Anti Fungal and Anti Protozoal
22
Click here to load reader
Transcript of Anti Fungal and Anti Protozoal

ANTI-FUNGAL DRUGS AGENTS
A. Subcutaneous and Systemic Anti-fungal Agents – Amphotericin B– Caspofungin – Flucytosine – Imidazoles: Ketoconazole, Itraconazole,
Fluconazole, Miconazole, Voriconazole – Nystatin – Terbinafine, Amorolfine
B. Topical Anti-fungal Agents– Amphotericin B, Butenafine, Butoconazole,
Griseofulvin, Ciclopirox, Clioquinol, Clotrimazole, Econazole, Gentian violet, Ketoconazole, Miconazole, Naftifine, Nystatin, Oxiconazole, Sulconazole, Terbinafine, Terconazole, Tolnaftate
Antifungal Antibiotics– Amphotericin B– Nystatin – Griseofulvin
MECHANISM OF ACTION OF SOME ANTI-FUNGAL DRUGS
AMPHOTERICIN B • A polyene antibiotic derived from Streptomyces
nodosus.• Broad spectrum of activity (C. albicans, H.
capsulatum, C. neoformans, C. immitis, aspergillus) both fungistatic and fungicidal activity.
• MOA: Binds to sterols (ergosterol) in the cell membranes, forming pores or channels
which increase membrane permeability, making the cell more susceptible to destruction.
• MOR: Decreased ergosterol content of the fungal membrane.
• Active in growing and resting cells; not highly selective and will interfere with membrane function of mammalian host cell.
Pharmacokinetic profile:– Given by slow IV injection, topical, intrathecal
(meningitis) or oral.– Highly CHON-bound; excreted very slowly
through the urine.ADR:Infusion reactions: Fever, shaking chills, hypotension, anorexia, NAV, headache, dyspnea, tachypnea.
Others: Renal toxicity (potentiated by sodium depletion), electrolyte impairment (hypokalemia, hypomagnesemia, hypocalcemia), normocytic normochromic anemia, impaired hepatic function, local thrombophlebitis; intrathecal à neurotoxicity; topical à skin rash.
Therapeutic Uses:Acute, severe, systemic fungal infections(primary drug – DOC).Local dermatophytic and mucocutaneous infections (topical).Fungal infections of the GIT (oral).
NYSTATIN • Isolated from Streptomyces; first antimycotic
antibiotic.• Polyene antibiotic with broad spectrum of activity.• MOA: Binds to sterols in fungal cell membranes,
thereby increasing membrane permeability and making the cell more susceptible to destruction.
Pharmacokinetic profile:– Given by oral or topical route.
• ADR: Local burning and itching (topical).GI upset (NAV, diarrhea), renal toxicity.
• Therapeutic Uses: Prevention and topical treatment of superficial candidal infections of the skin and mucous membranes (gums, GIT, rectum, vagina).

GRISEOFULVIN • Fungistatic in activity.• MOA: Inhibits fungal cell mitosis by being
accumulated in the newly-synthesized keratin-containing tissue, thus producing multinucleated defective cells that bind to the microtubules, thereby disrupting mitotic spindle.
• Pharmacokinetic profile:– Orally administered; t1/2: 24 hours.– Distributes to growing nails and skin,
binding to keratin and making the cells resistant to fungal infection.
– Biotransformed in the liver to 6-methyl-griseofulvin; urinary excr.
• ADR: Headache, lethargy, fatigue, blurred vision, insomnia, GI upset, hepatotoxicity.
Drug Interactions:– With anticoagulants à reduced
effectiveness of anticoagulants because of enhanced metabolism.
– With barbiturates à enhanced metabolism of griseofulvin.
– With alcohol à tachycardia and flushing; potentiation of intoxicating effects of alcohol.
– With oral contraceptives à amenorrhea, increased breakthrough bleeding.
Therapeutic Use: For tinea infections of the skin, hair, nails including athlete’s foot and ringworm caused by Microsporum, Epidermophyton, and Trichophyton (oral).
FLUCYTOSINE • Fluorinated pyrimidine derivative for candidiasis,
cryptococcosis, and chromomycosis.• Fungistatic, synergistic effect with Amphotericin B.• MOA: Converted to 5-FU in sensitive
fungi à biotransformed to 5-fluoro-deoxyuridylic acid that inhibits thymidylate synthetase, thus depriving the organism of thymidilic acid (essential DNA component) à disrupts DNA synthesis.
• MOR: Decreased level of the enzymes in the conversion of flucytosine to 5-FU.
Pharmacokinetic profile:– Administered by oral route; t1/2: 3-6
hours. Excretion: Urine.
• ADR: NAV, diarrhea, rash, anemia, leukopenia, thrombocytopenia; increased liver
enzymes, BUN, & creatinine.
SYSTEMIC IMIDAZOLE
Ketoconazole • Broad antifungal activity; fungistatic activity. • MOA: Selectively increases fungal cell membrane
permeability by blocking the demethylation of lanosterol to ergosterol. (effective only in growing cells)
• MOR: Mutation in the C14 a-demethylasegene à decreased azole binding; fungi’s ability to pump the azole out of the cell.
• Orally given; readily absorbed under acidic pH. • ADR: NAV, diarrhea, rash, itching, dizziness,
constipation, fever, chills, and headache; gynecomastia and impotence;
hepatocellular toxicity.Therapeutic Uses:Rx of systemic and vaginal candidiasis, mucocandidiasis, oral thrush, histoplamosis, chromomycosis. coccidioidomycosis, dermatophytosis.
Other Azoles• Fluconazole
– Administered PO or IV.– May produce teratogenic effects.– DOC for Cryptococcus neoformans.
• Itraconazole – DOC for blastomycosis, aspergillosis,
sporotrichosis, histoplasmosis, and paracoccidioidomycosis.
– Orally administered.– With teratogenic capability.
• Voriconazole – Administered orally and effective for
invasive aspergillosis and serious infections caused by Scedosporium apiospermum and fusarium species.
– ADR: Transient visual disturbance.
Caspofungin • First of the echinocandins class of antifungal drugs.

• MOA: Interferes with the synthesis of the fungal cell wall by inhibiting the synthesis of b-D-glucan à cell lysis and death.
• ADR: Fever, rash, nausea, phlebitis, flushing.
SYSTEMIC & TOPICAL IMIDAZOLE:
Miconazole • Administered both parenterally and topically.• Therapeutic Uses: For Rx of candidal and
dermatophytic infections of the skin and for vaginal candidiasis (topical).For severe systemic fungal infections unresponsive
or not tolerant to
Amphotericin B (IV)• ADR: Local burning, itching, and rash (topical).
NAV, anemia, anaphylactoid reactions, CNS toxicity, hyponatremia, phlebitis (IV).
TOPICAL IMIDAZOLE
Clotrimazole • Broad antifungal activity.• Therapeutic Uses: Vulvovaginal candidiasis
(topical) Oropharyngeal candidiasis (topical oral)• ADR: Erythema, blistering, edema, pruritus,
urticaria.TOPICAL IMIDAZOLESEconazole and Butoconazole
ECONAZOLE– Derivative of miconazole.– Used for the treatment of tinea pedis, tinea
cruris, tinea corporis, tinea versicolor, and cutaneous candidiasis.
– ADR: Burning, itching, rash.– BUTOCONAZOLE– Azole cream for vaginal use and is effective
against vaginal infections caused by Candida albicans and Candida tropicalis.
– May cause vulvovaginal burning and itching.
OTHER TOPICAL ANTIMYCOTIC AGENTS– Undecylenic acid, haloprogin.
• TERBINAFINE, NAFTIFINE, AMOROLFINE
TERBINAFINE• Fungicidal agent that acts by selectively inhibiting
squalene epoxidase that is involved in the synthesis of ergosterol from squalene in the fungal cell wall à accumulation of squalene à toxicity to organism.
• Given orally or topically for fungal infections of the nails.
• ADR: GI disturbances, rashes, pruritus, headache, dizziness, joint and muscle pains, hepatitis.
Related drug: Naftifine AMOROLFINE
• A morpholine derivative that interferes with fungal sterol synthesis.
• Given orally for fungal infections of the nails.
BUTENAFINE• A synthetic benzylamine.• MOA
– Alters fungal membrane permeability and growth inhibition.
– Interferes with sterol biosynthesis by allowing squalene to accumulate within the cell.
• Therapeutic Uses– Dermatophytoses, including tinea corporis,
tinea cruris, and tinea pedis (1% cream).CICLOPIROX
• MOA:– Intracellular depletion of amino acids and ions
necessary for normal cellular function.– Therapeutic Uses:– Tinea pedis, tinea cruris, tinea corporis, tinea
versicolor, cutaneous candidiasis (topical).
• Clioquinol – Available in 3% ointment for tinea pedis and
cruris.– May cause local irritation, rash, and sensitivity
reactions.• Oxiconazole
– Available in 1% cream or lotion for tinea cruris, corporis, mannum, and pedis and tinea versicolor.

• Sulconazole – Imidazole derivative available in 1% cream
or solution and used for tinea corporis, cruris, pedis, versicolor and impetigo.
• Terconazole – Imidazole derivative available in vaginal
cream and suppository and used for vulvovaginal candidiasis.
ANTIVIRAL DRUGS • STAGES OF VIRUS MULTIPLICATION
Phase 1: Adsorption, penetration, and uncoating as the virus enters the host cell and sheds its protective coating.Phase 2: Synthesis of viral components.Phase 3: Assembly and release of the virus which can destroy or permanently change the cell.
INHIBITORS OF VIRAL CELL MULTIPLICATION • Phase 1 and phase 3 inhibitor: Amantadine.• Phase 2 inhibitors: Acyclovir, Ganciclovir,
Vidarabine, Trifluoridine, Idoxuridine, Ribavirin, Zidovudine.
Drugs for Respiratory Virus Infections– Amantadine, Oseltamivir, Ribavirin,
Rimantadine, Zanamirvir Drugs for Hepatic Viral Infections
– Adefovir, Entecavir, Interferon, Lamivudine Drugs for Herpes and Cytomegalovirus Infections
– Acyclovir, Cidofovir, Famciclovir, Fomivirsen, Foscarnet, Ganciclovir, Penciclovir, Valacyclovir, Valgancyclovir, Vidarabine
Drugs for HIV Infections– Abacavir, Amprenavir, Atazanavir, Delavirdine,
Didanosine, Emtricitabine, Enfuvirtide, Efavirenz, Indinavir, Lamivudine, Lopinavir, Nelfinavir, Nevirapine, Ritonavir, Saquinavir, Stavudine, Tenofovir, Zalcitabine, Zidovudine
Treatment of Respiratory Virus Infections Neuraminidase Inhibitors: Oseltamivir, Zanamivir
– Sialic acid analogues– MOA: Inhibits the neuraminidase enzyme
à preventing the release of new virions and their spread from cell to cell.
– MOR: Mutation of the neuraminidase.
– Oseltamivir: Orally active prodrug à active metabolite in liver; ADR: GI discomfort and nausea.
– Zanamavir: Inhalation or intranasal administration; avoided in severe reactive asthma or COPD.
– Effective for influenza A and B infections.
Inhibitors of Viral Uncoating: Amantadine, Rimantadine, Ribavirin
AMANTADINE & RIMANTADINE • Adamantadine derivatives.• Synthetic tricyclic amine with a narrow spectrum
of activity.• Therapeutic Uses: Treatment or prophylaxis of
influenza A virus and for Parkinson’s disease.• MOA: >Inhibits the adsorption of viral particles to
host cells, resulting in delayed penetration of the virus into the cell and/or inhibition of uncoating.
> Inhibits virus assembly.• MOR: Change in one amino acid of the M2 matrix
protein.• Given orally; t1/2: 12-36 hours; peak effects in 2-4
hours.• ADR: Dizziness, insomnia, and slurred speech;
confusion, ataxia, sleep disorders, tumors, hallucinations; anorexia, NAV, orthostatic hypotension; edema.
RIBAVIRIN• A synthetic nucleoside analog.• MOA: Interferes with guanidine monophosphate,
thereby reducing nucleic acid synthesis.• Therapeutic Uses: RSV infections, herpes simplex
infections, influenza A and B infections.• ADR:Rash, headache, fatigue.
TREATMENT OF HEPATIC VIRAL INFECTIONS• Hepatitis B: Rx with interferon-a and lamivudine • Hepatitis C: Rx with interferon-a and ribavirin
INTERFERON– Immunomodulator.– Inducible proteins synthesized by
mammalian cells and now produced by recombinant DNA technology.

– MOA: Induces, in the ribosomes of the host cells, the production of enzymes that inhibit translation of viral mRNA into viral CHON à stops reproduction of viruses.
– Given IV; t1/2 of 2-4 hours.– Therapeutic Uses: Hepatitis B infection and
AIDS-related Kaposi sarcoma (a interferon)Hepatitis C infection (a2b interferon)
– ADR: Fever, lassitude, headache, myalgia, bone marrow depression, rashes, alopecia.
Other Drugs for Hepatic Viral Infections• Lamivudine
– Cytosine analog that inhibits both hepatitis B virus (HBV) DNA polymerase and human immunodeficiency (HIV) reverse transcriptase.
– Oral administration with t1/2 of 9 hours. • Adefovir
– Nucleotide analog that is phosphorylated into adefovir diphosphate and incorporated into the viral DNA à terminates further synthesis à prevents viral replication.
• Entecavir – Guanosine analog that is converted into
entecavir triphosphate which competes for viral reverse transcriptase.
ACYCLOVIR • Acycloguanosine, 9-2-OH-ethoxymethylguanine.• A nucleoside analog of the pyrimidine, guanosine.• MOA: Its triphosphate (acyclo GTP) competitively
inhibits viral DNA polymerase and is also incorporated into viral DNA where it functions as a chain terminator, thus preventing the further elongation of the DNA molecule and therefore viral replication.
• MOR: Changes in the viral genes coding for DNApolymerase.
• Given orally, topically, and intravenously; t1/2 of 2.5 - 3.5 hrs.
• Related drugs: Valaciclovir (prodrug of aciclovir)Famciclovir (met. to penciclovir - active)
• Therapeutic Uses: > Rx of mucocutaneous herpes and genital and disseminated adult herpes simplex.> Mgt. of initial herpes genitalis and in non-
life-threatening cutaneous simplex virus infections in immunocompromised px.>Rx or suppression of recurrent episodesof genital herpes infection and in varicella zoster.
• ADR: Mild pain, transient burning and stinging, pruritus, and rash (ointment); NAV, headache, diarrhea, dizziness, anorexia, fatigue, edema, skin rash, leg pain, adenopathy, sore throat (oral); phlebitis, transient elevation of serum creatinine, rash (IV).
GANCICLOVIR • A synthetic purine nucleoside analog.• Therapeutic Use: Cytomegalovirus infections (IV)
and for maintenance therapy in AIDS patients (oral).
• MOA: Activated to its triphosphate form which competes with guanosine triphosphate for incorporation into the viral DNA.
• Given intravenously and orally with t1/2 of 4 hours.
• ADR: Bone marrow depression, carcinogenicity.• Drug Interactions:
– With Probenecid à increased ganciclovir level à toxicity.
– With Imipenem-Cilastatin à generalized seizures.
– With Zidovudine and cytotoxic drugs à neutropenia.
VIDARABINE • Adenine arabinoside.• MOA: Its triphosphate inhibits viral DNA
polymerase, thus reducing DNA synthesis.• Administered topically or intravenously (slow
infusion).• T1/2: 4 hours.• Undergoes deamination to arabinosyl-
hypoxanthine.• Therapeutic Uses:
Herpes simplex keratitis (ophthalmic). Herpes simplex encephalitis, other severe
systemic herpes infections, and varicella zoster (IV).
• ADR: NAV, anorexia, diarrhea; decreased Hgb and Hct, increased SGOT, tremors, dizziness, hallucinations.

TRIFLURIDINE • Trifluorothymidine; a halogenated thymidine
derivative used as ophthalmic solution for herpes simplex-induced keratoconjunctivits.
• MOA: Converted to its triphosphate which inhibits DNA polymerase.
• ADR: Local burning or stinging.
IDOXURIDINE • Halogenated derivative of deoxyuridine.• MOA: Inhibits the replication of of DNA viruses
by its incorporation into the virus.• Given topically.• Used for the treatment of herpes simplex keratitis.• ADR: Inflammatory edema of the eyelids,
photophobia, lacrimal duct occlusion, and contact dermatitis.
FOSCARNET • Trisodium phosphonoformate hexahydrate or PFA• A synthetic non-nucleoside analog of
pyrophosphate; given IV.• MOA: Inhibits viral DNA polymerase by
binding directly to the pyrophosphate binding site.
• ADR: Nephrotoxicity; hyper/hypocalcemia, seizures.
ZIDOVUDINE • Azidothymidine or AZT.• Therapeutic Indication: Rx of AIDS patients with P.
carinii pneumonia or advanced AIDS-related complex.
• Given orally or by IV; t1/2: 1 hour.• MOA: Interferes with HIV replication by being
converted to triphosphate and inhibiting the DNA polymerase.
• MOR: Rapid mutation of the virus; decreased activation of the drug to its triphosphate; increased virus load due to reduction in immune mechanisms.
• ADR: Insomnia, myalgia, nausea, severe headache, anemia, and neutropenia.
DIDANOSINE • Dideoxyinosine, ddI.• A synthetic purine analog.
• MOA: Phosphorylated to triphosphate which acts as a chain terminator and inhibitor of the viral reverse transcriptase.
• Given orally with plasma t1/2 of 30 mins. and intracellular t1/2 of 12 hours.
• Used to treat AIDS.• ADR: Pain and sensory loss in the feet; dose-
related pancreatitis.
ZALCITABINE • Dideoxycytidine, ddC.• A synthetic nucleoside analog.• MOA: Inhibits the reverse transcriptase enzyme.• Given orally with a plasma t1/2 of 20 mins. and
intracellular t1/2 of 3 hours.• Used in the Rx of AIDS in combination with
Zidovudine.• ADR: Dose-related neuropathy, GI disturbances,
headache, mouth ulcers, edema of the lower limbs, general malaise, pancreatitis.
NUCLEOSIDE REVERSE TRANSCRIPTASE INHIBITORSAbacavir, Adefovir, Lamivudine, Stavudine, Zalcitabine, Didanosine, Zidovudine.
• Competitive inhibitors of reverse transcriptase à chain termination when incorporated into the viral DNA chain.
NON-NUCLEOSIDE REVERSE TRANSCRIPTASE INHIBITORSDelavirdine, Efavirenz, Nevirapine
• Competitive inhibitors of reverse transcriptase à chain termination when incorporated into the viral DNA chain.
PROTEASE INHIBITORSAmprenavir, Indinavir, Nelfinavir, Ritonavir, Saquinavir.
• Competitively inhibit the viral protease enzyme, preventing the enzyme from cleaving the polyprotein necessary for the production of the infectious virions.
Viral Fusion Inhibitor• Enfuvirtide
– Antiretroviral drug.– A 36 AA peptide that binds to gp41,
preventing the conformational change of the viral transmembrane that is necessary

for the fusion of the HIV membrane with that of the host cell
– Subcutaneous administration.
NATIONAL GUIDELINES FOR ANTI-HIV TREATMENT• When to begin treatment
– Treat any symptomatic patient.– Offer treatment to asymptomatic patients
with CD4 <500 or HIV-RNA >20,000 or recommend observing patients with CD4 350-500 and RNA <20,000.
– Observe or treat asymptomatic patients with CD4 >500 and HIV-RNA <20,000.
• Preferred Regimen – Choose from one of the protease
inhibitors and one of the nucleoside reverse transcriptase inhibitor combinations (NRTI) (zidovudine + lamivudine, zidovudine + didanosine, zidovudine + zalcitabine, stavudine + lamivudine)
• Alternative Regimen – Choose 2 NRTI combinations + 1 non-
nucleoside RTI, either nevirapine or delavirdine.
• Monitoring – Monitor HIV-RNA level; if HIV-RNA does
not fall more than 10-fold by week 8, change drug regimen and use 2-3 new agents.
– Consider changing if CD4 is falling or if there is clinical deterioration.
ANTI-PROTOZOAL DRUGS
ANTI-MALARIAL DRUGSDRUG CLASSIFICATION>Blood schizonticides
• Drugs for suppressive or clinical cure.• Affect the erythrocytic stage of life cycle.• Suppress the symptoms of actual attack by
destroying the schizonts and merozoites in the erythrocytes.
• CHLOROQUINE, AMODIAQUINE, MEFLOQUINE, QUININE, HALOFANTRINE.
>Tissue schizonticides • Effects radical cure by acting on the malarial hepatic
stage.• Destroys gametocytes, thus reducing the spread of
infection.• PRIMAQUINE.•
>Drugs that affect both exo- and erythrocytic forms• Anti-folate drugs or dihydorfolate reductase
inhibitors.• CHLOROGUANIDE, PYRIMETHAMINE,
TRIMETHOPRIM.
GAMETOCIDES• Prevent infection in mosquitoes by destroying the
gametocytes in the blood.• PRIMAQUINE, CHLOROQUINE.
SPORONTICIDES• Render the gametocytes non-infective in the
mosquito.• PYRIMETHAMINE, PROGUANIL.• BLOOD SCHIZONTICIDES• 4-AMINOQUINOLINES: Chloroquine, Amodiaquine.• QUINOLINE METHANOLS: Quinine, Mefloquine.• PHENANTHRENE METHANOL: Halofantrine.
CHLOROQUINE (Aralen)• MECHANISMS OF ACTION
– Blocks the enzymatic synthesis of DNA and RNA in humans and protozoal cells à forms a complex with DNA à prevents DNA from acting as template for the replication and transcription to RNA.

– Forms a complex with ferriprotoporphyrin à damage to cell membrane à lysis of the parasite and RBC.
• MECHANISM OF RESISTANCE– Impaired mechanism of drug transport
across the parasite cell wall à concentration of drug in resistant schizonts never reaches a level sufficient to arrest nucleic acid synthesis.
• PHARMACOKINETICS– Formulation: Phosphate, hydrochloride.– PPB: 50-65%.– High concentrations in the erythrocytes,
liver, spleen, kidneys, lungs, leukocytes.– Penetrates the CNS and crosses the
placenta.– T1/2: 3-5 days.
• PHARMACOLOGIC EFFECTS– Antimalarial effect.– Quinidine-like effect on the heart à
depresses the cardiac function.– Distinct anti-inflammatory capability
especially in rheumatoid arthritis and chronic discoid LE.
– CHLOROQUINE (Aralen)• THERAPEUTIC USES
– Acute malarial attacks.• Terminates fever in 24-48 hours.• Terminates parasitemia in 48-72
hours.– Chemophophylaxis vs all forms of malaria
except P. falciparum resistant to 4-aminoquinolines.
– Amoebiasis, autoimmune disorders as DMARD.
• ADR– Mild: GI complaints (nausea, epigastric
distress), skin rash, headache.– High dosage: Alopecia, graying of the hair,
skin eruptions and desquamations, keratopathy, retinopathy.
– Overdosage: Visual disturbances, hyperexcitability, convulsions, AV block, death.
QUININE• Alkaloid from the cinchona bark.• MECHANISM OF ACTION
– Complexes with double-stranded DNA to prevent strand separation, transcription, and CHON synthesis.
• PHARMACOLOGIC EFFECTS– Peripheral vosodilation.– Quinidine-like depression of myocardial
excitability and conduction velocity.– Direct relaxant effect on the smooth
muscles à severe or lethal hypotension.– Distinct curare-like action.– Contraction of the pregnant uterus.– Hypoglycemia.
• PHARMACOKINETICS– Administration: PO, IV, IM (7-day course).– PPB: 70-80%.– T1/2: 7-12 hours.– Highest concentrations in the liver, lungs,
kidneys, spleen.– Metabolism in the liver; excretion through
the urine.• THERAPEUTIC USES
– Parenteral treatment of severe falciparum malaria.
– Oral Rx of falciparum malaria resistant to Chloroquine.
– Prophylaxis for Chloroquine-resistant falciparum strains.
– Relief of nighttime leg cramps.– Severe babesiosis with Clindamycin.
• Adverse Reactions• GI: Irritation à NAV, epigastric pain.• Cinchonism: At a drug plasma level of 7-10 mg/ml.
– GI distress, tinnitus, vertigo, headache, blurred vision.
• Hematologic effects– Hemolysis, leukopenia, agranulocytosis,
thrombocytopenia purpura, Henoch-Schonlein purpura, hypoprothrombinemia.
• Hypoglycemia, thrombophlebitis, moderate-severe hypotension, seizures, ventricular fibrillation, death.
• Severe toxicity– Fever, skin eruptions, GI symptoms,
deafness, visual abnormalities, CNS effects (syncope, confusion), quinidine-like effects.
• Blackwater fever

– Characterized byexcessive intravascular hemolysis followed by hemoglobinuria, dark urine, azotemia, renal failure.
• DRUG INTERACTIONS (QUININE)– + aluminum-containing antacids à
delayed absorption of Quinine.– + Digoxin à decreased renal clearance of
Digoxin à increased serum concentration of Digoxin.
– + Warfarin and other anticoagulants à enhanced action of these anticoagulants.
– + Cimetidine à slowed elimination of Quinine.
MEFLOQUINE Synthetic 4-quinoline methanol derivative
chemically related to quinine.• MECHANISM OF ACTION
– Inhibition of heme polymerase (enzyme that polymerizes toxic free heme to hemozoin) à parasite becomes harmless.
• PHARMACOKINETICS– Administered by oral route; highly protein-
bound, concentrated in the RBC and extensively distributed to the tissues; t1/2 of > 6 days.
• PHARMACOLOGIC EFFECT– Quinidine-like effects on the heart à BP
reduction and depression of cardiac function.
• THERAPEUTIC USES– Prophylaxis and treatment of Chloroquine-
resistant strains of P. falciparum.• ADVERSE REACTIONS
– Prophylactic dose:• GI disturbances, headache,
dizziness, syncope, extrasystoles.• Transient leukocytosis,
thrombobocytopenia, aminotransferase elevations.
• Transient neuropsychiatric events as convulsions, depression, and psychosis.
– Treatment dose:• GI disturbances, fatigue,
neuropsychiatric symptoms, pruritus, skin rash, myalgia.
• CONTRAINDICATIONS– History of epilepsy, psychiatric illness,
arrhythmias, cardiac conduction defects, or sensitivity to quinidine or related drugs.
– Concurrent use with quinine, quinidine, or halofantrine.
– Pregnancy.– Persons whose work requires fine
coordination and spatial discrimination.– With anti-convulsant drugs à
breakthrough seizures.
HALOFANTRINE• Active against strains of P. falciparum resistant to
chloroquine, pyrimethamine, or quinine and the erythrocytic form of P. vivax.
• PHARMACOKINETICS– Administered PO with peak plasma
concentration 4-6 hours after ingestion.– Main metabolite: N-debutyl-
halofantrine; excretion: feces.– T1/2: 4-5 days.
• ADR– Abdominal pain, GI disturbances,
headache, cough, transient rise in hepatic enzymes, pruritus, syncope, dysrhythmias, hemolytic anemia, convulsions.
PRIMAQUINE An 8-aminoquinoline drug.• MECHANISM OF ACTION
– Forms quinoline-quinone metabolites which interfere with electron transport causing oxidative damage to mitochondrial enzyme system in the parasite à swelling and vacuolation of the mitochodria à lysis of the parasite.
• PHARMACOKINETICS– Administered PO.– Concentrated in the liver, lungs, brain,
heart, and skeletal muscles.– Rapidly biotransformed (liver) to
carboxyprimaquine.– T1/2: 3-5 hours.
• THERAPEUTIC USES– Terminal prophylaxis of vivax and ovale
malaria.

– Radical cure of acute vivax and ovale malaria.
– Gametocidal action.– Pneumocystis carinii pneumonia.–
• ADVERSE REACTIONS– Abdominal discomfort, nausea, headache,
changes in visual accommodation.– Leukopenia, agranulocytosis, leukocytosis,
pruritus, arrhythmias.– Primaquine sensitivity
• Intravascular hemolysis accompanied by the formation of methemoglobin in G6PD-deficient patients.
ANTIFOLATE DRUGS OR FOLATE METABOLISM INHIBITORS OR DIHYDROFOLATE REDUCTASE INHIBITORS
• DRUGS: Chloroguanide/Proguanil, Pyrimethamine, Trimethoprim
• MECHANISM OF ACTION– Inhibits plasmodial dihydrofolate
reductase (DHFR) à reduction of dihydrofolic acid to tetrachydrofolic acid (folinic acid) is inhibited.
PHARMACOKINETICS• Chloroguanide
– Slowly absorbed from the GIT; activated by conversion to the triazine compound; t1/2 of 16 hours.
• Pyrimethamine/Trimethoprim – Rapidly absorbed in the GIT; tissue
concentration is high; t1/2 of 4 days.• THERAPEUTIC USES
– Prophylaxis against malaria and in Chloroquine-resistant falciparum malaria (Chloroguanide.)
– Treatment of Chloroquine-resistant P. falciparum malaria (with sulfone or sulfonamide).
– ADVERSE REACTIONS– Anorexia (Chloroguanide).– Folic acid deficiency manifested as bone
marrow depression and megaloblastosis (Pyrimethamine).
ALTERNATIVE ANTIMALARIAL DRUG: QINGHAOSU • Also known as Artemisinin.
• Sesquiterpene lactone endoperoxide.• Extract from a Chinese herbal medicine (Artemisia
amma).• Other derivatives: Artesunate, artemether,
artether.• PHARMACOKINETICS
– Administered PO, IV, IM, rectal insertion.– Converted into dihydroqinghaosu or
dihydroartemisinin.– T1/2: Artemisinin - 4 hours; artesunate - 45
minutes; artemether - 4-11 hours.• CLINICAL USES
– Effective blood schizonticide against all malarial forms and Chloroquine-resistain falciparum malaria; cerebral falciparum malaria.
• ADVERSE REACTIONS – Abdominal pain, diarrhea; depression of
reticulocyte ct; transient heart block.
ALTERNATIVE ANTIMALARIAL DRUGS• QUINACRINE
– A blood schizonticide that suppresses all types of human malaria; effects radical cure of P. malariae and non-resistant strains of falciparum malaria.
– ADR: yellowish discoloration of the skin, psychotic rxns
– Also used in the treatment of giardiasis.• DOXYCYCLINE
– A tetracycline used vs multidrug resistant P. falciparum.
– Also for blood stages of the other Plasmodium species.
– With quinine for acute malaria.– ADR: GI symptoms, candidal vaginitis,
photosensitivity.• DAPSONE
– 4,4-diaminodiphenylsulfone (DDS) used in the prophylaxis of malaria usually combined with Pyrimethamine.
POTENTIAL NEW ANTIMALARIAL DRUGS• PYRONARIDINE
– Synthetic schizonticidal agent derived from mepacrine; developed in China.
– ATOVAQUONE

– Hydroxynapthoquinone for P. carinii penumonia.
THERAPEUTIC OPTIONS FOR THE TREATMENT AND PREVENTION OF MALARIA
AMOEBIASIS: E. histolytica • DRUG CLASSIFICATION
– Mixed amoebicidal drug• Effective against both luminal and
systemic forms.• METRONIDAZOLE.
– Luminal amoebicides • Act on the parasite in the lumen of
the bowel.• Dichloroacetamides: DILOXANIDE
FUROATE, TECLOZAN, ETOFAMIDE.• Halogenated hydrogquinolines:
IODOQUINOL, CLIOQUINOL.• Antibiotics: TETRACYCLINE,
PAROMOMYCIN.
– Systemic amoebicides • Effective against amoebae in the
intestine and liver.• EMETINE, DEHYDROEMETINE,
CHLOROQUINE.NITROIMIDAZOLES:>Metronidazole (Flagyl, Anerobia)>Tinidazole (Fasigyn)
• MECHANISM OF ACTION– Undergoes reductive bioactivation of its
nitro group by ferredoxin to form reactive cytotoxic products.
• PHARMACOKINETICS– Administered PO, IV, rectal insertion.– Peak plasma concentration 1-3 hours after
administration.– T1/2: Metronidazole - 7 hours; Tinidazole -
12-14 hours.• Drug of choice in severe intestinal wall disease and
in hepatic abscess and other extra-intestinal amoebic disease.
• CLINICAL USES: Mild-severe intestinal disease, liver abscess, amoeboma, extra-intestinal infections.
• TOXICITY: Bitter metallic taste, GI irritation, headache, discoloration of the urine, leukopenia, dizziness, ataxia.
• DRUG INTERACTION: Disulfiram-like rxn with ethanol and potentiation of coumarin anticoagulant effect.
DILOXANIDE FUROATE • Drug of choice in the treatment of asymptomatic
passers of cysts and in the treatment of intestinal amoebiasis.
• Direct amoebicidal action, affecting the amoeba before encystment.
• Administered PO; converted in the gut to diloxanide-free base which is active.
• ADR: Flatulence, dryness of the mouth, nausea, pruritus, urticaria.
• CI in pregnant women and children under 2 years old.
EMETINES: Emetine, Dehydroemetine
Alkaloid obtained from Brazil root.• MECHANISM OF ACTION
CONDITION DRUG
All Plasmodium species except Chloroquine-resistant P. falciparum
Chloroquine
Chloroquine-resistant P. falciparum
Quinine + Pyrimethamine-sulfadoxine or Doxycycline or Clindamycin Alternate drug: Mefloquine
Prevention of relapses: P. vivax and P. ovale only
Primaquine
Prevention of malaria
In Chloroquine-sensitive geographic areas: ChloroquineIn chloroquine-resistant geographic areas: Mefloquine
In pregnancy Chloroquine or Mefloquine

– Inhibits protein synthesis by blocking ribosomal movement along the messenger RNA.
• Used as back-up drugs for the treatment of severe intestinal or hepatic amoebiasis in hospitalized patients.
• Given parenterally (IM); widely distributed; excreted slowly by the kidneys.
• TOXICITY: Pain, tenderness, GI distress, muscle weakness, CV dysfunction (arrhythmias and CHF with dyspnea and hypotension.
• CLINICAL USES: Amoebic dysentery, amoebic liver abscess, amoebomas, and extra-intestinal amoebiasis.
HALOGENATED HYDROQUINOLINES: Iodoquinol, Clioquinol
• Orally active luminal amoebicides used as alternative drugs for mild to severe intestinal infections.
• CLINICAL USES– Intestinal amoebiasis, T. vaginalis vaginitis,
other intestinal parasites as B. coli, G. lamblia.
• ADVERSE REACTIONS– Mild: Diarrhea, NAV, gastritis, headache,
malaise.– Large doses and prolonged use: SMON
(subacute myelo-optic neuropathy.
OTHER DRUGS• CHLOROQUINE
– Active against amoebas in the liver especially when given with Emetine.
– Used in combination with Metronidazole and Diloxanide furoate to treat and prevent amoebic liver abscesss.
– PAROMOMYCIN (Humagel)– Aminoglycoside antibiotic used as a 2nd-
line amoebicide (luminal type).– Reduces the population of the intestinal
flora. – ADR: GI distress, diarrhea, headache,
rashes, arthralgia.– For mild intestinal disease à combine with
Doxycycline.
Therapeutic options for amoebiasis
Treatment for trypanosomiasis• African sleeping sickness
– Caused by Trypanosoma brucei gambiense and Trypanosoma brucei rhodiense.
– Live and grow in the blood à invade CNS à inflammation of the brain and spinal cord à lethargy and continuous sleep.
• American sleeping sickness – Chagas’ disease.– Caused by Trypanosoma cruzi.– Occurs in South America.
Melarsoprol
CLINICAL SYNDROME
DRUG
Asymptomatic cyst carriers
Iodoquinol or Paromomycin or Diloxanide furoate
Diarrhea / dysenteryExtraintestinal
Metronidazole + Iodoquinol or Paromomycin or Diloxanide furoate
Amoebic liver abscess
Chloroquine + Metronidazole or Emetine

– A derivative of mersalyl oxide that is used for the treatment of late stage of the infection with CNS involvement.
– MOA: Reacts with sulfhydryl groups of various substances, including the enzymes à toxic compounds.
– MOR: Decreased permeability of the drug.– Administered by IV; short t 1/2; rapidly
oxidized into nontoxic pentavalent arsenic compound.
– DOC in the Rx of T. brucei rhodiense and for meningoencephalitis caused by T. brucei gambiense.
– ADR: Encephalopathy; hypersensitivity reactions; GI disturbances, such as severe vomiting and abdominal pain; hemolytic anemia in G-6-PD deficiency.
Pentamidine isethionate– Administered IM or by aerosol; no
metabolized but excreted very slowly into the urine; t1/2 of 5 days.
– Used to prevent and treat the organism’s hematologic stage.
Nifurtimox– Used for Chagas’ disease.– Undergoes reduction into intrecellular
oxygen radicals (superoxide and hydrogen peroxide radicals) à toxic to organism.
– Administered orally.– ADR (elderly): Hypersensitivity reaction
and GI problems; peripheral neuropathy.
Suramin– Used for African trypanosomiasis.– MOA: Inhibits many enzymes involved in
energy metabolism.– Given IV.
Treatment for other protozoal infections LEISHMANIASIS
o Sodium stibogluconate TOXOPLASMOSIS
o Pyrimethamine o Sulfadiazine + Pyrimethamine
GIARDIASIS– Metronidazole
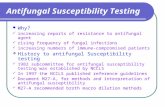
BACILLARY POPULATION (IN LUNG FIELDS)
• population A– bacilli lining the cavity wall– rapid growth and multiplication due to abundant
supply of O2– reside in neutral or slightly alkaline [pH]
environment– source of infectiousness, communicability, and
resistant mutants • population B (Persisters)
– bacilli in caseous nodules and inner linings of cavitary lesions
– slow or intermittent metabolism [persisters] – environment contains little O2 and pH is slightly
acidic– source of relapse à difficult to eradicate
• population C (Intracellular Bacilli)– bacilli inside macrophages [intracellular
population]– slow metabolizers [persisters]– environment is poorly oxygenated and frankly
acidic– source of relapse
S**M
Pop. A
INH RFP
PZA
Pop. B
Pop. C
active
Second most activeMost active
Most activeWeakly active
Most active
Less active than RFP 2ndmost active
Streptomycin (Oldest, 1944)
2
ETHAMBUTOL
• Bacteriostatic to populations A and C• Inhibits the growth of mutants resistant to INH and RFP• Not hepatotoxic but causes optic neuritis, give to adults
only, not in children.• Hepatotoxic:
– Isoniazid– Pyrazinamide ß Causes gout– Rifampicin

SHORT COURSE THERAPY OR SHORT COURSE CHEMOTHERAPY [AUGUST 19, 1986]
Given for the first 2 months - Intesnsive
– INH [Isoniazid] 300 mg PO daily– PZA [Pyrazinamide] 500 mg PO daily– RFP [Rifampicin] 450 mg PO AC OD
Given for the next 4 months – Maintenance
– INH– RFP Same dose as mentioned above
• Total number of Rx= 6 months
CONTRAINDICATIONS TO SCC
• History of liver disease (SGPT, SGOT, alcoholics)• History of chronic and acute renal disease• History of gout or predisposition to gout (PZA)• Patients taking steroids for more than 6 months –
Immunosuppression
VITAL FACTORS IN THE CHEMOTHERAPY OF TB
• Correct dosage• Regularity of administration• Adequate duration• Proper drug combination
PRIMARY HEALTH CARE [PHILIPPINES]
• For 2 months daily Rx -intensive– Rifampicin 450mg– INH 300mg– Pyrazinamide 1000mg to 15000mg
• For 4 months -maintenance– Rifampicin 450mg– INH 300mg
• Pyrazinamide 500mg/ tab (aka Para amino salicylic acid)
• Above 50 kilos – 3tabs (1,500 mg)• 50 kilos and below – 2tabs (1,000 mg)• Rifater, Pyrina – RNZ (Rifampicin, INH, PZA)
– For 2 months• Rifinah – RN (Rifampicin, and INH)
– For 4 months
REASONS FOR RX FAILURE
1.Non-observance of vital factors of Rx by either physician or px
2.Very extensive disease3.Uncontrolled DM and alcoholism4.Primary resistance to drugs5.Inherent of cellular immunity in the px
ADVERSE DRUG REACTIONS [ADR] – 1ST MONTH
• Loss of appetite and tiredness without reason - INH• Unexplained nausea and vomiting, collapse - INH• Rash and persistent itchiness - INH• Yellowish discolorations of skin and eyeballs - Rifamp• Flu-like syndrome- fever, chills, pain• When R is given intermittently in high dose - Rifamp• Tingling and burning sensation of hands and feet• Swelling and generalized edema• Shortness of breath - INH• Petechiae and ecchymoses – Rifampicin
• Advice- stop medication for few days and do desensitization
– Dose- 1/10, ¼, ½ à average dose
DRUG DOSE ADJUSTMENT
• INH – 5-10mg/kg, up to 400mg/ day• Rifampicin – 10mg/kg, up to 600mg/day• Pyrazinamide – 25-35 mg/kg, not to exceed 2grams
daily• irrespective of serum uric and level for as long as px is
asymptomatic• Ethambutol – 25mg/ kg/ day for 1st 2 months
– 15mg/ kg for next 4 months• Streptomycin – 15-20mg/ kg up to 1 gram daily by IM
INH PROPHYLACTIC USE
– Infants and children up to 6 years who converts to [+] PPD [without previous BCG]
– PPD [–] medical personnel and students who are in close contact with active cases in wards
– Recent tuberculin converters in close contact with open cases of TB
– Px on corticosteroid, anti-metabolite therapy with previous TB history • dose- 10mg/kg/ day
- 300-400mg daily
Best recommended Rx regimen for pulmonary TB [MDRTB ?]

– RHZE or RHZS daily [2 months]– RH [4 months] daily
• Chemoprophylaxis of adult patient [13-35 years]– INH + Ethambutol daily for 6 months;– Or INH + Rifampicin daily for 4 months
• 4 drugs given initially [2 months]– Big bacillary population especially cavitary lesion– Previous use of anti-TB drugs– High primary resistance to H ?– Close contact with resistant source case
MDT FOR LEPROSY [WHO]Disease Paucibacillary Multibacillary
Other Name Tuberculoid, Indeterminate type
Lepromatous, mid borderline (Serious, fingerless)
Rx Rifampicin 600mg once a month, Dapsone 100 mg 1-2 mg/kg/d
-Same
-Same-Clofazimine(Lamprene) 300mg once a month AND 50 mg/d
Rx duration 6 months 2 years or until skin smears are negative
Surveillance after Rx completion
Annual exams for at least 2 years
Annual exams for at least 5 years
14
SIDE NOTES
• Give Vitamin B complex (Pyridoxine) to prevent INH (Isoniazid H) toxicity• DOT – Direct Observance Therapy• Streptomycin – Only anti TB drug administered IM• Increased dose in INH causes convulsions• 2 months is INTENSIVE, 4 months is MAINTENANCE• Myrin P – Combination of the following drugs, 2 months: (INTENSIVE)
– R = Rifampicin– I = Isoniazid– P = Pyrazinamide– E = Ethambutol
• Myrin (4 months), only R I E• Rifampicin has PAE against leprosy, it is leprocidal• PHILCAT – Philippine Coalition Against tuberculosis
Rx regimen
I. 2 HRZE (2 RIPE) / 4HR (4 RI)I. New pulmonary smear (+) cases
II. New seriously ill pulmonary smear negative cases with parenchymal involvement
III. New seriously ill extrapulmonary TB cases
II. 2 HRZES (2 RIPES) / 1 HREZ (1 RIPE) / 5 HRE (5 RIE)
I. Failure casesII. Relapse cases
III. X-ray smear (+)
III. 2 HRZ (2 RIP) / 4 HR (4 RI) I. New cases, smear (--) but with minimal
pulmonary TB on x-ray confirmed by medical officer
II. New extrapulmonary TB (Not serious)
• H = Isoniazid H• R = Rifampicin• Z = Pyrazinamide• E = Ethambutol
• INH & rifampicin- hepatotoxic• Streptomycin & ethambutol- parenteral route• Rifampicin- nephrotoxic• Pyrazinamide- increase uric acid- gout• Ethambutol- cause optic neuritis in chidren