Anomalous origin of the coronary arteries in children: diagnostic role of three-dimensional coronary...
7
Anomalous origin of the coronary arteries in children: diagnostic role of three-dimensional coronary MR angiography Alberto Clemente a , Mario Del Borrello b , Pietro Greco c , Paolo Mannella a , Franco Di Gregorio d , Silvia Romano e , Aldo Morra b, ⁎ a Department of Radiology, University of Ferrara, Corso Giovecca n°203, 44100 Ferrara (Fe), Italy b Department of Radiology, Euganea Medica Diagnostic Centre, Via Colombo n°13, 35020 Albignasego (Pd), Italy c Department of Cardiology, Euganea Medica Diagnostic Centre, Via Colombo n°13, 35020 Albignasego (Pd), Italy d Medico S.p.A. Clinical Research, Via Pitagora 15, 35030, Rubano (PD), Italy e Department of Cardiology, University of Padua Medical School, Via Giustiniani n°2, 35128 Padova, Italy Received 22 July 2009; accepted 24 August 2009 Abstract When the anomalous origin of coronary arteries (AOCA) is suspected in children (especially athletes), due to signs and symptoms of myocardial ischemia or on the basis of echocardiographic assessment, three-dimensional coronary magnetic resonance angiography (3D- CMRA) can be proposed for the fine morphological evaluation of coronary branches anatomy and course. We tested the diagnostic potential of CMRA angiography in a prospective study on AOCA in young patients. Between July 2005 and June 2008, 15 patients aged 6–29 years (mean age, 13.5 years±5.6 S.D.; median, 14) with clinical and echocardiographic suspicion of AOCA underwent CMRA (1.5 T), 3D whole-heart, free-breathing technique, without the use of contrast medium and β-blockers, with a mean examination time of 30 min. We acquired a second scan of all patients to ameliorate the quality of the acquisition and to improve our experience. AOCA was confirmed by 3D-CMRA in 8 out of 15 cases (53%) and three different anatomical variants were demonstrated, that is, ectopic origin of the left circumflex artery arising from the right coronary artery with retro-aortic course in four cases, single coronary artery arising from the right sinus of Valsalva with interarterial course in one case, ectopic right coronary artery arising from the left sinus of Valsalva with interarterial course in one case; in two patients without anomalies of origin of the coronary arteries, elongated LMCA with angulation of the proximal segment of the left circumflex artery was present. When AOCA is suspected particularly in children (especially athletes), CMRA without the use of contrast medium is an effective diagnostic technique, which is useful to clarify the spatial position of the anomalous course of the main coronary branches in order to suggest the most convenient management of the disease. CMRA does not need contrast medium, needles, and β-blockers; is repeatable in the same examination without the exposure to X-rays; allows a parent to stay near the child; and needs low collaboration in low-stress conditions. © 2010 Elsevier Inc. All rights reserved. Keywords: Coronary MR (CMR); MR angiography (MRA); Anomalous origin of the coronary arteries (AOCA); 3D whole heart; Children 1. Introduction The anomalous origin of the coronary arteries (AOCA) is an anatomical and clinical condition featuring a wide spectrum ranging from totally asymptomatic patients, whose anomaly is accidentally detected by a routine examination, to severe impairment leading to myocardial ischemia, acute myocardial infarction, and possible sudden death. Anomalies can be divided into three general classifica- tions: these include anomalies of origin and course (ectopic ostium within proper sinus, ostium outside normal sinus, and absent vessel), anomalies of intrinsic coronary arterial anatomy (congenital stenosis of ostium, congenital aneur- ysms, and myocardial bridging), and anomalies of coronary termination (fistulas) [1]. Clinical Imaging 34 (2010) 337 – 343 ⁎ Corresponding author. Department of Radiology, Euganea Medica Diagnostic Centre, Via Colombo 13, I-35020 Albignasego [PD], Italy. Tel.: +39 049 804 4836; fax: +39 049 880 1599. E-mail address: [email protected] (A. Morra). 0899-7071/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.clinimag.2009.08.030
-
Upload
alberto-clemente -
Category
Documents
-
view
214 -
download
1
Transcript of Anomalous origin of the coronary arteries in children: diagnostic role of three-dimensional coronary...

Clinical Imaging 34 (2010) 337–343
Anomalous origin of the coronary arteries in children: diagnostic role ofthree-dimensional coronary MR angiography
Alberto Clementea, Mario Del Borrellob, Pietro Grecoc, Paolo Mannellaa, Franco Di Gregoriod,Silvia Romanoe, Aldo Morrab,⁎
aDepartment of Radiology, University of Ferrara, Corso Giovecca n°203, 44100 Ferrara (Fe), ItalybDepartment of Radiology, Euganea Medica Diagnostic Centre, Via Colombo n°13, 35020 Albignasego (Pd), ItalycDepartment of Cardiology, Euganea Medica Diagnostic Centre, Via Colombo n°13, 35020 Albignasego (Pd), Italy
dMedico S.p.A. Clinical Research, Via Pitagora 15, 35030, Rubano (PD), ItalyeDepartment of Cardiology, University of Padua Medical School, Via Giustiniani n°2, 35128 Padova, Italy
Received 22 July 2009; accepted 24 August 2009
Abstract
When the anomalous origin of coronary arteries (AOCA) is suspected in children (especially athletes), due to signs and symptoms ofmyocardial ischemia or on the basis of echocardiographic assessment, three-dimensional coronary magnetic resonance angiography (3D-CMRA) can be proposed for the fine morphological evaluation of coronary branches anatomy and course. We tested the diagnosticpotential of CMRA angiography in a prospective study on AOCA in young patients. Between July 2005 and June 2008, 15 patients aged6–29 years (mean age, 13.5 years±5.6 S.D.; median, 14) with clinical and echocardiographic suspicion of AOCA underwent CMRA (1.5T), 3D whole-heart, free-breathing technique, without the use of contrast medium and β-blockers, with a mean examination time of 30 min.We acquired a second scan of all patients to ameliorate the quality of the acquisition and to improve our experience. AOCA was confirmedby 3D-CMRA in 8 out of 15 cases (53%) and three different anatomical variants were demonstrated, that is, ectopic origin of the leftcircumflex artery arising from the right coronary artery with retro-aortic course in four cases, single coronary artery arising from the rightsinus of Valsalva with interarterial course in one case, ectopic right coronary artery arising from the left sinus of Valsalva with interarterialcourse in one case; in two patients without anomalies of origin of the coronary arteries, elongated LMCA with angulation of the proximalsegment of the left circumflex artery was present. When AOCA is suspected particularly in children (especially athletes), CMRA withoutthe use of contrast medium is an effective diagnostic technique, which is useful to clarify the spatial position of the anomalous course of themain coronary branches in order to suggest the most convenient management of the disease. CMRA does not need contrast medium,needles, and β-blockers; is repeatable in the same examination without the exposure to X-rays; allows a parent to stay near the child; andneeds low collaboration in low-stress conditions.© 2010 Elsevier Inc. All rights reserved.
Keywords: Coronary MR (CMR); MR angiography (MRA); Anomalous origin of the coronary arteries (AOCA); 3D whole heart; Children
1. Introduction
The anomalous origin of the coronary arteries (AOCA) isan anatomical and clinical condition featuring a widespectrum ranging from totally asymptomatic patients, whose
⁎ Corresponding author. Department of Radiology, Euganea MedicaDiagnostic Centre, Via Colombo 13, I-35020 Albignasego [PD], Italy. Tel.:+39 049 804 4836; fax: +39 049 880 1599.
E-mail address: [email protected] (A. Morra).
0899-7071/$ – see front matter © 2010 Elsevier Inc. All rights reserved.doi:10.1016/j.clinimag.2009.08.030
anomaly is accidentally detected by a routine examination, tosevere impairment leading to myocardial ischemia, acutemyocardial infarction, and possible sudden death.
Anomalies can be divided into three general classifica-tions: these include anomalies of origin and course (ectopicostium within proper sinus, ostium outside normal sinus, andabsent vessel), anomalies of intrinsic coronary arterialanatomy (congenital stenosis of ostium, congenital aneur-ysms, and myocardial bridging), and anomalies of coronarytermination (fistulas) [1].

Table 1Classification, characterization of the AOCA, and age of every evaluatedpatient
Class Anomaly of origin Age
Absent No anomalies of origin 9Absent No anomalies of origin 11Absent No anomalies of origin 13Absent No anomalies of origin 14Absent No anomalies of origin 14Absent No anomalies of origin 15Absent No anomalies of origin 21Benign Elongated LMCA with angulated origin of LCx 6Benign Elongated LMCA with angulated origin of LCx 14Benign LCx from RCA and retro-aortic course 9Benign LCx from RCA and retro-aortic course 12Benign LCx from RCA and retro-aortic course 14Benign LCx from RCA and retro-aortic course 29Malignant (severe) Single coronary artery, LMCA with
interarterial course and myocardial bridging7
Malignant (severe) RCA from LSV with interarterial course 15
LSV, left sinus of Valsalva.
338 A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
The anomalies with the highest risk of developing majorcardiac events include coronary anomalous origin withinterarterial course of the proximal segment, anomalousorigin from the pulmonary artery, and the coronaryarterovenous fistula [2,3]. Other anomalies, such as
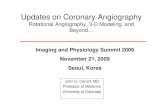
Fig. 1. Some examples of 3D-CMRA MIP, MPR, and VR images showing the a
anomalous origin from the wrong sinus or singular coronaryartery without interarterial course, are generally benign,although not completely free of cardiac risk [4–6].
Nowadays, a number of imaging techniques are availablefor AOCA diagnosis. Coronary angiography (CA) is aninvasive test frequently applied, whereas recent noninvasivetechniques that proved useful are magnetic resonance (MR)imaging [7–12] and multidetector computed tomography[13–23].
In this prospective study, we tested the efficacy of three-dimensional coronary magnetic resonance angiography (3D-CMRA) in the identification of AOCA in young athletes whohad clinical and echocardiographic suspicion of AOCA; dueto the young age of the patients, we preferred the MRapproach instead of multidetector computed tomography.
2. Materials and methods
2.1. Patients
Between July 2005 and May 2009, 15 patients aged 6–29 years (mean age, 13.5 years±5.6 S.D.; median, 14), withclinical and echocardiographic suspicion of AOCA, wereselected for a prospective study with coronary MR
nomalous origin of LCx from the RCA with retro-aortic course (arrows).

339A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
angiography (1.5 T, Philips Achieva). The data sets wereanalyzed by two expert cardioradiologists (MDB and AM),by one resident radiologist (AC) with 3 years of experience incardioradiology, and by one cardiologist experienced intomographic cardiac imaging (PG).
2.2. Technical aspects
2.2.1. Patient preparationNo special preparation was required.
2.2.2. Scan protocolAll subjects were studied in supine position. MR scans
were performed using a dedicated cardiac five-elementphased-array coil (1.5 T, Philips Achieva) and 3D whole-heart free-breathing technique, with no need of contrastmedium. Respiratory artefact suppression was achieved by adiaphragmatic navigator. The electrocardiogram (ECG) wasrecorded throughout the procedure.
2.2.3. Three-dimensional coronary MR angiographyAfter the scout and preparatory examinations were
performed, CMRA was obtained with the “whole hearttechnique” using a navigator gated and corrected (NAV) free-
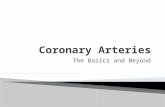
Fig. 2. 3D-CMRAMPR, MIP, and VR examples showing the anomalous single codistal origin of the LCx (arrows).
breathing 3D steady-state free precession sequence coveringthe heart volume (TR/TE 4.3/2.1 ms, 90° flip angle, 2 mmthickness, SENSE factor=2, 160 slices, 0.75 mm recon-structed slice thickness, in-plane resolution=0.99×0.99 mm).Mean scanning time was 7 min (N50% NAV efficiency) andmean examination time 30 min. A double acquisition wasperformed in all patients to optimize the acquisition qualityand to improve our specific experience.
2.2.4. Post-processingThe image data sets were analyzed and processed on a
separate workstation (TeraRecon Aquarius 3.6.2.3) toobtain 2D–3D images with volume rendering (VR),maximum intensity projection (MIP), and multiplanarreformatting (MPR) techniques for the evaluation of thecoronary anomalies.
3. Results
MR evaluation confirmed the AOCA suspicion in 6 cases;the normal coronary origin in 9 patients was clearly shown,of whom two were affected by angulation of origin of the leftcircumflex artery (LCx). As summarized in Table 1, the
ronary artery rising from the RSV with interarterial course of the LMCA and

Fig. 3. 3D-CMRA axial and MPR MIP images showing the anomalousorigin of the RCA from the left sinus of Valsalva, with an interarterial coursebetween the AO and the pulmonary artery (arrows).
340 A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
ectopic origin of the left circumflex artery (LCx) arising fromthe right coronary artery (RCA) with retro-aortic course wasthe most frequent anomaly (four cases) (Fig. 1) and classifiedas benign. In addition, the analysis revealed one case ofsingle coronary artery arising from the right sinus ofValsalva (RSV) with interarterial course and myocardialbridging of the left main coronary artery (LMCA) with distalorigin of the LCx (Fig. 2) and one case of ectopic leftcoronary artery arising from the RSV with interarterialcourse (Fig. 3), both classified as malignant. Besides, in twopatients (symptomatic) without anomalies of origin of thecoronary arteries, elongated LMCA with angulation of theproximal segment of the LCx was shown (Fig. 4). For thesereasons, we classified them as benign variants.
4. Discussion
Coronary artery anomalies (CAA) are rare and may existas isolate abnormalities in a leftover healthy heart, orassociated with congenital heart diseases. In the first case,they are the outcome of an isolate embryological error,which involves the connection of subepicardiac plexus with
the aortic wall. In the second case, they are part of a widercongenital heart anomaly, involving either the ventricularwall or the partition of the cardiac bulb. CAA prevalence isabout 1% in the general populations [4,24–28], andincreased to 2.2% in an autopsy population of congenitalheart disease [5]. CAA may cause myocardial ischemia withdifferent clinical manifestations as sudden death, fatal ornonfatal acute myocardial infarction, syncope, dyspnea,palpitations, and chest pain [4,27]. However, in the vastmajority of cases, they do not result in clinical symptomsand are detected only by chance during angiographicprocedures or autopsy [29]. The likelihood of ischemicevents in case of CAA is higher in young athletes, where thecongenital coronary anomalies are among the first causes ofsudden death during physical effort, often without premon-itory symptoms [30–32]. Moreover, CAA are the secondcause of sudden death in children affected by hypertrophiccardiomyopathy [33]. Since sudden death or myocardialinfarction are among the possible first clinical manifesta-tions of the presence of congenital anomalies of thecoronary arteries [4,27], early diagnosis is of paramountimportance for patients at risk, as children. A retrospectiveanalysis [34] of young patients who suddenly died duringphysical activity showed that the majority of them have hadsymptoms before the fatal event, but the diagnosis wasmissed. In the last years, more attention has been paid toexclude the presence of CAA during the preparticipationscreening, which is mandatory in our country [35,36].Patients younger than 30 years, without any risk factors ofatherosclerosis, who suffer from chest pain and who presentwith electrocardiographic modification during effort orrepetitive ventricular arrhythmias with apparently normalheart, have to be suspected of congenital coronaryanomalies. The difficulty in identifying the origin of thecoronary arteries by echocardiography might well be due tocongenital coronary artery anomaly and therefore usuallydeserves deeper investigation. In order to obtain a correctrisk stratification and to decide the most convenientmanagement of the disease (medical treatment or surgicalor percutaneous intervention), an accurate identification ofthe abnormality is fundamental. For a long time, theconventional CA has been used in identifying origin,course, and morphology of the coronary arteries, but it isan invasive test and it requires hospitalization. Transeso-phageal echocardiography [37] can be useful, but it is aninvasive technique too. Anyway, as an alternative, simpler,and noninvasive imaging technique, the transthoracic two-dimensional echocardiography [38] can be applied. Theseallow visualizing the coronary ostia and identifying theabnormalities in the coronary origin. Nevertheless, noconclusive study exists, to the best of our knowledge, onthe accuracy and reliability of echocardiography in suchexaminations. In the last few years, other noninvasiveimaging techniques such as computed tomography CA(CTCA) [12,13,16–19] and coronary MR [7–10] haveproved to provide the best and most complete information

Fig. 4. Examples of 3D-CMRA coronal and oblique MPR and VR images showing no anomalies of origin of the coronary arteries but angulation of the proximalsegment of the LCx (arrows).
341A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
for a correct diagnosis of coronary abnormalities. TheCTCA offers the best performance in terms of spatialresolution and acquisition time, but is not indicated inchildren because of the high X-ray exposure [39]. CTCAallows an accurate three-dimensional reconstruction of thewhole coronary artery course, with particular regard to theproximal segments, which are most frequently affected.Moreover, at variance with CA, it allows to simultaneouslyshow the whole coronary tree and to identify the coronaryostia, which are sometimes difficult to selectively cannulateduring CA, due to their ectopic origin; to distinguish amongintraarterial, retro-aortic, intraseptal and prepulmonarycourse of the anomalous coronary artery, thanks to thethree-dimensional reconstruction and the visualization of allthe cardiac chambers and the major vessels; to simulta-neously visualize, in case of coronary artery fistula, both thecoronary artery from which the fistula originates, oftenshowing a tortuous course and an ectasic caliber, the fistula,and even the surrounding structures. The main drawbacks ofthe CTCA technique in young patients are the radiationexposure and the utilization of iodinated contrast agents thatare potentially allergenic and nephrotoxic. Originally, MRalso needed the use of a contrast dye and featured somedisadvantages in cardiac examinations, such as the lengthy
acquisition time, the insufficient spatial resolution for anaccurate reconstruction of the coronary arteries and, inaddition, it is not compatible with the presence of metallicimplants such as hearing aids, neurostimulators, and pace-makers (but all of these are relative disadvantages inchildren). Nowadays, technical inconveniences have beenovercome by the use of dedicated cardiac coils, ECG, anddiaphragm recorder and 3D fast sequences. Because of thenew possibilities offered by 3D-CMRA to investigateAOCA without the use of contrast medium applied onyoung patients, we had excellent results in our experienceand nowadays we can strongly say that 3D-CMRA has anew role in the identification of the anomalies of coronaryarteries being able to clarify their origin as well as CTCA.
In comparison, CMRA acquisition is free-breath whileCTCA is breath-hold and it does not provide a low cardiacrate to reduce cardiac artifacts (limitation of CTCA). Thepossibility of studying coronary vessels without theincannulation of a peripheral vein to inject contrast mediumcauses less stress especially in children. In addition, CMRAis to repeat the examination in the same day in case ofartifacts for the absence of ionized radiations (otherimportant limitation of CTCA). All these advantages weresuccessfully overcome as evidenced in our study and 3D-

342 A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
CMRA permitted us to identify the coronaries of all of the 15young patients, with normal, benign, and malignant variants.
5. Conclusion
Coronary MR angiography is an state-of-the-art, accuratetechnique to clarify the spatial position of the anomalousorigin and course of the main coronary branches and todecide the most convenient management, particularly inchildren and young athletes. MR scans are free-breathing;quickly acquired; do not need the use of contrast medium,needles, and β-blockers; can easily be repeated withoutexposure to X-rays; require low collaboration; and aregenerally less stressing than other imaging procedures. In thespecific case of children, a parent can safely stay by thepatient during the examination. In conclusion, on the basis ofour experience, we consider coronary MR angiography asfirst-choice imaging technique when AOCA is suspectedin children.
References
[1] Angelini P, Velasco JA, Flamm S. Coronary anomalies. Incidence,patophysiology and clinical relevance. Circulation 2002;105:2449–54.
[2] Cebi N, Schulze-Waltrup N, Frömke J, Scheffold T, Heuer H.Congenital coronary artery fistulas in adults: concomitant pathologiesand treatment. Int J Cardiovasc Imaging 2008;24(4):349–55.
[3] Earls JP. Coronary artery anomalies. Tech Vasc Interv Radiol 2006;9(4):210–7.
[4] Wilkins CE, Betancourt B, Mathur VS, Massumi A, De Castro CM,Garcia E, Hall RJ. Coronary artery anomalies. A review of more than10,000 patients from the Clayton Cardiovascular Laboratories. TexHeart Inst J 1988;15:166–73.
[5] Frescura C, Basso C, Thiene G, et al. Anomalous origin of coronaryarteries and risk of sudden death: a study based on an autopsypopulation of congenital heart disease. Hum Pathol 1998;29:689–95.
[6] Angelini P. Coronary artery anomalies—current clinical issues.Definitions, classification, incidence, clinical relevance and treatmentguidelines. Tex Heart Inst J 2002;29:271–8.
[7] Post JC, van Rossum AC, Hofman MB, Valk J, Visser CA. Three-dimensional respiratory-gated MR angiography of coronary arteries:comparison with conventional coronary angiography. AJR Am JRoentgenol 1996;166(6):1399–404.
[8] McConnell MV, Ganz P, Selwyn AP, Li W, Edelman RR, ManningW.Identification of anomalous coronary arteries and their anatomic courseby magnetic resonance coronary angiography. Circulation 1995;92(11):3158–62.
[9] Bunce NH, Lorenz CH, Keegan J, Reyes EM, Firmin DN, Pennel DJ.Coronary artery anomalies: assessment with free-breathing three-dimensional coronary MR angiography. Radiology 2003;227:201–8.
[10] Casolo G, Del Meglio J, Rega L, et al. Detection and assessment ofcoronary artery anomalies by three-dimensional magnetic resonancecoronary angiography. Int J Cardiol 2005;103(3):317–22.
[11] Varghese A, Keegan J, Pennel DJ. Cardiovascular magnetic resonanceof anomalous coronary arteries. Coron Artery Dis 2005;16(6):355–64.
[12] Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E,Langerak SE, Weber OM, Pedersen EM, Schmidt M, Botnar RM,Manning WJ. Coronary magnetic resonance angiography for thedetection of coronary stenoses. N Engl J Med 2001;345(26):1863–9.
[13] Van Ooijen PMA, Dorgelo J, Zijlstra F, Oudkerk M. Detection,visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol 2004;14:2163–71.
[14] Shi H, Aschoff AJ, Brambs HJ, Hoffmann MHK. Multislice CTimaging of anomalous coronary arteries. Eur Radiol 2004;14(2172):2181.
[15] Ropers D, Moshage W, Daniel WG, Jessl J, Gottwik M, Achenbach S.Visualization of coronary artery anomalies and their anatomic courseby contrast-enhanced electron-beam coronary angiography. Am JCardiol 2001;87(2):193–7.
[16] Memisoglu E, Hobikoglu G, Tepe MS, Norgaz T, Bilsel T. Congenitalcoronary anomalies in adults: comparison of anatomic coursevisualization by catheter angiography and electron beam CT. CatheterCardiovasc Interv 2005;66(1):34–42.
[17] Deibler AR, Kuzo RS, Vohringer M, et al. Imaging of congenitalcoronary anomalies with multislice computed tomography. Mayo ClinProc 2004;79(8):1017–23.
[18] Schmitt R, Froehner S, Brunn J, et al. Congenital anomalies of thecoronary arteries: imaging with contrast enhanced, multidetectorcomputer tomography. Eur Radiol 2005;15:1110–21.
[19] Sato Y, Inoue F, Matsumoto N, Tani S, et al. Detection of anomalousorigin of the coronary artery by means of multislice computedtomography. Circ J 2005;69:320–4.
[20] Datta J, White CS, Gilkeson RC, et al. Anomalous coronary arteries inadults: depiction at multi-detector row CT angiography. Radiology2005;235(3):812–8.
[21] Hou K-Y, Jeng C-M, Liu Y-P, Wang T-H, Lin T-M, Chen S-W, ChenC-J, Mo Y-H. Diagnosis of anomalous coronary arteries in 64-MDCT.Chin J Radiol 2007;32:111–9.
[22] Cademartiri F, Runza G, Luccichenti G, Galia M, Mollet NR, AlaimoV, Brambilla V, Gualerzi M, Coruzzi P, Midiri M, Lagalla R. Coronaryartery anomalies: incidence, pathophysiology, clinical relevance androle of diagnostic imaging. Radiol Med (Torino) 2006;111(3):376–91Epub 2006 Apr 11. Review. English, Italian.
[23] Romano S, Morra A, Del Borrello M, Greco P, Daliento L. Multi-slicecomputed tomography and the detection of anomalies of coronaryarteries. J Cardiovasc Med (Hagerstown) 2008 Feb;9(2):187–94.
[24] Engel HJ, Torres C, Page HL. Major variations in anatomical origin ofthe coronary arteries: angiographic observations in 4.250 patientswithout associated congenital heart disease. Catheter Cardiovasc Diagn1975;1:157–69.
[25] Yamanaka O, Hobbs RE. Coronary artery anomalies in 126.595patients undergoing coronary arteriography. Catheter CardiovascDiagn 1990;21:28–40.
[26] Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenitalanomalies of the coronary arteries: a coronary arteriographic study. IntJ Cardiol 2000;74:39–46.
[27] Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence,pathophysiology and clinical relevance. Circulation 2002;105:2449–54.
[28] Cademartiri F, La Grutta L, Malagò R, Alberghina F, Meijboom WB,Pugliese F, Maffei E, Palumbo AA, Aldrovandi A, Fusaro M,Brambilla V, Coruzzi P, Midiri M, Mollet NRA, Krestin GP.Prevalence of anatomical variants and coronary anomalies in 543consecutive patients studied with 64-slice CT coronary angiography.Eur Radiol 2008;18:781–91.
[29] Lipsett J, Cohle SD, Berry PJ, Russell G, Byard RW. Anomalouscoronary arteries: a multicenter pediatric autopsy study. Pediatr Pathol1994;14(2):287–300.
[30] Basso C, Corrado D, Thiene G. Congenital coronary artery anomaliesas an important cause of sudden death in young. Cardiol Rev 2001;9(6):312–7.
[31] Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile ofcongenital coronary artery anomalies with origin from the wrong aorticsinus leading to sudden death in young competitive athletes. J Am CollCardiol 2000;35(6):1493–501.
[32] Maron BJ, Epstein SE, Roberts WC. Sudden death in youngcompetitive athletes. J Am Coll Cardiol 2000;35:1493–501.
[33] Corrado D, Pelliccia A, Bjornstad HH, et al. Cardiovascular pre-participation screening of young competitive athletes for prevention of

343A. Clemente et al. / Clinical Imaging 34 (2010) 337–343
sudden death: proposal for a common European protocol. Eur Heart J2005;26:516–24.
[34] Wisten A, Messner T. Symptoms preceding sudden cardiac death in theyoung are common but often misinterpreted. Scand Cardiovasc J 2005;39(3):143–9.
[35] Corrado D, Basso C, Schiavon M, Tthiene G. Pre-participationscreening of young competitive athletes for prevention of suddencardiac death. J Am Coll Cardiol 2008;52:1981–9.
[36] Thompson PD. Preparticipation screening of competitive athletes. Seekingsimple solutions to a complex problem. Circulation 2009;119:1072–4.
[37] Giannoccaro PJ, Sochowski RA, Morton BC, Chan KL. Complemen-tary role of transoesophageal echocardiography to coronary angiog-raphy in the assessment of coronary artery anomalies. Br Heart J 1993;70(1):70–4.
[38] Davis J, Jones TK, Portman MA. Major coronary artery anomalies in apediatric population: incidence and clinical importance. J Am CollCardiol 2001;37:593–7.
[39] Einstein AJ, Henzlova MJ, Rajagopalan S. Estimating risk of cancerassociated with radiation exposure from 64-slice computed tomogra-phy coronary angiography. JAMA 2007;298(3):317–23.