime Rep 2014;6:13.
31. Chanmee T, Ontong P, Konno K, Itano N. Tumor-associated macrophagesas major players in the tumor microenvironment. Cancers 2014;6:1670–90.
32. Lizotte PH, Baird JR, Stevens CA, Lauer P, Green WR, Brockstedt DG, et al.Attenuated Listeria monocytogenes reprogramsM2-polarized tumor-asso-ciatedmacrophages in ovarian cancer leading to iNOS-mediated tumor celllysis. Oncoimmunology 2014;3:e28926.
33. He D, Li L, Zhu G, Liang L, Guan Z, Chang L, et al. ASC-J9�Suppressesrenal cell carcinoma progression by targeting an androgen receptor-dependent HIF2a/VEGF signaling pathway. Cancer Res 2014;74:4420–30.
34. Verderio P, Pandolfi L, Mazzucchelli S, Marinozzi MR, Vanna R, GramaticaF, et al. Antiproliferative effect of ASC-J9� delivered by PLGAnanoparticlesagainst estrogen-dependent breast cancer cells. Mol Pharm 2014;11:2864–75.
35. Hsu JW, Hsu I, Xu D, Miyamoto H, Liang L, Wu XR, et al. Decreasedtumorigenesis andmortality frombladder cancer inmice lacking urothelialandrogen receptor. Am J Pathol 2013;182:1811–20.
36. Lai KP, Huang CK, Chang YJ, Chung CY, Yamashita S, Li L, et al. Newtherapeutic approach to suppress castration-resistant prostate cancer usingASC-J9� via targeting androgen receptor in selective prostate cells. Am JPathol 2013;182:460–73.
37. Lee SO, Ma Z, Yeh CR, Luo J, Lin TH, Lai KP, et al. New therapytargeting differential androgen receptor signaling in prostate cancerstem/progenitor vs. non-stem/progenitor cells. J Mol Cell Biol 2013;5:14–26.
Mol Cancer Ther; 14(11) November 2015 Molecular Cancer Therapeutics2594
Shang et al.
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T

2015;14:2586-2594. Published OnlineFirst August 11, 2015.Mol Cancer Ther Zhiqun Shang, Yanjun Li, Minghao Zhang, et al. Better Suppress Bladder Cancer ProgressionReceptor Degradation Enhancer ASC-J9 Enhances BCG Efficacy to Antiandrogen Therapy with Hydroxyflutamide or Androgen
Updated version
10.1158/1535-7163.MCT-14-1055-Tdoi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2015/08/11/1535-7163.MCT-14-1055-T.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/14/11/2586.full#ref-list-1
This article cites 37 articles, 4 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/14/11/2586To request permission to re-use all or part of this article, use this link
on September 12, 2018. © 2015 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 11, 2015; DOI: 10.1158/1535-7163.MCT-14-1055-T


















