Ante- and intra-partum factors that predict increased need for neonatal resuscitation
9
Click here to load reader
-
Upload
khalid-aziz -
Category
Documents
-
view
218 -
download
2
Transcript of Ante- and intra-partum factors that predict increased need for neonatal resuscitation

Resuscitation (2008) 79, 444—452
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / resusc i ta t ion
CLINICAL PAPER
Ante- and intra-partum factors that predictincreased need for neonatal resuscitation�
Khalid Aziza,∗, Mairi Chadwickb, Mary Bakerc, Wayne Andrewsb,c
a Department of Pediatrics, University of Alberta, Room 5027 DTC, Royal Alexandra Hospital,10240 Kingsway, Edmonton AB, Canada T5H 3V9b Faculty of Medicine, Memorial University, 300 Prince Philip Drive, St. John’s NL, Canada A1B 3V6c Division of Newborn Medicine, Janeway Children’s Health and Rehabilitation Centre,300 Prince Philip Drive, St. John’s NL, Canada A1B 3V6
Received 27 February 2008; received in revised form 31 July 2008; accepted 6 August 2008
KEYWORDSNeonatalresuscitation;Risk factors;Endotrachealintubation;Positive pressureventilation;Outcomes;Resuscitation team;Quality improvement
SummaryBackground: In the absence of identified risk factors, 7% of term newly borns require PPV-ETT(positive pressure ventilation and/or endotracheal intubation). Factors increasing need forresuscitation, and therefore for individuals with advanced resuscitation skills, require furtherevaluation.Objective: To evaluate the predictive value of ante- and intra-partum risk factors for PPV-ETTin ‘‘at-risk’’ deliveries.Design/methods: Over a 30-month period, the neonatal resuscitation team (NRT) at the tertiaryperinatal centre in St. Johns, Newfoundland and Labrador, prospectively recorded reasons forattending ‘‘at-risk’’ deliveries, and subsequent use of PPV-ETT, rates of low 1- and 5-min Apgarscores, and admission to neonatal intensive care or death.Results: Of 5691 deliveries, 3796 (66.7%) were attended by the NRT. Data were available for3564 (94%) at-risk attendances, of which 780 (22%) required PPV-ETT. Using multivariate logisticregression analysis, significant ante-partum risk factors for PPV-ETT included multiple preg-nancy <35 weeks, maternal infection, hypertension, and oligohydramnios; intra-partum factorswere preterm delivery at <36 weeks, breech presentation, meconium-stained amniotic fluid(MSAF), non-reassuring fetal heart rate, emergency Caesarean section (EmCS), shoulder dysto-cia, and opiates in normal labour. Elective Caesarean section (ElCS) was protective. Forceps,vacuum, and regional or general anaesthesia did not increase risk. EmCS and preterm birthpredicted PPV-ETT, low Apgar scores, and admission to neonatal intensive care (or death), andalong with MSAF, made up the majority of ‘‘at-risk’’ babies.
Conclusions: Given the baselinetertiary centre may not alter ththe exception of ElCS.© 2008 Elsevier Ireland Ltd. All� A Spanish translated version of the summary of this article appears adoi:10.1016/j.resuscitation.2008.08.004.∗ Corresponding author. Tel.: +1 780 735 4670; fax: +1 780 735 4072.
E-mail address: [email protected] (K. Aziz).
0300-9572/$ — see front matter © 2008 Elsevier Ireland Ltd. All rights redoi:10.1016/j.resuscitation.2008.08.004
risk (22%), factors that increase need for resuscitation in ae practice of the NRT attending all ‘‘at-risk’’ deliveries, with
rights reserved.
s Appendix in the final online version at
served.

uotri
M
TiNadddraNwisresd
cppmCsaflpiPf(ia
nparfutlrfteb
Predicting need for neonatal resuscitation
Introduction
For most newly born babies, transition to extrauterine lifeoccurs without the need for resuscitation. For those whomay require assistance, the 2005 American Heart Associa-tion (AHA) Guidelines state that ‘‘Anticipation, adequatepreparation, accurate evaluation, and prompt initiation ofsupport are critical for successful resuscitation’’.1
The AHA Guidelines also point out that ‘‘With careful con-sideration of risk factors, the majority of newborns who willneed resuscitation can be identified’’. A list of ante-partumand intra-partum risk factors may be found in the NeonatalResuscitation Program (NRP) (5th edition, 2006) text,2 how-ever, no mention is made of the relative importance of eachfactor.
Neonatal resuscitation, as taught in the NRP, is, to a largeextent, a basic life support skill: When compromise occurs,the first responder is expected to maintain the infant’s air-way and ensure lung inflation. The more advanced skillsof neonatal resuscitation, particularly on-going ventilation,endotracheal intubation, central venous access, and admin-istration of medications, require the proximity of a secondprovider to assist the first, or to provide the additionalskills. More accurate assessment of risk would ensure theimmediate presence of this additional person in advance ofdelivery.
Certain factors, such as preterm delivery, breech pre-sentation, and meconium-stained amniotic fluid (MSAF),have been established as predictors of need for resuscita-tive interventions. de Almeida et al. recently demonstratedthat late preterm babies were at substantially increasedrisk for neonatal resuscitation when compared to termcounterparts3: they also identified twin gestation, maternalhypertension, nonvertex presentation, Cesarean delivery,and lower gestational age as significant contributors to risk.Vain et al. found that 9% of babies born through MSAFneeded endotracheal suction.4 Molkenboer et al. foundthat term, breech deliveries were 4 times more likelyto need resuscitation by mask.5 It has also been arguedthat elective Caesarean section (C-section) at term has aprotective effect,6 reducing the need for advanced resus-citation skills. Given the numerous factors at play andtheir interaction, validity of these and other factors aspredictors of the need for resuscitation requires furtherevaluation.
An audit of Canadian institutions by Mitchell et al.7 foundthat the need for neonatal resuscitation was not anticipatedin 76% of cases. On the other hand, an audit of resuscitationteam practices (Aziz et al.8) using risk stratification permit-ted the identification of over 80% of babies who requiredpositive pressure ventilation (PPV): in that study, only 7%of babies with no identifiable risk factors required PPV, andall of them responded by 1 min of age (as demonstrated bynormal 1-min Apgar scores). Aziz et al. prospectively cate-gorized deliveries as low, moderate, or high risk accordingto a list of ante- and intra-partum factors, based on NRP rec-ommendations (modified by expert consensus). 16% and 47%
of moderate and high-risk scenarios respectively requiredPPV, supporting the effectiveness of risk stratification.The purpose of this study was to evaluate the relativeimportance of individual ante- and intra-partum risk factorsin determining the need for resuscitation of newborn babies,
losti
445
sing prospective data collected from a complete populationf at-risk newborn babies over a defined time period in a ter-iary perinatal centre. The results may be used to optimizeisk stratification and the planned attendance at delivery byndividuals with appropriate skill levels.
ethods
he Janeway Children’s Health and Rehabilitation Centres the single tertiary perinatal centre for the Province ofewfoundland and Labrador, Canada. As part of an on-goingudit of the Centre’s Neonatal Resuscitation Team (NRT),ata were collected before, and immediately following, alleliveries that were deemed ‘‘at-risk’’ according to a pre-etermined triage process (Table 1).8 As a consequence ofisk stratification, approximately 65% of all deliveries werettended by the NRT. Those deliveries not attended by theRT were cared for by delivery room (case room) staff whoere trained in the basic steps of NRP (including establish-
ng an airway, and bag-mask ventilation), and who wouldummon the NRT if advanced or prolonged resuscitation wasequired. Thus all patients requiring PPV for more than 30 s,ndotracheal intubation, or admission to neonatal inten-ive care would have been entered into the resuscitationatabase.
Immediately following attendance, the NRT nurse wouldomplete a data entry sheet which included (a) documentedarameters, such as gestation (in completed weeks), multi-le pregnancy, presentation (breech, cephalic, and other),ode of delivery (vaginal, elective C-section, or emergency-section, instrumentation (forceps or vacuum), maternaledation (use of opiates), regional or general anaesthesia,nd the presence or absence of meconium-stained amnioticuid; (b) verbally reported parameters, including failure torogress in labour and non-reassuring fetal heart rate trac-ng; (c) need for advanced airway management, includingPV, endotracheal intubation for resuscitation, or intubationor MSAF; (d) Apgar score at 1 and 5 min; and (e) dispositiondeath in the delivery room or transfer to normal nursery orntensive care). Low 1- and 5-min Apgar scores were defineds <4 and <7 respectively.
The nature of attendance at delivery, particularly at shortotice, was such that ‘‘verbally reported’’ ante-partumarameters may have been inconsistently communicatednd therefore suspected to be of limited reliability and accu-acy, particularly in the presence of more than one riskactor — as a consequence, the NRT were asked to doc-ment the single (principal) reason for being called, andhen others, if known. The use of drugs and urgent vascu-ar access for volume expansion was uncommon,8 and wouldarely occur in the absence of PPV-ETT — these were there-ore excluded from the analysis. It should also be notedhat PPV included the increasingly common practice of usingarly CPAP during the resuscitation of extremely pretermabies.
The primary outcome for this analysis, PPV-ETT was col-
ectively defined as the need for PPV or CPAP, or the insertionf an endotracheal tube (for ventilation or suctioning). Theecondary outcomes were: 1 and 5-min Apgar scores lesshan 4 and 7 respectively; and admission to NICU or deathn the delivery room.
446 K. Aziz et al.
Table 1 The levels of risk are assigned for attendance at each delivery, with the NRT attending moderate- and high-riskdeliveries (as well as neonatologists for high-risk deliveries).
Complication(s) Levels of risk
Ante-partum factors
Previous pregnancy loss LOWMultiple pregnancy ≥35 weeks MODMaternal diabetes; maternal hypertension;polyhydramnios; oligohydramnios; IUGR;isoimmunization; maternal infection; minor fetalcomplications
MOD
Multiple pregnancy <35 weeks; major fetalmalformations; hydrops
HIGH
Intra-partum factors
Normal delivery at ≥36 weeks LOWOpiates in normal labour LOWRuptured membranes >18 h LOWElective C-section at full term (normal fetus) MODEmergency C-section for failure to progress MODVacuum or forceps for maternal indications MODMeconium-stained fluid (thick or thin) MODUse of general anaesthesia MOD
Breech presentation MODNon-reassuring fetal heart rate patterns MODNormal delivery at 34 and 35 weeks MODScalp pH 7.1—7.2 MODScalp pH < 7.1 HIGHLess than 34 weeks HIGHElective or emergency C-section before term HIGHEmergency C-section for fetal compromise,
aeviaHIGH
indic
eona
r(uraoaiihoi
fCf
R
FdNwt(t
tbtai
2(t7ddPjpt
Pat((i
prolapsed cord, placenta prVacuum or forceps for fetal
This list was derived from risk factors stated in the Textbook of N
Univariate, bivariate, and multivariate stepwise logisticegression analyses were performed using Systat version 11SPSS Inc.). Two-by-two contingency tables were analysedsing Fisher’s exact test to show crude (unadjusted) oddsatios, p-values, and positive likelihood ratios. Multivari-te logistic regression was used to demonstrate adjusteddds ratios: a backwards, stepwise model, excluding vari-bles with p > 0.15, was created to identify factors that mostnfluenced need for PPV-ETT. 25 risk factors were includedn the model. Previous pregnancy loss, isoimmunization andydrops fetalis were excluded as less than 5 events occurredf each factor. Scalp pH was not included as reason for miss-ng values could not be verified or assumed.
Ethical approval for use of anonymous data was obtainedrom the Human Investigation Committee of the Health Careorporation of St. John’s and Memorial University of New-oundland.
esults
rom 1 February 2002 to 31 August 2004, there were 5691eliveries, of which 3796 (66.7%) were attended by the
RT. Data were complete for 3564 attendances (94%), ofhich 780 (21.9%) required PPV-ETT. The vast majority ofhese were designated moderate (3013, 84.5%) or high risk388, 10.9%) — babies with no identifiable risk factor(s) andhose not attended by the NRT and were not included in
apt
e
or abruptionation HIGH
tal Resuscitation (AAP), and modified by local consensus.8
he dataset. One hundred and sixty-three (4.6%) low riskabies were attended after delivery; 158 of them were dueo late identification of meconium (20 of these received PPVlone, and none were intubated); of the 5 remaining low risknfants, 2 unexpectedly required PPV-ETT.
The gestational age of deliveries attended ranged from3 to 42 weeks inclusive. Of 3564 deliveries attended: 82323%) were through MSAF; 318 (9%) were <36 weeks gesta-ional age; 181 (5%) were products of multiple pregnancies;04 (20%) were emergency C-sections; and 772 (22%) atten-ances were elective C-section at term. The frequency ofocumented ante- and intra-partum risk factors and need forPV-ETT is presented in Tables 2 and 3: These include unad-usted odds ratios, 95% confidence intervals, p-values andositive likelihood ratios for each risk factor with respect tohe primary outcome (PPV-ETT).
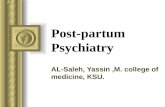
There was a non-linear (U-shaped) association ofPV-ETT frequency with gestational age (Figure 1): itppeared that need for this intervention increased whenhe NRT was requested both for babies with lower gestation<36 weeks) and for those of advanced gestational age>40 weeks). At more advanced gestations, MSAF was anncreasingly common cause for attendance (over 40% of
ttendances after 40 weeks), as well as for subsequentlacement, or attempted placement, of endotrachealubes (Figure 2).Twenty-five ante- and intra-partum factors were consid-red for multivariate logistic regression analysis (Table 4).

Predicting need for neonatal resuscitation 447
Table 2 Two-by-two contingency analysis showing crude (unadjusted) odds ratios, p-values (two-tailed), and positive likelihoodratios for use of PPV-ETT relating to each risk intra-partum factor.
Complication(s) Number ofinfants = 3564
Crude (unadjusted) odds ratios (and 95% confidence intervals)derived from two-by-two contingency tables of ante-partum factors
RequirePPV-ETT (%)
Odds ratio (95%confidence)
p-Value (Fisherexact test)
Positive likelihoodratio
Ante-partum factorsPrevious pregnancy lossa
Multiple pregnancy≥35 weeks
141 25 (22) 0.8 (0.5—1.2) 0.253 0.2
Maternal diabetes 106 22 (21) 0.9 (0.6—1.5) 0.905 0.9Maternal
hypertension180 64 (35) 2.1 (1.5—2.8) 0.000 2.0
Polyhydramnios 8 3 (38) 2.2 (0.6—8.1) 0.384 2.1Oligohydramnios 43 15 (35) 1.9 (1.0—3.6) 0.061 1.9IUGR 50 16 (32) 1.7 (0.9—3.1) 0.086 1.7
Isoimmunizationa
Maternal infection 76 25 (33) 1.7 (1.1—2.8) 0.035 1.7Minor fetal
complications6 2 (33) 1.8 (0.4—8.4) 0.618 1.8
Multiple pregnancy<35 weeks
58 40 (69) 8.3 (4.8—14) 0.000 7.9
Major fetalmalformations
26 9 (35) 1.9 (0.9—4.2) 0.149 1.9
r
Hydropsa
a Vacant cells indicate documented counts less than 5.
Factors that occurred in less than 5 babies, or for whichthere were a substantial number of missing values (specifi-
cally, scalp pH and term babies with no risk factors), wereexcluded from the analysis. A secondary backwards, step-wise analysis revealed similar dominant risk factors (boldedin the table).dtto
Figure 1 There is a non-linear association of gestation with thelowest at 36—40 weeks completed gestational age.
Ante-partum risk factors that predicted PPV-ETT in theegression model included maternal hypertension, oligohy-
ramnios, maternal infection, and multiple pregnancy (lesshan 35 weeks) — each of these approximately doubledhe risk. Polyhydramnios, major fetal malformations, andligohydramnios markedly increased the risk of a low 1-percentage of attendances that require PPV-ETT, rates being

448 K. Aziz et al.
Table 3 Two-by-two contingency analysis showing crude (unadjusted) odds ratios, p-values (two-tailed), and positive likelihoodratios for use of PPV-ETT relating to each risk intra-partum factor.
Complication(s) Number ofinfants = 3564
Crude (unadjusted) odds ratios (and 95% confidence intervals)derived from two-by-two contingency tables of intra-partum factors
RequirePPV-ETT (%)
Odds ratio (95%confidence)
p-Value (Fisherexact test)
Positivelikelihood ratio
Opiates in normal labour 108 33 (31) 1.6 (1.1—2.4) 0.033 1.6Ruptured membranes >18 h 418 96 (23) 1.1 (0.8—1.4) 0.571 1.1Elective C—section at full term
(normal fetus)772 55 (7) 0.2 (0.16—0.3) 0.000 0.3
Failure to progress 349 58 (17) 0.7 (0.5—0.9) 0.012 0.7Vacuum delivery 436 78 (18) 0.8 (0.6—1.0) 0.031 0.8Forceps delivery 333 74 (22) 1.0 (0.8—1.3) 0.889 1.0Meconium—stained fluid (thick
or thin)823 269 (33) 2.1 (1.8—2.5) 0.000 2.0
Use of general anaesthesia 53 26 (49) 3.5 (2.1—6.0) 0.000 3.4Breech presentation 314 77 (25) 1.2 (0.9—1.5) 0.253 1.2Non-reassuring fetal heart rate
patterns608 152 (25) 1.2 (1.0—1.5) 0.046 1.2
Normal delivery at 34 and 35weeks
122 31 (25.4) 1.2 (0.8—1.9) 0.372 1.2
Scalp pH 7.1—7.2a
Scalp pH < 7.1a
Less than 34 weeks 196 146 (75) 13 (9.0—18) 0.000 10.4Emergency C-section for fetal
compromise, prolapsed cord,placenta praevia orabruption (or pretermsection)
704 235 (33) 2.1 (1.8—2.6) 0.000 1.8
Shoulder dystocia 11 5 (45) 3.0 (1.0—9.2) 0.071 3.0Regional anaesthesia 1777 374 (21) 0.9 (0.8—1.1) 0.240 1.0
a Vacant cells indicate substantial missing values.
Figure 2 Meconium-stained amniotic fluid (MSAF) is increasingly common among attendances at later gestations, paralleled by arise in the likelihood of tracheal intubation for suctioning of MSAF.

Predictingneed
forneonatalresuscitation
449
Table 4 Designated levels of risk by complication demonstrating significant (adjusted) odds ratios and 95% confidence intervals (p < 0.05) of stepwise multivariate logisticregressions for each of the 5 major outcome variables.
Complication(s) Level of risk Significant (adjusted) odds ratios (95% confidence intervals)a
Need for PPV-ETT(n = 3564)
1 min Apgar <4(n = 3564)
5 min Apgar <7(n = 3564)
Admit to NICU ordeath (n = 3564)
Ante-partum factorsPrevious pregnancy lossb LOW
Multiple pregnancy > = 35 weeks MOD 1.3 (0.8—2.1) 0.8 (0.2—3.6) 0.4 (0.1—3.3) 2.6 (1.6—4.2)Maternal diabetes MOD 1.0 (0.6—1.7) 0.6 (0.1—2.9) 0.4 (0.05—3.0) 1.7 (0.9—3.0)Maternal hypertension MOD 1.8 (1.2—2.6) 0.6 (0.3—1.6) 0.6 (0.2—1.6) 2.2 (1.4—3.4)Polyhydramnios MOD 2.6 (0.5—13) 20((3.7—112) 8.1 (0.8—77) 2.2 (0.3—19)Oligohydramnios MOD 1.8 (0.9—3.7) 5.8 (1.8—18) 5.6 (1.5—21) 2.1 (0.9—5.0)IUGR MOD 1.8 (0.9—3.5) 3.0 (1.4—6.3)
Isoimmunizationb MODMaternal infection MOD 1.7 (1.0—2.9) 2.0 (0.6—7.1) 2.1 (0.6—7.3) 2.4 (1.2—4.8)Minor fetal complications MOD 1.5 (0.2—9.6) 1.3 (0.2—9.2)Multiple pregnancy <35 weeks HIGH 2.1 (1.0—4.2) 1.5 (0.6—3.7) 0.9 (0.4—2.4) 20((4.3—95)Major fetal malformations HIGH 1.9 (0.8—4.9) 4.2 (1.1—16) 2.3 (0.4—12) 34 (13—88)
Hydropsb HIGH
Intra-partum factorsOpiates in normal labour LOW 1.6 (1.0—2.6) 2.0 (0.7—6.1) 1.0 (0.2—4.4) 0.8 (0.4—1.8)Ruptured membranes >18 h LOW 1.3 (1.0—1.7) 0.7 (0.3—1.5) 0.9 (0.4—1.8) 1.1 (0.7—1.7)Elective C—section at full term (normal fetus) MOD 0.4 (0.3—0.5) 0.2 (0.1—0.8) 0.3 (0.1—1.1) 0.9 (0.6—1.4)Failure to progress MOD 0.9 (0.6—1.3) 0.7 (0.3—1.6) 0.4 (0.1—1.3) 0.2 (0.1—0.4)Vacuum delivery MOD 1.0 (0.8—1.3) 1.5 (0.7—3.2) 2.2 (1.1—4.8) 1.2 (0.8—1.8)Forceps delivery MOD 1.1 (0.8—1.5) 1.2 (0.6—2.5) 1.7 (0.8—3.5) 1.1 (0.7—1.8)Meconium—stained fluid (thick or thin) MOD 3.1 (2.6—3.9) 2.1 (1.2—3.7) 1.5 (0.8—2.9) 1.1 (0.8—1.5)Use of general anaesthesia MOD 1.8 (0.9—3.6) 4.6 (1.7—13) 2.2 (0.7—7.2) 1.7 (0.7—4.0)Breech presentation MOD 1.9 (1.3—2.7) 0.8 (0.4—1.9) 0.5 (0.2—1.3) 1.8 (1.2—2.7)Non—reassuring fetal heart rate patterns MOD 1.4 (1.1—1.8) 0.5 (0.3—1.0) 0.7 (0.3—1.4) 1.0 (0.7—1.4)Normal delivery at 34 and 35 weeks MOD 1.8 (1.2—2.9) 1.8 (0.5—6.2) 3.8 (1.2—12) 20 (13—31)
Scalp pH 7.1—7.2c MODScalp pH < 7.1c HIGH

450
Tabl
e4
(Con
tinu
ed)
Com
plic
atio
n(s)
Leve
lof
risk
Sign
ifica
nt(a
djus
ted)
odds
rati
os(9
5%co
nfide
nce
inte
rval
s)a
Nee
dfo
rPP
V-ET
T(n
=35
64)
1m
inAp
gar
<4(n
=35
64)
5m
inAp
gar
<7(n
=35
64)
Adm
itto
NIC
Uor
deat
h(n
=35
64)
HIG
H13
((9.
0—19
)6.
7(3
.5—
13)
11((
5.4—
21)
646
(200
—20
91)
Emer
genc
yC—
sect
ion
for
feta
lco
mpr
omis
e,pr
olap
sed
cord
,pl
acen
tapr
aevi
aor
abru
ptio
n(o
rpr
eter
mse
ctio
n)
HIG
H1.
4(1
.0—
1.8)
2.1
(1.2
—3.
8)2.
9(1
.6—
5.4)
4.2
(2.9
—5.
9)
Shou
lder
dyst
ocia
—6.
3(1
.9—
21)
16((
3.1—
79)
Regi
onal
anae
sthe
sia
—1.
0(0
.9—
1.3)
1.5
(0.9
—2.
5)1.
4(0
.8—
2.5)
1.1
(0.8
—1.
5)
Bold
ing
indi
cate
ssi
gnifi
cant
fact
ors
inth
eba
ckw
ards
,st
epw
ise
anal
ysis
.a
Der
ived
from
mul
tiva
riat
elo
gist
icre
gres
sion
anal
ysis
of25
ante
-par
tum
and
intr
a-pa
rtum
fact
ors
(vac
ant
cells
indi
cate
mis
sing
valu
es,
insu
ffici
ent
data
,or
noev
ents
).Bo
ldin
gin
dica
tes
sign
ifica
nce
ina
back
war
ds,
step
wis
elo
gist
icre
gres
sion
anal
ysis
atp
<0.
05.
bVa
cant
cells
indi
cate
insu
ffici
ent
num
bers
.c
Vaca
ntce
llsin
dica
tem
issi
ngda
ta.
msd
Ei(rCcaus
Clswp
aadpp
‘im15
D
Tecwtanrspf(isptrapw1
coiof
K. Aziz et al.
in Apgars — with the latter also impacting 5-min Apgarcores. A number of factors predicted admission to NICU oreath.
For intra-partum risk factors the primary outcome of PPV-TT was associated with low gestation (<36 weeks), with riskncreasing substantially at <34 weeks gestation (odds ratioOR) 13, 95% confidence interval 9.0—19). Other significantisk factors included MSAF, breech presentation, emergency-section, non-reassuring heart rate, and shoulder dysto-ia. Elective C-section was protective (OR 0.4, CI 0.3—0.5)gainst the need for PPV-ETT. Instrumental delivery (vac-um or forceps) and regional anaesthesia were not found toignificantly increase risk.
Low 1-min Apgar was predicted by gestation <34 weeks,-section under general anaesthesia, and MSAF, but not by
ate preterm delivery (34 or 35 weeks); again, elective C-ection being protective. Low 5-min Apgar was associatedith vacuum-assisted delivery, emergency C-section andreterm delivery (<36 weeks).
MSAF and vacuum-assisted delivery, however, were notssociated with admission to NICU or death. The strongestssociations with NICU admission or death were pretermelivery (<36 weeks), emergency C-section, and multipleregnancy. Elective C-section and failure to progress wererotective for this outcome.
A post hoc analysis of 761 C-sections described as‘elective’’ showed that 82 (10.8%) occurred at 35—37 weeksnclusive, and that these early deliveries were significantlyore likely to result in PPV-ETT (unadjusted 0R 3.5, 95% CI
.8—3.8) or admission to NICU (unadjusted 0R 12, 95% CI
.9—24) than those at 38 or more weeks gestation.
iscussion
his is a prospective study of a complete cohort of mod-rate and high-risk newborns born in a Canadian perinatalentre — it is important to note that ‘‘low-risk’’ babiesith no identifiable risk factor(s) were not included in
he analysis. The study evaluates the association of ante-nd intra-partum risk factors with the likelihood of earlyeonatal morbidities, as reflected by the need for, and theesponse to, neonatal resuscitation. The principal findingsuggest, firstly, that there are ante-partum and intra-artum factors which are associated with increased needor PPV-ETT, low Apgar scores, and admission to NICUor death); secondly, that multiple pregnancy, maternalnfection, maternal hypertension, and oligohydramnios areignificant ante-partum factors with respect to need for res-iratory support during resuscitation (PPV-ETT); and thirdly,hat preterm delivery, breech presentation, MSAF, non-eassuring heart rate patterns, and emergency C-sectionre significant intra-partum factors for PPV-ETT — of these,reterm delivery (<34 weeks) has the greatest effect,ith an unadjusted positive likelihood ratio exceeding0.
It is interesting that, despite the resource and medi-
olegal implications of unexpected neonatal resuscitation,ur literature search revealed a limited number of sim-lar observational studies that looked at a wide rangef risk factors.3—6 It was only through the purpose-ul audit of neonatal resuscitation team practices that
deCsNaaf
agcepdqmd
toomvprlfdaa
amigmltont
nnpiboptfdp
C
Predicting need for neonatal resuscitation
these data were obtained — thus reinforcing the valu-able role of teams in quality improvement and researchinitiatives.
On the surface, it appears that risk stratification, partic-ularly using factors with higher and significant odds ratios,might improve the likelihood that a skilled team is in atten-dance at moderate and high-risk deliveries. Unfortunately,the poor sensitivity and specificity of most risk factors forpredicting need for resuscitation meant that the resus-citation team attended over half of all deliveries. Thebaseline rate for PPV-ETT (22%) for moderate and high-riskdelivery was such that one would be reluctant to removerisk factors unless they were demonstrated to be protec-tive. The only such risk factor was uncomplicated electiveC-section, which represented approximately one-fifth ofattendances and reduced risk by 60%; a caveat being thatelective C-section at less than 38 weeks conferred markedlyincreased risk of PPV-ETT and admission to NICU. Ourstudy was insufficiently powered to discriminate between38 and 39 weeks, but our observation is consistent publisheddata.9
Approximately 5% of attendances were low-risk, largelyin association with late identification of meconium in amni-otic fluid — 14% of low-risk babies needed PPV-ETT (less thanthe population risk): we feel that including these data clar-ified NRT function, and did not adversely affect the analysisor conclusions.
A useful observation is that preterm delivery (<36 weeks),MSAF, obstetrical emergencies (including shoulder dystociaand those requiring general anaesthesia), and breech pre-sentation contributed to over one-third of all attendances,and to a substantial proportion of risk: these factors shouldcertainly be targeted by a resuscitation team. Our dataalso add to the concern that babies at 34 and 35 weekshave increased need for resuscitation,3 and therefore forthe presence of skilled and experienced caregivers. Simi-larly, one should not underestimate the importance of skilledoperators when caring for infants with MSAF, many of whom,given current guidelines,2 require endotracheal intubationimmediately following birth.
Something our analysis cannot tell us is what absenceof risk factors predicts, as these babies were not attendedby the NRT, and therefore not entered into our database.However, previously published data from this centre suggestthat caseroom (delivery room) staff can be trained to pro-vide initial support to low risk babies requiring brief periodsof PPV8 without increased neonatal morbidity — it appearsthat approximately 7% of normal term deliveries effectivelyreceived this support in that population.
Of the ante-partum risk factors, it is noteworthy thatmaternal hypertension, maternal infection, multiple preg-nancy, and oligohydramnios are independent risk factors forneed for PPV-ETT. They are not uncommon and resuscitatorsshould be aware of the increased risk. Most would already beaware of the minimal increase in risk associated with opiatesin normal labour.
The measurement of 1- and 5-min Apgar scores pro-
duced interesting results but it was difficult to make outa distinct pattern that related need for PPV-ETT to sub-sequent low Apgar scores, and then to admission to NICU.We should not be surprised by this lack of association asApgar score is documented ‘‘after the fact’’, and thereforeIiqfi
451
oes not necessarily reflect the need for resuscitation. Thexceptions were preterm birth (<34 weeks) and emergency-section, which, not unexpectedly, demonstrated a clearequence from resuscitation, to low Apgar scores, and toICU admission. The attendance of the NRT, who also initi-ted stabilization (including ventilation and line placement)nd admission to NICU, contributed to the continuity of careor these babies.
A potential limitation of this study is the question ofccuracy of documented risk factors. These data wereathered in an environment where a dedicated NRT, whoollectively attended several thousand deliveries over sev-ral years. Although the data abstraction forms wererepared prospectively, and staff were trained and man-ated to enter data immediately following delivery as auality improvement initiative, biases of definition, com-unication, and interpretation could have influenced theocumentation.
Communication played a very important part in the func-ioning of the team, and certainly would in the translation ofur conclusions into practice. Poor communication betweenbstetric and neonatal services would undoubtedly result inissed risk factors, perhaps an explanation for the obser-
ations of Mitchell et al.7 that need for resuscitation isoorly predicted. Good lines of communication would permitapid deployment of the team in situations where prob-ems were unexpected. Given the dedicated role of theull-time NRT nurse to the delivery area, and prospectiveocumentation, it is likely that our data on risk factorsre an accurate representation of the main reasons forttendance.
The NRT consisted of an experienced neonatal nurseccompanied by a respiratory therapist (and resident oredical staff when indicated). Many team members were
nstructors in neonatal resuscitation. One might question theeneralizability of these results to centres where resourcesay be limited, or resuscitators with advanced skills may be
ess available. We believe, however, that the expertise ofhe team enhances the validity of our results, both in termsf data collection, and in terms of assessment of each baby’seed for resuscitation. We remain strong advocates of theeam approach in perinatal centres.
Perhaps the greatest concern for all responsible foreonatal resuscitation is that a newly born will unexpectedlyeed advanced resuscitation, and that staff with the appro-riate skill set will not be immediately available. This studys insufficiently powered to predict these events, and noneut the largest tertiary centres can ensure maximal responsef experienced resuscitators for every delivery. Realistically,olicies should be in place to make sure that initial resuscita-ion can be provided by all healthcare providers responsibleor newly born infants10 Data from this study may helpetermine when the second line of resuscitators should beresent.
onclusion
n conclusion, this paper outlines factors that significantlyncrease the need for neonatal resuscitation and subse-uent admission to NICU in ‘‘at-risk’’ deliveries. Thesendings may be beneficial in developing strategies to

4
aaut
C
N
A
TsgtaWNp
R
52
nticipate circumstances which require individuals withdvanced neonatal resuscitation skills. They may also beseful in developing and evaluating neonatal resuscitationeams.
onflicts of interest
one to declare.
cknowledgements
his study was supported by a Memorial University summertudent grant and in-kind support of Eastern Health Inte-rated Regional Health Authority. We wish to acknowledgehe support and diligence of the nurses, respiratory ther-pists, and physicians of the Neonatal Resuscitation Team.e wish to thank Ms. Janet Halabi, Royal Alexandra Hospitaleonatal Intensive Care Unit, for her help with manuscriptreparation.
eferences
1. American Heart Association. American Heart Association(AHA) guidelines for Cardiopulmonary Resuscitation (CPR) andEmergency Cardiovascular Care (ECC) of pediatric and neona-tal patients: neonatal resuscitation guidelines. Circulation2005;112(Suppl I):IV-188—95.
1
K. Aziz et al.
2. American Academy of Pediatrics. Textbook of neonatal resusci-tation. 5th ed. American Academy of Pediatrics and AmericanHeart Association; 2006.
3. de Almeida MF, Guinsburg R, da Costa JO, Anchieta LM, FreireLM, Campos Junior D. Resuscitative procedures at birth in latepreterm infants. J Perinatol 2007;27(12):761—5 [Epub 2007October 25].
4. Vain NE, Szyld EG, Prudent LM, Wiswell TE, Aguilar AM, VivasNI. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multi-centre, randomised controlled trial. Lancet 2004;364(August(9434)):597—602.
5. Molkenboer JF, Vencken PM, Sonnemans LG, et al. Conservativemanagement in breech deliveries leads to similar results com-pared with cephalic deliveries. J Matern Fetal Neonatal Med2007;20(8):599—603.
6. Hogston P. Is a paediatrician required at caesarean section? EurJ Obstet Gynecol Reprod Biol 1987;26(1):91—3.
7. Mitchell A, Niday P, Boulton J, Chance G, Dulberg C. A prospec-tive clinical audit of neonatal resuscitation practices in Canada.Adv Neonatal Care 2002;2(6):316—26.
8. Aziz K, Chadwick M, Downton G, Baker M, Andrews W. The devel-opment and implementation of a multidisciplinary neonatalresuscitation team in a Canadian perinatal centre. Resuscitation2005;66(1):45—51.
9. Zanardo V, Simbi KA, Vedovato S, Trevisanuto D. The influence
of timing of elective cesarean section on neonatal resuscitationrisk. Pediatr Crit Care Med 2004;5(6):566—70.0. Health Canada. Family-centred maternity and newborn care:national guidelines. Ottawa: Minister of Public Works and Gov-ernment Services; 2000.