Predicting Answering Behaviour in Online Question Answering Communities
Executive summary: Improved care results in cost savingsSeveral tools are currently being deployed in provider environments to improve
quality and efficiency of care. Chief among these are electronic medical records
(EMR), computerized physician order entry (CPOE), E-prescribing, and medication
bar-coding systems.
However, it is imperative that quality improvement initiatives also include a
clinical knowledge system. Physicians generate one question for every two or
three patient encounters and two-thirds of those questions go unanswered.
If physicians had access to the appropriate clinical information system, and
could answer clinical questions as they arise, some 40 percent of management
decisions would be changed, improving patient care. Regularly updated electronic
clinical knowledge systems have decreased barriers to answering these questions.
However, there has previously been little evidence as to whether they have an
impact on health outcomes.
The Hospital Clinical Knowledge Systems and Health Outcomes Study was
designed to evaluate whether a leading clinical knowledge system (UpToDate®)
was associated with improvement in patient safety and efficiency in hospitalized
patients, and to estimate the financial impact associated with its implementation.
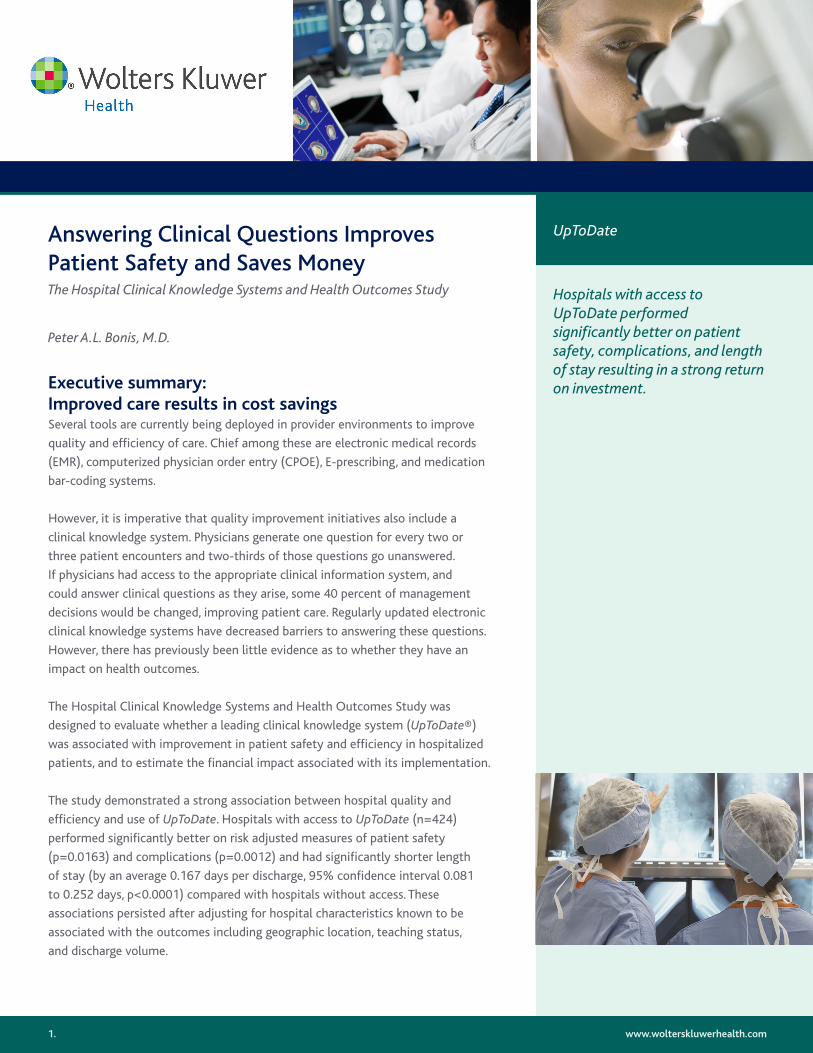
The study demonstrated a strong association between hospital quality and
efficiency and use of UpToDate. Hospitals with access to UpToDate (n=424)
performed significantly better on risk adjusted measures of patient safety
(p=0.0163) and complications (p=0.0012) and had significantly shorter length
of stay (by an average 0.167 days per discharge, 95% confidence interval 0.081
to 0.252 days, p<0.0001) compared with hospitals without access. These
associations persisted after adjusting for hospital characteristics known to be
associated with the outcomes including geographic location, teaching status,
and discharge volume.
Answering Clinical Questions Improves Patient Safety and Saves MoneyThe Hospital Clinical Knowledge Systems and Health Outcomes Study
Peter A.L. Bonis, M.D.
www.wolterskluwerhealth.com
Hospitals with access to UpToDate performed significantly better on patient safety, complications, and length of stay resulting in a strong return on investment.
UpToDate
1.
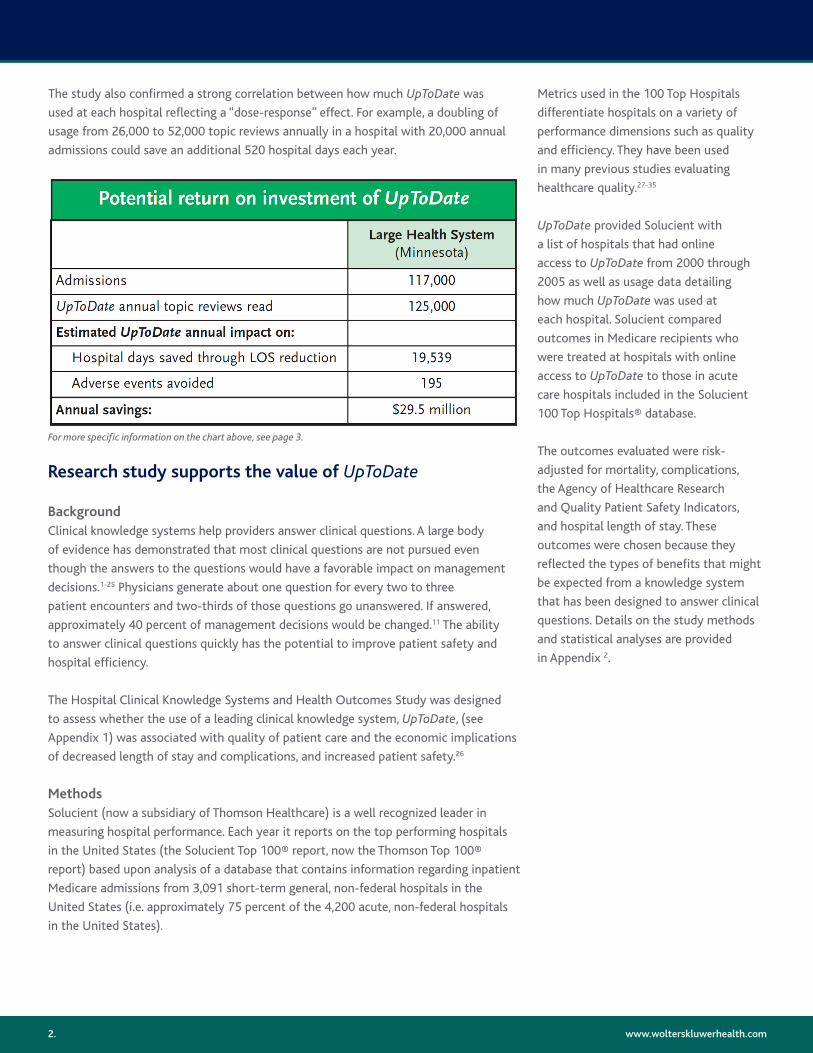
The study also confirmed a strong correlation between how much UpToDate was
used at each hospital reflecting a “dose-response” effect. For example, a doubling of
usage from 26,000 to 52,000 topic reviews annually in a hospital with 20,000 annual
admissions could save an additional 520 hospital days each year.
www.wolterskluwerhealth.com
Research study supports the value of UpToDate
BackgroundClinical knowledge systems help providers answer clinical questions. A large body
of evidence has demonstrated that most clinical questions are not pursued even
though the answers to the questions would have a favorable impact on management
decisions.1-25 Physicians generate about one question for every two to three
patient encounters and two-thirds of those questions go unanswered. If answered,
approximately 40 percent of management decisions would be changed.11 The ability
to answer clinical questions quickly has the potential to improve patient safety and
hospital efficiency.
The Hospital Clinical Knowledge Systems and Health Outcomes Study was designed
to assess whether the use of a leading clinical knowledge system, UpToDate, (see
Appendix 1) was associated with quality of patient care and the economic implications
of decreased length of stay and complications, and increased patient safety.26
MethodsSolucient (now a subsidiary of Thomson Healthcare) is a well recognized leader in
measuring hospital performance. Each year it reports on the top performing hospitals
in the United States (the Solucient Top 100® report, now the Thomson Top 100®
report) based upon analysis of a database that contains information regarding inpatient
Medicare admissions from 3,091 short-term general, non-federal hospitals in the
United States (i.e. approximately 75 percent of the 4,200 acute, non-federal hospitals
in the United States).
Metrics used in the 100 Top Hospitals
differentiate hospitals on a variety of
performance dimensions such as quality
and efficiency. They have been used
in many previous studies evaluating
healthcare quality.27-35
UpToDate provided Solucient with
a list of hospitals that had online
access to UpToDate from 2000 through
2005 as well as usage data detailing
how much UpToDate was used at
each hospital. Solucient compared
outcomes in Medicare recipients who
were treated at hospitals with online
access to UpToDate to those in acute
care hospitals included in the Solucient
100 Top Hospitals® database.
The outcomes evaluated were risk-
adjusted for mortality, complications,
the Agency of Healthcare Research
and Quality Patient Safety Indicators,
and hospital length of stay. These
outcomes were chosen because they
reflected the types of benefits that might
be expected from a knowledge system
that has been designed to answer clinical
questions. Details on the study methods
and statistical analyses are provided
in Appendix 2.
2.
For more specific information on the chart above, see page 3.
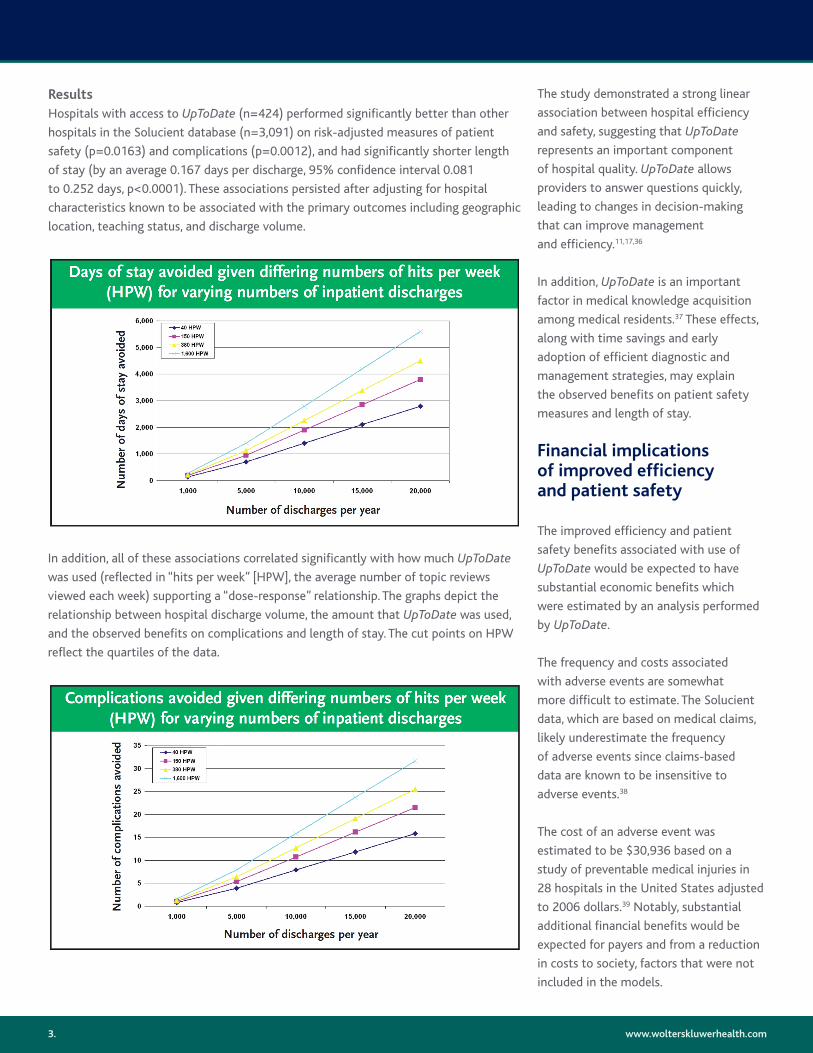
ResultsHospitals with access to UpToDate (n=424) performed significantly better than other
hospitals in the Solucient database (n=3,091) on risk-adjusted measures of patient
safety (p=0.0163) and complications (p=0.0012), and had significantly shorter length
of stay (by an average 0.167 days per discharge, 95% confidence interval 0.081
to 0.252 days, p<0.0001). These associations persisted after adjusting for hospital
characteristics known to be associated with the primary outcomes including geographic
location, teaching status, and discharge volume.
www.wolterskluwerhealth.com
In addition, all of these associations correlated significantly with how much UpToDate
was used (reflected in “hits per week” [HPW], the average number of topic reviews
viewed each week) supporting a “dose-response” relationship. The graphs depict the
relationship between hospital discharge volume, the amount that UpToDate was used,
and the observed benefits on complications and length of stay. The cut points on HPW
reflect the quartiles of the data.
The study demonstrated a strong linear
association between hospital efficiency
and safety, suggesting that UpToDate
represents an important component
of hospital quality. UpToDate allows
providers to answer questions quickly,
leading to changes in decision-making
that can improve management
and efficiency.11,17,36
In addition, UpToDate is an important
factor in medical knowledge acquisition
among medical residents.37 These effects,
along with time savings and early
adoption of efficient diagnostic and
management strategies, may explain
the observed benefits on patient safety
measures and length of stay.
Financial implications of improved efficiency and patient safety
The improved efficiency and patient
safety benefits associated with use of
UpToDate would be expected to have
substantial economic benefits which
were estimated by an analysis performed
by UpToDate.
The frequency and costs associated
with adverse events are somewhat
more difficult to estimate. The Solucient
data, which are based on medical claims,
likely underestimate the frequency
of adverse events since claims-based
data are known to be insensitive to
adverse events.38
The cost of an adverse event was
estimated to be $30,936 based on a
study of preventable medical injuries in
28 hospitals in the United States adjusted
to 2006 dollars.39 Notably, substantial
additional financial benefits would be
expected for payers and from a reduction
in costs to society, factors that were not
included in the models.
3.
The financial impact of UpToDate is directly associated with the amount that UpToDate
is used at each hospital. Use grows spontaneously year after year (both in the number
of users and the amount of use for each user) at hospitals that subscribe. Thus, the
economic benefits described above would grow proportionally to the rate of adoption
and the amount that UpToDate is used. Efforts to stimulate use of UpToDate could
further increase the benefits.
www.wolterskluwerhealth.com
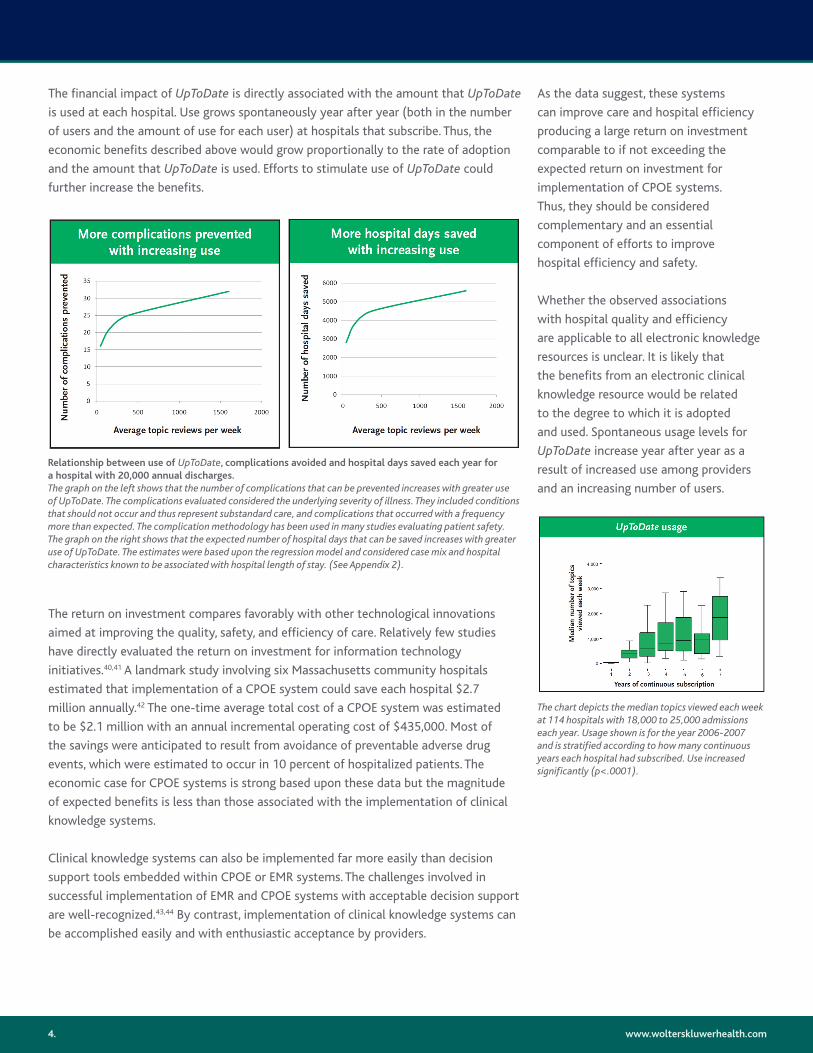
Relationship between use of UpToDate, complications avoided and hospital days saved each year for a hospital with 20,000 annual discharges. The graph on the left shows that the number of complications that can be prevented increases with greater use of UpToDate. The complications evaluated considered the underlying severity of illness. They included conditions that should not occur and thus represent substandard care, and complications that occurred with a frequency more than expected. The complication methodology has been used in many studies evaluating patient safety. The graph on the right shows that the expected number of hospital days that can be saved increases with greater use of UpToDate. The estimates were based upon the regression model and considered case mix and hospital characteristics known to be associated with hospital length of stay. (See Appendix 2).
As the data suggest, these systems
can improve care and hospital efficiency
producing a large return on investment
comparable to if not exceeding the
expected return on investment for
implementation of CPOE systems.
Thus, they should be considered
complementary and an essential
component of efforts to improve
hospital efficiency and safety.
Whether the observed associations
with hospital quality and efficiency
are applicable to all electronic knowledge
resources is unclear. It is likely that
the benefits from an electronic clinical
knowledge resource would be related
to the degree to which it is adopted
and used. Spontaneous usage levels for
UpToDate increase year after year as a
result of increased use among providers
and an increasing number of users.
The return on investment compares favorably with other technological innovations
aimed at improving the quality, safety, and efficiency of care. Relatively few studies
have directly evaluated the return on investment for information technology
initiatives.40,41 A landmark study involving six Massachusetts community hospitals
estimated that implementation of a CPOE system could save each hospital $2.7
million annually.42 The one-time average total cost of a CPOE system was estimated
to be $2.1 million with an annual incremental operating cost of $435,000. Most of
the savings were anticipated to result from avoidance of preventable adverse drug
events, which were estimated to occur in 10 percent of hospitalized patients. The
economic case for CPOE systems is strong based upon these data but the magnitude
of expected benefits is less than those associated with the implementation of clinical
knowledge systems.
Clinical knowledge systems can also be implemented far more easily than decision
support tools embedded within CPOE or EMR systems. The challenges involved in
successful implementation of EMR and CPOE systems with acceptable decision support
are well-recognized.43,44 By contrast, implementation of clinical knowledge systems can
be accomplished easily and with enthusiastic acceptance by providers.
The chart depicts the median topics viewed each week at 114 hospitals with 18,000 to 25,000 admissions each year. Usage shown is for the year 2006-2007 and is stratified according to how many continuous years each hospital had subscribed. Use increased significantly (p<.0001).
4.
www.wolterskluwerhealth.com
Use of UpToDate was an independent
predictor of performance. Remarkably,
use for 20 minutes a day was associated
with a comparable increase in IM-ITE
scores as an entire year of residency.
Methods to increase use Increased benefits from clinical
knowledge support systems can be
realized by increasing their usage. For
example, a doubling of UpToDate usage
from 500 to 1000 topic reviews per
week in a hospital with 20,000 annual
discharges could result in more than
520 hospital days saved each year (and
more than $800,000 in annual savings).
Increasing use can be accomplished by:
• Increasing awareness and training
• Reducing the click distance to the
resource by integrating it into the
EMR system
• Rewarding providers for use by granting
continuing medical education credits
Conclusions and recommendationsMany factors are involved in hospital
quality and efficiency. The value of
clinical knowledge systems such as
UpToDate as part of efforts to improve
care has not been fully recognized.
The Hospital Clinical Knowledge
Systems and Health Outcomes Study
demonstrated that use of an electronic
clinical knowledge system was associated
with hospital quality and efficiency.
Such systems can improve care and
efficiency and are well-accepted by
providers. The benefits on patient
safety and efficiency also translate into
a large return on investment, and require
minimal resources to be implemented.
That return on investment can be
continually improved by efforts to
increase usage.
The march toward broad implementation
of electronic medical record, CPOE,
E-prescribing, and medication bar-coding
systems is continuing. The costs and
complexity involved in implementing
such systems have overshadowed the
comparatively easily acquired benefits
of implementing clinical knowledge
support systems.
Such systems can be implemented
rapidly leading to almost immediate
improvements in patient care. In
addition, these systems are important
for education of trainees and continuing
medical education of providers.
The acceptance of UpToDate among
providers has translated into widespread
adoption. Over 88% of academic medical
centers in the United States subscribe to
UpToDate and nearly 320,000 healthcare
providers use it worldwide. About 98
percent of hospitals that subscribe
to UpToDate continue to renew their
subscription year after year. UpToDate
users at these hospitals depend on it for
their practices. Hospitals that subscribe to
UpToDate frequently report that providing
access is important for recruiting and
retaining their physicians.
Studies of users in community hospitals
have demonstrated that use is not
confined to doctors. UpToDate is also
used extensively by nurses, nurse
practitioners, physician assistants, and
pharmacists. This permits UpToDate to
become the standard of care, thereby
helping to ensure consistent care that
is well-integrated across all caregivers.
This degree of use means that UpToDate
impacts more than 90 million patient
visits a year in more than 140 countries.
Use has an impact on learning The widespread adoption and use
of UpToDate has had an impact on
learning among providers and trainees.
A study performed by the Mayo Clinic,
for example, examined the impact of
learning habits (use of UpToDate and
conference attendance) on medical
knowledge acquisition as measured
by the Internal Medicine In-training
Examination (IM-ITE).37 The IM-ITE
assesses medical knowledge acquisition
during residency; scores correlate
with subsequent performance on the
American Board of Internal Medicine
Certification Examination.
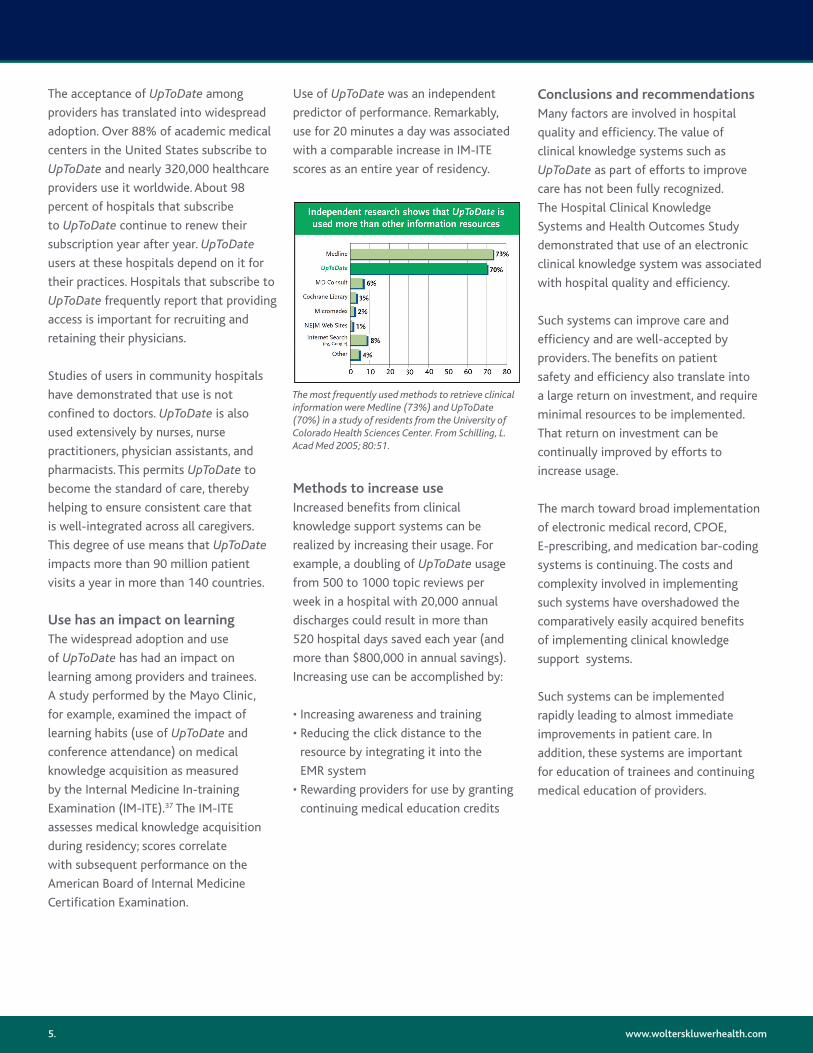
The most frequently used methods to retrieve clinical information were Medline (73%) and UpToDate (70%) in a study of residents from the University of Colorado Health Sciences Center. From Schilling, L. Acad Med 2005; 80:51.
5.
Appendix 1: Description of UpToDate
UpToDate is an evidence-based, peer reviewed information resource—available via the
Web, desktop, and PDA. UpToDate is designed to answer clinical questions quickly and
provide synthesized recommendations for treatment. Over 90 million patient-related
problems are researched each year with UpToDate.
The UpToDate community includes our faculty of more than 3,800 leading physicians,
peer reviewers, and editors and nearly 320,000 users. Our faculty writes topic
reviews that include a synthesis of the literature, the latest evidence, and specific
recommendations for patient care. Our users provide feedback to the editorial group.
This community’s combined efforts result in the most trusted, unbiased medical
information available.
UpToDate is available through institutional or individual subscriptions. Providers at
hospitals that subscribe to UpToDate can access it through an Internet connection
at any terminal within the facility.
UpToDate contentUpToDate includes more than 7,400 clinical topics, each an average of 10 pages of
text, figures, references, and abstracts, as well as drug and drug interactions programs,
guidelines, patient handouts, and clinical calculators. Access to the content of UpToDate
is through a search screen with a search box. UpToDate uses a proprietary search
engine. The search engine is not static but undergoing continual adjustments to
provide the best search results given the content offering. The search engine can handle
multiple concepts from a “natural language” question like: Treatment of hypertension
in a pregnancy. The search concepts here are: treatment, hypertension, and pregnancy.
During the search, the entire database gets reorganized in order of relevancy.
AuthorsAll topics in UpToDate are written by the listed authors in conjunction with a deputy
editor. Authors are identified as experts by the Editors-in-Chief, our editorial staff,
and participating societies.
www.wolterskluwerhealth.com
Exceptions are guidelines from major
societies, which are added to UpToDate
in their original form. All material is
originally prepared by the contributing
author(s) whose name(s) and affiliation(s)
appear in the upper left corner of
each topic.
This material is reviewed extensively by
our physician editors and peer reviewers
for accuracy and completeness of the
literature search, and for consistency
with all aspects of the editorial policy.
Physician editors suggest changes
to ensure that the topics summarize
the relevant evidence, and that the
recommendations are consistent with
the evidence, with our understanding of
patients’ values and preferences, and with
UpToDate’s editorial policy. Some of the
content may be taken from other topics
in UpToDate. In such cases, the text is
hyperlinked to the topic from which
it originated.
EvidenceUpToDate follows a hierarchy of evidence
consistent with most evidence-based
resources. At the top of the hierarchy are
randomized trials of high methodological
quality, followed by randomized trials with
methodological limitations, observational
studies, and unsystematic clinical
observations. Inferences are stronger
when the evidence is summarized in
systematic reviews of the literature that
present all relevant data.
Each topic has an author who is an
expert in the area discussed, and at
least two separate physician reviewers.
This group works together to perform
a comprehensive review of the
literature and carefully select studies
for presentation based upon the quality
of the study, the hierarchy of evidence
discussed above, and clinical relevance.
6.
When current, high-quality systematic reviews are available, UpToDate topics and
recommendations rely heavily on these reviews. When such reviews are unavailable,
UpToDate summarizes the key studies bearing on the clinical issues at hand. Systematic
reviews and the design of primary studies (randomized trial, observational studies) are
often identified explicitly in the text with the relevant data. However, in cases where
either the type of study or the data are not stated explicitly, users can click on the
reference and bring up the Medline abstract to obtain this information. Evidence is
derived from a number of resources, including but not limited to:
• Hand-searching of over 400 peer reviewed journals
• Electronic searching of databases including MEDLINE, The Cochrane Database,
Clinical Evidence, and ACP Journal Club
• Guidelines that adhere to principles of evidence evaluation described above
• Published information regarding clinical trials such as reports from the Food and Drug
Administration, as well as other sources of information produced by federal agencies
such as the Centers for Disease Control and Prevention and the National Institutes
of Health
• Proceedings of major national meetings
• The clinical experience and observations of our authors, editors, and peer reviewers
RecommendationsUpToDate strives to provide a “Summary and Recommendations” section
(see figure below) where appropriate.
www.wolterskluwerhealth.com
Structured questionsUpToDate’s process of arriving at
recommendations involves constructing
a structured clinical question. That
structure includes carefully defining
the patient population of interest, the
alternative management strategies, and
the outcomes of importance to patients.
Values and preferencesA fundamental principle of evidence-
based medicine, as described by Dr.
Gordon Guyatt from McMaster University,
is that “Evidence alone is never sufficient
to make a clinical decision. Decision
makers must always trade the benefits
and risks, inconvenience, and costs
associated with alternative management
strategies, and in doing so consider the
patient’s values.”45
This principle has led some evidence-
based resources to avoid making specific
recommendations for patient care, since
the recommendation needs to account
for all of the factors cited. UpToDate
has taken a different approach. It is the
policy of UpToDate to make specific
recommendations for patient care
whenever possible. Recommendations
in UpToDate are based upon a synthesis
of evidence including that from clinical
trials and clinical experience; whenever
possible, the evidentiary basis for
recommendations is stated explicitly.
When there is no published systematic
evidence available (eg, prednisone dosing
regimen in pulmonary sarcoidosis),
recommendations are based upon
the unsystematic clinical observations
of our experts and reviewers, and
on pathophysiologic rationale.
7.
www.wolterskluwerhealth.com
UpToDate recommendations identify situations in which different decisions might be
appropriate for patients with different values and preferences. Furthermore, UpToDate
recognizes that recommendations will not apply to every patient, and counts on
clinicians to evaluate the recommendations in light of the individual circumstances
of their patient. Nevertheless, UpToDate feels that giving clinicians access to
recommendations based on a sophisticated understanding of the clinical issues,
the best evidence, and a consideration of patient values and preferences, allows
them to make informed decisions with and for their patients.
GradingUpToDate began grading recommendations for treatment and screening in 2006.
This is a continuing process and not all such recommendations have yet been graded.
Graded recommendations appear in the Summary and Recommendations sections
at the end of topics.
UpToDate uses the UTD-GRADE format, a modification of the GRADE system.46,47
Grades have two components, a number (1 or 2) reflecting the strength of the
recommendation and a letter (A, B, or C) reflecting the quality of the evidence
supporting that recommendation.
A Grade 1 recommendation is a strong recommendation to do (or not do) something,
where the benefits clearly outweigh the risks (or vice versa) for most, if not all patients.
A Grade 2 recommendation is a weaker recommendation, where the risks and benefits
are more closely balanced or are more uncertain. The majority of recommendations will
be Grade 2 recommendations. UpToDate uses wording that reflects the strength of the
recommendation: strong (Grade 1) recommendations are “recommended” and weak
(Grade 2) recommendations are “suggested.”
Grade A evidence means high-quality evidence that comes from consistent results
from well-performed randomized controlled trials, or overwhelming evidence of some
other sort (such as well-executed observational studies with very strong effects). Grade
B evidence means moderate-quality evidence from randomized trials that suffer from
serious flaws in conduct, inconsistency, indirectness, imprecise estimates, reporting bias,
or some combination of these limitations, or from other study designs with special
strength. Grade C evidence means low-quality evidence from observational evidence,
or from controlled trials with several very serious limitations.
8.
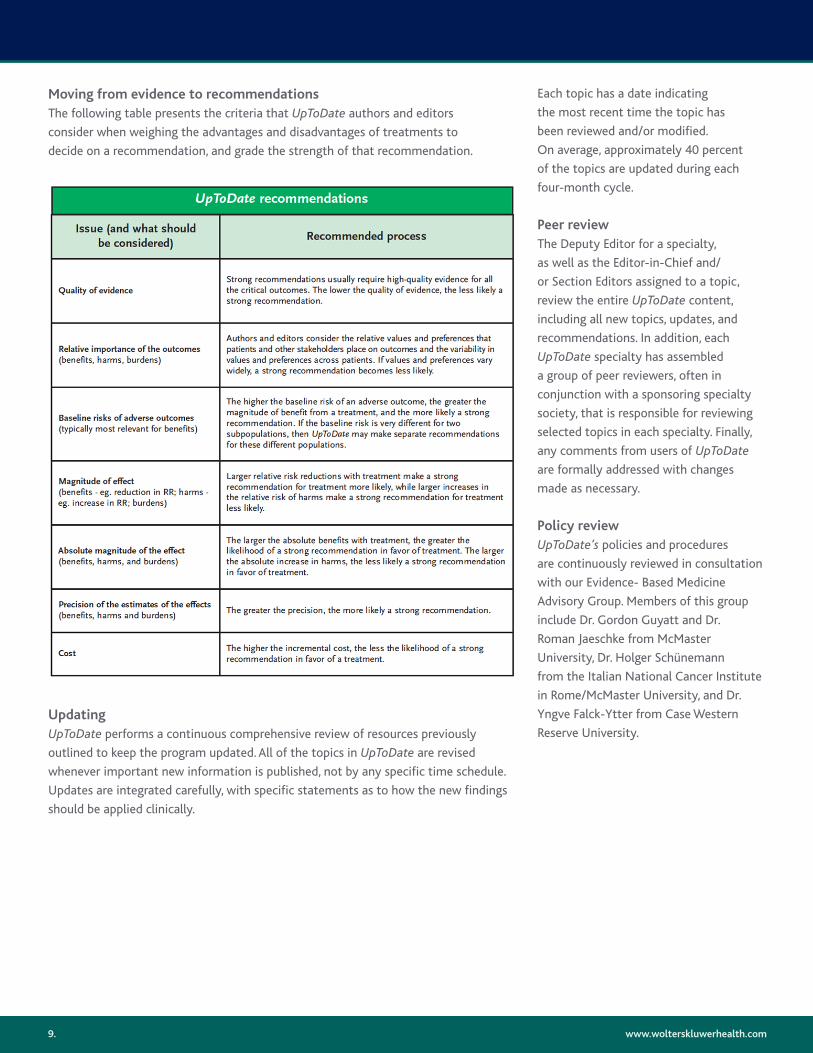
Moving from evidence to recommendationsThe following table presents the criteria that UpToDate authors and editors
consider when weighing the advantages and disadvantages of treatments to
decide on a recommendation, and grade the strength of that recommendation.
UpdatingUpToDate performs a continuous comprehensive review of resources previously
outlined to keep the program updated. All of the topics in UpToDate are revised
whenever important new information is published, not by any specific time schedule.
Updates are integrated carefully, with specific statements as to how the new findings
should be applied clinically.
www.wolterskluwerhealth.com
Each topic has a date indicating
the most recent time the topic has
been reviewed and/or modified.
On average, approximately 40 percent
of the topics are updated during each
four-month cycle.
Peer review The Deputy Editor for a specialty,
as well as the Editor-in-Chief and/
or Section Editors assigned to a topic,
review the entire UpToDate content,
including all new topics, updates, and
recommendations. In addition, each
UpToDate specialty has assembled
a group of peer reviewers, often in
conjunction with a sponsoring specialty
society, that is responsible for reviewing
selected topics in each specialty. Finally,
any comments from users of UpToDate
are formally addressed with changes
made as necessary.
Policy review UpToDate’s policies and procedures
are continuously reviewed in consultation
with our Evidence- Based Medicine
Advisory Group. Members of this group
include Dr. Gordon Guyatt and Dr.
Roman Jaeschke from McMaster
University, Dr. Holger Schünemann
from the Italian National Cancer Institute
in Rome/McMaster University, and Dr.
Yngve Falck-Ytter from Case Western
Reserve University.
9.

www.wolterskluwerhealth.com
The database permits analysis of
hospital-level data for two general
types of complications: 1) “Conditions
of concern” in which there are outcomes
that should not occur and thus represent
substandard care (e.g. air embolism); 2)
“Expected complications” (e.g. venous
thrombosis) that (when occurring in
higher than expected frequencies) may
indicate opportunities for improving
patient safety.
Complication rates can be compared
across hospitals after adjusting for
differences in the severity of illness,
geographic location, hospital size and
teaching status, and community setting
(urban versus rural). Thus, facilities
are compared to other facilities with
similar characteristics. The complications
methodology has been extensively
validated and used in many studies
evaluating patient safety.49-51
Mortality Risk-adjusted mortality is determined
based upon normative comparisons using
patient-level data to control for case mix
and severity of illness.52,53 Thus, patients
are compared to other patients with
similar characteristics and co-morbid
conditions. The risk-adjusted mortality
index has been extensively validated.52,53
Length of stayDetermination of average length of
stay was based upon severity-adjusted
diagnostic related groups (DRGs).54,55
Severity-adjusted DRGs are intended
to distinguish discharges that are
clinically similar and require comparable
resources (e.g. diagnostic, therapeutic,
and nursing services).
Severity of illness is based upon the
patient’s medical condition or evidence
of physiologic decompensation. The
DRG system is used to determine
reimbursement by the Centers for
Medicare and Medicaid Services and
most private insurers.
EligibilityHospitals included in the Solucient
database were required to have a Centers
for Medicare and Medicaid Services (CMS)
Medicare Provider Analysis and Review
(MEDPAR) dataset for 2003 to 2004, CMS
standard analytic files outpatient dataset
for 2002 and 2003, and a CMS cost
report for 2004. Hospitals were excluded
from the Solucient database if a current
Medicare cost report was unavailable,
if they were specialty hospitals (e.g.
children’s, women’s, psychiatric, substance
abuse, rehabilitation, cardiac, orthopedic,
long-term acute care), had fewer than
25 acute care beds, 500 total facility
admissions, or 100 Medicare patient
discharges in fiscal year 2004, or had
Medicare average lengths of stay longer
than 30 days. All UpToDate hospitals
fulfilling these criteria were included
in the analysis.
Weighting strategyHospitals that subscribed to UpToDate
were compared to the Solucient database
on bed size, teaching status, and
geographic region. These are variables
known to be associated with the
primary outcome measures. Two
weighting strategies were used to allow
the model coefficients to be applicable
to a national distribution of acute-care
hospitals. Because all the outcome
variables were based on discharge-
level observations, weighting for
hospital volume was done to account
for differences across hospital
inpatient volume.
Appendix 2: Hospital clinical knowledge systems and health outcomes study methods26
Patient safety indicatorsThe patient safety indicator (PSI)
scores represent a set of measures
on potential complications and adverse
events on hospitalized patients. They
were developed with a comprehensive
literature synthesis, analysis of ICD-9
codes, and review by expert clinicians
and implementation of risk adjustment
and empirical studies.48 The Agency for
Healthcare Research and Quality (AHRQ)
provides free, publicly available tools
necessary to determine PSI scores and
they are a widely used measure of patient
safety. The AHRQ Patient Safety Indicators
are used in at least 9 states for public
reporting on hospital performance. The
rationale is that hospitals that show good
performance on these measures are likely
to be providing good quality of care.
There are 23 AHRQ PSIs that are relevant
for provider-level (hospital-level) analysis.
Seven, which are birth-related, are not
relevant to a Medicare population and
were thus excluded. Five require “Cause
of Injury” or E-codes, which are not coded
consistently across acute-care hospitals in
the United States, and were therefore not
included in the study.
ComplicationsSolucient has constructed a database
containing normative, case-level data
on a national level; it contains more than
21 million annual patient discharge levels.
The case-level data include age, sex, race,
payer, length of stay, clinical grouping
(Diagnosis Related Groups or Refined
Diagnosis Related Groups), comorbid
conditions, and hospital
identification information.
10.
Weighting by hospital class was done to derive model coefficients that would better
reflect the national distribution of hospitals on bed size category, teaching status, and
region. Thus, the analysis was performed without weighting, by weighting for discharge
volume only, and by weighting for discharge volume and hospital class. Hospital class
was categorized as small community (bed size 25-99), medium community (bed size
100-249), or large community (bed size >250). Teaching hospitals were classified as
standard teaching (bed size >250 and resident-to-bed ratio of >0.03 or total residency
programs >3), or major teaching (bed size >400 and residents-to-beds ratio >0.25 and
>10 residency programs, or resident-to-bed ratio >0.60 if fewer residency programs).
Statistical analysisHospital-specific performance on mortality, complications, and patient safety were
represented by a z-score for each measure, while severity-adjusted length of stay
(LOS) was based upon the Yale Refined Diagnosis-Related Group methodology.28,56
Severity-adjusted LOS was represented in the models in units of days. Hospital-level,
risk-adjusted mortality, complications, and PSI were based on two years of data (2003
and 2004) to increase the precision of hospital-level measures through larger sample
sizes; LOS was based on 2004 data only.
The PSI composite measure was created by calculating the average of the normalized
z-scores for 11 individual AHRQ PSI indicators that were appropriate for a Medicare
population aged 65 years and older, and did not depend on E-codes. As noted above,
use of cause of injury codes, or E-codes, varies extensively from hospital to hospital,
thus PSI measures that used E-codes were omitted.
The measure-specific z-scores were calculated by subtracting the expected number
from the observed number and dividing by the standard error.57,58 The mortality,
complications, and PSI z-scores, as well as the severity-adjusted LOS, were used
as outcome variables in the analyses.
Separate linear regression models were developed for each combination of outcome
and weighting strategy. All models included adjustment variables described above
to control for hospital bed size category, teaching status, and geographic region
(i.e. Northeast, Midwest, South, and West).
The primary predictor variables of interest were: 1) the UpToDate status of the hospital
and, 2) in separate models, the average number of topic reviews per week (hits per
week, or HPW). HPW refers to the average number of topic reviews that were viewed
at each institution each week. All comparisons were between UpToDate hospitals versus
all nonUpToDate hospitals in the Solucient database.
www.wolterskluwerhealth.com
Data regarding the average hits per
week were also matched to the
Solucient database to determine
whether associations with the primary
outcomes correlated with the amount
that UpToDate was used at each facility.
Thus, UpToDate status was evaluated
in two ways: 1) as a binary variable
indicating whether a given hospital was
using UpToDate and 2) as a continuous
variable representing HPW. Hospitals that
were not UpToDate users were assigned
a zero HPW. The relationship between
the primary outcome measures and HPW
was presented graphically by converting
changes in z-scores associated with
UpToDate HPW to risk-adjusted rates.
11.
www.wolterskluwerhealth.com
Wolters Kluwer Health | ProVation® Medical800 Washington Avenue NorthSuite 400Minneapolis, MN 55401
ProVationMedical.com888.952.6673612.313.1500
References
1. Alper BS, White DS, Ge B. Physicians answer more clinical questions and change clinical decisions more often with synthesized evidence: a randomized trial in primary care. Ann Fam Med 2005;3(6):507-13.
2. Barrie AR, Ward AM. Questioning behaviour in general practice: a pragmatic study. BMJ 1997;315(7121):1512-5.
3. Bergus GR, Emerson M. Family medicine residents do not ask better-formulated clinical questions as they advance in their training. Fam Med 2005;37(7):486-90.
4. Chambliss ML, Conley J. Answering clinical questions. J Fam Pract 1996;43(2):140-4.
5. Cheng GY. A study of clinical questions posed by hospital clinicians. J Med Libr Assoc 2004;92(4):445-58.
6. Covell DG, Uman GC, Manning PR. Information needs in office practice: are they being met? Ann Intern Med 1985;103(4):596-9.
7. Currie LM, Graham M, Allen M, Bakken S, Patel V, Cimino JJ. Clinical information needs in context: an observational study of clinicians while using a clinical information system. AMIA Annu Symp Proc 2003:190-4.
8. D’Alessandro DM, Kreiter CD, Peterson MW. An evaluation of information-seeking behaviors of general pediatricians. Pediatrics 2004; 113(1 Pt 1):64-9.
9. Del Mar CB, Silagy CA, Glasziou PP, et al. Feasibility of an evidence-based literature search service for general practitioners. Med J Aust 2001;175(3):134-7.
10. DeZee KJ, Durning S, Denton GD. Effect of electronic versus print format and different reading resources on knowledge acquisition in the third-year medicine clerkship. Teach Learn Med 2005;17(4):349-54.
11. Ely JW, Osheroff JA, Chambliss ML, Ebell MH, Rosenbaum ME. Answering physicians’ clinical questions: obstacles and potential solutions. J Am Med Inform Assoc 2005;12(2):217-24.
12. Ely JW, Osheroff JA, Ebell MH, et al. Analysis of questions asked by family doctors regarding patient care. BMJ 1999;319(7206):358-61.
13. Ely JW, Osheroff JA, Ebell MH, et al. Obstacles to answering doctors’ questions about patient care with evidence: qualitative study. BMJ 2002;324(7339):710.
14. Fozi K, Teng CL, Krishnan R, Shajahan Y. A study of clinical questions in primary care. Med J Malaysia 2000;55(4):486-92.
15. Gorman P. Information needs in primary care: a survey of rural and nonrural primary care physicians. Medinfo 2001;10(Pt 1):338-42.
16. Gorman P. Information needs in primary care: a survey of rural and nonrural primary care physicians. Medinfo 2001;10(Pt 1):338-42.
17. Graber MA, Randles BD, Ely JW, Monnahan J. Answering clinical questions in the ED. Am J Emerg Med 2008;26(2):144-7.
18. Green ML, Ciampi MA, Ellis PJ. Residents’ medical information needs in clinic: are they being met? Am J Med 2000;109(3):218-23.
19. Green ML, Ruff TR. Why do residents fail to answer their clinical questions? A qualitative study of barriers to practicing evidence-based medicine. Acad Med 2005;80(2):176-82.
20. Jerome RN, Giuse NB, Gish KW, Sathe NA, Dietrich MS. Information needs of clinical teams: analysis of questions received by the Clinical Informatics Consult Service. Bull Med Libr Assoc 2001;89(2):177-84.
21. Kim GR, Bartlett EL, Jr., Lehmann HP. Information resource preferences by general pediatricians in office settings: a qualitative study. BMC Med Inform Decis Mak 2005;5:34.
22. Koonce TY, Giuse NB, Todd P. Evidence-based databases versus primary medical literature: an in-house investigation on their optimal use. J Med Libr Assoc 2004;92(4):407-11.
23. Leff B, Harper GM. The reading habits of medicine clerks at one medical school: frequency, usefulness, and difficulties. Acad Med 2006;81(5):489-94.
24. Ramos K, Linscheid R, Schafer S. Real-time information-seeking behavior of residency physicians. Fam Med 2003;35(4):257-60.
25. Swinglehurst DA, Pierce M, Fuller JC. A clinical informaticist to support primary care decision making. Qual Health Care 2001;10(4):245-9.
26. Bonis PA, Rind DM, Pickens G, Foster D. Association of a Clinical Knowledge Support System with Improved Patient Safety, Reduced Complications and Shorter Length of Stay among Medicare Beneficiaries in Acute Care Hospitals in the United States. Int J Med Inform 2008:(in press).
27. Dickinson T, Riley J, Zabetakis PM. External validation of compliance to perfusion quality indicators. Perfusion 2004;19(5):295-9
28. Edwards N, Honemann D, Burley D, Navarro M. Refinement of the Medicare diagnosis-related groups to incorporate a measure of severity. Health Care Financ Rev 1994;16(2):45-64.
29. Griffith JR, Alexander JA, Jelinek RC. Measuring comparative hospital performance. J Healthc Manag 2002;47(1):41-57.
30. Griffith JR, Knutzen SR, Alexander JA. Structural versus outcomes measures in hospitals: a comparison of Joint Commission and Medicare outcomes scores in hospitals. Qual Manag Health Care 2002;10(2):29-38.
31. Kirchheimer B. Hospitalists make a mark. Emerging specialty linked to shorter lengths of stay and improved mortality, but not to lower costs, Solucient finds. Mod Healthc 2006;Suppl:8- 10, 2, 4 passim.
32. McDonagh KJ. Hospital governing boards: a study of their effectiveness in relation to organizational performance. J Healthc Manag 2006;51(6):377-89; discussion 90-1.
33. Nallamothu BK, Saint S, Ramsey SD, Hofer TP, Vijan S, Eagle KA. The role of hospital volume in coronary artery bypass grafting: is more always better? J Am Coll Cardiol 2001;38(7):1923-30.
34. Proenca EJ, Rosko MD, Dismuke CE. Service collaboration and hospital cost performance: direct and moderating effects. Med Care 2005;43(12):1250-8.
35. Safavi K. The measurement conundrum. J Healthc Manag 2006;51(5):287-90.
36. Lucas BP, Evans AT, Reilly BM, et al. The impact of evidence on physicians’ inpatient treatment decisions. J Gen Intern Med 2004;19 (5 Pt 1):402-9.
37. McDonald FS, Zeger SL, Kolars JC. Factors Associated with Medical Knowledge Acquisition During Internal Medicine Residency. J Gen Intern Med 2007;22(7):962-78.
38. Resar RK, Rozich JD, Classen D. Methodology and rationale for the measurement of harm with trigger tools. Quality & safety in health care 2003;12 Suppl 2:ii39-45.
12.
www.wolterskluwerhealth.com
Wolters Kluwer Health | ProVation® Medical800 Washington Avenue NorthSuite 400Minneapolis, MN 55401
ProVationMedical.com888.952.6673612.313.1500
39. Thomas EJ, Studdert DM, Newhouse JP, et al. Costs of medical injuries in Utah and Colorado. Inquiry 1999;36(3):255-64.
40. Krohn R. In search of the ROI from CPOE. J Healthc Inf Manag 2003;17(4):6-9.
41. Menachemi N, Brooks RG. Reviewing the benefits and costs of electronic health records and associated patient safety technologies. Journal of medical systems 2006;30 (3):159-68.
42. Adams M, Bates DH, Coffman GA, Everett W. Saving Lives, Saving Money: The imperative for computerized physician order entry in Massachusetts Hospitals. In: Massachusetts Technology Collaborative and the New England Healthcare Institute; 2008.
43. Ash JS, Sittig DF, Poon EG, Guappone K, Campbell E, Dykstra RH. The extent and importance of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc 2007;14(4):415-23.
44. Poon EG, Blumenthal D, Jaggi T, Honour MM, Bates DW, Kaushal R. Overcoming barriers to adopting and implementing computerized physician order entry systems in U.S. hospitals. Health affairs (Project Hope) 2004;23(4): 184-90.
45. McAlister FA, Straus SE, Guyatt GH, Haynes RB. Users’ guides to the medical literature: XX. Integrating research evidence with the care of the individual patient. Evidence-Based Medicine Working Group. JAMA 2000;283(21):2829-36.
46. Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490.
47. Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an american college of chest physicians task force. Chest 2006;129(1):174-81.
48. AHRQ. Quality Indicators--guide to Patient Safety Indicators. version 21, Revision 3 ed: Agency for Healthcare Research and Quality; 2005.
49. Iezzoni LI, Daley J, Heeren T, et al. Identifying complications of care using administrative data. Med Care 1994;32(7):700-15.
50. Iezzoni LI, Davis RB, Palmer RH, et al. Does the Complications Screening Program flag cases with process of care problems? Using explicit criteria to judge processes. Int J Qual Health Care 1999;11(2):107-18.
51. Weingart SN, Iezzoni LI, Davis RB, et al. Use of administrative data to find substandard care: validation of the complications screening program. Med Care 2000;38(8):796-806.
52. DesHarnais S, McMahon LF, Jr., Wroblewski R. Measuring outcomes of hospital care using multiple risk-adjusted indexes. Health Serv Res 1991;26(4):425-45.
53. DesHarnais SI, Chesney JD, Wroblewski RT, Fleming ST, McMahon LF, Jr. The Risk-Adjusted Mortality Index. A new measure of hospital performance. Med Care 1988;26(12):1129-48.
54. Fetter RB. Casemix classification systems. Aust Health Rev 1999;22(2):16-34; discussion 5-8.
55. Freeman JL, Fetter RB, Park H, et al. Diagnosisrelated group refinement with diagnosis- and procedure-specific comorbidities and complications. Med Care 1995;33(8):806-27.
56. MacKenzie T. Patient classification systems: An evaluation of the state of the art. 1991.
57. Iezzoni LI, Ash AS, Shwartz M, Daley J, Hughes JS, Mackiernan YD. Judging hospitals by severity-adjusted mortality rates: the influence of the severity-adjustment method. Am J Public Health 1996;86(10):1379-87.
58. Iezzoni LI, Shwartz M, Ash AS, Hughes JS, Daley J, Mackiernan YD. Using severity-adjusted stroke mortality rates to judge hospitals. Int J Qual Health Care 1995;7(2):81-94.
13.