![Summary of Financial Statements for the Fiscal Year Ended ... · SymBio Pharmaceuticals Limited (4582) Summary of Financial Statements [Japanese GAAP] (Non-consolidated) Results for](https://static.fdocuments.in/doc/165x107/5f072b5d7e708231d41ba6e1/summary-of-financial-statements-for-the-fiscal-year-ended-symbio-pharmaceuticals.jpg)
Annual Report and Summary Financial Statements
136
County Durham and Darlington NHS Foundation Trust Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Transcript of Annual Report and Summary Financial Statements
County Durham and DarlingtonNHS Foundation Trust
Annual Report and SummaryFinancial Statements
1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 1

County Durham and Darlington NHS Foundation Trust
Annual Report and Summary Financial Statements1 April 2010 – 31 March 2011
Presented to Parliament pursuant toSchedule 7, Paragraph 25(4) of theNational Health Service Act 2006
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 2

Contents Page
Chairman’s and Chief Executive’s Statement 04
About the Trust 08
Highlights of the Year 09
Directors’ Report and Business Review 14Operating and Financial ReviewRegulatory Ratings
Quality Accounts 23Independent Auditor’s Report to the Governing Council of County Durham and Darlington NHS Foundation Trust
Service Developments 68
Research and Development 73
Our People and Community Involvement 76WorkforceEquality and DiversityStaff SurveySocial Responsibility and SustainabilityHealth and Safety PerformanceFormal ConsultationsPartners and Stakeholders
Board of Directors 92Audit CommitteeRemuneration The NHS Foundation Trust Code of Governance
Governing Council 98
Membership 102
Statement of the Chief Executive’s responsibilities 104as the Accounting Officer of the Trust
Statement on Internal Control 105
Summary Financial Statements for the year ended 31 March 2010 115Independent Auditor’s Report on the Summary Financial Statements to the Governing Council of County Durham and Darlington NHS Foundation Trust
Glossary of Terms 131
How to find out more 133
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 3
04
Chairman’s and Chief Executive’s Statement
Welcome to the Trust’s Annual Report for2010/2011, reviewing our fourth full yearas a foundation trust.
2010/11 was a successful year for the Trust,during which we responded well to thedemands of meeting the healthcare needs ofour communities in a challenging economicenvironment.
At a strategic level, the year’s main featurewas the “Transforming Community Services”project to integrate acute and communityservices, whilst, operationally, deliveringquality services to patients and maintaining ahigh standard of performance and financialdelivery.
The Trust's vision as a foundation trust hasbeen to “deliver excellent care in hospital,home and community" and “to maintain anddevelop our position as the premier providerof healthcare in County Durham andDarlington”.
The Trust took a significant step towards fullrealisation of this vision when it completedthe legal acquisition of County Durham andDarlington Community Health Services(Community Health Services) from NHSCounty Durham and Darlington in May 2011.
The context for this was the requirement forour commissioning PCT, NHS County Durhamand Darlington, to become a “commissioningonly” organisation, and divest itself ofprovider responsibilities, in line with theDepartment of Health “TransformingCommunity Services” guidance.
The Trust submitted a strategic outline caseto NHS County Durham and Darlington inMay 2010 and was named “preferredmanagement partner” for communityservices. Since then, a combined Trust andcommunity services team, led by ChiefOperating Officer Sue Jacques, has workedon a detailed and robust due diligenceprocess. This led to the signing of a businesstransfer agreement in time for the start ofthe financial year and an assessment byMonitor in May 2011.
The Trust believes that bringing acute andcommunity services together will benefitpatients, staff and the organisation by:
• Improving outcomes for patients –by ensuring high quality care at the mostappropriate time and place;
• Offering a better patient experience –by improving care pathways and reducinghand offs between organisations;
• Creating organisational developmentand workforce opportunities –including new roles working across a widerrange of settings, and providing long termstability and direction for communityservices; and
• Improving our efficiency –by streamlining services and reducingoverhead costs, such as “back office”functions.
The new integrated acute and communityprovider begins its first year on a strongfooting.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 4

05Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Both the Trust and Community HealthServices performed strongly on key indicatorslast year, including healthcare acquiredinfection rates, urgent and emergency careservices and achieving many of the goalsunder performance related quality measures(CQUIN).
This performance was achieved against thebackdrop of a long and difficult winter,during which services were often undersignificant pressure, with many staff workingabove and beyond the call of duty.
Both organisations also delivered againstfinancial obligations - the Trust reporting a£5.9 million surplus for reinvestment, whileCommunity Health Services were transferredto the Trust with an underlying surplus of£1.8 million.
This was not achieved easily. The Trustdelivered almost £9 million of savingsthrough the “Towards 2014” programme toimprove efficiency and reduce costs. Savingsincluded £0.5 million identified by staffthrough the “Quality Challenge” campaign.
The work carried out during2010/11 means that the newintegrated acute and communityCounty Durham and DarlingtonNHS Foundation Trust hasbegun its first year ofoperations further ahead ofmany other newly integratedorganisations in the North Eastand across the country.
We are also well advanced with work on our first integrated clinical strategy. TheGovernors, Directors and staff see thecreation of the new integrated provider as an opportunity to:
“shift the centre of gravity from hospital to community and develop fully integrated care pathways”.
During the year we have developed plans totake this forward in six areas:
Long term conditions;
Care of older people;
Women and children;
Acute medicine and emergency care;
Surgery; and
End of life care.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 5

06
Chairman’s and Chief Executive’s Statement (continued)
Our aim is to develop a national profile as apathfinder for new ways of offering healthservices in hospital, home and community,reducing unnecessary hospital admissions byproviding a range of alternative servicescloser to home.
The Trust also agreed to hosttwo important regional healthimprovement bodies – FRESHand Balance – which focus onreducing the impact of tobaccoand alcohol harm. These are inaddition to the local healthimprovement portfolio, acquiredas part of community services,which we believe can createvalue added opportunities toreduce local health inequalities.
The Trust Board has realigned executiveportfolios and senior corporate servicesstructures to support the new extendedclinical portfolio and the successfulintegration of services.
This includes the appointment of Tom Hunt,a former PCT and community servicesDirector on the patch for ten years, asExecutive Director of Commercial Servicesand Chris Lisle as Director of HumanResources and Organisational Development.
The revised corporate services structure andintegration of “back office” functions hasensured a single system of internal control andfacilitated a synergy saving of £2.7 million.
The Trust has also strengthened thecommunity focus amongst the Non-ExecutiveDirectors. The Governing Council hasappointed to the Trust Board BaronessArmstrong of Hilltop, former CabinetMinister and MP for North West Durham andAndrew Young, former Chief Executive ofDurham and Chester-le-Street PCT andDurham Dales PCT.
Tony Wolfe and Paul Stewartstepped down as Non-ExecutiveDirectors during 2010/11, andwe would like to take thisopportunity, on behalf of theDirectors and Governors, tothank them both for theircontribution to the Board and tothe organisation more widely.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 6

07
We would like to thank all of our Governorsincluding those who have stepped down thisyear, in supporting and challenging the Trustacross the range of our activities. We wouldalso like to welcome newly electedrepresentatives to the Governing Council.
Finally we would like to put formally onrecord our appreciation of the efforts madeby staff this year for their hard work,
resilience and dedication. We are confidentyou will display these same virtues in facingthe challenges of the exacting and excitingyear ahead.
Tony Waites Stephen EamesChairman Chief Executive
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Prime Minister and Earl Howe visit County Durham & Darlington NHS Foundation Trust
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 7

08
During 2010/11, County Durham and Darlington NHS Foundation Trustprovided acute hospital services for apopulation of around 500,000 peopleliving in County Durham, Darlington andNorth Yorkshire and some specialist subregional services for a wider populationof around 1.2 million people in theNorth East.
The Trust was authorised by Monitor, theindependent regulator, on 1 February 2007to operate as an NHS foundation trust. As a foundation trust, the Trust enjoysgreater autonomy from central control andlocal people are able to have a greater say in the way we run and deliver our services.
The Trust provides acute hospital servicesfrom two sites, the University Hospital of
North Durham (UHND) and DarlingtonMemorial Hospital. Bishop Auckland Hospitalprovides a range of planned services forpatients across County Durham andDarlington, as well as more local services.
During the year, the Trust also providedcommunity hospital services from ShotleyBridge and Chester-le-Street communityhospitals as well as a range of outpatient,community and outreach services from other sites.
From 1 April 2011, community healthservices, previously provided by NHS CountyDurham and Darlington, have become partof the Trust. This has increased our staff from 6,000 to around 8,500 and ourturnover from £340 to £460 million.
About the Trust
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Bishop Auckland Hospital Darlington Memorial Hospital
University Hospital of North Durham Chester-le-Street Community Hospital Shotley Bridge Community Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 8

09
Great North Children’s HospitalThe Trust strengthened links with the GreatNorth Children’s Hospital, part of Newcastleupon Tyne Hospitals NHS Foundation Trust, tobuild on opportunities for joint working todeliver high quality care for children andyoung adults across the North East.Consultants from the Great North Children’sHospital hold specialist clinics at DarlingtonMemorial Hospital and UHND and consultantsfrom Durham and Darlington are workingpart time at the Great North Children’sHospital to develop their special interests.
National Accreditation for GUM ServiceThe Genito-Urinary Medicine Department inBishop Auckland Hospital was the first in theregion to achieve 'You're Welcome'accreditation. This accreditation is awarded bythe Department of Health to highlightservices which are “young people friendly”.Services undertake the initiative with a viewto eliminating barriers to services for youngpeople.
Dementia CollaborativeStaff on Ward 51 at Darlington MemorialHospital have been at the forefront of locallyand nationally recognised improvements indementia care. Working with the DementiaCollaborative, in alignment with the NationalDementia Strategy, they have madesignificant improvements in the quality ofservice they offer to patients with dementiaand have genuinely modernised the service
they are able to offer to patients with thiscondition. These include introducing newsignage and colours, introducing thedischarge team at the beginning of apathway and basing the mental health teamon the ward providing quicker and moredirect access to mental health support. Withthe support of the ‘Friends of the Hospital’ atDurham, Bishop Auckland and Darlington wehave also introduced new specialist crockeryto improve mealtimes for those patients withdementia. The Collaborative is a joint ventureworking with NHS County Durham, Tees Eskand Wear Valleys NHS Foundation Trust andthe local authority.
£5.5 Million Investment in ITU at Darlington Memorial Hospital A new Intensive Therapy Unit opened inJanuary 2011 at Darlington MemorialHospital following a £5.5m investment.
Highlights of the Year - A Year of Good News
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
For the fourth consecutive year, the Trust is named as one of the CHKS 40 Top Hospitals
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 9

10 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The new unit has created additional capacityfor intensive care patients and is built andequipped to the latest standards, offeringpatients, visitors and staff first class facilitiesand accommodation.
£26 Million Investment inDarlington Memorial HospitalThe Trust demonstrated its long termcommitment to the Darlington site with a £26million investment in the hospital’sinfrastructure. This includes a new greenerenergy centre and new engineering services.Work continues on this process and therenewal of Darlington Memorial Hospital willcontinue to require further investment overthe coming years.
Investment in CT ScannersPatients at each of our main sites, BishopAuckland Hospital, Darlington MemorialHospital and UHND, are benefitting from
investment in the latest diagnostictechnology. We now provide access to a 64slice CT scanner at each of these sites.
Improvements to EmergencyDepartment at UHNDThe Emergency Department at UHND hasbeen remodelled to create new facilitieswhich have increased capacity and improvedpatient experience. The new facilities includea six bedded acute monitoring bay and a twobedded dedicated resuscitation area.
Quality ChallengeDuring 2010/11, hundreds of staff gotinvolved in the Trust’s ‘Quality Challenge’.Through the launch of a dedicated websiteand local discussions, staff were encouragedto come up with ideas which could improvequality and efficiency in their areas ofpractice. Staff across the organisationcontributed some excellent and innovativeideas including standardising stock cupboardsand ordering systems, introducing an “a lacarte” menu at Darlington Memorial Hospitaland developing a ‘Good HousekeepingGuide’ for staff to follow when managingmedical records. All of the initiatives aremaking a real difference to patient care acrossthe Trust and have also contributed to over£500,000 in efficiency savings.
Staff Shine at Annual AwardsStaff were recognised for their dedication andachievements when they attended the Trust’sAnnual Awards ceremony in November 2010.Nine awards were presented on the night
The Special Care Baby Unit at Darlington Memorial Hospital receives adonation from local business Clipper Logistics
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 10

11Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
which showcased the quality of care andtreatment being delivered by staff. Individualawards were presented to staff nurse BarbaraDent and to Carole King who works in daysurgery. Barbara is a fitness instructor in herspare time and has set up a weekly class on avoluntary basis for more than 30 patientswith chronic obstructive pulmonary disease.Carole was awarded the ‘Making You FeelBetter Award’ after being nominated by apatient who said “Carole is warm hearted,patient with the nicest smile and attitude inher approach to care and treatment”. ThePatient Experience team also picked up anaward for their work with local partners onthe ‘Hospital Passport’ and producing easyread versions of patient information. TheHospital Passport provides hospital staff withimportant information about patients withlearning disabilities to help provide a moreindividual approach to their care.
Leading on Research and Development Dr Anjan Dhar, one of the Trust’s ConsultantGastroenterologists, was selected as one ofonly twenty five applicants nationally toreceive The British Society ofGastroenterology Endoscopy Fellowship lastyear. Dr Dhar travelled to Japan to learn moreabout advances in the endoscopic treatmentof cancer after being awarded the prestigiousnational fellowship. Dr Dhar is also leadingfive hospitals across the region in a clinicalresearch study to pioneer a new technique for treating the narrowing of the oesophagus (gullet).
Dr Jerry Murphy, a Consultant Cardiologistwith the Trust, was appointed Professor ofCardiovascular Medicine in DurhamUniversity’s School of Medicine and Healthwhich is based at its Queen’s Campus inStockton. He is leading a number of researchprojects to investigate cardiovascularconditions and how these can be diagnosedand managed better whilst also continuinghis clinical duties with the Trust.
Dr Julie Cox, a Consultant Radiologist, isleading a pioneering research trial whichcould change the way breast cancer isdetected and treated across the country. Thestudy will investigate whether multi-detectorCT scanning can be used to accurately assesswhether breast cancer has spread from thebreast to the lymph nodes (cells) in the axilla(arm pit). If so, this would mean that morepatients are able to get the best surgicaltreatment for their condition the first time,reducing the distress and complications thatmay result from additional surgery.
Surgeons at the Trust are pioneering a lifechanging technique for people suffering frombowel incontinence. Approximately 3% ofthe population suffer from bowelincontinence and as the leading centre in theregion for delivering the sacral nervestimulation treatment, the Trust is significantlyimproving the quality of life for thesepatients.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 11

12 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Patient Donations Over the past year, the Trust has beenprivileged to receive a number of donationsboth from patients and their friends andfamilies and local businesses. The Trust isextremely grateful for these valuabledonations and extends a warm thank you toall those who throughout the past year haveshown their support in this manner. Just afew of these have included:
• Danny McAuley and his family andfriends. Danny spent three months in thecritical care department at DarlingtonMemorial Hospital after contractingMeningococcal septicaemia. Danny’s mum,Edie, led the fundraising and altogetherraised nearly £15,000 for a newHaemofiltration machine.
• Mr William Frankland kindly donated sixelectric fans to Ward 13 at UHND as atoken of his support after having to spendsome time in the hospital for treatment.
• Clipper Logistics Group Limited, basedat Faverdale in Darlington, made agenerous donation to the Special CareBaby Unit at Darlington Memorial Hospital.
Leadership AcademyThe NHS North East Leadership Academy was established in April 2010 followingconsultation between the North East StrategicHealth Authority and NHS organisations inthe region. Bids were invited for an
organisation to host the Academy and theTrust was successful with Stephen Eamestaking the Chair.
The core purpose of the Academy is tocontinuously develop leaders and managersto maximise NHS capability and capacity witha view to improving services to patients andto the communities of the North East.
The Academy Aims:
• To improve support for Boards and forpeople already in senior roles;
• To establish a strong pool of local talentand systematically develop people with thehighest potential to excel;
• To develop clinicians in leadership roles toachieve more clinicians as senior leaders;
• To enable a more diverse leadershipcommunity;
• To attract more people into leadership rolesfrom outside the NHS;
• To continue the development of currentleadership programme initiatives and toevaluate their impact;
• To act as a 'think tank' and to facilitatedebate on 'hot' topics;
• To showcase our expertise to raise ourprofile nationally and internationally;
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 12

13Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• To develop strategic alliances with otherinstitutions to transfer learning and leadingedge practice; and
• To act on behalf of the membership andfocus on adding value, supportinginnovation and practical support.
The North East Leadership Academy hasmade remarkable progress in its inauguralyear making it perfectly placed to play a full
part in supporting the drive to accelerateleadership development across the NorthEast. This will ensure that we continue tohave the right leaders, in the right place, andat the right time to continuously improve thequality of services as experienced by ourpatients and their communities.
Closer links with the Great North Children's Hospital (GNCH), part of Newcastle upon Tyne Hospitals NHS FoundationTrust, are building on opportunities for joint working to deliver high quality care for children and young adults
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 13

14
Operating and Financial Review2010/11 was yet another successful year for the Trust with operationalperformance continuing to improve andfinancial performance remaining solid.Alongside this, many staff have beenworking hard in preparation for theintegration of community services from 1 April 2011 to ensure that we can levereven greater gain.
Operational PerformancePerformance as assessed by our regulator,Monitor, has been strong, as hasperformance against our own and ourcommissioners’ clinical priorities. A review ofthese clinical priorities can be found in thesection ‘Quality of Services’.
We are once more proud of theimprovement in our performance againsttargets for health care associated infection.MRSA fell by 57% from 7 to 3 and thenumber of Clostridium difficile cases from95 to 70, a reduction of over 26%. Weachieved the requisite screening targets forMRSA and introduced a screening policy forboth elective and non-elective patients.
We exceeded all of our targets in respect ofcancer:
• 99.7% of all cancers needing surgerywere treated within 31 days;
• 99.7% of all cancers needing anti cancerdrugs were treated within 31 days;
• 89% of all cancers were first treatedwithin 2 months (62 days) following anurgent GP referral;
• 97.8% of all cancers were first treatedwithin 2 months (62 days) following ascreening referral;
• 99.2% of all cancer urgent GP referral(first treatments) were diagnosed within31 days;
• 98.6% of all cancer urgent GP referralwere seen within 14 days; and
• 98.7% of all cancer urgent referrals forbreast symptoms were seen within 14days.
Some 98.32% of patients waited fewerthan four hours to be dealt with in ourAccident and Emergency departmentsagainst the revised target of 95%. This is
Directors’ Report and Business Review
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Tony Waites, Chairman of County Durham and Darlington NHS Foundation Trust
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 14
15
despite an increase of almost 7% in thenumber of people attending thedepartments.
We have worked hard to comply withAccess to Healthcare for patients withLearning Disabilities and declared fullcompliance in March.
Over 94% of admitted patients and some98.5% of non-admitted patients weretreated within 18 weeks of referral.
We secured level 2 for all essentialInformation Governance Toolkit standardsdemonstrating our commitment and resolveto taking good care of the sensitiveinformation that we hold.
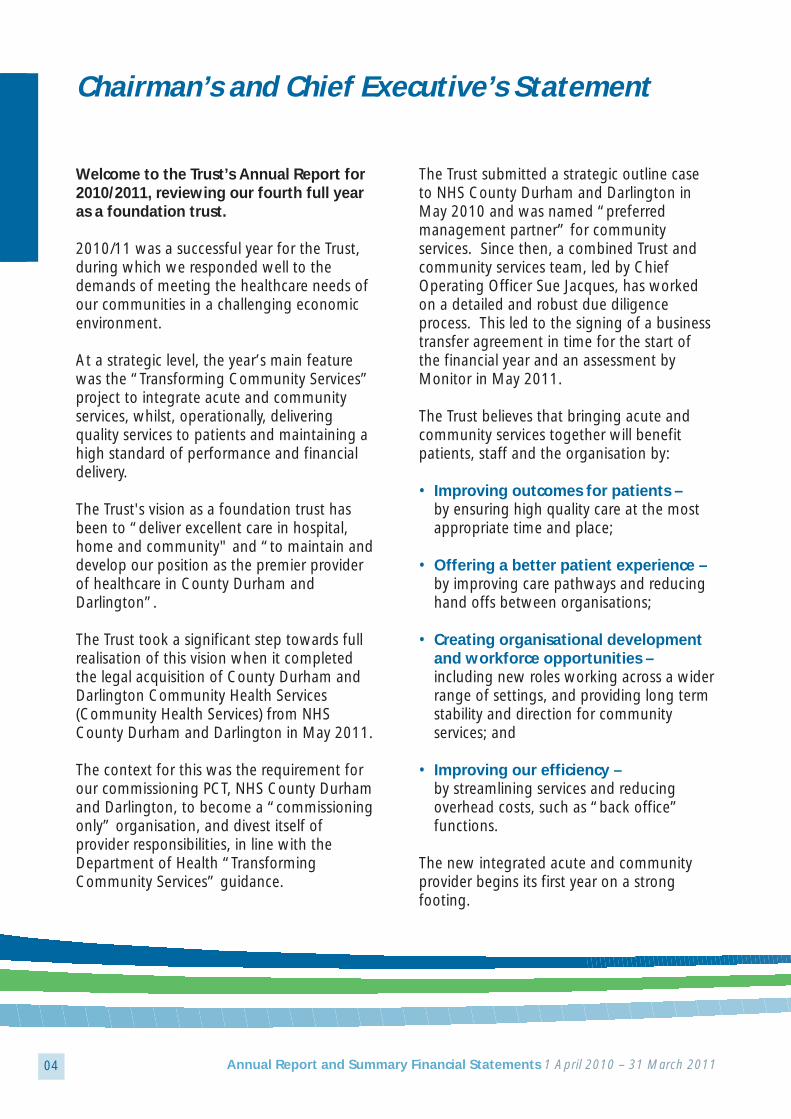
What Our Regulator SaysMonitor, the independent regulator offoundation trusts, requires each foundationtrust to submit an Annual Plan and at leastquarterly performance reports during the
year. Monitor assigns each foundation trustwith an annual and quarterly risk ratingwhich reflect the level of compliance withthese plans and the Trust’s terms ofauthorisation.
At the end of 2010/11, Monitor rated theTrust green/amber for governance and gaveus a financial risk rating of 3. Both of theseare in line with our plans and, as you willnote from the tables below, our governancerating throughout 2010/11 was better thanthat in 2009/10. This stemmed largely fromthe improvements that we made toeliminate infections. The amber/green ratingin the last quarter of the year (2010/11)reflects some minor improvements that weagreed to implement following a visit by theCare Quality Commission – these have allnow been implemented.
Further details of the way in which Monitorrates foundation trust can be found onMonitor’s web site. (www.monitor-nhsft.gov.uk)
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Q4 2009/10
Q2 2009/10
Annual Plan 2009/10
Q1 2009/10
Q3 2009/10
4
GREEN
Financial Risk rating
Governance Risk rating
4
AMBER
3
RED
4
RED
4
AMBER
Q4 2010/11
Q2 2010/11
Annual Plan 2010/11
Q1 2010/11
Q3 2010/11
3
AMBER GREEN
Financial Risk rating
Governance Risk rating
3
GREEN
3
GREEN
3
GREEN
3
AMBER GREEN
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 15

16
Performance Risks2011/12 is a year that, while full ofopportunity, inevitably brings risk. Largescale change, such as our integration withcommunity services, commonly fails to fullydeliver the benefit intended. We are acutelyaware of this and have put a suite ofmeasures in place to ensure that this is notthe case, ranging from revised leadershiparrangements to investment in staff tosupport the organisation deliver the servicetransformation we desire.
Changes to the way that the NHS isorganised and operated, both nationally andlocally, have been proposed; competition isincreasingly more likely and the amount weare paid for the work that we do is set toreduce. Inevitably this will require a stepchange in our efficiency and productivity.Whilst this will not be easy, we have astrong track record and a dedicatedworkforce who have identified opportunitiesto increase efficiency, whilst improvingclinical outcomes and patient experienceand eliminating duplication. Our plans for2011/12 are well developed but it isimportant that we make good progressduring the year to refine plans for 2012/13as part of our new clinical strategy, which itwill be critical to mobilise our workforcebehind.
We have performed strongly during 2010/11,but have nonetheless identified a few areasthat we wish to focus on moving forward, inaddition to those priorities in our QualityAccount and CQUIN targets. These are:
• that we consistently deliver the existingand newly introduced Accident &Emergency targets across all sites; and
• that we continue to deliver the minimumwaiting times for breast patients acrossour catchment area.
Financial PerformanceOverall financial performance for the yearhas been excellent, with our year endsurplus of £5.9m significantly above thatplanned. (It is important that we generatesurpluses so that we can use the additionalcash associated with them to support ourcapital programme which is summarisedlater.) Such performance is a credit to thehard work of everyone in the Trust and isparticularly noteworthy given the significantimprovements in non-financial performancethat have also been made.
Almost £3.9m of the surplus arises from arevaluation of our estate (which wasdevalued by just over £19m last year) and,as such, is an accounting entry to which nocash is attributed, and a provision of£1.68m for estimated one-off restructuringarising from our integration withCommunity Services is included as cost.
Although the Trust delivered a good overallfinancial position, it struggled to implementall of the cost improvement plans that it hadoutlined. This was in part due to asignificant increase in the emergencyworkload that we experienced for which wewere compensated, in part, throughadditional income from our commissioners.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 16

17
Plans for 2011/12 are much betterdeveloped through the financial duediligence work that was undertaken, as arequisite step in our plans to integrate withCommunity Services. We have alsostrengthened our performance managementarrangements and expect to be able todeliver much greater efficiency in 2011/12through the integration of services. It will beimportant that during the course of thatyear we begin to refine plans for 2012/13.
In 2010/11, we invested almost £25m ofcapital in our estate, IT systems and medicalequipment - an increase from the £19minvested in the previous year. Theseinvestments included new CT scanners, newand upgraded Intensive Therapy Unit/HighDependency Unit and Accident &Emergency facilities and a major upgrade ofthe estate infrastructure at DarlingtonMemorial Hospital. These investments werein line with our seven year capital strategyand resulted in the planned reinstatement ofour working capital facility of £22m, asagreed in our terms of authorisation withMonitor.
Almost £7m of additional revenueinvestments were approved during thecourse of the year, including a £3mexpansion of our orthopaedic services and£1.7m in contraception and sexual healthafter securing a contract to provide theseservices.
In summary, 2010/11 has provided a soundfinancial base from which to move forwardas an integrated organisation. Turnover in2011/12 will increase by over a third, tosome £468m as a result of our integrationwith Community Services. Accordingly, wehave strengthened our governancearrangements to allow us to manage themuch larger entity well.
Key Financial Performance TargetsThe Trust exceeded its key financial targetsfor the year to 31 March 2011. The targetsand our performance against them are asfollows:
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
EBITDA margin
Definition: The Net Earnings beforeInterest, Taxation andDividends shown as apercentage of total income.
Purpose: This measures theunderlying financialperformance of the Trust.
Source of data: Trust audited annualfinancial statements.
Plan Target: 8.4 %
Result: 6.3 %
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 17

18 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Income and Expenditure Surplus Margin
Definition: Net Surplus (excludingexceptional items andimpairments) shown as apercentage of total income.
Purpose: To ensure that the Trust istrading profitably.
Source of data: Trust audited annualfinancial statements.
Plan Target: 0.0 %
Result: 0.7 %
Liquid Ratio
Definition: Cash plus Trade Debtorsplus Unused WorkingCapital Facility minus (Trade Creditors plus OtherCreditors) expressed as thenumber of days’ operatingexpenses that this sumwould cover.
Purpose: To ensure that the Trustmaintains sufficient cash to run its business.
Source of Data: Trust audited annualfinancial statements.
Plan Target: 20 days
Result: 38 days
Darlington Memorial Hospital introduces an a la carte menu for patients
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 18
19Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
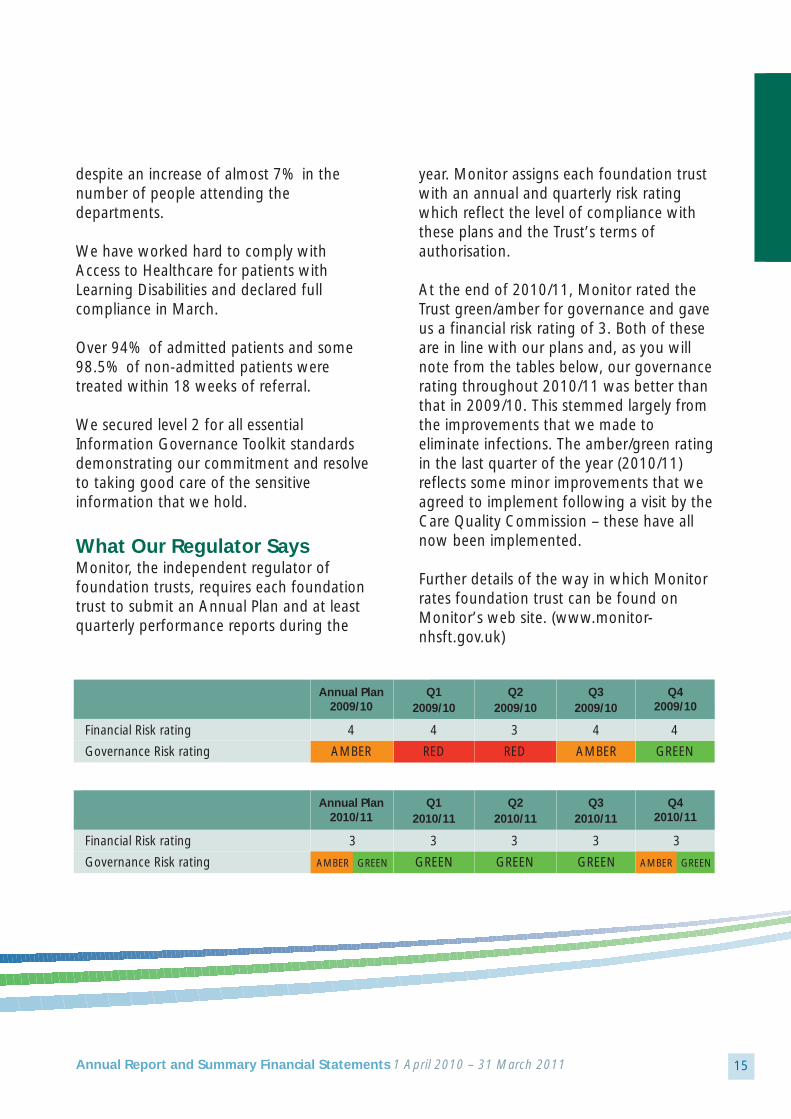
Prudential Borrowing Limit
Definition: A limit to the amount ofborrowings (including PFIschemes) that the Trustmay undertake set for eachNHS foundation trust bythe independent regulatorguided by the PrudentialBorrowing code.
Purpose: Used to protect the publicinterest and financialstability of individual NHSfoundation trusts.
Source of Data: Trust audited annualfinancial statements.
Plan Target: Borrowings less than£129.3m
Result: Borrowings were £124.5m
Private Patient Cap
Definition: The level of Private Patientincome is capped at thelevel (as a percentage oftotal patient income) as atthat in financial year2002/03.
Purpose: To ensure the Trust limitsthe amount of non-NHSwork it undertakes.
Source of Data: Trust audited annualfinancial statements.
Plan Target: < 0.23 %
Result: 0.03 %
Bishop Auckland’s GUM services receive the ‘You’re Welcome’ accreditation
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 19

20 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Trust achieved this target for non-NHSinvoices. However, although it achieved thetarget for NHS invoices by number, itnarrowly failed by value. The relatively lownumbers of invoices mean that a single largevalue invoice paid late can have a materialimpact on the results.
A detailed breakdown of the figures isshown in table 01 below:
Public Sector Payment Policy
Definition: Unless other terms areagreed, the Trust is requiredto pay its creditors within30 days of the receipt ofgoods, or a valid invoice,whichever is the later.
Purpose: To ensure that the Trustcomplies with the BetterPayment Practice Code.
Source of Data: Trust audited financialstatements.
Non-NHS NHS
Target: 95% Target: 95%
Result by number: 97% Result by number: 89%
Result by value: 95% Result by value: 91%
Total bills paid in the year to 31 March 2011
Total bills paid within target
Percentage of bills paid within target
£000
134,385
128,053
95.1%
Number
83,614
80,778
96.6%
Number
2,682
2,377
88.6%
NHS Creditors Non NHS Creditors
£000
36,465
33,071
90.7%
Table 01: Prompt Payment Code (30 Days)
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 20
21Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Late Payment InterestLegislation is in force which requires truststo pay interest to small companies, ifpayment is not made within thirty days (LatePayment of Commercial Debts (Interest) Act1998). The Trust was not required to makeany such payment during the year.
During 2008, the Government requestedthat all Public Bodies review their paymentpractices with a view to making paymentswithin ten days. The Trust has prioritisedpayments for small and medium localcompanies with a view to achieving the tenday payment policy where possible and theresults for all suppliers are shown in table 02 below:
Non NHS Trade Creditors
Total bills paid in the year to 31 March 2011
Total bills paid within target
Percentage of bills paid within target
£000
129,217
80,981
62.7%
Number
78,781
71,206
90.4%
Table 02: Prompt Payment Code (10 Days)
The Trust’s medical education team
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 21

22 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Members of the Governing Council – March 2011
Statement of Compliance withCost Allocation and ChargingRequirementsThe Trust has complied with the costallocation and charging requirements setout in HM Treasury and Office of PublicSector Information Guidance.
Post Balance Sheet EventOn 25 May 2011, the Trust received afinancial risk rating of 3 with anamber/green risk assessment for its intendedintegration with Community Health Services.The Trust Board considered this rating anddetermined to sign a contract for theprovision of community services for an initialperiod of two years and ten monthscommencing 1 June 2011. (A two monthcontract for such provision had previouslybeen signed on 31 March 2011, effectivefrom 1 April 2011).
Going ConcernAfter making enquiries, the Directors have areasonable expectation that the Trust hasadequate resources to continue inoperational existence for the foreseeablefuture. For this reason, they continue toadopt the going concern basis in preparingthe accounts.
Directors’ DeclarationSo far as the Directors are aware, there is norelevant audit information of which theauditors are unaware and the Directors havetaken all steps that they ought to asdirectors in order to make themselves awareof any relevant information and to establishthat the Trust’s auditor is aware of thatinformation.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 22
23Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Quality AccountThis Quality Account is produced by County Durham and DarlingtonFoundation Trust as it enters a new phase of its development as a provider of health care. From 1 April 2011, theTrust becomes a provider of both acuteand community care following theacquisition of County Durham andDarlington Community Health Services.The ambition of the Board is to be thepremier provider of healthcare in CountyDurham and Darlington and to providethe best quality care to the populationthat we serve.
The purpose of this Quality Account is:
• To improve our organisation’saccountability to the public and to engagethe Trust Board in the quality improvementagenda;
• To enable us to review our services andshow where we are doing well and whereimprovement is required;
• To enable us to demonstrate plannedimprovements;
• To provide information on the quality ofservices we provide to patients and thepublic; and
• To demonstrate how we involve andrespond to feedback from patients, thepublic, governors and other stakeholders.
Vision‘To shift the centre of gravity fromhospital to community and develop fully integrated care pathways’.
• The Board has articulated its vision to bethe premier provider of health care inCounty Durham and Darlington including:
- Prevention and enablement,- Community services, and- Planned and emergency hospital care;
• Be a major provider of women andchildren’s services in the North East;
• Have a reputation for excellent specialistservices; and
• Have a national profile as a pathfinder fornew ways of offering health services inhospital, home and community.
Clinical Strategy – Our Aims • The best health outcomes for patients; • An excellent patient experience; and • High quality, low cost services for our
commissioners
County Durham and Darlington NHSFoundation Trust’s commitment to ourpatients and community is at the heart of our values:
• Quality • Care • Respect • Leadership • Achievement
Quality Accounts
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 23
24 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
QualityWhether by setting ourselves challengingtargets, or simply bettering our best in smallways, we are committed to continuallyimproving standards and ensuring everypenny spent provides maximum benefit toour patients and community.
Care Our patients and community are at the centreof our every thought and every action. Eitherthrough direct contact or by supporting ourcolleagues, we do everything we can, asquickly as we can, to make life better andeasier for our patients.
RespectEveryone who comes into contact with theTrust and community is treated with the samehigh level of respect and dignity. We areproud of our Trust and are loyal andsupportive of its goals, progress andachievements.
LeadershipWe take decisions and act. People followthrough on commitments and take personalownership of their actions. Everyone has acritical role in our future and is aware of thepart they have to play.
Achievement We value and encourage success andachievement. Those who improve the patientexperience and our performance are
rewarded; whilst those who create problemsfor their colleagues or patients are dealt withpromptly.
The Trust Board is accountable for the qualityof care provided by the staff of theorganisation and has a number ofmechanisms in place to ensure that weprovide high quality care and to ensure thatwhere standards are falling, or there is acause for concern, immediate action is takento improve standards.
The Board has a patient safety and qualityreport at each of its meetings. The Board alsohas two sub-committees dealing with qualityissues. These are the Quality and InnovationCommittee and the Healthcare GovernanceCommittee. The Board receives a summary ofall complaints made against the Trust and allserious untoward incidents are reported tothe Board at each meeting. The Governorsalso have a Quality and HealthcareGovernance Committee, where Trust officersreport to the Governors regarding the qualityof care provided. The primary commissionerof the Trust’s services, NHS County Durhamand Darlington, agreed a range of QualityIndicators which have been monitoredthroughout the year (CQUIN targets). TheBoard has also scrutinised the reportspublished during the year where lessonscould be learned from failures in care andproduced improvement plans to ensure thatservices continue to improve.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 24

25Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Sir John Oldham visited Darlington Memorial Hospital in recognitionof the Trust’s work on improving care for patients with dementia
Each division has a quality structure andprocesses in place to ensure that they providehigh quality care. The divisions are held toaccount by the Board through theperformance monitoring processes. Serviceline management is the preferred mechanismfor the divisions to manage their business.Incorporated into the process are the qualityperformance measures designed to make thedivisions the preferred provider of health carethrough application of quality improvementtechniques.
The Trust uses CHKS as a mechanism tobenchmark services and understand thequality of our services relative to other Trusts.
NHS QUEST is a new venture for the Trust.Eleven high performing Trusts nationally aremembers of NHS QUEST. The purpose is toensure that the Trusts work together to drivequality performance above that of theexpected. We have also joined localorganisations in the process of benchmarkingthrough TURBO Benchmarking. Six localorganisations are working together tobenchmark quality and cost. Thesemechanisms are used to ensure that we areamongst the best performing organisations inthe NHS and demonstrate our unfailing driveto improve the quality of care we provide forpatients.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 25

26
This Quality Account has been produced inconsultation with Darlington Borough Counciland Durham County Council Overview andScrutiny Committees (OSCs), the GoverningCouncil’s Quality and Healthcare GovernanceCommittee, the local LINks organisations, the Board of Directors and staff of theorganisation. Local GP commissioners aresignificantly concerned about the quality ofdischarge communication and this is,therefore, included as a priority for action. Anumber of complaints have highlighted issuesabout patient movement around the hospitalsand this is also included as a priority. Thenumber of patients falling in the care of ourhospitals gives cause for concern and a wholestream of work is focussed on reducing suchfalls. The ward managers have raised theirconcern about discharge medication and thisis supported by discussions with OSCs and
LINks. During the year the Trust was alertedto higher than average mortality rates in twospecific conditions through the Dr. FosterGood Hospital Guide. This alert was takenvery seriously and close scrutiny and auditrevealed that the documentation of cause ofdeath and the Trust’s model of stroke caremay have been responsible for this apparentconcern. Mortality is, therefore, included as apriority in order to enable close monitoringand ensure safe and effective care.
The priorities listed in the Quality Accountshave their origins from a variety of sources.They are complemented by the CQUINtargets. Their selection is in response to thequality monitoring undertaken through theyear and represent areas for improvement.They are not our only quality monitoringcriteria but are the focus of this documentfollowing consultation.
We are confident that we provide high qualitycare to our patients with high levels ofsatisfaction and good clinical outcomes. Wecontinue to make quality our priority with thefollowing goals as part of our patient safetyand quality improvement strategy.
Quality GoalsThe three domains of quality are wellrehearsed and documented in suchdocuments as:
• Darzi – Next Stage Review • Quality Outcomes Framework
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Bishop Auckland Hospital staff take part in International Nurses Day
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 26

27
High quality care is only achieved when allthree work in harmony. Delivery of only oneor two will not deliver the level of quality thatthe patient requires.
Safety1. To eliminate avoidable harm; 2. To prevent people from dying prematurely
when healthcare interventions could help;3. To treat and care for people in a safe
environment;4. To reduce risk through delivery of
evidence based care; 5. To ensure policies and procedures are
followed by all staff of the organisation;and
6. To develop a culture of accountability,continuous improvement and fairness.
Experience1. To ensure patients have a positive
experience of care;2. To respond to concerns and complaints to
ensure improvement is evident;3. To implement systems that deliver care in
the right place at the right time for thepatient’s needs;
4. To ensure patients who are at the end oflife have the opportunity to receive thecare they require in the environment oftheir choice; and
5. To enable patients to be involved in theircare planning and make informed choices.
Effectiveness1. To comply with national guidance and
best practice; 2. To audit compliance and ensure that
practice is evidence based;3. Continually improve and transform
services to deliver quality and safety;4. To participate in national audits of care
and put in place improvement plans toenable the Trust to be amongst the bestperforming; and
5. To use available evidence to informpractice.
Statement from the Chief ExecutiveAs the responsible officer for County Durhamand Darlington NHS Foundation Trust, Iconfirm that the information contained inthese accounts is a true and fair reflection ofthe quality of care provided by the Trust.
Stephen EamesChief Executive
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 27

28
PrioritiesPriorities for improvement are divided into thethree components of quality
• Safety• Experience• Effectiveness
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Priority Rationale for choice Measure
SAFETY
Patient Falls National QIPP priority Reduction in falls per patientHigh levels of falls reported bed dayin the hospitals Reduction in fallsNPSA monitoring falls resulting in injuryresulting in fracture
Safeguarding Training Identified in serious case Numbers of staff trained inreview and compliance accordance with the trainingassessment of the standards strategy
Discharge Communication Concerns of OSC and Reduction in complaints andGP consortia incidents regarding dischargePoor quality of discharge Higher levels of patientinformation identified satisfactionthrough auditPatient complaints regarding lack of information
HCAI Maintenance of current Achieve reduction in lineimprovement with targetBoard and national priority
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 28

29Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Priority Rationale for choice Measure
EXPERIENCE
Nutrition and Hydration Features in complaints %Completion of in Hospital National attention nutritional assessment
High level of support by OSCs %Completed food charts%Completed fluid balancecharts
Complaints about the Feature of complaints Reduction in complaintsAttitude of Staff related to staff attitude
Boarding of Patients on CQC assessment critical Cessation of boarding patientsother Wards of boarding policy outside of normal working
Board debate and concern hoursIR1s completed and monitored for breaches of the policy
Priority Rationale for choice Measure
EFFECTIVENESS
Mortality of Specific Performance in Dr. Foster Maintain mortality at orConditions Review. Strategic objective below SMR of 100
to reduce avoidable injury or death
Compliance with NICE Essential compliance for Audit evidence ofRecommendations registration compliance
Medications Management Concerns of OSC. Audit Audit of omitted medication.evidence from pharmacy Audit of discharge medicationdetails high level of error
Compliance with Sentinel National priority. Local priority Audit of stroke pathway andAudit Standards for Stroke following stroke discussion monthly returns
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 29

30 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Community PrioritiesPrior to merging with the Trust, CommunityServices identified their priorities. These aresimilar to the priorities of the acute hospitalsand are:
1. Reducing falls in community hospitals; 2. Reduction in the numbers of pressure
sores; and 3. Focus on under-nutrition of patients in
community hospitals.
Details can be found within County Durhamand Darlington Community Health ServicesQuality Account.
The reporting against these priorities will bewithin the Trust’s performance report.
Identification of PrioritiesThe table above details the rationale for thechoice of the improvement. Stakeholdersconsidered the long list of issues and thepriorities were agreed.
The long list of issues identified from ourperformance monitoring during the yearwere:
• Safeguarding children and adults;• Mortality – specific conditions;• ‘A good death’- place of death;• Falls in hospital and the community;• Catheterisation and UTI;• Breast feeding rates;• Smoking;• Alcohol related illness;• Managing demand in winter;• Discharge letters;• Venous Thromboembolism prevention;• Complaints;• Car parking;• Stroke; and• Nutrition and hydration in hospital.
Improvement plans for the priorities will bemonitored through the Trust’s Quality andHealthcare Governance Committee withprogress reported to the Board, theGovernors and the local OSCs at intervalsthroughout the year.
Nationally Requested Content The aim of this section is to ensure that thepublic have consistent information from all
Supporting National Diabetes Day with a community roadshow
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 30

31Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
providers. The content is set out in the revisedregulations for the Quality Accounts and canbe found in the Quality Accounts Toolkit.
Review of ServicesDuring 2010/11, County Durham andDarlington NHS Foundation Trust providesNHS services. The County Durham andDarlington NHS Foundation Trust hasreviewed all of the data available to them onthe quality of care in all of these services. The income generated by the NHS Servicesreviewed in 2010/11 represents 88.2% of thetotal income generated from the provision ofNHS Services by the County Durham andDarlington NHS Foundation Trust for2010/11. Assurance frameworks are available for theQuality and Innovation Committee and theHealthcare Governance Committee. These aremonitored through internal audit. A numberof audits have been undertaken during theyear to provide assurance regarding thequality of data and processes used by theTrust.
The Ward Performance FrameworkThe Ward Performance Framework wasdeveloped in 2006 as a tool to assist Matronsin undertaking an objective assessment of thequality of care provision within eachward/department.
Matrons undertake an assessment everymonth on each of their ward/departmentalareas. This assessment includes a care audit
whereby five sets of current in-patient nursingrecords are reviewed. Secondly, five currentin-patients are interviewed in relation to theircurrent experience using semi-structuredinterviews. The third component is a reviewof a range of quality indicators e.g. numberof complaints, drug administration errors andso on.
Following this assessment, the Matron is ableto give immediate feedback to the WardManager regarding their findings and agreeappropriate action plans developed for anyareas identified as needing improvement.
Depending on the results, each indicator isRAG (Red, Amber, Green) rated whichprovides a visual picture of the performance.The results from all ward areas areaggregated into one spreadsheet and thisprovides an overview of how the Trust isdoing against all of the indicators. Thisoverview enables identification of where theTrust may have issues across several wardswhich might require corporate action to betaken.
The Ward Performance Framework results arediscussed at the Quality and InnovationCommittee on a monthly basis and form partof the Trust’s Assurance Framework.
Quality Monitoring VisitsEvery month senior managers and cliniciansvisit all the wards and departments in theTrust to review the quality of the care and the
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 31

32
environment. The visits provide anopportunity for discussion and scrutiny andenhance ward to Board communication. Theresults are reported to the weekly qualitymeeting.
Participation in Clinical AuditsDuring 2010/11, forty one national clinicalaudits and five national confidential enquiriescovered NHS services that County Durhamand Darlington NHS Foundation Trustprovides.
During that period, County Durham andDarlington NHS Foundation Trust participatedin 100% of the national confidential enquiriesand 89% of the national clinical audits andnational confidential enquiries which it waseligible to participate in.
The national clinical audits and nationalconfidential enquiries that County Durhamand Darlington NHS Foundation Trust wasboth eligible and did participate in, for whichdata collection was completed during2010/11, are contained within the tables onpages 58 to 62. Each audit or enquiryparticipation is presented as a percentage ofthe number of registered cases required bythe terms of that audit or enquiry.
The reports of sixteen national clinical auditswere reviewed by the provider in 2010/11and County Durham and Darlington NHSFoundation Trust intends to take thefollowing actions to improve the quality ofhealthcare provided:
• Improvements in communication to GPs,via the electronic discharge letters for theirpatients with community acquiredpneumonia;
• Action to improve the waiting times forantibiotics being undertaken by MedicalAssessment Unit and Antibiotic Group;
• Clinical forms adapted to include annualscreening for paediatric diabetic patients asrecommended by NICE, and thyroidfunction tests adapted to allow for capillarysampling from the same patient cohort;
• Clinician documentation improved withinneonatal unit regarding consultation withparents/carers;
• Review processes to increase the level ofgeriatrician support to increase theproportion of patients who have a pre-operative geriatric assessment;
• Review of allocated operating time toincrease the percentage of patientsoperated within 36 hours of fractured neckof femur; and
• Purchase of ultrasound to provide bedsidethoracic ultrasound for pleural procedures.
Confidential Enquiries:
• The findings of and recommendations ofNCEPOD Parental Nutrition Study havebeen addressed by the relevant services. Atwelve month action plan is underwayincluding guidelines for criteria foradministration, patient monitoring anddocumentation, storage of parentalnutrition and care of central venouscatheters. Completion of this is dueSeptember 2011.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 32

33
• The findings of and recommendations ofNCEPOD Surgery in the elderly have beenaddressed by the relevant services. Fullcompliance with the recommendationsnoted with mental capacity assessment,senior clinicians in-put into decisionmaking, nutritional assessment, intra-operative care and the availability of anAcute Pain Service. The remainingrecommendations including assessment offrailty, daily input from physicians andmonitoring of delays to surgery are part ofa twelve month action plan. Completion ofthis is due November 2011.
The reports of one hundred and eight localclinical audits were audits reviewed by
provider in 2010/ 11 and County Durham andDarlington NHS Foundation Trust intends totake the following actions to improve thequality of healthcare provided:
• Change to guideline regardingadministration of antibiotics and infectionscreening for management of earlypregnancy failure;
• Reformatting of pre assessment guidelinesto identify which patients need to havereview by General Practitioner if cataractsurgery is cancelled;
• Emergency Department audit identifiedthat there is adherence to NICE guidanceon the timing of CT head scan;
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Trust invests in new high spec CT scanner for Bishop Auckland Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 33

34
• Venous thrombembolism (VTE) audit withinthe surgical unit showed improvement inVTE assessment since the audit of recordkeeping was carried out earlier in the year;
• Weekly consultant nurse led hair clinic tostart in May 2011 following the results ofan audit of diphencyprone treatment inalopecia areata;
• To investigate the roll out of voicerecognition (VR) in ultrasound as an auditin Radiology demonstrated that VR at onesite reduced report verification time;
• Electronic requesting to be implemented inradiology; and
• Normal birth champions identified topromote normal birth.
ResearchThe number of patients receiving NHS servicesprovided or sub-contracted by CountyDurham and Darlington NHS Foundation Trust(Trust) in 2010/2011 that were recruitedduring that period to participate in researchapproved by a research ethics committee wastwo thousand and seventeen.
Participation in clinical research demonstratesCounty Durham and Darlington NHSFoundation Trust’s commitment to improvingthe quality of care we offer and to makingour contribution to wider healthimprovement. Our clinical staff stay abreast ofthe latest possible treatment possibilities andactive participation in research leads to betterpatient outcomes.
During 2010/2011, the Trust was involved inconducting NIHR Portfolio clinical researchstudies as follows:
Cancer Studies – Medical Directorate;Cancer Studies – Surgical Directorate;Cancer Study – Obstetrics and Gynaecology;Cancer Study – Radiology;Cancer Study – Pathology;Anaesthetics and critical care;Cardiovascular;Dementias and Neurodegenerative; Diabetes; Eye;Generic Health Relevance;Infection;Musculoskeletal (Rheumatology);Paediatrics;Oral and Gastrointestinal (inc. colorectal);Reproductive Health and Childbirth;Skin (dermatology); andStroke.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Cardio Team at Darlington Memorial Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 34
35
The Trust was also involved in the followingnon-NIHR clinical research studies:
• Anaesthetics and critical care;• Cardiovascular;• Musculoskeletal (Orthopaedic);• Musculoskeletal (Rheumatology);• Musculoskeletal (Physiotherapy);• Paediatrics;• Renal and Urogenital;• Reproductive Health; and• Skin.
Our engagement with clinical research alsodemonstrates County Durham and DarlingtonNHS Foundation Trust’s commitment totesting and offering the latest medicaltreatments and techniques.
CQUINA proportion of County Durham andDarlington NHS Foundation Trust’s income in2010/11 was conditional on achieving qualityimprovement and innovation goals agreedwith NHS County Durham and Darlingtonthrough the Commissioning for Quality andInnovation payment framework.
Further details of the agreed goals for2010/11 and for the following twelve monthperiod are available electronically atwww.cddft.nhs.uk.
CQC StatementCounty Durham and Darlington is required toregister with the Care Quality Commissionand it is registered to deliver care from thefollowing locations:
- University Hospital of North Durham (UHND);- Darlington Memorial Hospital;- Bishop Auckland Hospital;- Shotley Bridge Community Hospital; and - Chester-le-Street Community Hospital.
The Trust is registered to deliver the following:
- Maternity and Midwifery Services; - Surgical procedures; - Termination of pregnancy; - Treatment of disease, disorder or injury; and - Diagnostic and screening procedures.
County Durham and Darlington NHSFoundation Trust has no conditions on itsregistration.
The Care Quality Commission has not takenenforcement action against County Durhamand Darlington NHS Foundation Trust as of 31March 2011.
Registration has been extended to includepersonal care and community provision for2011/12.
Data QualityData quality improvement plans have beenagreed with our commissioners. CountyDurham and Darlington NHS Foundation Trustwill be taking the following actions toimprove data quality:
• Continuation and expansion ofindependent assurance;
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 35

36
• an annual programme of external auditlooking at both data capture and reportingprocesses in relation to key indicators;
• Spot check processes – Information Serviceswill be undertaking random unannouncedreviews;
• Introduction of a data quality trainingprogramme as part of the lifelong learningannual programme; and
• Expansion of the data quality team andresponsible assurance group membership(to include more clinical and ward basedstaff).
NHS Number and GeneralMedical Practice Code ValidityCounty Durham and Darlington NHSFoundation Trust submitted records during2010/11 to the Secondary Uses Service forinclusion in the Hospital Episode Statisticswhich are included in the latest publisheddata. The percentage of records in thepublished data are in the upper quartile ofperformance and continue to be activelymanaged through the Trust’s informationassurance processes and associated workingforums. An action plan is beingimplemented to ensure all systems whereverpossible are compliant with the use of theNHS number. During 2011/12 thisprogramme includes ED systems as currentperformance is just below the national levelfor use of the NHS number due to lack ofintegration with the main PAS system whichholds the core master patient index.
Performance as follows:
• In-patients – NHS number 99.2% (National 98.4%);
• In-patients – allocated to GP practice 100%(National 99.8%);
• Out-patients – NHS number 99.6%(National 98.8%);
• Out-patients – allocated to GP practice100% (National 99.8%);
• Accident & Emergency NHS number –90.6% (National 91.65%); and
• Accident & Emergency GP practiceidentified 100% (National 99.7%).
Information Governance Toolkit Attainment LevelCounty Durham and Darlington NHSFoundation Trust Information GovernanceAssessment Report overall score for 2010/11was 88% and was graded “green”.
Clinical Coding Error RateThe clinical coding external audit independentassurance programme, supporting PBR dataquality, was replaced in 2010/11 by a referencecost audit which resulted in an overallassessment of “good”, with adequate controlsbeing recognised as being in place. Internally,the accredited clinical coding auditors havecontinued to undertake local audit (as pernational guidance). Results indicate thatperformance is in line with InformationGovernance Toolkit Level 2 requirements, with performance for primary diagnosis andprocedures being identified in 90% of cases orbetter and secondary being 80% or better.
Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 36

37Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Stroke Rehabilitation Evaluation ProjectThe Patient Experience evaluation project ofstroke services has now concluded. ThePhase Two Report and the ComparativeReport are being included within the ‘Seizingthe Future Report’.
Review of Quality PerformanceThis section reflects the priorities identified inthe 2009/10 Quality Account and is dividedinto the three sections of Patient Safety,Effectiveness and Experience.
Patient SafetyReduce MRSA to the Department of Health’sagreed profile. Following considerable effortover a number of years the number of MRSAbacteraemias which are attributed to the Trusthas reduced significantly. There have been atotal of three hospital acquired MRSAbacteraemias during the year whichdemonstrates significant improvement. TheMRSA cases are now divided into pre andpost- 48 hours with the post-48 hour casesbeing attributed to the acute hospital. Awide range of measures are in place andremain under close scrutiny to ensure thatthis fundamental measure of patient safetycontinues to improve.
Monthly MRSA cases against monthly target
0
1
2
3
4
5
6
7
8
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
MRS
A
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 37

38 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Reduce Clostridium difficile infections by70%. During the year we focussed onClostridium difficile reduction throughimproved antibiotic prescribing. The Trust hasmanaged to achieve a 70% reduction in post-48 hour Clostridium difficile infections.
A comprehensive improvement plan was inplace for reduction in Clostridium difficile andthe actions taken by staff have been effectivein reducing cases. A major component of thisis the effective use of antibiotics both inchoice and in duration.
Monthly CDIFF cases against monthly target
0
10
20
30
40
50
60
70
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
CDIF
F
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 38
39Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
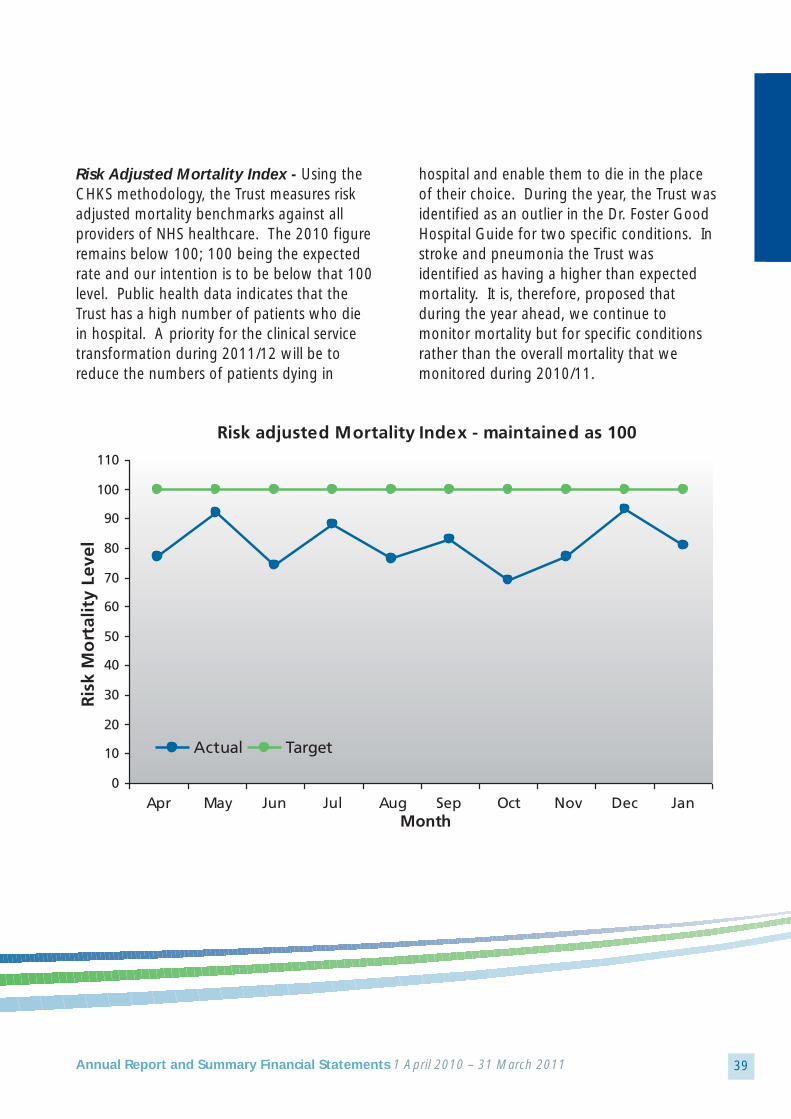
Risk Adjusted Mortality Index - Using theCHKS methodology, the Trust measures riskadjusted mortality benchmarks against allproviders of NHS healthcare. The 2010 figureremains below 100; 100 being the expectedrate and our intention is to be below that 100level. Public health data indicates that theTrust has a high number of patients who diein hospital. A priority for the clinical servicetransformation during 2011/12 will be toreduce the numbers of patients dying in
hospital and enable them to die in the placeof their choice. During the year, the Trust wasidentified as an outlier in the Dr. Foster GoodHospital Guide for two specific conditions. Instroke and pneumonia the Trust wasidentified as having a higher than expectedmortality. It is, therefore, proposed thatduring the year ahead, we continue tomonitor mortality but for specific conditionsrather than the overall mortality that wemonitored during 2010/11.
Risk adjusted Mortality Index - maintained as 100
0
10
20
30
40
50
60
70
80
90
100
110
Apr May Jun Jul Aug Sep Oct Nov Dec JanMonth
Ris
k M
ort
alit
y Le
vel
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 39

40 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Hospital Cardiac Arrests - In order toensure that patients were appropriatelymanaged and their conditions closelymonitored the Trust set in place a system forreducing the number of in-hospital cardiacarrests. Every cardiac arrest is audited by theresuscitation team and if there are indicationsthat the arrest could have been prevented, a
process of audit and education ensues toensure that all staff use the early warningscoring system to identify those patients whoare at risk of deterioration and to takeappropriate action. There has been a slightimprovement in the number of in-hospitalcardiac arrests during the year and this auditwork continues.
Reduce In Hospital Cardiac Arrest (Inappropriate resuscitation) by 10% (No more than 153 - cumulative)
0
20
40
60
80
100
120
140
160
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
Card
iac
Arr
ests
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 40

41Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
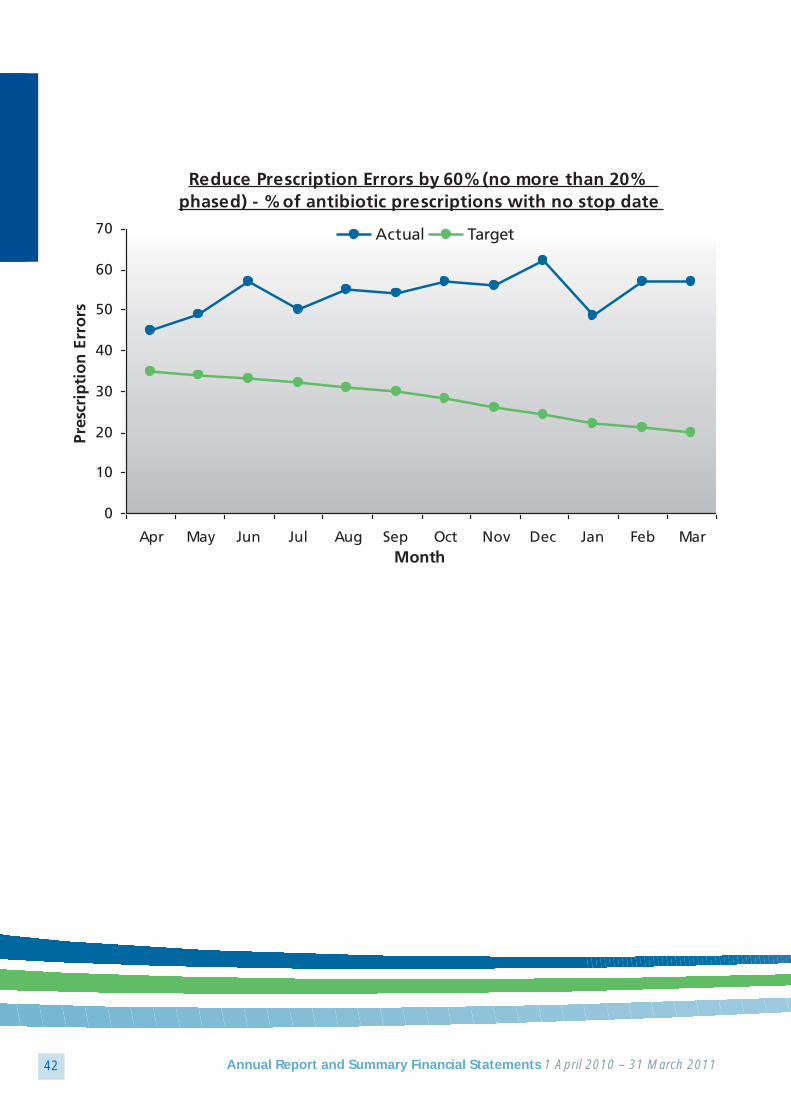
Patient EffectivenessReduction in the Prescription Error Rate -In order to monitor this indicator, we haveused the prescribing of antibiotics and theprocess for review and stopping them. This isaudited on a weekly basis by the antibioticpharmacists. The two graphs below indicatethat there are still some issues to addressabout the appropriate use of antibiotics.
However, we have seen a reduction in theamount of antibiotics prescribed and, whilststop dates are not regularly identified onprescription, review dates are often used byconsultant staff. We will continue with thedrive to reduce antibiotic dependence andensure that appropriate prescription and useis a priority for the organisation.
Reduce Prescription Errors by 60% (no more than 10%) - % of inappropriate antibiotics prescribed
0
2
4
6
8
10
12
14
16
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
Pres
crip
tio
n E
rro
rs
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 41
42 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Reduce Prescription Errors by 60% (no more than 20% phased) - % of antibiotic prescriptions with no stop date
0
10
20
30
40
50
60
70
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
Pres
crip
tio
n E
rro
rs
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 42

43Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Access to CT scans within 24 hours for all stroke admissions
0
10
20
30
40
50
60
70
80
90
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
Acc
ess
to C
T Sc
ans
Actual Target
Access to CT Scans within 24 Hours for atleast 70% of Stroke Admissions - Theambition of the Trust is to improve stroke careand ensure that we adhere to all of thestandards within the National Sentinel Audit.Access to CT scans was a challenge for theTrust and this work has been monitored veryclosely during the year along with all other
stroke standards. A consultation process iscurrently underway around the centralisationof hyper-acute stroke services, in order toinform services. However, we have seenthroughout the year good performance inenabling stroke patients to access CT scansquickly.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 43

44 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Surgery within 36 hours for FracturedNeck of Femur for at least 60% ofPatients - The Trust has been targeting thisarea by providing additional trauma list toensure that patients can get to theatre assoon as possible, as it is well known thatoutcomes improve if the patient is operated
on rapidly after the event. A significantpressure on the trauma service has beenevident during the winter months but theTrust continues to strive to improve the ‘eventto operation time’ for fractured neck of femur.
Surgery with 36 hours - All medically fit Fractured neck Femur patients
0
10
20
30
40
50
60
70
80
90
100
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
Surg
ery
wit
hin
36
ho
urs
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 44
45Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
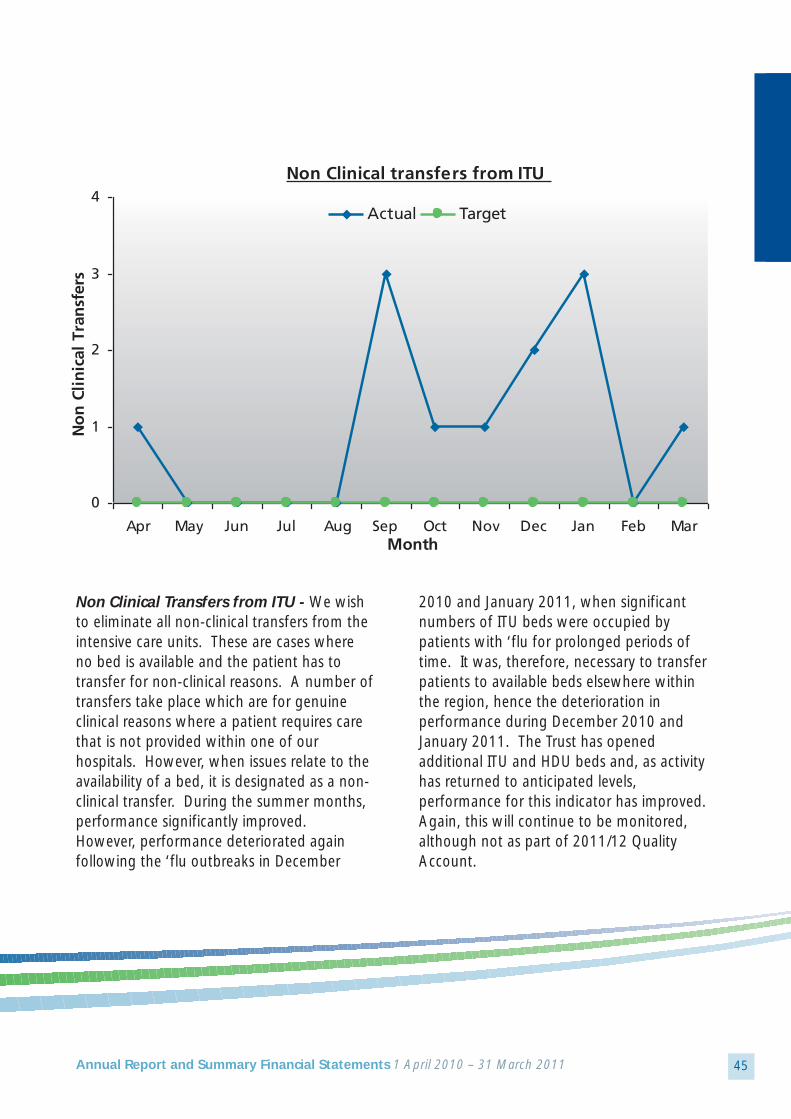
Non Clinical Transfers from ITU - We wishto eliminate all non-clinical transfers from theintensive care units. These are cases whereno bed is available and the patient has totransfer for non-clinical reasons. A number oftransfers take place which are for genuineclinical reasons where a patient requires carethat is not provided within one of ourhospitals. However, when issues relate to theavailability of a bed, it is designated as a non-clinical transfer. During the summer months,performance significantly improved.However, performance deteriorated againfollowing the ‘flu outbreaks in December
2010 and January 2011, when significantnumbers of ITU beds were occupied bypatients with ‘flu for prolonged periods oftime. It was, therefore, necessary to transferpatients to available beds elsewhere withinthe region, hence the deterioration inperformance during December 2010 andJanuary 2011. The Trust has openedadditional ITU and HDU beds and, as activityhas returned to anticipated levels,performance for this indicator has improved.Again, this will continue to be monitored,although not as part of 2011/12 QualityAccount.
Non Clinical transfers from ITU
0
1
2
3
4
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
No
n C
lin
ical
Tra
nsf
ers
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 45
46 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
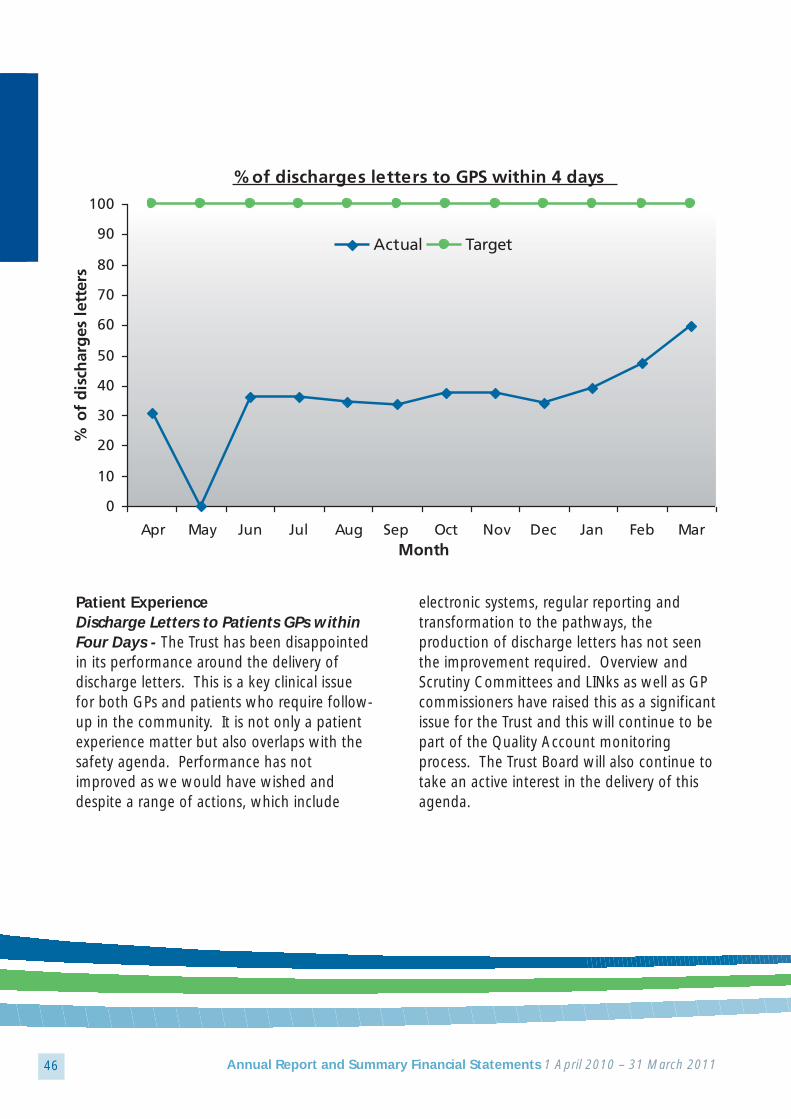
Patient ExperienceDischarge Letters to Patients GPs withinFour Days - The Trust has been disappointedin its performance around the delivery ofdischarge letters. This is a key clinical issuefor both GPs and patients who require follow-up in the community. It is not only a patientexperience matter but also overlaps with thesafety agenda. Performance has notimproved as we would have wished anddespite a range of actions, which include
electronic systems, regular reporting andtransformation to the pathways, theproduction of discharge letters has not seenthe improvement required. Overview andScrutiny Committees and LINks as well as GPcommissioners have raised this as a significantissue for the Trust and this will continue to bepart of the Quality Account monitoringprocess. The Trust Board will also continue totake an active interest in the delivery of thisagenda.
% of discharges letters to GPS within 4 days
0
10
20
30
40
50
60
70
80
90
100
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarMonth
% o
f d
isch
arg
es l
ette
rs
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 46

47Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Complaints from Patients and Relativesabout Car Parking - It was identified during2010/11 that car parking was of graveconcern to patients and relatives particularlyfollowing the ‘Seizing the Future’reconfiguration of hospital services.Complaints remain relatively low, however,this is not reflected in conversations withpatients who often quote car parking as one
of their significant problems when attendingthe hospital. It is proposed during 2011/12 to implement a system for immediatefeedback from patients which will assist us inaddressing concerns about car parking. TheTrust has also received additional planningpermission to provide extra spaces on theDarlington Memorial Hospital site whichshould alleviate some of the difficulties.
Complaints from patients and relatives about Car Parking (Cumulative)
0
5
10
15
20
25
Month
Com
pla
ints
Actual Target
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 47

48 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Complaints about the attitude of staffComplaints monitoring and learningprocesses identified that the attitude of staffwas frequently mentioned as a reason for thecomplaint. During 2010/11 we monitoredclosely and requested feedback on actionfollowing a complaint about attitude. Wherewe identified an issue with an individual thiswas managed through the Trust internalprocesses. Wider issues associated with staff
stress and provocation are managed throughmanagement processes in place. As thisindicator continues to increase we will beundertaking further as part of our dignity incare campaign during the coming year toensure patients receive appropriate respectand are treated with the utmost dignity whilstin our care. We are disappointed with thisperformance and view it as a very significantconcern that needs to be addressed.
Complaints about the attitude of staff
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 48

49Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Quality MonitoringAn overview of all of the quality indicators ismonitored by the Trust Board not only for theQuality Accounts but also for CQUIN, Monitorand for the CQC. These indicators give a fullassessment of the quality of care provided bythe Trust.
Clinical Strategy DevelopmentAs a result of the merger between hospitaland community services and, in order to takethe Trust the forward in becoming thepremier provider of healthcare for the peopleof this area, a new clinical strategy is beingdeveloped. The clinical strategy aims toensure the best health outcomes for patients,an excellent patient experience and highquality, low cost services for commissioners.It aims to ensure we provide more care closerto the patient’s home and to shift theemphasis from treatment of disease towardsprevention of ill health. There are a numberof implications and challenges within thestrategy that are currently being workedthrough. The clinical strategy has sevenwork-streams. These are:
• Long-term conditions; • Care of older people; • Women and children; • Acute medicine and emergency care; • Elective medical care;• Surgery; and• End of life.
Each one of these work-streams has a plan inplace to deliver significant improvements and
achieve the aims of the strategy. Large scaleplanning events have been held with all ofour stakeholders and it is expected that thestrategy will be completed during the year2011/12.
Patient Involvement Activity
Divisional Surveys Fifty six divisional surveys were concludedbetween January 2010 and March 2011.Twenty two divisional surveys havecommenced since October 2010.
It is essential that feedback provided bypatients is acted upon in order to ensure safe,effective practice and enhance the patientexperience. All staff requesting local surveysagreed to complete an action plan as a resultof issues identified. All action plans will beavailable to survey leads, divisional managersand nurse leads.
As a result of patient feedback, actions havebeen agreed to improve the patientexperience. Key themes have emergedthroughout the Trust, including issuespertaining to communication, serviceprovision and the environment.
CommunicationNew patient leaflets have been produced andconsent leaflets updated. Informationregarding waiting times has been displayed.General displays are regularly updated.Improvements have been made to
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 49

50 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
information provided in appointment lettersto allow for improved understanding. Policiesand guidelines have been updated. There isan improved, timelier response to patientsafter initial diagnosis of some conditions.Work practices have been reviewed in orderto provide timely information to patients.
EnvironmentImprovements have been made to thehospital environment to increase privacy andto improve access to areas. Issues aboutcleanliness have been acted upon.
Post Discharge SurveyA post-discharge survey has been carried out quarterly throughout 2010/2011. Thequestions were agreed with commissionersand reflect the national in-patient survey. All
CQUIN indicator questions are also included.Results are compared to the national in-patient survey scores. This allows divisions toidentify emerging themes and areas whereimprovements are necessary. Divisional actionplans are prepared in order to tackle theissues identified.
Areas where the Trust has consistentlycompared favourably to the national in-patient survey include two of the CQUINindicator questions:
a) Finding a member of staff to discuss anyworries, concerns or fears; and
b) Staff telling patients about the side effectsof medication to watch out for when they returned home, in a way that they couldunderstand.
Patient Experience Indicator Questions National Q2 Q3 Q4In-Patient Survey 2009/10 2010 2010 2011
Did you feel involved enough in decisions about your 74 78 74 70 care and treatment?
Were you given enough privacy when discussing your 82 83 82 70condition or treatment?
Did you find a member of staff to discuss any 65 85 84 79worries or fears that you had?
Did a member of staff tell you about any medication side 53 70 56 63effects that you should watch out for after you got home in a way that you could understand?
Did hospital staff tell you who you should contact 87 75 67 76if you were worried about your condition or treatment after you left hospital?
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 50
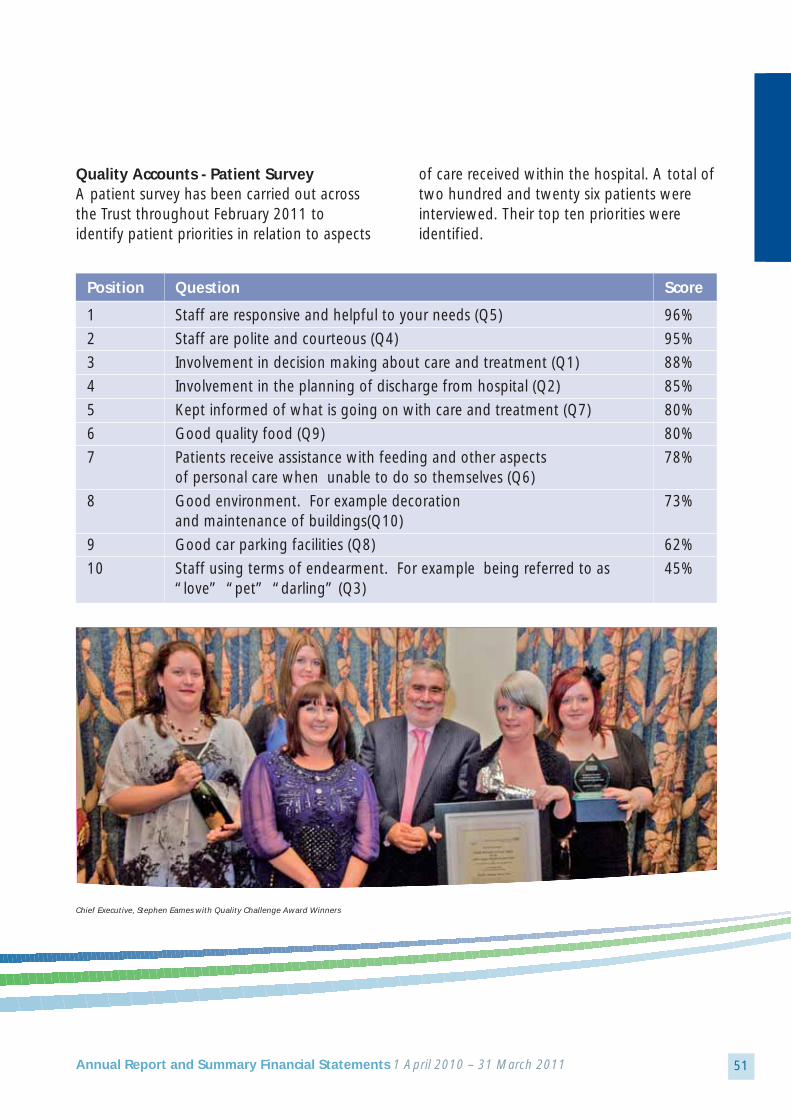
51Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Quality Accounts - Patient SurveyA patient survey has been carried out acrossthe Trust throughout February 2011 toidentify patient priorities in relation to aspects
of care received within the hospital. A total oftwo hundred and twenty six patients wereinterviewed. Their top ten priorities wereidentified.
Chief Executive, Stephen Eames with Quality Challenge Award Winners
Position Question Score
1 Staff are responsive and helpful to your needs (Q5) 96%
2 Staff are polite and courteous (Q4) 95%
3 Involvement in decision making about care and treatment (Q1) 88%
4 Involvement in the planning of discharge from hospital (Q2) 85%
5 Kept informed of what is going on with care and treatment (Q7) 80%
6 Good quality food (Q9) 80%
7 Patients receive assistance with feeding and other aspects 78%of personal care when unable to do so themselves (Q6)
8 Good environment. For example decoration 73%and maintenance of buildings(Q10)
9 Good car parking facilities (Q8) 62%
10 Staff using terms of endearment. For example being referred to as 45%“love” “pet” “darling” (Q3)
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 51

52 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Clinical Strategy
Patient SurveyIn line with the Clinical Strategy agenda, apatient survey has been carried outthroughout February 2011 to identify patientopinion in relation to offering care andservices closer to home. Ninety six patientswere interviewed across the Trust.
Summary of FindingsOver half of respondents felt thatphysiotherapy and blood tests should beavailable in the community.
Advantages of Delivering Services in the Hospital SettingRespondents felt that the advantages ofcontinuing to deliver services in a hospitalsetting were that staff were better qualifiedand specialised in their fields than staff in thecommunity.
A hospital can offer all services under oneroof which makes visits faster and moreconvenient for patients. Patients explainedthat they feel more secure in a hospitalsetting, knowing there is back up available formore serious or emergency situations at alltimes of day and night.
Patients like the continuity of care they getfrom seeing the same staff members everytime and they feel better looked after in ahospital setting.
Disadvantages of Delivering Services in the Hospital SettingRespondents felt the main disadvantages ofdelivering services in a hospital settingcentred on access to hospital, car parking andcar parking costs, which were thought to beinconvenient and too expensive.
In addition, they find a hospital settingstressful. Waiting times are too long andgetting an appointment (which subsequentlygets cancelled) to be particularly frustrating.
Advantages of Delivering Services in the Community SettingRespondents felt the main advantages ofdelivering services in the community werethat they would be more accessible and less
Local school pupils learn CPR skills as part of the successful William Harvey Project
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 52
53Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
time consuming. They would travel less andbe able to get treatment quicker from staff intheir own GP surgeries who they werefamiliar with and who knew them.
Disadvantages of Delivering Services in the Community SettingRespondents felt that if services wererelocated to the community there would befewer services available to them. Therewould be fewer skilled, specialised staff and alack of specialised equipment available. Theyfeel that they would have to wait longer toreceive treatment and have to see differentdoctors who did not know their histories.
They feel that relocation to the communitywould cause a duplication of services whichwould be costly and time consuming for staff.They would not feel as confident receivingtreatment knowing they were not in ahospital as they get security from knowingthere is back-up available should there be anyproblems. They feel that it is not appropriateand hospitals are better equipped to deliverservices.
Relocating them to the community wouldcause extreme pressure on GP surgeries andthey may have to make multiple visits aseverything may not be under one roof.
Respondents also felt that they get anexcellent service from their local hospitals,although they feel Bishop Auckland Hospital
is under-utilised. Although some respondentsfeel that services should be available in boththe community and hospitals, many arehappy with things the way they are andwould not like things to change.
National Surveys
In-patient SurveyThe 2010/2011 in-patient survey hasconcluded. The final report is being publishedby the CQC. Divisional action plans will bedeveloped to address such issues as areidentified.
The National Maternity Survey has concludedand the results have been issued to the Trust.An Action Plan has been completed.
Cancer SurveyThe National Cancer Survey has concluded.An action plan is under development by theCancer Services Team.
Feedback from NHS Choices A review of patient feedback from NHSChoices has been undertaken.
The new Trust website will include a link toNHS Choices. The NHS Choices site offers theopportunity for Trusts to promote theirdepartments, services and profiles. In order toencourage feedback to the NHS Choiceswebsite, we are in the process of providing acard to be given to patients. The card will
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 53

54 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
contain website details for NHS Choices aswell as the County Durham and DarlingtonNHS Foundation Trust website address toprovide online feedback. This will be pilotedacross agreed wards and departments.
The CQC quality and risk profile 2010highlighted a number of positive and negativecomments displayed on NHS Choices website.
Outcome: Positive Negative
1. Respecting and involving people who use services 9 8
4. Care and welfare of people who use services 9 8
5. Nutrition 1 2
6. Co operating with other providers 0 0
7. Safeguarding people from abuse 0 0
8. Cleanliness and infection control 4 2
9. Management of medicines 0 0
10. Safety and suitability of premises 0 3
11. Safety and suitability of equipment 0 0
12. Requirements relating to workers 0 1
13. Staffing 0 2
14. Supporting staff 0 0
16. Assessing and monitoring service provision 0 0
17. Complaints 0 0
21. Records 0 0
TOTAL 23 26
NHS Choices feedback relating to CQC Outcomes 1-9-09 to 31-12-09
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 54

55Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Corporate LeafletsAll corporate leaflets are being reviewed toensure that an easy read version is available.Service users are involved in this work and theHealth and Wellbeing sub-group of theLearning Disability Partnership Board isratifying the leaflets prior to publication.
Leaflets now ratified are:
• Chaplains;• Concerns/complaints;• Compliments/comments;• Your Rights; and• Your Responsibilities.
Research re PPIThe Trust is supporting Durham University in aresearch project on patient and publicinvolvement (PPI). PPI representatives are alsomembers of the County Durham and TeesValley NIHR (National Institute for HealthResearch) Comprehensive Local ResearchNetwork.
Race Equality CharterLiaison with BME Community Services isongoing to allow the Trust to promote theRace Equality Charter across all hospital sites.
This includes:
• Posters “Delivering Race Equality Charter”;• Drop down interpreter card; and• Interpreter training.
The project has been agreed by the Trust and will be initiated early in 2011/12.
DAD ProjectWe are working with DAD (DarlingtonAssociation on Disability) Carers Services toenhance the experience of carers. The projectwill identify and support carers who do nottraditionally identify themselves as carers orreveal their caring responsibilities to statutoryor third sector services.
The DAD Service will liaise with outpatientdepartments at Darlington Memorial Hospitalto support staff to identify carersaccompanying patients to appointments.
DAD will support the production of postersand leaflets to help carers identify themselves.
DAD will provide training to appropriate staff,specifically those involved in falls clinics andwithin stroke services to identify and supportcarers.
Sister Greta Jones leading her team in the Quality Challenge
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 55

56 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Gypsy Traveller ProjectA health needs assessment of gypsy andtraveller communities in County Durham andDarlington was commissioned by DurhamCounty Council and NHS Darlington. The eightmonth assessment concluded in December2010. The approach to commissioning theassessment was based on the regional healthstrategy “Better Health, Fairer Health: AStrategy for 21st Century Health and WellBeing in the North East of England”.
The Health Needs Assessment consisted of:
• Identification of the population of gypsiesand travellers in County Durham andDarlington;
• A household survey about gypsy/travellerhealth and social care needs;
• A family history project identifying historicpatterns of health and well-being;
• Consultation with stakeholders to find outthe views of service providers;
• A review of policies and services for gypsiesand travellers;
• A summary of service review findings andstakeholder views is available; and
• Focus groups and service planning eventshave taken place in February 2010 in orderto identify and plan appropriate services.
Experiences of CarersWe are currently working in partnership withDurham Carers Network (DCN) and DADCarers Support Services to ascertain the viewsof carers who have experienced acute Trustservices across County Durham and Darlington.
Information has been received after a requestfor carers’ views was published in CarerNetwork newsletters. We have currentlyreceived eleven responses and are in theprocess of sharing the content withappropriate wards and departments. Actionplans will be produced in response tocomments received and a generic responsewill be provided via carer newsletters.
Local Involvement NetworksWe are currently working with both Durhamand Darlington LINks to arrange Enter andView sessions in early 2011/12. The sessionswill focus on the views and experiences ofpatients who access out-patient departmentsacross the Trust.
LINk has the right in certain circumstances toenter and view health and social care servicepremises to observe and assess the natureand quality of those services and to obtainthe views of the people using those services.
Durham County Council's Adults’Wellbeing and Health Overviewand Scrutiny Committee ResponseThe Committee welcomes County Durhamand Darlington NHS Foundation Trust’sQuality Accounts and the opportunity toprovide comment on it. This is the secondyear the Committee has provided commentand acknowledge progress by the Trusttowards delivery of their priority areas for2010/11. Within last year’s response,Members commented on the timeliness ofinformation and need for earlier engagement
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 56

57Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
to identify forthcoming priorities. It is pleasingto report that the Trust has engaged with theCommittee to provide comment and shapepriorities within this year’s plan. The Committee held a workshop session withExecutive Members from the Trust andreceived progress against delivery of 2010/11priorities and debated the suggested priorityareas within the 2011/12 Quality Accountsreport. Following this workshop, theCommittee submitted a response thatidentified key points from debate and weacknowledge that the Trust has includedcomments from the Committee within itspriority areas. Additional comments raised byMembers identified concern with monitoringfood and nutrition intake for patients withspecific medical conditions i.e. diabetes. Members of the Committee suggested thatthe Trust ensure robust monitoring of theincidence of falls amongst patients receivingcommunity health services within their home. Members of the Committee note the mergerof Community Health Services to the Trustfrom April 2011 and acknowledge the Trust’snew vision and note that priorities fromCommunity Health Services are reflectedwithin the Trust’s 2011/12 Quality Accounts.To conclude, the Committee agree that, fromthe information received from the Trust, theidentified priorities are a fair reflection ofhealthcare services provided by the Trust. Inaddition, the Committee request to receive asix monthly progress report on delivery of2011/12 targets.
LINk ResponseDarlington LINk feels that the QualityAccounts seem accurate and representative ofthe quality of service provided by CountyDurham and Darlington NHS Foundation Trustfrom the information available and it hasgiven us comprehensive details of the servicesdelivered over the year.
Darlington LINk would welcome theopportunity to continue to be involved in thedevelopment of the quality agenda andpriorities in future years.
NHS County Durham and Darlington(NHSCDD) ResponseExamples of the patient involvement activitydemonstrate a vast array of differentmethodologies to capture the patientexperience and involvement. AsCommissioners we would like to reflect onsome of these examples and explore furtherwith the Foundation Trust some of the resultsto work together to improve the patient’sexperience.
Information contained in the Quality Accountprovides a broad overview of what the Trusthas achieved and NHSCDD can corroboratethe progress the Trust is making in relation toa range of quality indicators included in thereport and are pleased with the ambitiousplans to improve the quality of servicesdelivered in terms of patient safety, patientexperience and clinical effectiveness in thecoming year.
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 57

58 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
NHSCDD agree with the priorities for thecoming year and the rationale for their choice.NHSCDD also believe they are achievable andwill work with the Trust to deliver thesepriorities. The plans for implementation anddelivery will be monitored through the existingreporting mechanisms in place, andCommissioner visits.
The coming year will hold many challenges notleast of which is delivering high quality, safe,and effective services during a time ofeconomic uncertainty, major organisationalchallenges with the transfer of County Durhamand Darlington Community Services and widerNHS reforms. NHSCDD will continue to workcollaboratively with CDDFT to ensure thatquality remains at the heart of everything wedo in the NHS County Durham and Darlington.
National Audit/National Applicable Data collection % casesConfidential Enquiry Title to Trust Participation completed submitted
Services Apr 10 – Mar 11
Peri and neonatal
Perinatal mortality (CEMACH) Ongoing 100%
Neonatal intensive and special care (NNAP) 100%
Children
Paediatric pneumonia (British Thoracic Society) 100%
Paediatric asthma (British Thoracic Society) 84%
Paediatric fever (College of Emergency Medicine) 100%
Childhood epilepsy (RCPH National Childhood Data collectionEpilepsy Audit) 2011/12
Paediatric intensive care (PICANet) X
Paediatric cardiac surgery (NICOR Congenital XHeart Disease Audit)
Diabetes (RCPH National Paediatric 100% casesDiabetes Audit) on database
sent
Acute Care
Emergency use of oxygen (British Thoracic Society) X
Adult community acquired pneumonia (British Thoracic Society) *100%
Non invasive ventilation (NIV) - adults (British Thoracic Society) X
Pleural procedures (British Thoracic Society) *100%
*Required sample of 20 patients collected
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 58

59Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
National Audit/ National Applicable Data collection % casesConfidential Enquiry Title to Trust Participation completed submitted
Services Apr 10 – Mar 11
Cardiac arrest (National Cardiac Arrest Audit) X
Vital signs in majors 99%(College of Emergency Medicine)
Adult critical care (Case Mix Programme) 100%
Potential donor audit (NHS Blood & Transplant) 100%
Long Term Conditions
Diabetes (National Adult Diabetes Audit) 100% of cases on database
Heavy menstrual bleeding (RCOG National XAudit of HMB)
Chronic pain (National Pain Audit) Not Organisational applicable
data only
Ulcerative colitis & Crohn’s disease X(National IBD Audit)
Parkinson’s disease (National Parkinson’s Audit) X (Participate 2011/12)
COPD (British Thoracic Society/European Audit) X
Adult asthma (British Thoracic Society) X
Bronchiectasis (British Thoracic Society) X
Elective procedures
Hip, knee and ankle replacements Obtaining(National Joint Registry)
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 59

60 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
National Audit/National Applicable Data collection % casesConfidential Enquiry Title to Trust Participation completed submitted
Services Apr 10 – Mar 11
Elective surgery (National PROMs Programme) 52.3%
Cardiothoracic transplantation X(NHSBT UK Transplant Registry)
Coronary angioplasty (NICOR Adult cardiac Xinterventions audit)
Peripheral vascular surgery 60%(VSGBI Vascular Surgery Database)
Carotid interventions 39%(Carotid Intervention Audit)
CABG and valvular surgery X(Adult cardiac surgery audit)
Cardiovascular Disease
Familial hypercholesterolaemia Not(National Clinical Audit of Mgt of FH) Organisational applicable
Audit return only
Acute Myocardial Infarction & other ACS 100%(MINAP)
Heart failure (Heart Failure Audit) **Ongoing 60%
Pulmonary hypertension X(Pulmonary Hypertension Audit)
Acute stroke (SINAP) Ongoing Qtrly/Interimdata collection reports rec’d
on ongoing basis
Stroke care (National Sentinel Stroke Audit) 100%
Renal disease
Renal replacement therapy (Renal Registry) X
Renal transplantation X(NHSBT UK Transplant Registry)
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 60

61Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
National Audit/National Applicable Data collection % casesConfidential Enquiry Title to Trust Participation completed submitted
Services Apr 10 – Mar 11
Patient transport (National Kidney Care Audit) X
Renal colic (College of Emergency Medicine) 91%
Cancer
Lung cancer (National Lung Cancer Audit) ** 100%
Bowel cancer (National Bowel Cancer ** 99%Audit Programme)
Head & neck cancer (DAHNO) ** 100%
Trauma
Hip fracture (National Hip Fracture Database) *100%
Severe trauma (Trauma Audit X& Research Network)
Falls and non-hip fractures 100%(National Falls & Bone Health Audit)
Psychological conditions
Depression & anxiety (National Audit Xof Psychological Therapies)
Prescribing in mental health services (POMH) X
National Audit of Schizophrenia (NAS) X
Blood transfusion
O neg blood use (National Comparative 100%Audit of Blood Transfusion)
Platelet use (National Comparative 100%Audit of Blood Transfusion)
* Validation of cases not totally complete for data in 10/11 but 100% indicated. **Data collection deadline in 2010/11 for patients covering period 09/10
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 61
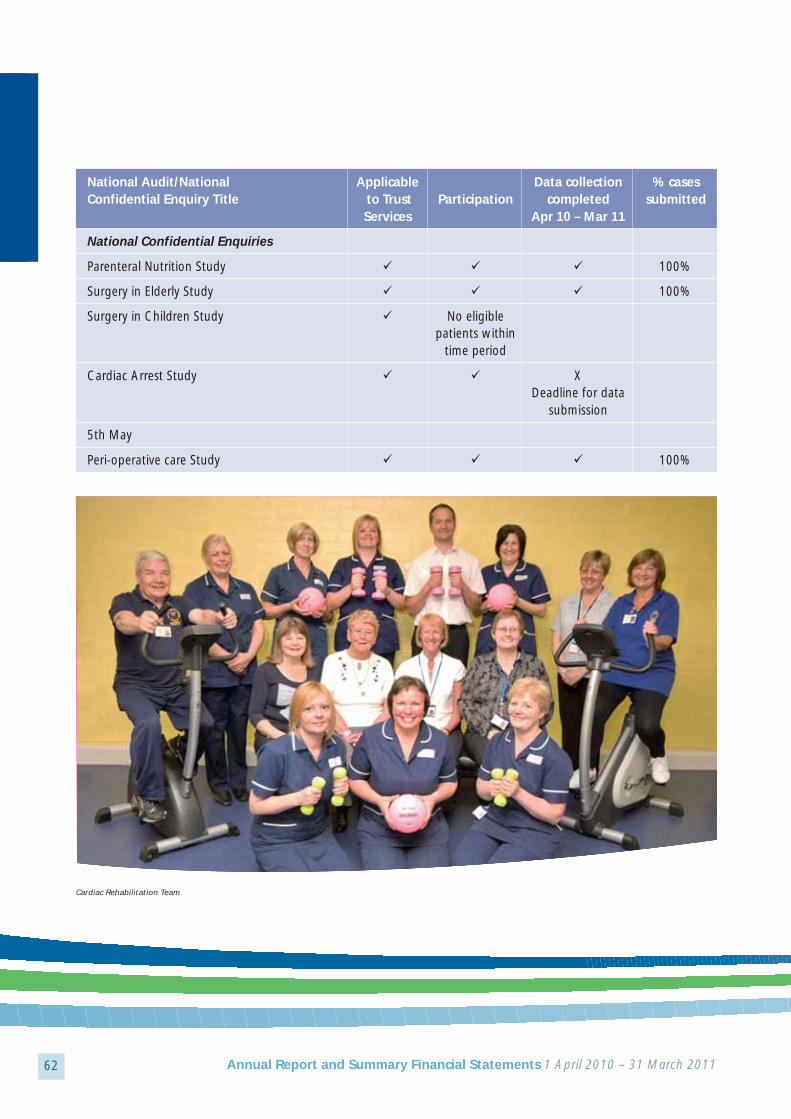
62 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
National Audit/National Applicable Data collection % casesConfidential Enquiry Title to Trust Participation completed submitted
Services Apr 10 – Mar 11
National Confidential Enquiries
Parenteral Nutrition Study 100%
Surgery in Elderly Study 100%
Surgery in Children Study No eligible patients within
time period
Cardiac Arrest Study XDeadline for data
submission
5th May
Peri-operative care Study 100%
Cardiac Rehabilitation Team
32868_AR_Public_32868_AR_Public 30/06/2011 14:58 Page 62

63Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Statement of Directors’ Responsibilities in respect of the Quality ReportThe Directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations 2010 to prepare Quality Accounts for each financial year.
Monitor has issued guidance to NHS foundation trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that foundation trust boards should put in place to support the data quality for the preparation of the quality report.
In preparing the quality report, the Directors are required to take steps to satisfy themselves that:
• the content of the quality report meets the requirements set out in the NHS Foundation Trust Annual ReportingManual 2010-11;
• the content of the Quality Report is not inconsistent with internal and external sources of information including:
• Board minutes and papers for the period April 2010 to June 2011• Papers relating to Quality reported to the Board over the period April 2010 to June 2011• Feedback from the commissioners dated 13 May 2011• Feedback from governors dated 9 May 2011• Feedback from LINks dated 12 May 2011• The Trust’s complaints report published under regulation 18 of the Local Authority
Social Services and NHS Complaints Regulations 2009, dated 1 August 2010• The national patient survey dated 26 May 2011• The national staff survey dated 16 March 2011• The Head of Internal Audit’s annual opinion over the Trust’s
control environment dated 20 May 2011• CQC quality and risk profiles dated 6 December 2010
• the Quality Report presents a balanced picture of the NHS foundation trust’s performance over the period covered;
• the performance information reported in the Quality Report is reliable and accurate;
• there are proper internal controls over the collection and reporting of the measures of performance included in theQuality Report, and these controls are subject to review to confirm that they are working effectively in practice;
• the data underpinning the measures of performance reported in the Quality Report is robust and reliable,conforms to specified data quality standards and prescribed 107 definitions, is subject to appropriate scrutiny andreview; and the Quality Report has been prepared in accordance with Monitor’s annual reporting guidance (whichincorporates the Quality Accounts regulations) (published at www.monitornhsft.gov.uk/annualreportingmanual) aswell as the standards to support data quality for the preparation of the Quality Report (available at www.monitornhsft.gov.uk/annualreportingmanual) ).
The Directors confirm to the best of their knowledge and belief they have complied with the above requirements inpreparing the Quality Report.
By order of the Board
.............................................. Date ......................................................................... Chairman
.............................................. Date ......................................................................... Chief Executive
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 63

64 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Prime Minister and Earl Howe visit Darlington Memorial Hospital
Local communities are kept up to date with investments being madeat Darlington Memorial Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 64

65Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Independent Auditor’s Opinionon the Quality Accounts
We have been engaged by the Council ofGovernors of County Durham and DarlingtonNHS Foundation Trust to perform anindependent assurance engagement inrespect of the content of County Durham andDarlington NHS Foundation Trust’s QualityReport for the year ended 31 March 2011(the “Quality Report”).
This report, including the conclusion, hasbeen prepared solely for the Council ofGovernors of County Durham and DarlingtonNHS Foundation Trust as a body, to assist theCouncil of Governors in reporting CountyDurham and Darlington NHS FoundationTrust’s quality agenda, performance andactivities. We permit the disclosure of thisreport within the Annual Report for the yearended 31 March 2011, to enable the Councilof Governors to demonstrate they havedischarged their governance responsibilitiesby commissioning an independent assurancereport in connection with the Quality Report.To the fullest extent permitted by law, we donot accept or assume responsibility to anyoneother than the Council of Governors as abody and County Durham and DarlingtonNHS Foundation Trust for our work or thisreport save where terms are expressly agreedand with our prior consent in writing.
Scope and subject matterWe read the Quality Report and consideredwhether it addresses the contentrequirements of the NHS Foundation TrustAnnual Reporting Manual, and consideredthe implications for our report if we becameaware of any material omissions.
Respective responsibilities of the Directors and auditorsThe Directors are responsible for the contentand the preparation of the Quality Report inaccordance with the criteria set out in theNHS Foundation Trust Annual ReportingManual 2010/11 issued by the IndependentRegulator of NHS Foundation Trusts(“Monitor”).
Our responsibility is to form a conclusion,based on limited assurance procedures, onwhether anything has come to our attention
The Trust’s ‘Innovation Day’ celebrated new ideas and recognised improvements driven by our talented staff
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 65
66 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
that causes us to believe that the content ofthe Quality Report is not in accordance withthe NHS Foundation Trust Annual ReportingManual or is inconsistent with thedocuments. We read the other information contained inthe Quality Report and considered whether itis inconsistent with the specified documentsin the Monitor guidance.
We considered the implications for our reportif we became aware of any apparentmisstatements or material inconsistencieswith those documents (collectively, the“documents”). Our responsibilities do notextend to any other information.
Assurance work performedWe conducted this limited assuranceengagement in accordance with InternationalStandard on Assurance Engagements 3000(Revised) – ‘Assurance Engagements otherthan Audits or Reviews of Historical FinancialInformation’ issued by the InternationalAuditing and Assurance Standards Board(‘ISAE 3000’). Our limited assuranceprocedures included:
• Making enquiries of management;
• Comparing the content requirements ofthe NHS Foundation Trust AnnualReporting Manual to the categoriesreported in the Quality Report and;
• Reading the documents.
A limited assurance engagement is less inscope than a reasonable assuranceengagement. The nature, timing and extentof procedures for gathering sufficientappropriate evidence are deliberately limitedrelative to a reasonable assuranceengagement.
LimitationsIt is important to read the Quality Report inthe context of the criteria set out in the NHSFoundation Trust Annual Reporting Manual.
Nursing Quality Conference 2010
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 66
67Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Jenny Chapman MP visited the Trust to recognise International Nurses Day
ConclusionBased on the results of our procedures,nothing has come to our attention thatcauses us to believe that, for the year ended31 March 2011, the content of the QualityReport is not in accordance with the NHSFoundation Trust Annual Reporting Manual.
Deloitte LLPChartered Accountants Leeds6 June 2011
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 67
68 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
This year has again witnessed rapidtransformation of the NHS environment,during which our key objective has beento carry out and complete the duediligence process on the merger with ourlocal community services. We have alsocontinued to consolidate and improve thequality and range of our secondary careservices with a view to moving care closerto home.
The most significant changes in servicedelivery during 2010 have been as a result ofwork undertaken under the auspices of theTowards 2014 programme which has focusedon the following areas:
1. Theatre transformation- the Trust reviewedthe way in which theatre capacity wasused and is currently trialling a system ofextended operating sessions; that is,operating for longer during the daythereby delivering increased capacity on allthe Trust sites.
2. Outpatient review – an on going review tolook at the efficiency and effectiveness ofthe Trust’s outpatient departments,focusing on reducing the time patientswait to be seen when they arrive forappointments and the system forcancelling and re-arranging appointmentsto reduce instances when patients “do notattend” (DNA) for appointments. Thegroup is currently exploring alternativemodels for the delivery of outpatientservices which could revolutionise the wayin which these services are provided.
3. Bed utilisation – the Trust is reviewing howlong patients need to stay in hospital witha view to discharging patients home withappropriate support as soon as possible.
Here is just a sample of the other servicedevelopments through 2010:
1. The appointment of a new vascularsurgeon which will allow us to carry out agreater range of procedures at DarlingtonMemorial Hospital;
2. The appointment of more specialisedorthopaedic surgeons enabling the fullrange of orthopaedic procedures to bedelivered;
3. We continue to grow the plastic surgeryprovision to ensure that patients do nothave to travel to South Tees for theirprocedures;
4. The development of self referral service forpatients requiring termination ofpregnancy. Currently, 70% of patientsrefer themselves rather than goingthrough a health professional;
5. The reconfiguration and integration ofCASH (contraception and sexual health)services across County Durham andDarlington to ensure the service is more inline with patient needs;
Service Developments
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 68

69Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
6. The Ophthalmology service has continuedto expand in the north of the Trust withthe expansion of diagnostic services andlaser treatment for diabetic retinopathy;
7. The joint appointment with South TeesHospitals NHS Foundation Trust of a headand neck cancer specialist means thatpatients will receive a full diagnostic workup of their condition at DarlingtonMemorial Hospital before going to JamesCook University Hospital for surgery;
8. We have worked with colleagues inprimary care to develop a more efficientpathway for patients with suspected deepvein thrombosis (DVT);
9. Development of an ambulatory care modelto assess patients in a timelier manner,generally speeding up their care; and
10.Development of an integrated pathway fordermatology patients across primary andsecondary care. This will be implementedin 2011/12.
In 2010-11, the All Specialties 1st Outpatientmarket in both Durham and Darlington hasgrown. Our share of it has also grown slightly,largely as a result of service expansions. Weare still seeing growth in our market share inSouth Durham and Darlington arising frompast expansions in Dermatology,Rheumatology and Plastics. The more recentexpansions of Ear, Nose and Throat (ENT) andOphthalmology services into North Durhamhave had differing impacts. Growth in ENT hasbeen limited so far but we have capturedabout 55% of the Durham ophthalmologymarket.
Friends of Chester-le-Street Hospital donate a CPX bike to University Hospital of North Durham
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 69

70 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Our new to review ratio also continues to be consistently good.
All Specialties New to Review Ratio: Jan – Dec 2010 *
CDDFT 1.8
South Tees 2.8
City Hospitals Sunderland 2.5
Newcastle 3.2
North Tees and Hartlepool 2.7
Gateshead 3.7
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 70

71Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Our market share continues to be higher inDarlington than in County Durham, partlybecause GPs in Easington, Chester le Streetand North Derwentside tend to refer morefrequently to other nearby trusts; and partlybecause the full effects of the ENT andOphthalmology expansions in the north have
not yet been seen. GP referral patterns tend tochange only slowly as GPs build contact with,and confidence in, new consultants andservices.
We have also broadly maintained our share ofPCT markets close to our boundaries:
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 71
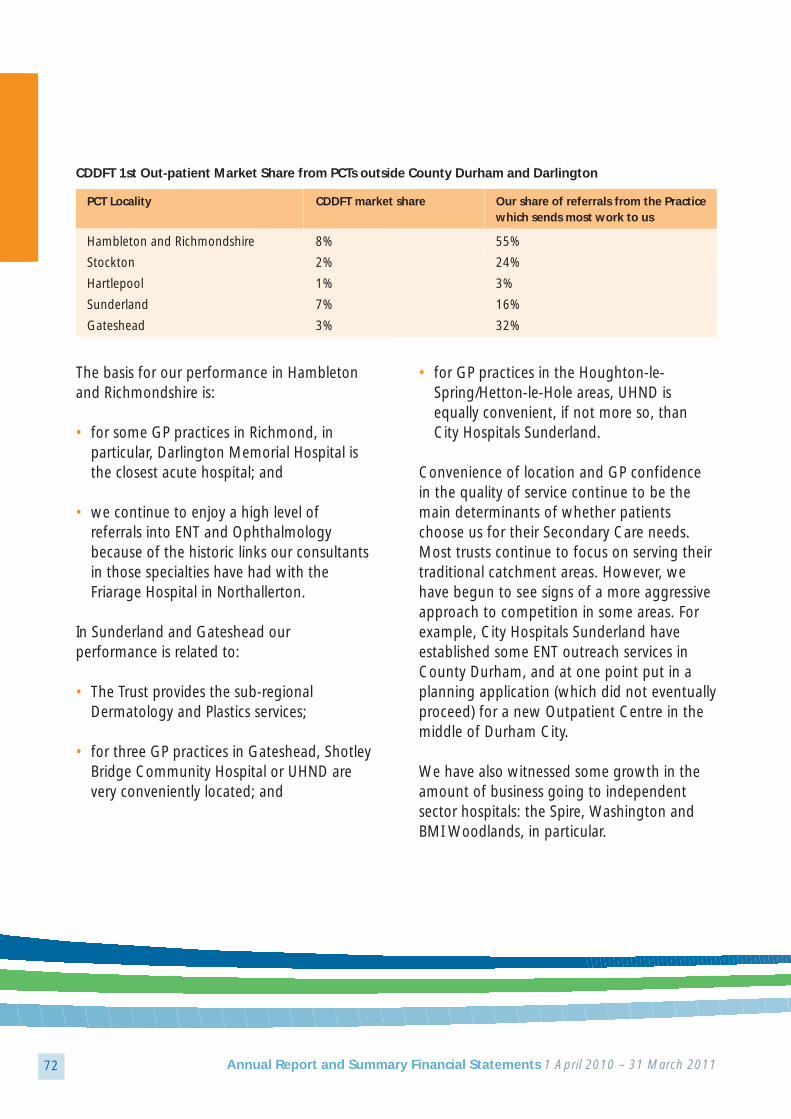
72 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
CDDFT 1st Out-patient Market Share from PCTs outside County Durham and Darlington
PCT Locality CDDFT market share Our share of referrals from the Practice which sends most work to us
Hambleton and Richmondshire 8% 55%
Stockton 2% 24%
Hartlepool 1% 3%
Sunderland 7% 16%
Gateshead 3% 32%
The basis for our performance in Hambletonand Richmondshire is:
• for some GP practices in Richmond, inparticular, Darlington Memorial Hospital isthe closest acute hospital; and
• we continue to enjoy a high level ofreferrals into ENT and Ophthalmologybecause of the historic links our consultantsin those specialties have had with theFriarage Hospital in Northallerton.
In Sunderland and Gateshead ourperformance is related to:
• The Trust provides the sub-regionalDermatology and Plastics services;
• for three GP practices in Gateshead, ShotleyBridge Community Hospital or UHND arevery conveniently located; and
• for GP practices in the Houghton-le-Spring/Hetton-le-Hole areas, UHND isequally convenient, if not more so, thanCity Hospitals Sunderland.
Convenience of location and GP confidencein the quality of service continue to be themain determinants of whether patientschoose us for their Secondary Care needs.Most trusts continue to focus on serving theirtraditional catchment areas. However, wehave begun to see signs of a more aggressiveapproach to competition in some areas. Forexample, City Hospitals Sunderland haveestablished some ENT outreach services inCounty Durham, and at one point put in aplanning application (which did not eventuallyproceed) for a new Outpatient Centre in themiddle of Durham City.
We have also witnessed some growth in theamount of business going to independentsector hospitals: the Spire, Washington andBMI Woodlands, in particular.
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 72
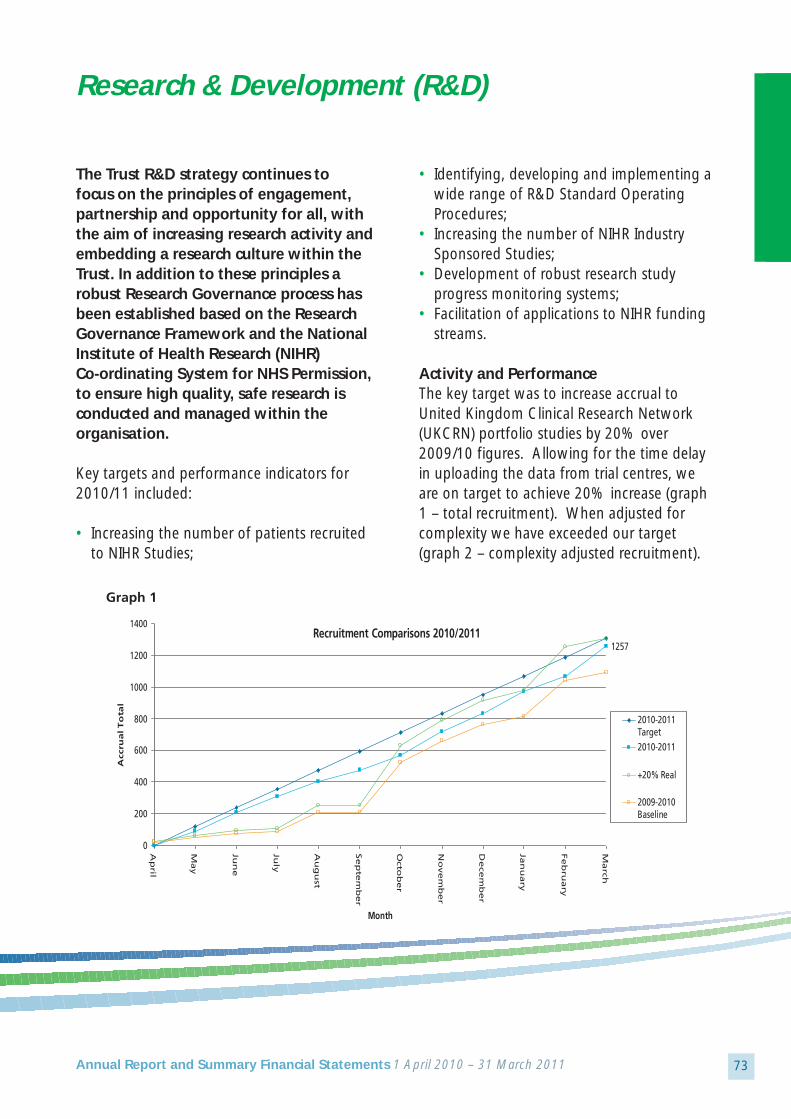
Graph 1
Recruitment Comparisons 2010/20111257
0
200
400
600
800
1000
1200
1400A
pril
Ma
y
Jun
e
July
Au
gu
st
Se
pte
mb
er
Octo
be
r
No
ve
mb
er
De
cem
be
r
Jan
ua
ry
Fe
bru
ary
Ma
rch
Month
Acc
rua
l T
ota
l
2010-2011Target2010-2011
+20% Real
2009-2010Baseline
73Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Trust R&D strategy continues to focus on the principles of engagement,partnership and opportunity for all, withthe aim of increasing research activity andembedding a research culture within theTrust. In addition to these principles arobust Research Governance process hasbeen established based on the ResearchGovernance Framework and the NationalInstitute of Health Research (NIHR) Co-ordinating System for NHS Permission, to ensure high quality, safe research isconducted and managed within theorganisation.
Key targets and performance indicators for2010/11 included:
• Increasing the number of patients recruitedto NIHR Studies;
• Identifying, developing and implementing awide range of R&D Standard OperatingProcedures;
• Increasing the number of NIHR IndustrySponsored Studies;
• Development of robust research studyprogress monitoring systems;
• Facilitation of applications to NIHR fundingstreams.
Activity and PerformanceThe key target was to increase accrual toUnited Kingdom Clinical Research Network(UKCRN) portfolio studies by 20% over2009/10 figures. Allowing for the time delayin uploading the data from trial centres, weare on target to achieve 20% increase (graph1 – total recruitment). When adjusted forcomplexity we have exceeded our target(graph 2 – complexity adjusted recruitment).
Research & Development (R&D)
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 73

74 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
As well as an overall increase in ourrecruitment, there has been an increase in theproportion of interventional accruals from44% to 56%, indicative of an increasedcomplexity weighted portfolio and increasedworkload.
Commercially funded research studies withinthe Trust have in the past been limited.However, working closely with the NIHRIndustry Team and Comprehensive LocalResearch Network Industry Manager, we haveestablished strong links with pharmaceuticalcompanies and commercially funded research.Consequently the number of commerciallyfunded studies is steadily increasing.
Funding and Grants
Comprehensive Local Research Network (CLRN) Funding
Our strong performance in increasing portfoliostudies has been supported by funding fromCounty Durham and Tees ValleyComprehensive Local Research Network, withwhich there has been strong engagement.CLRN support funding for support services(Pharmacy, Radiology and Pathology) andresearch teams has increased year on year inline with the increase in performance and thissupport will continue through 2011/12.
Springboard GrantTo encourage individuals to develop their ownresearch the Trust has offered SpringboardGrants (up to a value of £8k) to allinvestigators who achieve Trust and EthicalCommittee approval. The number of Trustinitiated studies has grown steadily and thisyear we have awarded six Springboard Grants.
Graph 2
2010-11 Complexity Adjusted
0100200300400500600700800900
1000
Ap
ril
Ma
y
Jun
e
July
Au
gu
st
Se
pte
mb
er
Octo
be
r
No
ve
mb
er
De
cem
be
r
Jan
ua
ry
Fe
bru
ary
Ma
rch
2010-11ComplexityAdjusted
2009-10ComplexityAdjusted
09-10ComplexityAdjusted + 20%
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 74

75Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Research FellowshipThe Trust offers Research Fellowships, incollaboration with Durham University, tofacilitate individuals to apply for NIHR grantfunding. These Fellowships comprise fundingfor 1 session per week for one year, to givethe individual time to complete the arduoustask of external grant application. In2010/2011, two research studies, awardedRfPB Grants in 2009/2010, have commencedrecruitment and are meeting their predictedtarget. This year we have awarded threeResearch Fellowships; two projects have beensubmitted and are awaiting final outcome andthe third project is progressing towardssubmission in the summer of 2011.
Research Management and GovernanceThe R&D Team has strengthened themanagement and governance processthroughout the year. The NIHR OperatingGuidelines for gaining NHS Permission havebeen embedded into our governance processfor approving research studies. Working incollaboration with other Trusts in the CountyDurham and Tees Valley CLRN, StandardOperating Procedures have been developedand implemented. We have also adopted theNIHR Research Service Support (RSS) StandardOperating Procedures for SponsorOrganisations and the NPSA NRES EthicsProportionate Review Standard OperatingProcedure. Internal Audit have complimentedR&D on the management of research under the
research governance framework and we haveimplemented their recommendation tostrengthen the risk assessment process ofresearch studies.
As part of our drive to achieve excellence in ourmanagement of Clinical Trials of MedicinalProducts (CTIMPs) we commissioned a MHRAPreparedness Training and Inspection GapAnalysis, which proved invaluable inenlightening R&D Management, Investigators,Research Teams and Support Departmentsabout the expectations of the MHRA Inspectorsas well as identifying areas for development.Our newly appointed Clinical Trials Pharmacistwill be key to achieving the recommendationsby the end of the coming year.
The Trust introduced the ‘Green Bag’ pharmacy scheme to improve safetyand reduce medicines waste when patients are admitted to hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 75

76 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
WorkforceOur ability to deliver the Trust’s vision isdependent on the talent, leadership andcommitment of all our employees, theirmotivation to succeed, and their passionfor delivering excellent services
Our Human Resource and OrganisationalDevelopment Strategy aims to create theconditions in which our staff can support eachother and contribute to the highest qualitypatient care and experience.
The Trust’s approach to organisationaldevelopment remains one of looking at thingsfrom a whole systems approach, developingadaptable and flexible leadership within aculture/climate that supports its core valuesand ensures delivery of strategy through itsstaff. In 2010, there were a number of keythemes and these will continue into 2011.These include:
• Establishing (through staff and stakeholderengagement) and sharing thevision/common purpose;
• Staff engagement and staff advocacy;• Performance management and
development of high performing teams;• Reward and incentivisation;• Values and behaviours; • Leadership development and talent
management;• Service transformation; • Workforce development; and• Climate (work environment).
Trust values and behaviours underpin ourvision and form the basis of a staff compact.In 2010, our values and behaviours were atthe centre of the appraisal and performancemanagement cycle, clearly establishing theeffective behaviours required of our managersand staff. Work will take place in 2011 todevelop a values and behaviours frameworkwhich is representative of the newlyintegrated Trust, with “patient care and highquality services” at the heart of theframework.
The values (will) take into account the rights,pledges, and expectations that our staff canexpect and which are now enshrined in theNHS Constitution.
Our People and Community Involvement
The Trust introduced the Hypobox, a one-stop kit that provides a range ofglucose products for use in cases of hypoglycaemia in people with diabetes
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 76

77Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Our key strategic workforce aims are:
• To ensure we become the best place for ourstaff to work;
• To develop the best ways of working; and• To provide the best leadership.
We remain committed to the provision of ahealthy workplace for our staff, theengagement of staff in all our key decisionsand that communication with all staff ismeaningful, timely, and effective.
The Trust has an excellent track record ofproviding training, education anddevelopment for its entire staff (clinical andnon clinical) as it acknowledges that staff areits greatest asset and key to the delivery ofquality, efficient services. One of the mainways in which we ensure staff have the rightknowledge and skills to fulfil their role isthrough annual Performance andDevelopment Appraisal and the Trust hascommitted to the appraisal of each memberof staff annually. The 2010 Staff Surveyresults show a 32% improvement in annualappraisal since 2009.
Leadership development and talentmanagement is a key priority for the Trust andin 2010 the Trust continued to invest in thedevelopment of leadership and talent (futureleaders and managers) at every level of theTrust. A driving force is the expectation thatthe Trust recruits and retains the best staff inorder that our patients receive the best careand treatment.
The Trust made a concerted effort with staff toreduce the levels of sickness absence resultingin a reduction in these levels from an averageof 4.2% in 2009/2010 to 3.83% in2010/2011.
Equality and DiversityThe Trust is committed to providing the bestservice for patients, to meet individual needsand to be the employer of choice for staff.
In 2008, the Trust Board approved the SingleEquality Scheme, which contains the aims,objectives, and actions agreed with ourstakeholders in order to eliminatediscrimination and promote equality ofopportunity within our service delivery andemployment practices. This Scheme has beena three-year rolling document which has gonebeyond legal compliance to not only ensurehuman rights underpin our work, but also toembrace six areas of equality: age, disability,gender, race, religion/belief and sexualorientation. Our progress on implementingthe Scheme is monitored through our Equality,Diversity and Human Rights Steering Groupthat provides regular assurance to the TrustBoard that we are fulfilling our obligations.
Significant progress has been made in movingthe equality agenda forward in this financialyear.
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 77

78 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Examples include:
• Launch of the NHS Help Card pilot. The NHSHelp Card has been designed to give extrahelp or support to people when they visit ourservices by assisting with some of thecommon problems people face such as,hearing an appointment being called, beingguided where to go, supporting a relative orcarer or understanding the English language;
• In addition, this year we have also put inplace a number of provisions to supportpeople with learning disabilities. An acuteliaison nurse has been appointed to assisthospital staff to understand issues and putin place adjustments for patients withlearning disabilities, as well as support theimplementation of the hospital passport;
• We also have a number of employmentpolicies in place to ensure fairness andequality for staff, such as the Equality andDiversity (Equal Opportunities) Policy,Disability Policy, Religious Observance Policyand so on which have been updated toreflect changes in the law following theEquality Act 2010; and
• Equality impact assessments have continuedto be undertaken throughout the Trust onpolicies, procedures, services, functions andorganisational changes and the requirementto undertake these now forms the basis ofstandardised processes so that any potentialfor discrimination or any unintendedbarriers can be removed or mitigated at theearliest opportunity.
Over the next 12 months, the Trust willdevelop a new Equality Strategy to replace itscurrent Single Equality Scheme todemonstrate how we will meet the newgeneral public sector duties under the EqualityAct 2010 and the requirements of the NHSEquality Delivery System, which is theperformance management framework beingintroduced by the Department of Health in2011.
We will engage with our workforce and ourlocal community to develop our equalityobjectives ready for 2012 to focus ourpriorities based on feedback from those whoprovide and use our services. In addition, tomeet the requirements of the specific duties ofthe Equality Act, the Trust will put processes inplace to improve the quality of the equalitydata held on staff and service users tofacilitate more effective monitoring of thisinformation.
In order to measure how well we areachieving our aims, the Trust reports the fulldetails of our progress in the Equality, Diversityand Human Rights Annual Report which alsoprovides information on the equalitymonitoring which has been undertaken onour workforce and employment practices. Acomparison of this year and the previousyear’s equality monitoring of the Trust’s profilewith regard to age, ethnicity, gender anddisability is set out in table 03 below:
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 78

79Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Table 03 – Staff Equality & Diversity
Age 2009/10 Staff % 2010/11 Staff %<25 225 4.6% 226 4.16%25-34 976 17.5% 931 17.13%35-44 1484 26.7% 1,411 25.97%45-49 1000 17.9% 958 17.63%50-54 889 15.9% 921 16.95%55-56 267 4.8% 299 5.50%57-58 235 4.2% 221 4.07%59-59 112 2% 112 2.06%60+ 349 6.3% 355 6.53%
Ethnic Origin
White - British 4854 86.94% 4756 87.52%White - Irish 25 0.45% 24 0.44%White - Any other White background 58 1.04% 54 0.99%White Scottish 1 0.02% 1 0.02%White Cypriot (non specific) 1 0.02% 1 0.02%White Greek 0 0 1 0.02%White Polish 1 0.02% 3 0.06%White Other European 1 0.02% 1 0.02%Mixed - White & Black Caribbean 2 0.04% 2 0.04%Mixed - White & Black African 2 0.04% 2 0.04%Mixed - White & Asian 3 0.05% 3 0.06%Mixed - Any other mixed background 4 0.07% 8 0.15%Asian or Asian British - Indian 139 2.49% 140 2.58%Asian or Asian British - Pakistani 27 0.48% 24 0.44%Asian or Asian British - Bangladeshi 2 0.04% 6 0.11%Asian or Asian British - Any other Asian background 35 0.63% 33 0.61%Asian British 0 0 10 0.18%Black or Black British - Caribbean 3 0.05% 1 0.02%Black or Black British - African 16 0.29% 22 0.40%Black or Black British - Any other Black background 4 0.07% 4 0.07%Black Nigerian 2 0.04% 1 0.02%Black Unspecified 1 0.02% 1 0.02%Chinese 10 0.18% 15 0.28%Any Other Ethnic Group 26 0.48% 26 0.48%Filipino 1 0.02% 1 0.02%Not Stated 365 6.54% 294 5.41%
Gender
Male 1043 18.68% 964 17.74%Female 4540 81.32% 4470 82.26%Transgender 0 0 0 0
Disability
Yes 68 1.22% 64 1.18%No 0 0 196 3.61%Not stated 0 0 5174 95.22%
The new integrated Trust will provide opportunities to improve how we meet the individual needs of vulnerable minoritygroups within our community, by providing joined up pathways of care between hospital-based care and that within thecommunity. It will also enable us to focus on prevention through addressing known health inequalities throughoutCounty Durham and Darlington.
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 79

80 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The new integrated Trust will provideopportunities to improve how we meet theindividual needs of vulnerable minority groupswithin our community, by providing joined uppathways of care between hospital-based careand that within the community. It will alsoenable us to focus on prevention through
addressing known health inequalitiesthroughout County Durham and Darlington. Equality and Diversity of Public Members
The Trust also records the following dataregarding equality and diversity of its publicmembership:
* Total population of catchment area** Population aged 16-74 in catchment area
Population includes the areas Gateshead,South Tyneside, Sunderland, Hartlepool,Middlesbrough, Redcar and Cleveland,Stockton-on-Tees, Darlington, Chester-le-
Street, Derwentside, Durham, Easington,Sedgefield, Teesdale, Wear Valley, Hambleton,RichmondshireSource: Office for National Statistics
Public constituency Last year (2010/2011) Eligible Population*
As at start (April 1) xNew Members 1,330Members leaving xAt year end (March 31) 7,340 1,888,178Public constituency Number of members Eligible Population*Age(years):0 - 16 115 404,86817 - 21 317 120,49122+ 6,737 1,362,818Ethnicity:White 7,111 1,851,205Mixed 61 8,678Asian 50 20,109Black 8 2,540Other 24 5,649Socio-economic groupings**:ABC1 3,618 624,069C2 2,657 250,003D 248 305,236E 685 295,429Gender analysis:Male 2,981 917,184Female 4,345 970,994
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 80

81Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Staff SurveyThe 2010 Staff Survey was structuredaround the four Staff Pledges within the NHS Constitution with two additionalthemes of Equality and Diversity andStaff Satisfaction.
The 4 Pledges shaped questions around:
Pledge 1 roles, responsibilities andrewarding jobs;
Pledge 2 personal development, access totraining and development andsupport from line managers;
Pledge 3 maintaining health and wellbeingand safety; and
Pledge 4 engaging staff in decisions thataffect them.
In 2010, four hundred and forty seven Truststaff members participated in the survey. Thisis a response rate of 55%, which is aboveaverage for acute trusts in England, comparedwith a response rate of 60% in the Trust inthe 2009 survey.
Table 04 provides a summary of performancefollowing the results of the 2010 Staff Surveyhighlighting the areas where the Trustperformed well and the areas where the Trustwill be working on in the year to come. Thesefindings, which have been considered in
conjunction with the results of theCommunity Health Services’ Staff Survey, willform the basis of the 2011 Integrated StaffSurvey Action Plan which has been developedjointly by management and staff siderepresentatives.
Last year, the Trust action planned aroundissues key to the development of theorganisation throughout 2009/2010. TheTrust developed an Action Plan aroundimproving three key areas, namely improvingthe take up of Appraisal and PersonalDevelopment Planning and Equality andDiversity training and improving levels of staffengagement. Worthy of note is thestatistically significant improvements inAppraisal and Personal Development Planninguptake (+ 31%) and Equality and Diversitytraining (+ 18%).
The response rate for staff engagement,however, deteriorated slightly. There are threedimensions to staff engagement which, whencombined, determine the weighting for staffengagement as a whole. These are:
• Staff ability to contribute towardsimprovements at work – Trust score 58%(national average 62%). Substantial efforthas been made to engage staff in a numberof ways; including large scale corporate anddivisional events to identify qualityimprovements at the front line branded asthe “Quality Challenge”, communication
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 81

82 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
and discussion events around the“Transforming Community Services”agenda and road shows where staff canmeet and debate issues with members ofthe Executive Team;
• Staff recommending the Trust as a place towork or receive treatment – Trust score 3.26– (national average for acute trusts was3.52); and
• Staff motivation at work – Trust score 3.78(higher score better) – (national average3.83).
Staff engagement is key to the success of theorganisation and 2011 will see the furtherdevelopment and establishment ofinterventions to strengthen staff engagementand improve staff feedback. The interventionshighlighted below are corporate interventionsbut all leaders and managers are required todevelop local arrangements for ensuring staffare involved in decisions that affect servicesand working arrangements.
The Staff Engagement Plan for 2011 is alreadybeing developed and a number of events arealready planned for 2011 including:
• Quarterly Executive road shows are plannedthroughout the year across acute andcommunity premises, providing anopportunity for staff to meet the ExecutiveTeam, to be kept up to date and to allowstaff to provide feedback on mattersimportant to them and their patients andcolleagues;
• Quality Challenge team events are plannedto engage staff in the development of thenewly integrated Trust’s Values andBehaviours and to shape the new corporatebranding and logo. Separate events are alsoplanned to consider the 2010 Staff Surveyresults and to seek feedback on what stafffeel will make the Trust an even better placeto work;
• The Quality Challenge website will befurther developed and staff can continue topost quality ideas and be engaged inimplementing ideas that are taken forwardthroughout the year;
• Staff engagement is key to the“Transforming Clinical Services” Strategyand a number of staff and stakeholderevents will be held throughout the year; and
• The Chief Executive Blog is a regular staffcommunication which allows staff tofeedback via a dedicated web link. Staffreceive a response from the Chief Executiveon any matters they raise.
The Eales family make a generous donation toward 51 at Darlington Memorial Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 82

83Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
2009/10 2010/11 Trust Improvement/Deterioration
Response Rate % Trust National Trust NationalAverage Average
60% 55% 55% 54%
Table 04 – Staff Survey Results
2009/10 2010/11 Trust Improvement/Deterioration
Response Rate % Trust National Trust NationalAverage Average
Experiencing physical 10% 11% 4% 8% Improvementviolence from patients, relatives, public
Appraised in the previous 59% 70% 90% 78% Improved from 59% in12 months 2009 when CDDFT was
ranked in bottom 4 of acute trusts
Appraised with PDP in 52% 59% 82% 66% Improvementthe previous 12 months
Impact of health & 1.50 1.57 1.48 1.57 Improvement as lower wellbeing on ability score is betterto perform work/daily activities
2010 Top 4 Ranking
A new £5.5 million intensive therapy unitopened at Darlington Memorial Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 83
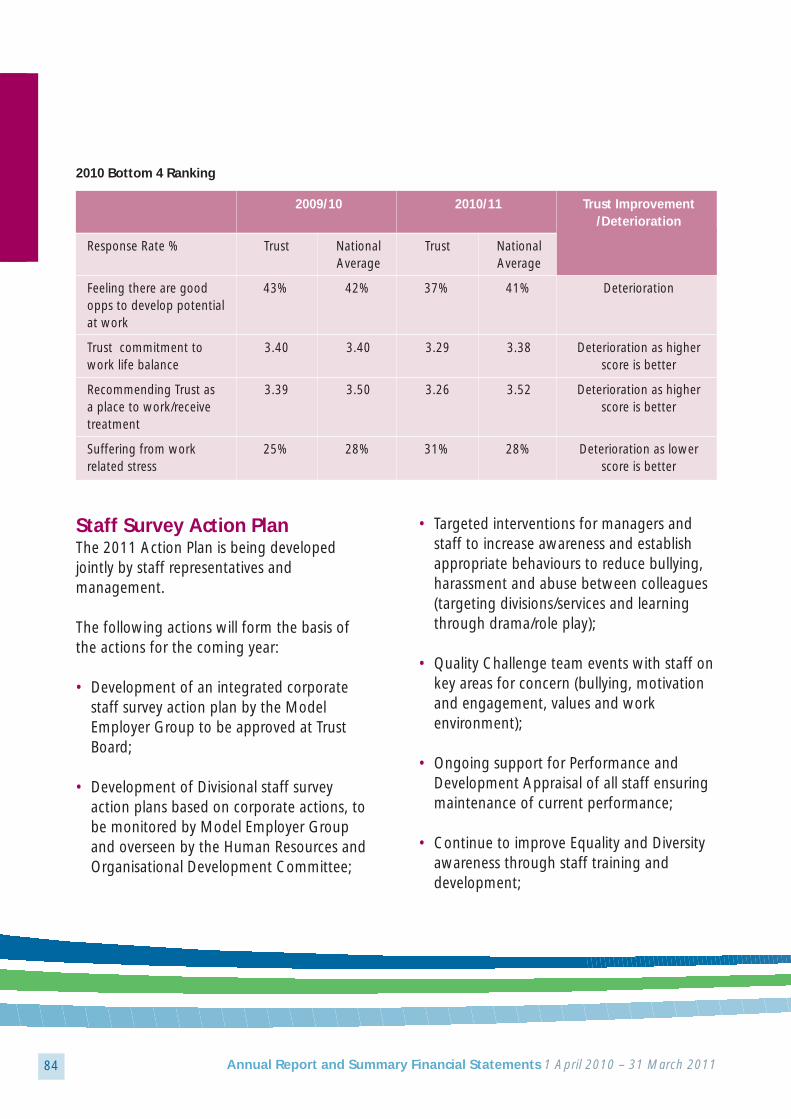
84 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
2009/10 2010/11 Trust Improvement/Deterioration
Response Rate % Trust National Trust NationalAverage Average
Feeling there are good 43% 42% 37% 41% Deteriorationopps to develop potential at work
Trust commitment to 3.40 3.40 3.29 3.38 Deterioration as higherwork life balance score is better
Recommending Trust as 3.39 3.50 3.26 3.52 Deterioration as highera place to work/receive score is bettertreatment
Suffering from work 25% 28% 31% 28% Deterioration as lowerrelated stress score is better
2010 Bottom 4 Ranking
Staff Survey Action PlanThe 2011 Action Plan is being developedjointly by staff representatives andmanagement.
The following actions will form the basis ofthe actions for the coming year:
• Development of an integrated corporatestaff survey action plan by the ModelEmployer Group to be approved at TrustBoard;
• Development of Divisional staff surveyaction plans based on corporate actions, tobe monitored by Model Employer Groupand overseen by the Human Resources andOrganisational Development Committee;
• Targeted interventions for managers andstaff to increase awareness and establishappropriate behaviours to reduce bullying,harassment and abuse between colleagues(targeting divisions/services and learningthrough drama/role play);
• Quality Challenge team events with staff onkey areas for concern (bullying, motivationand engagement, values and workenvironment);
• Ongoing support for Performance andDevelopment Appraisal of all staff ensuringmaintenance of current performance;
• Continue to improve Equality and Diversityawareness through staff training anddevelopment;
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 84

85Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• Development and establishment of newvalues and behaviours and subsequent staffcompact;
• Strengthen and improve team briefing andlocal cascade/feedback arrangements; and
• Executive and “Transforming ClinicalServices” road shows.
Health and Safety PerformanceThe Trust’s staff incident/accident reportingprocess has indicated a decrease from 940 in2009/2010 to 861 in 2010/2011. All staffincidents are investigated thoroughly withappropriate actions taken.
The Trust has continued to audit departmentsto review health and safety awareness againstcompliance with the Local SafetyDocumentation. The Trust’s Health and Safetyand Security Committees have continued tobe proactive in reviewing incident trends andmonitoring compliance against best practice.
There have been 2 Health and SafetyExecutive (HSE) visits over the last 12 months,one in relation to Latex use and the other inrelation to the Trust’s Category 3 room inPathology. Following the visits, action plansfor both areas were put into place as follows:
• The objective is to reduce the use of Latexgloves and replace with non Latex productsover the next 12 months. Actions arisingfrom the visit are being progressed and theTrust Latex Policy has been updated; and
• The Category 3 room actions have beencompleted.
There has been no enforcement orimprovement notices issued following the 2visits.
Training is fundamental to health and safetyperformance and 81% of staff have receivedhealth and safety training as reported in thelatest Staff Survey for 2010.
Social Responsibility and SustainabilityThe Trust acknowledges our corporate socialresponsibility to consider the environmentalimplications of our business strategy. With agrowing global population and ever increasinglevels of consumption, these environmentalimpacts are widely known and need to beaddressed in order to provide a sustainablefuture. In recognition of these economic,social and environmental pressures, the Trusthas convened a Sustainability Steering Groupto establish and implement ways ofneutralising our environmental impact.
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 85

86 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Sustainability Steering Group, supportedby the Director of Estates and Facilities,manages the Trust’s strategic approach to theenvironment. The group consists of managersfrom energy, waste, transport, finance,procurement, corporate management andhuman resources.
In 2008 and in recognition of the Trust’senvironmental responsibilities, the Trust Boardcommitted the Trust to a target of 15%carbon reduction from the 2007 verified levelsby 2014. This involved an extensiveconsultation process with the Carbon Trustwith the verified baseline being calculated forenergy, waste and transport. The strategy aimsto reduce our carbon footprint by investmentin new technology and minimising waste andtransport carbon emissions.
In 2010/11 the Trust has continued itsinvestment in the £26m infrastructure projectwhich will provide combined heat and powerplant, generating both heating and electricitytogether with de-steaming, at DarlingtonMemorial Hospital. This project will play amajor role in the overall carbon reductioncommitment of the Trust.
The Sustainability Steering Group and CarbonManagement Programme are part of theoverall objective of the Trust to achieve anenhanced score in the Good CorporateCitizenship benchmarking tool for socialresponsibility, with suggested targets of‘Getting Started’ by 2012, ‘Getting There’ by 2015 and ‘Excellent’ by 2020.
WRVS volunteer Alan Klottrup officially opened the new monitoring bay andresuscitation facilities in the A&E department at University Hospital of North Durham
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 86

87Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Area Non Financial data 2010/11
Wasteminimisationandmanagement
Finite Resources
1,935t
Landfill, Recycling,Incineration,Alternative Treatment
263,539 m3
73,254 Gj
198,372 Gj
2,537 Gj
Financial data (£k)2009/10
£472,354
£378,989
£3,461,738
Expenditureon wastedisposal
Water
Electricity
Gas
Oil
Financial data (£k)2010/11
Non-financialdata 2009/10
Absolute valuesfor total amountof wasteproduced by the Trust
Methods ofdisposal
Water
Electricity
Gas
Oil
£493,328
£376,297.27
£2,921,866.94
1,934t
Landfill, Recycling,Incineration,Alternative Treatment
246361 m3
84927.44GJ
181567.48GJ
1602.09GJ
Finite ResourceEmissions T/CO2
Finance LeasedVehicleEmissions
9228.34 T/CO2
8232.17 T/CO2
190.27 T/CO2
Electricity
Gas
Oil
12668.34 T/CO2
9582.72 T/CO2
120.15 T/CO2
97.16 T/CO2
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 87

88 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Formal ConsultationsAlthough there have been no formal publicconsultation exercises carried out during theyear, in 2010/11, scrutiny was concluded onimplementation of the Seizing the Futureprogramme.
Seizing the Future was a clinically led servicereview which led to a series of importantchanges to ensure the safety and sustainabilityof services.
As a result of these changes, acute hospitalservices are now concentrated at DarlingtonMemorial Hospital and the UHND. BishopAuckland Hospital has a key strategic role as acentre for planned care for patients across theTrust’s catchment area.
The Trust, the health scrutiny committees andthe local involvement networks for CountyDurham and for Darlington were representedon an “Oversight Board” monitoringimplementation to ensure that it was carriedout in line with the consulted position anddelivered the intended improvements inclinical services.
The Oversight Board was chaired by ourcommissioners, NHS County Durham andDarlington. To mark the conclusion ofimplementation, a full report has beenpublished on the Seizing the Future process,including learning for similar work in thefuture. The report is available atwww.seizingthefuture.org.uk.
During the year, the Trust’s stroke team hasworked with NHS County Durham andDarlington on a commissioner-led review ofacute stroke services. Since Seizing theFuture, these services have been provided atDarlington Memorial Hospital and at UHND.There is broad consensus that these servicesshould be provided on a single site and thecommissioner plans to consult on its preferredoption, of a single site at UHND, during2011/12.
Partners and StakeholdersThe Trust continues to work closely withpartners in health and social care to improvelocal health services.
During 2010/11, the Trust has worked withNHS County Durham and Darlington on theintegration of our acute services withcommunity health services provided by thecommissioner, under the TransformingCommunity Services national policy guidancefor separating commissioning and providerfunctions.
The Trust was identified as preferredmanagement partner following an assessmentin May, and began a full due diligence processwhich has run through into 2011/12.
On 1 April 2011, County Durham andDarlington Community Health Services andCounty Durham and Darlington NHSFoundation Trust became one organisation.
The formal assessment of the integration byMonitor, the independent regulator for
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 88

89Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
foundation trusts, was completed after theyear end. This was as a result of Monitor’sworkload pressures in assessing all theapplications nationally, and not due to anyissues relating to the business case.
NHS County Durham and Darlington workedclosely with the Trust in agreeing interimarrangements which enabled the TUPEtransfer of staff to proceed on 1 April.
An acute and community foundation trust forCounty Durham and Darlington will improvethe co-ordination of healthcare betweenhospital and community health services,working closely with primary care and socialcare.
Engagement with partners has been achievedthrough a Transforming Community ServicesStrategic Partnership Board, chaired by PatKeane, Joint Chief Executive of NHS County
Durham and Darlington and Trust ChiefExecutive Stephen Eames. Membershipincludes representatives from the six local GPpathfinder consortia localities and localauthorities.
A joint workforce forum included trade unionrepresentation from both the Trust andcommunity services.
During 2010/11, the Trust also held twostakeholder events to discuss future clinicalstrategy for the integrated organisation. The Clinical Strategy will be published in2011/12.
We maintain close relationships with localtrusts in order to ensure the delivery of a widerange of specialist services as locally aspossible. This includes contracts with:
• South Tees Hospitals NHS Foundation Trustfor outpatient services at Bishop Aucklandand Darlington Memorial Hospitals inspecialties we do not provide, such asneurology and areas of oncology; andconsultant capacity to enable us to run ourown urology and oral surgery services atDarlington Memorial Hospital;
• Newcastle upon Tyne Hospitals NHSFoundation Trust for consultant capacity to deliver a neurology service in NorthDurham. We are also working withNewcastle to ensure continued localprovision of haematology and immunologyservices;Dr Richard Hardern, A&E consultant has developed a 'Wilderness Medicine'
course for medical students at Newcastle University
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 89

90 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• South Tyneside NHS Foundation Trust andCity Hospitals Sunderland NHS FoundationTrust for the provision of nursing andadministrative services to support our sub-regional Dermatology and Plastics servicesand for our support to Sunderland’s urologyservice at Bishop Auckland and UHND;
• Lodestone, an independent provider, fortheir provision of scanning facilities on oursites at Darlington and Bishop Auckland;and
• Tees Esk and Wear Valley NHS FoundationTrust (mental health) for the provision ofmental health services to us and acuteassessment and diagnostics services tothem.
We also have significant on-goingrelationships with private providers of healthcare to undertake elective work for us, toassist us to continue to achieve the 18 weekreferral to treatment (RTT) target, particularlyin orthopaedics.
During 2010/12 the Trust established closerlinks with the Great North Children's Hospital,part of Newcastle upon Tyne Hospitals NHSFoundation Trust;
For many years the Trust has worked in closecollaboration with colleagues at Newcastle. Inpaediatrics, patients sometimes need to bereferred to specialist centres for care andtreatment. By strengthening our links with theGreat North Children’s Hospital, the regional
Dr Julie Cox, Consultant Radiologist is leading a pioneering trial into the treatment of breast cancer
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 90

91Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
specialist centre for paediatrics, the Trust canbring that expertise to patients in CountyDurham and Darlington and provide the bestpossible care for children as locally as possible;
Consultants from the Great North Children’sHospital hold specialist clinics at DarlingtonMemorial Hospital and UHND and consultantsfrom Durham and Darlington work part timeat the Great North Children's Hospital todevelop their special interests;
Children in need of specialist care benefit fromreferral to the Great North Children's Hospitalfrom Durham and Darlington and there willalso be collaboration between the Great NorthChildren's Hospital and community paediatricservices in Chester-le-Street and Stanley; and
The Trust continues to be a member of theDurham Dales Integrated Care Organisationwhich includes major statutory and voluntaryproviders of health and social care in the Dales,and other stakeholders and aims to addressdeterminants of health, including fuel povertyand rural transport, as well as improving accessto services such as urgent care.
We have also been involved in a Collaborativein Darlington with the PCT, DarlingtonBorough Council and Tees Esk and WearValley Trust (mental health) to improve servicesfor patients with dementia which has receivednational attention.
Three of the Trust’s hospitals, and the non-clinical support services within them, areprovided by private sector consortia underPrivate Finance Initiative (PFI) arrangements.
The details of these arrangements are summarised in the table below:
Hospital Bishop AucklandGeneral Hospital
Operator
Capital Value
Financial Close
Operational Date
Termination Date
2010/11 fee
Indexation
Consort
£114m
March 1998
April 2001
March 2028
£19.074m
Various
Criterion
£49m
May 1999
June 2002
June 2032
£11.773m
RPI
UHND Chester-le-StreetGeneral Hospital
Robertson Health
£10m
May 2002
October 2003
May 2032
£2.489m
RPI
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 91

92 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Board is responsible for exercising all ofthe powers of the Trust and is the body thatsets the strategic direction, allocates the Trust’sresources and monitors its performance.
The Board is made up of five executivedirectors, five non executive directors and anon-executive chairman. The Chairman andNon-Executive Directors are appointed by theRemuneration and Nomination Committee ofthe Governing Council for varying terms notexceeding 3 years. All of the Non-Executive
Directors are considered to be independent.The Executive Directors are appointed by theNominations Committee of the Board onpermanent contracts. The appointments ofNon-Executive Directors may be terminatedfor a number of reasons set out within theTrust’s constitution and within their terms ofappointment. The composition of the Boardfor the year of report is set out in table 05below which also includes details ofbackground, committee membership andattendance.
Board of Directors
2/2
1/1
2/2
4/4
1/1
4/49/9
14/14
6/6
14/14
Previous board level positions in industryincluding positions as Chairman, ManagingDirector and Finance Director. Previously theChairman of County Durham and TeesValley Strategic Health Authority.
Retired schoolteacher. Previously a Non-Executive Director of the County Durhamand Darlington Acute Hospitals NHS Trustand its predecessor Trust.
Fellow of the Institute of CharteredAccountants of England and Wales.Previously a Non-Executive director of theCounty Durham and Darlington AcuteHospitals NHS Trust.
Tony Waites,Trust ChairmanAppointed 1/2/2007Re-Appointed 1/2/2010until 28/2/2013
Tony Wolfe, Vice-Chairman and NonExecutive DirectorAppointed 1/2/2007 until13/10/2010
Kathryn Larkin-Bramley,Vice Chairman, NonExecutive Director andAudit Committee ChairAppointed 1/2/2008Reappointed 1/8/2010until 31/7/2012
Name and Position Background Trus
t Bo
ard
Aud
itCo
mm
itte
e
Nom
inat
ions
&
Rem
uner
atio
nCo
mm
itte
e
Join
t Bo
ard
Gov
erno
rsm
eeti
ngs
Table 05: The Board of Directors 2010/2011
N/A
N/A
Trust Board Meeting Attendance
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 92

93Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Paul Stewart,Non Executive Director,Senior IndependentDirector Appointed1/2/2007 until 30/06/2010.
The Right Hon Baroness Armstrong Non-Executive Director,Senior IndependentDirectorAppointed 1/10/2010 until 30/9/2011
Andrew YoungNon- Executive DirectorAppointed 1/7/2010 until30/6/2013
Dr Robert MichaelWaterstonNon- Executive Director Appointed 1/2/2007 Reappointed 1/6/2010 until 31/5/2013
Dr Ian RobsonNon- Executive Director Appointed 1/6/2007 Reappointed 1/6/2010until 31/5/2013
Stephen EamesChief Executive
Commercial litigation partner in a majorNewcastle law firm. Previously a Non-Executive Director of the County Durhamand Darlington Acute Hospitals NHS Trust.
Member of the House of Lords and PrivyCouncil and a Board member of severalcharitable organisations. FormerParliamentary Secretary to the Treasury and Government Chief Whip, Chancellor of the Duchy of Lancaster and Minister for the Cabinet Office and Social Exclusion,Minister of State at the Dept ofEnvironment, Transport & the Regions.
Former Chief Executive of Durham andChester-le-Street and Durham Dales PCTs.Former Director of Commissioning andDeputy Chief Executive of County Durhamand Darlington Health Authority.
Owner and Managing Director of ITconsultancy. Previously a Non-Executivedirector of the County Durham andDarlington Acute Hospitals NHS Trust.
Independent consultant with board levelexperience in sales, marketing and businessdevelopment in healthcare, utilities andenvironmental services.
Extensive experience as an NHS ChiefExecutive. Member of European Mentoring& Coaching Council, the Society forOrganisational Learning, and the EuropeanHealth Management Association.
4/4
8/8
6/10
13/14
13/14
14/14
2/3
9/12
4/5
8/9
N/A
N/A
1/1
3/3
2/3
4/4
3/4
N/A
1/1
1/1
0/1
1/2
2/2
2/2
N/A
N/A
N/A N/A
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 93
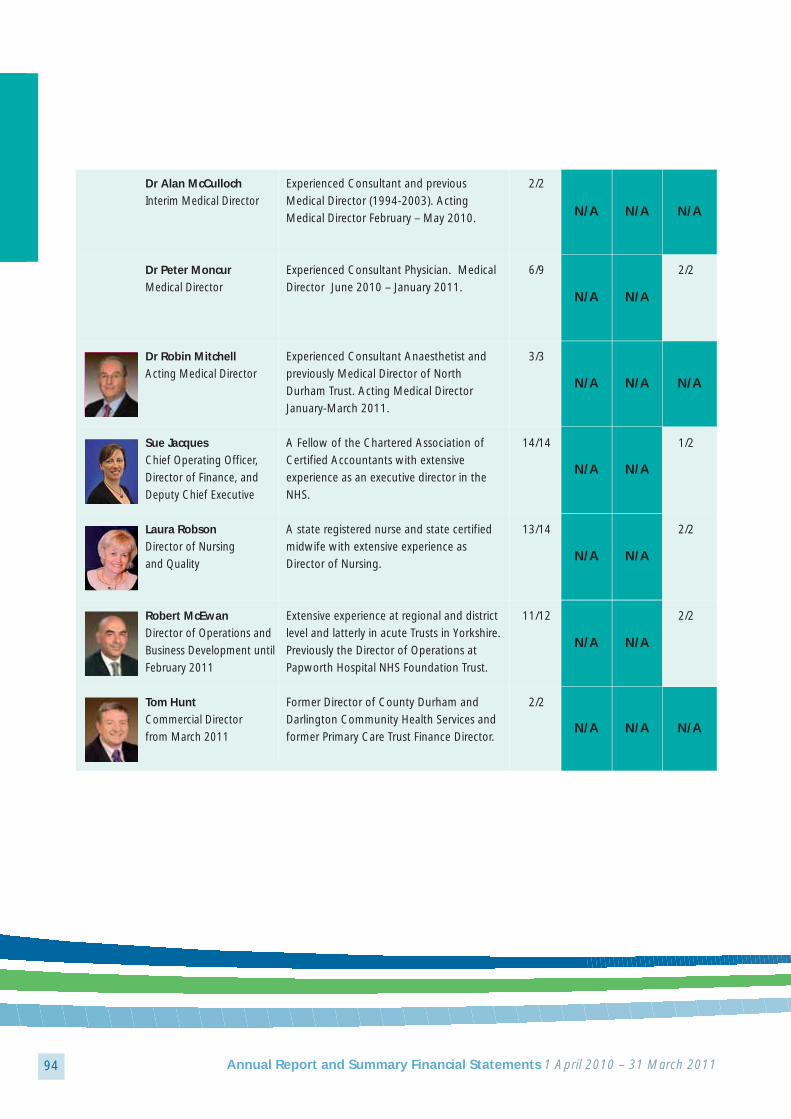
94 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Dr Alan McCullochInterim Medical Director
Dr Peter Moncur Medical Director
Dr Robin MitchellActing Medical Director
Sue JacquesChief Operating Officer,Director of Finance, andDeputy Chief Executive
Laura RobsonDirector of Nursing and Quality
Robert McEwanDirector of Operations andBusiness Development untilFebruary 2011
Tom HuntCommercial Director from March 2011
Experienced Consultant and previousMedical Director (1994-2003). ActingMedical Director February – May 2010.
Experienced Consultant Physician. MedicalDirector June 2010 – January 2011.
Experienced Consultant Anaesthetist andpreviously Medical Director of NorthDurham Trust. Acting Medical DirectorJanuary-March 2011.
A Fellow of the Chartered Association ofCertified Accountants with extensiveexperience as an executive director in theNHS.
A state registered nurse and state certifiedmidwife with extensive experience asDirector of Nursing.
Extensive experience at regional and districtlevel and latterly in acute Trusts in Yorkshire.Previously the Director of Operations atPapworth Hospital NHS Foundation Trust.
Former Director of County Durham andDarlington Community Health Services andformer Primary Care Trust Finance Director.
2/2
6/9
3/3
14/14
13/14
11/12
2/2
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
2/2
N/A
1/2
2/2
2/2
N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A N/A
N/A
N/A N/A N/A
N/A N/A N/A
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 94

95Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Board may delegate any of its powers to acommittee of Directors or to an ExecutiveDirector and these matters are set out in theScheme of Decisions Reserved to the Boardand the Scheme of Delegation. Decisionmaking for the operational running of theTrust is delegated to the ExecutiveManagement Group.
The Board has an annual schedule of businesswhich ensures that it focuses on itsresponsibilities and the long term strategicdirection of the Trust. It meets no less than tentimes per year to conduct its business andBoard members also attend seminars andtraining events throughout the year.
Each year the Board holds an event to evaluateits performance and that of its committees.The performance of the Non-ExecutiveDirectors and the Chairman is conducted bythe Chairman and the Nomination andRemuneration Committee of the GoverningCouncil respectively. The Senior IndependentDirector leads the Committee in this process.The performance of the Executive Directors isappraised by the Chief Executive whose ownperformance is, in turn, appraised by theChairman. As a consequence of theassessment of collective and individualperformance, the Board considers that it hasthe appropriate balance and completeness inits membership to meet the requirements ofan NHS foundation trust.
A register is maintained of the businessinterests of directors which may conflict with
their responsibilities as managers of the Trust.This register is available for inspection by thepublic and anyone who wishes to inspect itshould make an appointment to do so bycontacting the Trust Secretary, County Durhamand Darlington NHS Foundation Trust,Darlington Memorial Hospital, Hollyhurst Road,Darlington, DL3 6HX or by e-mailing:[email protected].
Audit CommitteeThe Audit Committee is comprised of threeNon-Executive Directors and is chaired byKathryn Larkin-Bramley, a charteredaccountant.
The committee is responsible for providing theBoard with advice and recommendations onmatters which include the effectiveness of theframework of controls in the Trust, theadequacy of the arrangements for managingrisk and how they are implemented, theadequacy of the plans of the Trust’s auditorsand how they perform against them, theimpact of changes in accounting policy andthe Committee’s review of the annualaccounts.
The committee met on eight occasions duringthe year with the Chief Operating Officer andDirector of Finance, other Trust officers and theTrust’s auditors in attendance. The attendanceof members is shown in table 05 above.
In order to ensure that the independence andobjectivity of the auditor is not compromisedby providing the Trust with additional non
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 95

96 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
audit services, the Trust has agreed a policythat requires the Audit Committee (underdelegated authority from the GoverningCouncil) to approve the arrangements for allproposals to engage the auditors on non auditwork. The auditors themselves comply withthe standards of the Auditing Practises Boardin this matter.
The duty to appoint the auditors lies with theGoverning Council. A committee of theGoverning Council, supported by Trust officers,was established to oversee the procurement ofexternal audit services and make arecommendation to the council. Theprocurement was taken forward in accordancewith the appropriate regulations for publicsector procurement and Deloitte ToucheTohmatsu was appointed as the Trust’sauditors with effect from 1 April 2009 for a 3year period.
RemunerationThe Trust has two remuneration andnomination committees: a committee of theBoard and a committee of the GoverningCouncil.
The committee of the Board deals with theappointment and remuneration of the ChiefExecutive and the Executive Directors. It ischaired by the Trust’s Chairman and all of theNon-Executive Directors are members.Members’ attendance at meetings of thecommittee is shown in table 05 above. TheChief Executive attends the committee exceptwhen it is dealing with matters concerning him.
The committee reviews the salary levels of theChief Executive and the Executive Directors atannual intervals. In doing so, it takes accountof the overall performance of the Trust, theperformance of individual directors, the awardsto other staff groups, the prevailing rate ofawards in other similar organisations andpublished benchmark information such as theIDS NHS Boardroom Pay Report. However,none of the remuneration is directly related toperformance.
All of the Executive Directors, with theexception of the Medical Director, areappointed on permanent contracts with anotice period of six months. The MedicalDirector is appointed for a term of five years.
The contracts of employment make no specialprovisions regarding early termination ortermination payments. Terminations resultingfrom redundancy and retirement are inaccordance with the provisions of nationalterms and conditions and the NHS PensionScheme.
Details of Directors’ remuneration and the cashequivalent transfer values of the pensions ofthe Executive Directors can be found on pages141 to 142.
The committee of the Governing Council deals with the appointment and remunerationof the Trust Chairman and Non-ExecutiveDirectors and makes recommendations to the Governing Council as appropriate. The committee also has a role in the annualappraisal of the Trust Chairman’s performance,
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 96
97Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
a process in which committee members are ledby the Senior Independent Director.
The committee reviewed the levels ofremuneration and agreed, as in the previousyear, to uplift them at an equivalent level tothe recommendations of the NHS pay reviewbodies. This offer was, however, not taken upby the Trust Chairman and the Non-ExecutiveDirectors. The committee also dealt with there-appointment of the Trust Chairman and theappointment/re-appointment of the Non-Executive Directors during the year.
Stephen EamesChief Executive
The NHS Foundation Trust Code of GovernanceThe NHS Foundation Trust Code ofGovernance (Code) is published byMonitor. It is based on the CombinedCode on Corporate Governance and itspurpose is to further the development ofcorporate governance in individualfoundation trusts by making governors anddirectors aware of the principles of goodgovernance and how to develop bestpractise in their application.
The Board ensures compliance with theCode through the arrangements it puts inplace for its governance structures, policiesand processes and how it keeps themunder review. These arrangements are setout in documents that include:
• The constitution;• Standing orders;• Standing financial instructions;• Schemes of delegation and decisions
reserved to the Board;• Terms of reference of Board and
Governing Council committees; and• Codes of conduct.
The Directors consider that the Trustcomplies with the provisions of the Codewith the exception of the requirement tohave arrangements in place to resolvedisputes between the Board and theGoverning Council. These arrangementsare being drawn up.
A new coffee and snack bar opened as part of the award winningcatering services at Darlington memorial Hospital
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 97

98 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Governing Council is comprised ofthirty-seven governors who represent theTrust’s public and staff constituencies andthose stakeholder organisations who areentitled to appoint governors under theterms of the Trust’s constitution. For2011/12 the number of staff governorswill increase by two to reflect the increasein the number of staff working within theTrust following the integration ofcommunity services.
The Governing Council has a number ofstatutory duties, including the appointmentand removal of the Chairman and Non-Executive Directors, the appointment of theTrust’s auditors and the approval of changesto the constitution of the Trust. They also holdto account the Board for its management ofthe Trust. The Trust values the contribution ofits Governors and the particular perspectivesthat they bring to the development ofservices. Consequently, the Governors are
active in developing the Trust’s strategies and its Annual Plan.
The Governing Council has strong workinglinks with the Board. A joint meeting with theBoard is held twice a year and board membersattend relevant Governing Council committeesand participate in joint seminars. Similarly,elected governors are fully engaged in thedifferent working groups established by theBoard. The Board considers that thesearrangements are an effective way tounderstand the views of the GoverningCouncil and maintain engagement with itsmembers.
Governors from the public and staffconstituencies are elected to office for varyingterms up to three years and may seek electionfor further terms up to a maximum of three.Elections were held in seven constituenciesduring the year as shown in table 06.
Governing Council
Table 06 - The details of these arrangements are summarised in the table below:
Date of election Constituencies involved Turnout (%)
04-Jun-2010 Public – Sedgefield No nominations
13-Aug-2010 Staff – Medical Elected unopposed
15-Dec-2010 Staff – Nursing & Midwifery Elected unopposed
15-Dec-2010 Public – Derwentside Elected unopposed
15-Dec-2010 Public – Wear Valley & Teesdale Elected unopposed
15-Dec-2010 Public – Darlington 31.3%
15-Dec-2010 Public – Durham 28.7%
15-Dec-2010 Public – Sedgefield 20.7%
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 98
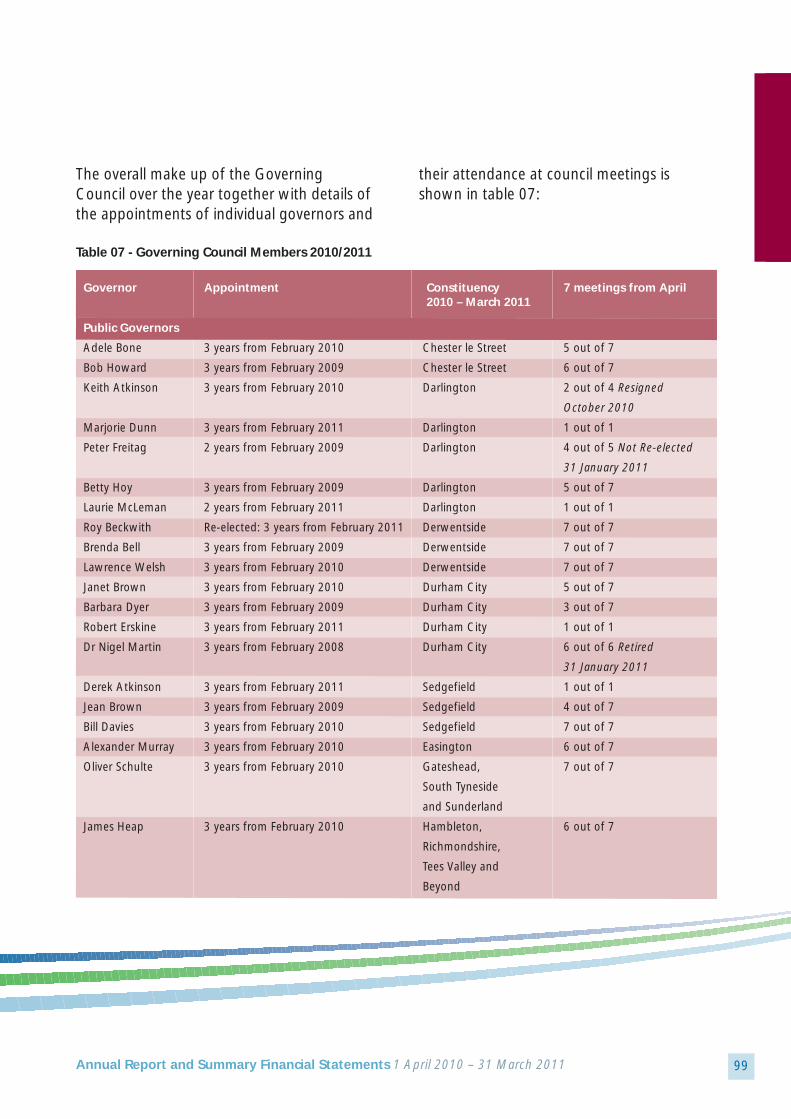
99Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The overall make up of the GoverningCouncil over the year together with details ofthe appointments of individual governors and
their attendance at council meetings isshown in table 07:
Table 07 - Governing Council Members 2010/2011
Governor Appointment Constituency 7 meetings from April 2010 – March 2011
Public Governors
Adele Bone 3 years from February 2010 Chester le Street 5 out of 7
Bob Howard 3 years from February 2009 Chester le Street 6 out of 7
Keith Atkinson 3 years from February 2010 Darlington 2 out of 4 Resigned
October 2010
Marjorie Dunn 3 years from February 2011 Darlington 1 out of 1
Peter Freitag 2 years from February 2009 Darlington 4 out of 5 Not Re-elected
31 January 2011
Betty Hoy 3 years from February 2009 Darlington 5 out of 7
Laurie McLeman 2 years from February 2011 Darlington 1 out of 1
Roy Beckwith Re-elected: 3 years from February 2011 Derwentside 7 out of 7
Brenda Bell 3 years from February 2009 Derwentside 7 out of 7
Lawrence Welsh 3 years from February 2010 Derwentside 7 out of 7
Janet Brown 3 years from February 2010 Durham City 5 out of 7
Barbara Dyer 3 years from February 2009 Durham City 3 out of 7
Robert Erskine 3 years from February 2011 Durham City 1 out of 1
Dr Nigel Martin 3 years from February 2008 Durham City 6 out of 6 Retired
31 January 2011
Derek Atkinson 3 years from February 2011 Sedgefield 1 out of 1
Jean Brown 3 years from February 2009 Sedgefield 4 out of 7
Bill Davies 3 years from February 2010 Sedgefield 7 out of 7
Alexander Murray 3 years from February 2010 Easington 6 out of 7
Oliver Schulte 3 years from February 2010 Gateshead, 7 out of 7
South Tyneside
and Sunderland
James Heap 3 years from February 2010 Hambleton, 6 out of 7
Richmondshire,
Tees Valley and
Beyond
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 99

100 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Governor Appointment Constituency 7 meetings from April 2010 – March 2011
Ian Jennings 3 years from February 2009 Wear Valley & 5 out of 7
Teesdale
John Short MBE Re-elected: 3 years from February 2011 Wear Valley & 7 out of 7
Teesdale
Doug Forster 3 years from February 2010 Wear Valley & 0 out of 7
Teesdale
Staff Governors
Gill Findley 3 years from February 2010 Administrative, 4 out of 7
Clerical and Managers
Robert Kent 3 years from February 2010 AHPs, Professional & 3 out of 7
Technical & Pharmacists
Dr Robin Mitchell 2.5 years from August 2010 Medical 2 out of 2 Resigned
January 2011
Dr Sarah Pearce 3 years from February 2010 Medical 2 out of 3 Retired
July 2010
Kevin Hull 3 years from February 2010 Ancillary 4 out of 7
Carole Bailey 3 years from February 2010 Nursing & Midwifery 4 out of 7
Carole Fletcher 3 years from February 2008 Nursing & Midwifery 3 out of 6 Retired
January 2011
Jean Fruend 3 years from February 2011 Nursing & Midwifery 0 out of 1
Kay Stewart 3 years from February 2009 Nursing & Midwifery 5 out of 7
Appointed Governors
Colin Burnett 3 years from February 2010 Appointed by North East 7 out of 7
Chamber of Commerce
Councillor Veronica 3 years from June 2008 Appointed by Darlington 4 out of 7
Copeland Borough Council
Lesley Crawford 3 years from May 2008 Appointed by Tees Esk 3 out of 7
and Wear Valleys NHS FT
Councillor Eunice 3 years from March 2009 Appointed by Durham 6 out of 7
Huntington County Council
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 100

101Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Governor Appointment Constituency 7 meetings from April 2010 – March 2011
Professor Paul Re-appointed: 3 years from Appointed by 5 out of 7
Keane OBE February 2010 Universities for the
North East
Professor Royston Re-appointed: 3 years from Appointed by North 4 out of 7
Stephens February 2010 East Strategic Health
Authority
David Gallagher 3 years from October 2009 Appointed by Primary 3 out of 7
Care Trusts
Dorothy Teasdale Re-appointed: 3 years from March 2010 Appointed by North 4 out of 7
East Ambulance Service
NHS Trust
Dr Paul Walton Re-appointed: 3 years from Appointed by the 3 out of 7
February 2010 Co. Durham Local
Medical Committee
A register is maintained of the interests ofgovernors in companies or related partiesthat are likely to do, or may seek to do,
business with the Trust. This register isavailable for inspection by the public byarrangement with the Trust Secretary.
The Trust Governing Council with Trust Chairman, Tony Waites, and SeniorIndependent Director, The Right Hon Baroness Hilary Armstrong
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 101

102 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Trust has two membershipconstituencies: the public constituencyand the staff constituency.
Public membership is open to anyone over theage of fourteen who resides within thegeographic area served by the Trust. Thisconstituency is divided into nine classes; six ofwhich reflect local authority borough or wardboundaries with the remaining three reflectingtraditional links with our hospitals eitherthrough the provision of sub-regional servicesbeyond our main catchment areas or becauseof ease of access:
• Chester-le-Street• Durham City• Darlington• Derwentside• Easington• Sedgefield• Wear Valley and Teesdale• Gateshead, South Tyneside,
Sunderland and beyond • Tees Valley, Hambleton,
Richmondshire and beyond.
At 31 March 2011 there were 7,340 membersin the public constituency as shown in table08 below.
Membership
Table 08 - Public Constituency Membership 2010/11
Public Constituency Membership 2010-2011
At year start (April 1) 6,047
New Members 1,330
Members leaving 37
At year end (March 31) 7,340
Members of Constituency Class
Chester-le-Street 503 6.85%
Darlington 1369 18.65%
Derwentside 1012 13.79%
Durham City 1593 21.70%
Easington 123 1.68%
Gateshead, South Tyneside, Sunderland & beyond 175 2.38%
Sedgefield 1072 14.60%
Tees Valley, Hambleton & Richmondshire & beyond 140 1.91%
Wear Valley & Teesdale 1334 18.17%
Other 19 0.26%
Grand Total 7,340 100.00%
32868_AR_Public_32868_AR_Public 30/06/2011 14:59 Page 102

103Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Staff who are employed directly by the Truston permanent contracts or who are employedon temporary or fixed term contracts for morethan twelve months automatically becomemembers of the staff constituency unless theyinform the Trust that they do not wish to doso. Staff who work for Trust contractors suchas our PFI partners may join the staffconstituency after twelve months. The staffconstituency is split into classes whichrepresent the major staff groups in the Trust.As at 31 March 2011, there were 5,414members in the staff constituency.
The Trust’s membership strategy envisagesstrong and continued growth in the publicmembership constituency. Delivery of thestrategy is led by the Governing Council whichhas established a specific committee todevelop both new recruitment initiatives andeffective arrangements for keeping membersengaged. Successful recruitment initiativeshave seen the membership grow significantlyduring the year.
Previously the ENT service at University
Hospital of North Durham (UHND) was
provided by City Hospitals Sunderland NHS
Foundation Trust. From April 2010, County
Durham and Darlington NHS Foundation
Trust will be providing a new ENT service at
the hospital and also at Shotley Bridge and
Chester-le-Street hospitals to enable the
service to grow and ensure patients can
receive care and treatment as close to
their home as possible. What does this mean for patients?
Until recently, patients requiringdiagnostics, day case or inpatienttreatments had to travel out of the area.
By providing a wider range of services,
including Day Case surgery at UHND,
we hope to provide more convenient
care for patients.
A new local Ear Nose Throat (ENT)service provided by County Durhamand Darlington Foundation Trust atUniversity Hospital of NorthDurham, Shotley Bridge Hospitaland Chester-le-Street Hospital• A full range of outpatient and post
operative follow-up appointments,including paediatric ENT; and mostdiagnostics
• Named Clinician via Choose and Book• A full hearing aid service• One site diagnostic and treatmentprocedures
• Adult and Paediatric day caseprocedures
• Access to a full range of complex and short stay ENT procedures
• Day Case Surgery at UHND• Full support from the audiology service• Access to balance clinics• Post operative follow up appointments
at the hospital nearest your home
“Delivering excellent carein hospital, home andcommunity”- Our Vision
Chester-le-StreetHospital
University Hospitalof North DurhamBishop AucklandHospitalDarlingtonMemorialHospital
Shotley BridgeHospital
Shotley BridgeHospital
Chester-le-StreetHospital
University Hospitalof North DurhamBishop AucklandHospitalDarlingtonMemorialHospital
Map of County Durham andDarlington Hospital sites
Short stay inpatient surgery will be carried
out at Darlington Memorial Hospital but
patients will receive post operative follow-
up care at their local hospital.We are setting aside some urgent slots in
clinics to enable patients to be seen on the
day of referral or shortly after. In the short
term until we have received approval from
the local Cancer Network, two weekcancer wait referrals must still be referred
to the local Cancer Centres.
County Durham and Darlington
NHS Foundation Trust
Your New ENT Service
from April 2010
acton
ces/Surgical
ormation
luding
ests.
NEWSROUNDNews for Members of County Durham and Darlington NHS Foundation Trust
Extra!
County Durham and DarlingtonNHS Foundation Trust
Page 2Seizing theFuture
Page 4Meet yourGovernors
Award for ‘excellent’
maternity services
Spring 2008
The Trust received
an excellentresponse and I am delighted
to welcome the four new and two
returning Members to the Governing
Council. I wish them well in their roles
and I look forward to working with
them in the coming months. I would
also like to take this opportunity to
thank those Governors who were not
re-elected for their valued contributions
over the past year. As I introduced in the last edition, the
Trust’s new Chief Executive, Stephen
Eames, has started to look at how we
can develop our hospitals and services in
the future. The Seizing the Future review is now well
underway with clinicians, managers,
directors and Governors all playing an
important role. We will soon be asking for your
views and comments on how you
would like to see our hospitals develop
over the next five years. We will be
hosting a series of events in the
different constituency areas to bring
you more information on the review
and to give you the opportunity to
have your say. The middle two pages of this edition are
dedicated to Seizing the Future and bring
you further details on these events as
well as the latest news on the work we
have done so far and our next steps.
I hope that as many of you as possible
will get involved as we work together
towards our future.Tony Waites
Trust Chairman
I would like to thank all of our Members who voted in the elections
at the start of the year.
Read the latest news about
Seizing the Future on pages
2 & 3 and then come along and
find out more at one of our
special events for FT Members.
During April and May we are inviting
FT Members to a series of ‘Member
workshop’ events. You’ll be able to
hear the latest information on
Seizing the Future and have your
say on the review.Turn to the back page for more details,
including dates, venues and how to
register a place.
Memberworkshops!
The Trust’s maternity services have
scooped a double accolade picking up
a top award and an ‘excellent’ rating
from the Healthcare Commission.
Earlier this year the Trust’s maternity
services received the Charter Mark award.
The Charter Mark is the Government’s
national standard for excellence and
maternity services had to go through a
detailed assessment to gain the status.
The accreditation, which is valid for three
years, covers all of the Trust’s four main
sites and means there is a quality of care
throughout the county.In the Healthcare Commission’s ‘Review of
Maternity Services 2007’, the Trust was
rated as ‘best performing’ delivering
‘excellent’ services in each of the three
maternity areas assessed.
Debbie Bunford, Head of Midwifery &
Gynaecology said; “We are delighted to
receive the Charter Mark and such good
results from the Healthcare Commission’s
report. They both recognise our
commitment to patients and to delivering
a high standard of care.”The three areas assessed were ‘clinical
focus’, ‘women centred care’ and
‘efficiency and capability’. The Trust came
top in the region for delivering the best
‘women centred care’ and third overall.
In a joint message of congratulations, the
Trust’s Chairman and Chief Executive said;
“The Trust can be extremely proud of
these results which show a true
commitment and dedication to deliver the
highest quality of care for which staff are
thanked and commended.”
Message from the ChairmanNEWSROUND
For future Members of a new NHS Foundation Trust for County Durham and DarlingtonExtra!Page 2
Meet our new
governors!
Royal Appointment
HRH The Princess Royal visited us to open formally our new cardiac suite
at Darlington Memorial Hospital. The Trust has a similar unit at University
Hospital of North Durham, funded by the Big Lottery Fund.
Patients needing vital heart tests,
who would previously have visited
hospitals in Newcastle or Middlesbrough, can now have their angiography
tests closer to home.
CO. DURHAM & DARLINGTON
SUNDERLAND
NORTH TEES
SOUTH TEES
GATESHEAD
NEWCASTLE
S. TYNESIDE
NORTHUMBRIA
Quality
Good
Excellent
Good
Good
Good
Good
Good
Good
Use of Resources
Good
Fair
Weak
Weak
Good
Good
Excellent
Good
The results say our performance for both
‘Service Quality’ and ‘Use of Resources’ is
‘Good’.
Only 52 Trusts – including Primary Care
Trusts and Mental Health Trusts, a
s well as
Acute Trusts, were rated ‘Good’ or better
for both of these key areas.
Chief Executive John Saxby said: “We are
very encouraged by our score in this first
Healthcheck, which follows two years in
which the Trust won the maximum three
star rating.
“The indicators are tougher than in
previous years so we do believe they
show solid and steady progress and are a
credit to our sta
ff.
“Where the results suggest th
at further
improvements can be made, we will be
working hard to deliver these over the
next year.”
“Good/Good” Score in
Annual Health Check
A Message from the Chairman
Dear Member
Our application to become a foundation
trust is moving on apace.
Having been approved by the Secretary of
State, we have now begun a rigorous
assessment by Monitor, the independent
regulator for foundation trusts.
This assessment will continue into the
new year, when we hope to be
authorised as a foundation trust from
February.
A key part of our new arrangements as
an FT is, of course, our governing body.
I am delighted that we have had such a
vibrant election process, and that can only
be a good thing in giving the governors
real legitimacy as representatives of the
membership.
Congratulations go to those who were
successful in the elections.
My thanks to those who were prepared
to stand but were not elected are as
sincerely felt. Your contribution has been
crucial in making sure that we had
meaningful elections by giving members a
real choice. Although you were not
successful on this occasion, you played a
key role in getting the Board of Governors
off to an excellent sta
rt.
Tony Waites
Trust Chairman
How we compare to local Trusts
The Trust’s full “Health Check” report is
on our website at www.cddah.nhs.uk.
For more information, see the Healthcare Commission website at
www.healthcarecommission.org.uk
Hospitals in County Durham and Darlington have
been rated highly in the Healthcare Commission’s
Annual Health Check – the new national system for
assessing the performance of trusts.
The Trust keeps its members informed with regular newsletters
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 103

104 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The NHS Act 2006 states that the ChiefExecutive is the Accounting Officer ofthe Trust. The relevant responsibilities of the Accounting Officer, including their responsibility for the propriety and regularity of public finances forwhich they are answerable, and for thekeeping of proper accounts, are set outin the NHS Foundation Trust AccountingOfficer Memorandum issued by theIndependent Regulator of NHSFoundation Trusts (“Monitor”).
Under the NHS Act 2006, Monitor hasdirected County Durham and Darlington NHSFoundation Trust to prepare for each financialyear a statement of accounts in the form andon the basis set out in the Accounts Direction.The accounts are prepared on an accrualsbasis and must give a true and fair view of thestate of affairs of the Trust and of its incomeand expenditure, total recognised gains andlosses and cash flows for the financial year.
In preparing the accounts, the AccountingOfficer is required to comply with therequirements of the NHS Foundation TrustAnnual Reporting Manual and in particular to:
• observe the Accounts Direction issued byMonitor, including the relevant accountingand disclosure requirements, and applysuitable accounting policies on a consistent basis;
• make judgements and estimates on a reasonable basis;
• state whether applicable accountingstandards as set out in the NHS FoundationTrust Annual Reporting Manual have beenfollowed, and disclose and explain anymaterial departures in the financialstatements; and
• prepare the financial statements on a going concern basis.
The Accounting Officer is responsible forkeeping proper accounting records whichdisclose with reasonable accuracy at any timethe financial position of the Trust and toenable him to ensure that the accountscomply with requirements outlined in theabove mentioned Act. The Accounting Officeris also responsible for safeguarding the assetsof the Trust and hence for taking reasonablesteps for the prevention and detection offraud and other irregularities.
To the best of my knowledge and belief, I have properly discharged the responsibilitiesset out in Monitor's NHS Foundation TrustAccounting Officer Memorandum.
Signed
Stephen EamesChief Executive
Date: 6 June 2011
Statement of the Chief Executive’s Responsibilitiesas the Accounting Officer of the County Durham &Darlington NHS Foundation Trust
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 104
105Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Scope of responsibilityAs Accounting Officer, I have responsibilityfor managing a sound system of internalcontrol that supports the achievement of theTrust’s policies, aims and objectives, whilstsafeguarding the public funds anddepartmental assets for which I ampersonally responsible, in accordance withthe responsibilities assigned to me. I am alsoresponsible for ensuring that the Trust isadministered prudently and economicallyand that resources are applied efficiently and effectively. I also acknowledge myresponsibilities as set out in the NHSFoundation Trust Accounting OfficerMemorandum.
The purpose of the system ofinternal controlThe system of internal control is designed tomanage risk to a reasonable level rather thanto eliminate all risk of failure to achievepolicies, aims and objectives; it can thereforeonly provide reasonable and not absoluteassurance of effectiveness. The system ofinternal control is based on an ongoingprocess designed to identify and prioritisethe risks to the achievement of the polices,aims and objectives of the County Durhamand Darlington NHS Foundation Trust, toevaluate the likelihood of those risks beingrealised and the impact should they berealised, and to manage them efficiently,effectively and economically. The system ofinternal control has been in place in the
County Durham and Darlington NHSFoundation Trust for the year ended 31March 2011 and up to the date of approvalof the Annual Report and Accounts.
Capacity to handle riskAs Chief Executive and Accounting Officer I am responsible for risk management.However, the day to day responsibility forclinical risk is delegated to the MedicalDirector and the Director of Nursing; whilstresponsibility for non-clinical risk is delegatedto the Chief Operating Officer. Managerswith responsibility for clinical and non-clinicalrisk management, health and safety,information governance and financial risksupport the Executive Leads on risk. Theyalso provide support to managers across theTrust on risk assessment, risk management,staff training and the development of goodpractice.
Members of staff receive regular mandatorytraining on the key aspects of the Trust’s riskmanagement strategy. In addition, a rangeof training programmes have been deliveredthroughout the year to raise clinical and non-clinical risk management awareness amongststaff and to ensure that individuals achievethe appropriate levels of competence andexpertise.
All of these processes are informed by theanalysis of incident reports, complaints andsurvey feedback, risk identification exercises,
Statement on Internal Control 2010/11
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 105

106 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
planning processes, national guidance andstudies of best practice. Wherever possible,opportunities are taken to learn lessons fromadverse events and near misses.
Good risk management practice is shared anddisseminated across the Trust using a varietyof media including the publication of a risknewsletter, good practice bulletins and theestablished risk management intranet site.
The risk and control frameworkThe Trust’s risk management strategyprovides the framework within which risk ismanaged. The key elements of the riskmanagement strategy are:
• A clear framework of accountability andresponsibility for the management of risk;
• A clearly defined committee structure,which supports timely decision making inresponse to organisational risk;
• Robust systems for the identification,analysis, prioritisation and mitigation ofrisk;
• Clinical and non-clinical risk teams tosupport risk control processes and thedevelopment of capacity within thedivisional and departmental teams;
• A mandatory training programme toembed risk management processes intothe day to day activities of the Trust;
• Communication processes to ensure thatinformation about key risks and lessonslearned is disseminated at all levelsthroughout the Trust; and
• External communication with stakeholdersand the general public through establishedpartnership forums and the GoverningCouncil.
The objectives of the risk managementstrategy are to ensure the safety of patients,staff and visitors, to ensure that the qualityof clinical care continues to improve and toprotect the Trust’s funds, assets andreputation. The strategy is reviewedregularly and is published on the Trust’sintranet site.
The Trust maintains a corporate risk registerwhich draws together the individual registersmaintained by divisions and departmentsand the overarching strategic risk identifiedby the Trust Board. The register records thenature of each risk, its relative priority withregards to other risks, the risk owner and theaction plan in place to mitigate or manage it.
Decision making about risk managementpriorities is made by the Risk Register Group.Priorities identified by the group are includedin the corporate risk register and fed into theTrust Board in order to support decisionmaking on prioritisation and the allocation of resources. The Risk Register Group alsocommunicates with the Audit Committee and the Quality and Healthcare GovernanceCommittee in relation to specific areas of risk.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 106

107Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Assurance Framework provides the TrustBoard with assurance that organisational riskis being managed appropriately. Theframework provides a high level analysis ofrisks in relation to the delivery of the Trust’skey objectives across all areas of activity. Foreach risk, the framework assesses thecontrols and processes that are in place toensure that the risks are managed effectivelyand the specific evidence that is available togive the Trust Board the necessary assurancethat the risk management and controlprocesses are effective. Gaps in assuranceare identified in order to ensure that theseare addressed.
The Assurance Framework is monitored bythe Trust Board, the Audit Committee and,during 2010/11, the following sub-committees of the Board: Business andInfrastructure, Healthcare Governance,Quality and Innovation and Marketing andService Development. These arrangements
have been streamlined for 2011/12 by theestablishment of a single clinical committee,the Quality and Healthcare GovernanceCommittee, and a single businesscommittee, the Business and OperationsCommittee.
These risk management arrangements are embedded within the divisions anddepartments of the Trust but are also used to provide an appropriate control systemaround the Trust’s special projects orprogrammes. Accordingly, risk registers andAssurance Frameworks were maintained forthe Towards 2014 programme and, morerecently, for the due diligence exerciseassociated with the TransformingCommunity Services agenda.
In 2010/11, the Trust Board identified thefollowing high level strategic risks whichwere managed dynamically through theCorporate Risk Register with success beingmeasured against defined indicators:
• The risk of clinical services becomingunsustainable as a result of a change ofclinical vision, a failure to engage partnersor changes to the commissioning process.A further risk to clinical standards andfinancial performance was identified ifclinical transformation was not delivered.The Trust Board responded to these risksby establishing the Clinical Services TaskForce under the leadership of the ChiefExecutive to undertake a systematic and
Dr Anjan Dhar, Consultant Gastroenterologist is leading a national research study
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 107

108 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
radical review of services and to developthe integrated Trust’s Clinical Strategygoing forward.
• The risk to the delivery of high class healthservices posed by the aging DarlingtonMemorial Hospital and concern around ITresilience. These issues were addressed bysignificant capital investment in the estateat Darlington Memorial Hospital duringthe year and in Trust-wide IT systems.
• The risk of a failure to deliver on financialperformance targets and on the Trust’schallenging cost improvement programmewas managed through the application ofrobust financial controls, the clearcommunication of financial objectives andtargets and the flexing of budgets inaccordance with activity. For 2011/12 anew system of inter-divisional trading hasbeen instituted.
• During the year, the Trust undertookrequisite due diligence in respect of theacquisition of the community servicesprovider. The risk that the demands of thisprocess would distract from operationalperformance was identified andsuccessfully mitigated through strongperformance arrangements and the use ofadditional resource where appropriate.
The Trust will continue to manage all majorrisks going forward through the riskmanagement system.
The Trust recognises that it is not possible, or always desirable, to eliminate all risks andthat systems should not stifle innovation.When all reasonable control mechanismshave been put in place there will inevitablyremain some residual risk and this level ofrisk must be accepted. Risk acceptancewithin the Trust is systemic and transparent.Where residual risk remains, the risk isscored “low” on the risk register. Thisensures that it is regularly reviewed throughthe control system, as opposed to beingremoved from the risk register and being lostfrom sight.
As a foundation trust, the Trust’s Board ofDirectors is accountable to the GoverningCouncil. The Corporate Risk Register ispresented on a quarterly basis to theGoverning Council’s Quality and HealthcareGovernance Committee which in turnreports to the Governing Council. Inaddition, the Trust reports all SeriousUntoward Incidents to its commissioners aspart of its contractual arrangements andworks with the local authority Overview andScrutiny Committees to address issues raisedby the public or local councillors.
The Trust has robust procedures in place forthe management of risks associated with theholding and processing of personalinformation. The Trust has a dedicatedmanager with responsibility for informationgovernance and data security. Informationgovernance and data security are overseen
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 108

109Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
by the Chief Operating Officer, who is thedesignated Senior Information Risk Officer,and the Information Governance SteeringGroup which reports via the Board’s Businessand Operations Committee to the TrustBoard.
The Trust conducts an annual review of itsarrangements using the InformationGovernance Toolkit Assessment and wasrated “Green - Satisfactory” with 88 %compliance against the relevant standards.
During the year, there were no SeriousUntoward Incidents relating to informationgovernance.
The Head of Internal Audit Opinion for2010/11 identified the following as areas ofconcern during the year where controls weredeemed to be in need of improvement,although it should be noted that there wereno “no assurance” reports issued during theyear:
• A lack of compliance with policies andprocedures to ensure robust pre-employment checks were completed forall junior doctors recruited by the LeadEmployer Trust was identified. A detailedaction plan was put in place bymanagement at the Lead Employer Trustto reinforce adherence to procedures forfuture recruitment drives.
• Weaknesses in the planning, monitoringand implementation mechanisms for costimprovement programmes at divisionallevel were identified. The Trust reviewedits approach to the development andmanagement of cost reduction schemesfor 2011/12 with the aim of improvinggranular planning, accountability andcontingency planning to ensure thattargets are met.
Thanks to funding from the Friends of the Hospital, each of the Trust’s threemain sites has introduced specialist crockery to support patients with dementia
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 109

110 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• Testing revealed a lack of compliance withthe Trust’s policy for Real-Time DataCapture to the patient administrationsystem, resulting in delays and someinaccuracies in data input at ward level,which could impact on performancetargets and the timely issue of dischargeletters to GPs. The Nursing Directorateidentified a number of potential barriers toeffective implementation of the Real-TimeData Capture Policy which are beinginvestigated further.
• Clinical audit arrangements were found to be in need of further development toensure that agreed programmes weredelivered and that there was a consistentlyrobust process to identify, implement andassess the impact of actions to improveclinical practice (where necessary) within
the Trust. The Associate Director ofPatient Safety and Governance is leadingwork to develop clinical audit proceduresin line with best practice.
• Whilst sound policies and procedures werein place with respect to Information RiskManagement, the roles of InformationAsset Owner (IAO) and Information AssetAdministrator (IAA) were identified as notbeing fully embedded within some areas.The Information Governance Team iscontinuing to oversee a programme to roll out Information Risk Managementpractices across the Trust, includingmonitoring the quality of informationasset registers and risk assessments. The completion of training for all IAOs and IAAs will continue to be monitored.
The Trust supports World Aids Day with local health economy partners
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 110

111Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• Some aspects of the Safeguardingarrangements were identified as needingstrengthening, including training records,performance monitoring and follow upprocedures where children “flagged” asbeing at risk miss appointments. Actionplans are now in place to improveSafeguarding arrangements in the areasidentified.
The Trust is fully compliant with therequirements for registration with the Care Quality Commission.
As an employer with staff entitled tomembership of the NHS Pension Scheme,control measures are in place to ensure allemployer obligations contained within theScheme regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions andpayments into the Scheme are in accordancewith the Scheme rules and that memberPension Scheme records are accuratelyupdated in accordance with the timescalesdetailed in the regulations.Control measures are in place to ensure that the Trust’s obligations under equality,diversity and human rights legislation arecomplied with.
The Trust has undertaken risk assessmentsand Carbon Reduction Delivery Plans are in place in accordance with emergencypreparedness and civil contingencyrequirements, as based on UKCIP 2009
weather projects, to ensure that thisorganisation’s obligations under the ClimateChange Act and the Adaptation Reportingrequirements are complied with.
Review of economy, efficiencyand effectiveness in the use ofresourcesThe Trust has arrangements in place foragreeing strategic and annual objectives thattake account of the need to demonstrateeconomy, efficiency and effectiveness in theuse of resources. The business strategy andannual plans include specific objectives forimproving economy, efficiency andeffectiveness through the use of detailedcost improvement programmes, capitalinvestment and workforce control. Theseplans are considered by the GoverningCouncil and approved by the Trust Board.
The Trust Board reviews all aspects of theTrust’s financial performance in detail on amonthly basis. The Trust Board has in placea robust control framework which includes:
• Budgetary control processes with clearescalation arrangements and contingencyplans;
• Performance management arrangements;
• Regular routine review by the Trust Boardand Executive Directors Group of financialand operational performance;
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 111

112 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
• Procurement arrangements on a consortiumbasis working with other NHS bodies;
• Review of the effectiveness of the use ofresources by the Audit Committee; and
• Rolling programme of audits inaccordance with an agreed plan of workpresented by the Trust’s internal auditors.
The control framework within the Trust has been enhanced during 2010/11 by a rigorous review of the Trust’s StandingOrders, Standing Financial Instructions andScheme of Delegation which provide thestructure for financial decision making.
Annual Quality ReportThe Directors are required under the HealthAct 2009 and the National Health Service(Quality Accounts) Regulations 2010 toprepare Quality Accounts for each financialyear. Monitor has issued guidance to NHSfoundation trust boards on the form andcontent of annual Quality Reports whichincorporate the above legal requirements inthe NHS Foundation Trust Annual ReportingManual.
A number of steps have been taken toassure the Trust Board that the 2010/11Quality Report provides a balanced view andthat appropriate controls are in place toensure the accuracy of data.
These include the following:
• The appointment of the Director ofNursing to provide leadership on allmatters relating to the development of the Quality Report;
• The Trust Board receives monthlyperformance and patient safety reports,the data from which is used to inform theQuality Report;
• The Quality Report priorities areformulated through discussion with theTrust Board, the Governing Council, ourstaff, our commissioner, local LINksorganisations and the local authorityOverview and Scrutiny Committees;
• Assurance around the accuracy andsuitability of data is provided by theHealthcare Governance and Quality andInnovation Committees (as appropriate);
• Independent assurance around thesystems and processes in place to ensurethat the internal controls over thecollection and processing of dataunderpinning the Quality Accounts areadequate and effective is provided byInternal Audit; and
• Additional external assurance is taken asappropriate to address specific concerns.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 112
113Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Review of effectivenessAs Accounting Officer, I have responsibilityfor reviewing the effectiveness of the systemof internal control. My review of theeffectiveness of the system of internalcontrol is informed by the work of theinternal auditors and the executive managerswithin the Trust who have responsibility forthe development and maintenance of theinternal control framework, and commentsmade by the external auditors in theirmanagement letter and other reports. I havebeen advised on the implications of theresult of my review of the effectiveness ofthe system of internal control by the Board,the Audit Committee and the Quality andHealthcare Governance Committee and aplan to address weaknesses and ensurecontinuous improvement of the system is inplace.
The Trust Board and its sub-committees haveroutinely reviewed the component parts ofthe Trust’s system of internal control. TheAudit Committee has also scrutinised andundertaken work to strengthen aspects ofthe Trust’s system of internal control,including reviewing the risk managementand Assurance Framework arrangements.
Internal audit has reviewed and reportedupon various aspects of the system ofinternal control in accordance with the auditplan approved by the Audit Committee.That work was carried out in accordance
with the Audit Code for NHS FoundationTrusts. The implementation of agreedinternal audit recommendations has beenmonitored by the Audit Committee.
The Head of Internal Audit opinion 2010/11has been received on the effectiveness of thesystem of internal control. The overallopinion is that significant assurance can begiven that there is a generally sound systemof internal control designed to meet theorganisation’s objectives and that controlsare generally being applied consistently.
The only significant internal control issuesidentified during the year have beendescribed within this Statement on InternalControl and action plans have been, or arebeing, developed and implemented tostrengthen controls in these areas. Thebenchmarking and external assessmentsthroughout the year continued to recognisethe Trust as a high performing and efficientlymanaged NHS foundation trust.
Signed
Stephen EamesChief Executive
Date: 6 June 2011
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 113

114 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Territorial Army presents two pieces of commemorative artwork to Trust Chairman, Tony Waites. The Artworkcan be seen displayed at Darlington Memorial Hospital and the University Hospital of North Durham
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 114

115Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Summary Financial Statements for the yearended 31 March 2010
Accounts for the year ended 31 March2011 have been prepared under directionfrom Monitor and have been audited by Deloitte.
The accounts have received an unqualifiedopinion that they give a true and fair view ofthe state of affairs of the Trust as at 31 March2011 including its income and expenditurefor the year to that date.
This report contains summarised financialstatements which have received a similaraudit opinion.
The accounts relating to the Trust'sCharitable Funds will be available from 1st February 2012.
Full sets of accounts are available from:Mrs Sue Jacques,Director of Finance,County Durham and Darlington NHSFoundation Trust,Darlington Memorial Hospital, HollyhurstRoad, Darlington, DL3 6HX.
Or email [email protected]
Going ConcernAfter making enquiries, the Directorsreasonably expect that the County Durhamand Darlington NHS Foundation Trust has adequate resources to continue inoperational existence for the foreseeablefuture. For this reason, they continue toadopt the going concern basis in preparingthe accounts.
Director’s declarationSo far as the Directors are aware, there is no relevant audit information of which theauditors are unaware and the Directors havetaken all steps that they ought to as Directorsin order to make themselves aware of anyrelevant information and to ensure theauditors were aware of that information.
PensionsThe accounting policies for pensions andother retirement benefits are set out in page7 of the full annual accounts and details ofsenior employee remuneration can be foundin page 124 of this annual report.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 115
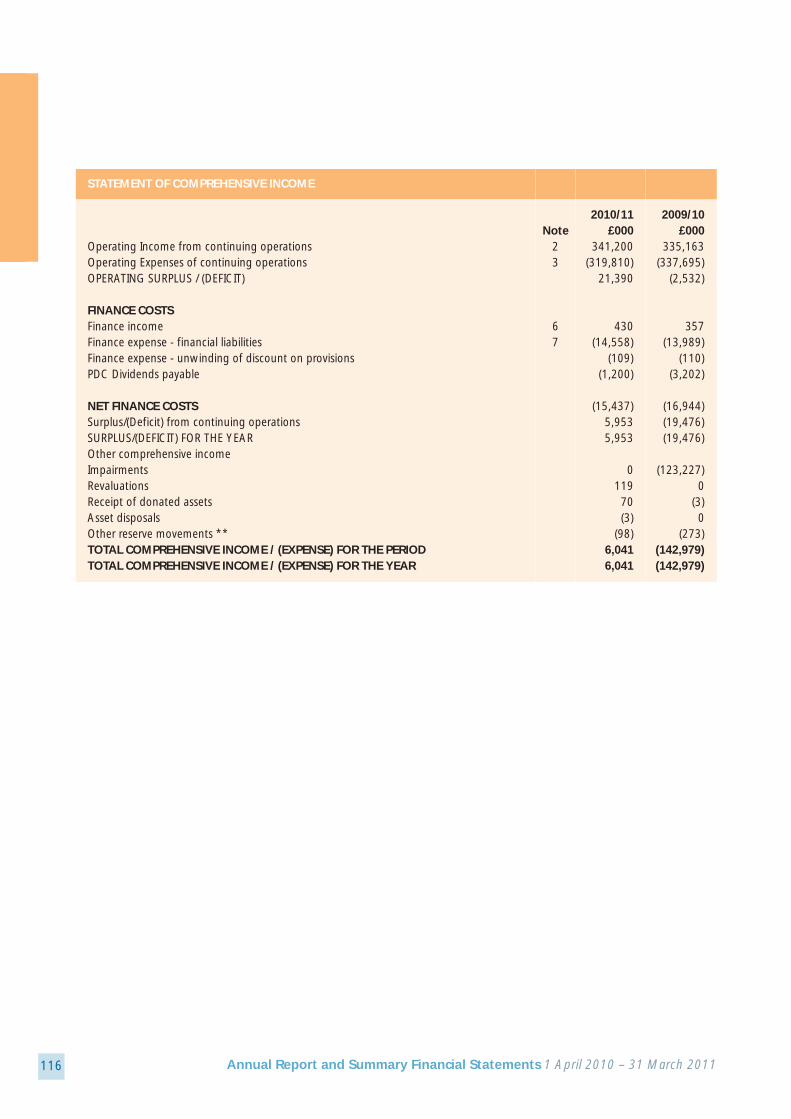
116 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
STATEMENT OF COMPREHENSIVE INCOME
2010/11 2009/10Note £000 £000
Operating Income from continuing operations 2 341,200 335,163Operating Expenses of continuing operations 3 (319,810) (337,695)OPERATING SURPLUS / (DEFICIT) 21,390 (2,532)
FINANCE COSTSFinance income 6 430 357Finance expense - financial liabilities 7 (14,558) (13,989)Finance expense - unwinding of discount on provisions (109) (110)PDC Dividends payable (1,200) (3,202)
NET FINANCE COSTS (15,437) (16,944)Surplus/(Deficit) from continuing operations 5,953 (19,476)SURPLUS/(DEFICIT) FOR THE YEAR 5,953 (19,476)Other comprehensive incomeImpairments 0 (123,227)Revaluations 119 0Receipt of donated assets 70 (3)Asset disposals (3) 0Other reserve movements ** (98) (273)TOTAL COMPREHENSIVE INCOME / (EXPENSE) FOR THE PERIOD 6,041 (142,979)TOTAL COMPREHENSIVE INCOME / (EXPENSE) FOR THE YEAR 6,041 (142,979)
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 116

117Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
STATEMENT OF COMPREHENSIVE INCOME
Note: Allocation of Profits/(Losses) for the period: 2010/11 2009/10£000 £000
(a) Surplus/(Deficit) for the period attributable to:(i) minority interest, and 0 0(ii) owners of the parent. 5,953 (19,476)TOTAL 5,953 (19,476)(b) total comprehensive income/ (expense) for the period attributable to:(i) minority interest, and 0 0(ii) owners of the parent. 6,041 (142,979)TOTAL 6,041 (142,979)
* Impact of Property Plant and Equipment revaluations £000 £000Operating Surplus before accounting adjustments 17,519 20,924Change in the value of Trust Property Plant and Equipment 3,871 -23,456Net Operating Surplus 21,390 (2,532)
Operating expenses include a non cash notional credit of £3.8m (a charge of £23.5m in 2009/10) which reflects the change inthe replacement value of the Trust's land and buildings. Accounting standards require this change in value to be charged tothe Statement of Comprehensive Income. The underlying operating surplus was £17.5m (£20.9m in 2009/10) which wouldhave covered the planned interest and dividend charges, leaving a £2.1m (£3.9m in 2009/10) net surplus for the year.
** The format of the SOCI changed in 2010/11 with the 2009/10 figures for the reduction in the donated asset reserve due todepreciation etc now being shown within the Other reserve movement line
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 117

118 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
STATEMENT OF FINANCIAL POSITION
31 March 2011 31 March 2010 note £000 £000
Non-current assetsIntangible assets 9 374 143Property, plant and equipment 10 212,270 193,632Total non-current assets 212,644 193,775Current assetsInventories 16 2,578 2,639Trade and other receivables 17 8,124 7,486Non-current assets for sale and assets in disposal groups 13 1,100 1,100Cash and cash equivalents 20 70,409 74,861Total current assets 82,211 86,086Current liabilitiesTrade and other payables 23 (37,641) (34,338)Borrowings 24 (4,526) (4,522)Provisions 28 (2,156) (560)Tax payable (6,690) (6,528)Other liabilities 26 (17,444) (7,308)Total current liabilities (68,457) (53,256)Total assets less current liabilities 226,398 226,605Non-current liabilitiesBorrowings 24 (120,020) (124,816)Provisions 28 (3,428) (4,880)Total non-current liabilities (123,448) (129,696)Total assets employed 102,950 96,909Financed by (taxpayers' equity)Public Dividend Capital 108,421 108,421Revaluation reserve 30 1,311 1,603Donated Asset Reserve 518 574Income and expenditure reserve (7,300) (13,689)Total taxpayers' equity 102,950 96,909
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 118

119Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Taxpayers' Equity at 1 April 2010 - aspreviously stated
Taxpayers' Equity at 1 April 2010 - restated
Surplus/(deficit) for the year
Revaluations
Receipt of donated assets
Asset disposals
Other reservemovements
Taxpayers' Equity at 31 March 2011
Total MinorityInterest
PublicDividendCapital
DonatedAssets
Reserve
OtherReserves
MergerReserve
Income andExpenditure
Reserve
Availablefor Sale
investmentReserve
RevaluationReserve
£000 £000
96,909 0 108,421 1,603 574 0 0 0 (13,689)
96,909 0 108,421 1,603 574 0 0 0 (13,689)
5,953 0 0 0 0 0 0 0 5,953
119 0 0 119 0 0 0 0 0
70 0 0 0 70 0 0 0 0
(3) 0 0 0 (3) 0 0 0 0
(98) 0 0 (411) (123) 0 0 0 436
102,950 0 108,421 1,311 518 0 0 0 (7,300)
£000 £000 £000 £000 £000 £000 £000
STATEMENT OF CHANGES INTAXPAYERS' EQUITY
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 119

120 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
STATEMENT OF CHANGES IN TAXPAYERS' EQUITY CONTINUED
Taxpayers' Equity at 1 April 2009 - aspreviously stated
Taxpayers' Equity at 1 April 2009 - restated
Surplus/(deficit) for the year
Impairments*
Receipt of donated assets
Asset disposals**
Other reservemovements
Taxpayers' Equity at 31 March 2010
Total MinorityInterest
PublicDividendCapital
DonatedAssets
Reserve
OtherReserves
MergerReserve
Income andExpenditure
Reserve
Availablefor Sale
investmentReserve
RevaluationReserve
£000 £000
239,888 0 108,421 123,207 837 0 0 0 7,423
239,888 0 108,421 123,207 837 0 0 0 7,423
(19,476) 0 0 0 0 0 0 0 (19,476)
(123,227) 0 0 (123,227) 0 0 0 0 0
(3) 0 0 0 (3) 0 0 0 0
0 0 0 (411) 0 0 0 0 411
(273) 0 0 2,034 (260) 0 0 0 (2,047)
96,909 0 108,421 1,603 574 0 0 0 (13,689)
£000 £000 £000 £000 £000 £000 £000
STATEMENT OF CHANGES INTAXPAYERS' EQUITY
*The Trust moved to a new method of valuing its land and buildings in 2009-10, based on the Modern Equivalent Asset value.The full impact of this has been disclosed in note 10.
** Transfers to the I & E reserve are in respect of Equipment indexation which is being written off on a straightline basis over a four year period.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 120
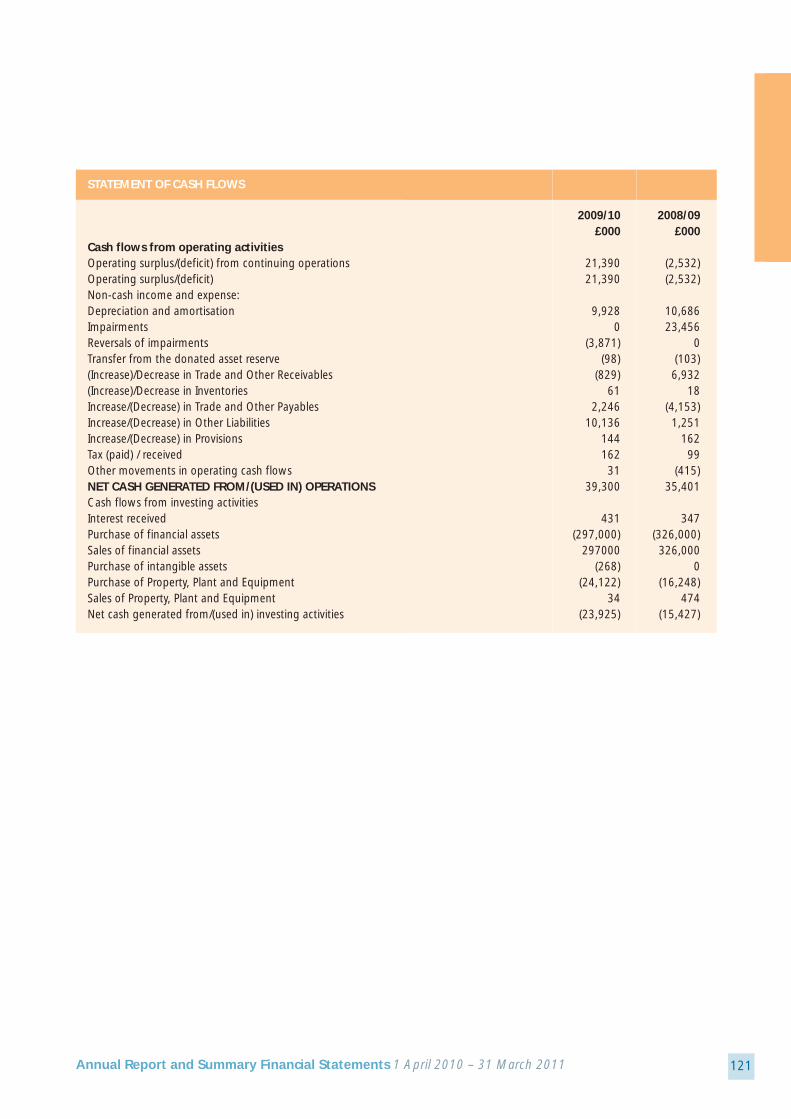
121Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
STATEMENT OF CASH FLOWS
2009/10 2008/09£000 £000
Cash flows from operating activitiesOperating surplus/(deficit) from continuing operations 21,390 (2,532)Operating surplus/(deficit) 21,390 (2,532)Non-cash income and expense:Depreciation and amortisation 9,928 10,686Impairments 0 23,456Reversals of impairments (3,871) 0Transfer from the donated asset reserve (98) (103)(Increase)/Decrease in Trade and Other Receivables (829) 6,932(Increase)/Decrease in Inventories 61 18Increase/(Decrease) in Trade and Other Payables 2,246 (4,153)Increase/(Decrease) in Other Liabilities 10,136 1,251Increase/(Decrease) in Provisions 144 162Tax (paid) / received 162 99Other movements in operating cash flows 31 (415)NET CASH GENERATED FROM/(USED IN) OPERATIONS 39,300 35,401Cash flows from investing activitiesInterest received 431 347Purchase of financial assets (297,000) (326,000)Sales of financial assets 297000 326,000Purchase of intangible assets (268) 0Purchase of Property, Plant and Equipment (24,122) (16,248)Sales of Property, Plant and Equipment 34 474Net cash generated from/(used in) investing activities (23,925) (15,427)
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 121
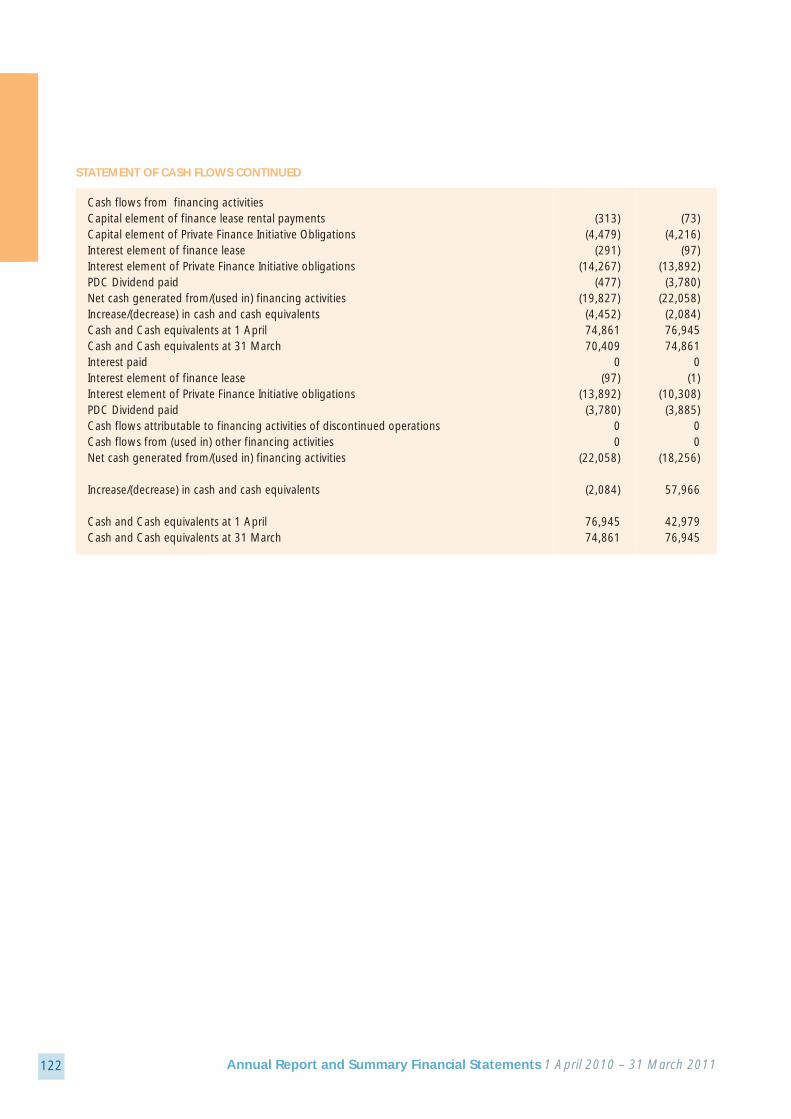
122 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Cash flows from financing activitiesCapital element of finance lease rental payments (313) (73)Capital element of Private Finance Initiative Obligations (4,479) (4,216)Interest element of finance lease (291) (97)Interest element of Private Finance Initiative obligations (14,267) (13,892)PDC Dividend paid (477) (3,780)Net cash generated from/(used in) financing activities (19,827) (22,058)Increase/(decrease) in cash and cash equivalents (4,452) (2,084)Cash and Cash equivalents at 1 April 74,861 76,945Cash and Cash equivalents at 31 March 70,409 74,861Interest paid 0 0Interest element of finance lease (97) (1)Interest element of Private Finance Initiative obligations (13,892) (10,308)PDC Dividend paid (3,780) (3,885)Cash flows attributable to financing activities of discontinued operations 0 0Cash flows from (used in) other financing activities 0 0Net cash generated from/(used in) financing activities (22,058) (18,256)
Increase/(decrease) in cash and cash equivalents (2,084) 57,966
Cash and Cash equivalents at 1 April 76,945 42,979Cash and Cash equivalents at 31 March 74,861 76,945
STATEMENT OF CASH FLOWS CONTINUED
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 122

123Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
The Trust contributed £18m in 2010-11 tothe NHS Pensions Agency on behalf of itsemployees.
The NHS pension scheme is subject to a fullvaluation every four years by the GovernmentActuary. The latest published valuation relatesto the period 1 April 1999 to 31 March 2004which was published in December 2007 andis available on the Pensions Agency website :http://www.nhsbsa.nhs.uk/Pensions/Valuation.aspx
The notional deficit of the scheme was £3.3billion as per the last scheme valuation by theGovernment Actuary for the period 1 April
1999 to 31 March 2004. The conclusion ofthe valuation was that the scheme continuesto operate on a sound financial basis.Employer contribution rates are reviewedevery four years following the schemevaluation, on advice from the actuary. At thelast valuation, it was recommended thatemployer contribution rates should continueat 14% of pensionable pay. From 1 April2008, employees’ contributions will be on atiered scale from 5% to 8.5% of theirpensionable pay.
The Trust agreed the following severancearrangements in 2010/11
Exit package cost Number of Number of other Total number ofband compulsory departures agreed exit packages by
redundancies cost band
< £10,000 0 8 8
£10,000 - £25,000 0 1 1
£25,001 - £50,000 0 1 1
£50,001 – £100,000 0 4 4
£100,000 - £150,000 0 2 2
£150,001 - £200,000 0 1 1
Total number ofexit packages by 0 17 17type
Total resource cost 0 739 739£000
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 123

124 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
2010-2011
Sala
ry
(ban
ds o
f £50
00)
Oth
er re
mun
erat
ion
(ban
ds o
f £50
00)
Bene
fits
in K
ind*
(roun
ded
to th
ene
ares
t £10
0)
Sala
ry
(ban
ds o
f £50
00)
Oth
er re
mun
erat
ion
(ban
ds o
f £50
00)
Bene
fits
in K
ind*
(roun
ded
to th
ene
ares
t £10
0)
2009-2010
Note 4.5a Senior Manager's Short term Employment benefits
£000s £000s £000s £000s £000s £000s
Current Senior Mgrs (Full Year 2010/2011)
Mr S Eames - Chief Executive 180-185 14.0 185-190 15.2Mrs S Jacques - COO / Director of Finance 145-150 145-150Miss LI Robson - Director of Nursing 100-105 100-105Mr RT McEwan - Director of Ops and Bus Devt 110-115 110-115Mr W Headley - Director of Estates & Facilities 110-115Mr IM Bain - Divisional Clinical Director 35-40 180-185 0.4 35-40 195-200 0.4Dr PH Moncur - Medical Director 40-45 105-110Dr NC Munro - Divisional Clinical Director 30-35 135-140 30-35 130-135Mr TA Waites - Chairman 50-55 50-55Mrs KA Larkin-Bramley - Non-Executive Director 15-20 15-20Dr RM Waterston - Non-Executive Director 10-15 10-15Dr IG Robson - Non-Executive Director 10-15 15-20
Current Senior Mgrs (Part Year 2010/2011)
Dr RWD Mitchell - Acting Medical Director 5-10 25-30 0.2 from 17 January 2011Dr SM Cronin - Divisional Clinical Director 15-20 70-75 2.1from 1 October 2010Dr S Dabner - Divisional Clinical Director 15-20 55-60from 1 October 2010Ms HJ Armstrong - Non-Executive Director 5-10from 1 November 2010Mr AL Young - Non-Executive Director 10-15from 1 July 2010
Name and Title
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 124

125Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Former Senior Mgrs (Part Year 2010/2011)
Mr ASM Ali - Divisional Clinical Director to 30 September 2010 15-20 70-75 30-35 145-150Dr RWD Mitchell - Divisional Clinical Director to 30 September 2010 15-20 65-70 0.4 35-40 145-150 0.9Mr AG Wolfe - Non-Executive Director to 30 September 2010 5-10 15-20Mr PR Stewart - Non-Executive Director to 30 June 2010 0-5 10-15
Former Senior Mgrs (Part Year 2009/2010)
Mr R H Aitken - Medical Director 45-50 100-105to 1 Feb 2010Dr DJ McCullough - Acting Medical 10-15 10-15Director from 1 Feb 2010 to 31 Mar 2010Total 955-960 725-730 17.1 880-885 730-735 16.5
Benefits in kind are comprised as follows: Trust Total Trust Totallease car lease car
£000 £000 £000 £000Mr S Eames 14.0 14.0 15.2 15.2Mr IM Bain 0.4 0.4 0.4 0.4Dr SM Cronin 2.1 2.1 0.0 0.0Dr RWD Mitchell 0.6 0.6 0.9 0.9
17.1 17.1 16.5 16.5
Following the Trust's restructuring of the senior management ahead of the 'transforming community services'initiative, Mr RT McEwan will be made redundant with effect from 15 May 2011 and will receive a redundancypayment of £168,960. This is accounted for in 2010/11 as the decision was agreed before 1 April 2011.
Note 4.5a Senior Manager's Short term Employment benefits Continued
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 125

126 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Real
incr
ease
in p
ensio
n at
age
60 (b
ands
of £
2500
)
Lum
p Su
m a
t Age
60
rela
ted
to re
al in
crea
se in
pens
ion
(ban
ds o
f £25
00)
Tota
l acc
rued
pen
sion
at a
ge 6
0 at
31
Mar
ch20
11 (b
ands
of £
5000
)
Lum
p Su
m a
t age
60
rela
ted
to a
ccru
ed p
ensio
n at
31
Mar
ch 2
011
(ban
ds o
f £50
00)
Cas
h Eq
uiva
lent
Tran
sfer
Val
ue a
t31
mar
ch 2
011
Cas
h Eq
uiva
lent
tran
sfer
Val
ue a
t31
Mar
ch 2
010
real
incr
ease
in c
ash
equi
vale
nt tr
ansf
erva
lue
(em
ploy
er fu
nded
)
Empl
oyer
s C
ontr
ibut
ion
to S
take
hold
er P
ensio
n(n
eare
st £
100)
Senior Managers Pension Information
Name and Title £000s £000s £000s £000s £000s £000s £000s £000s
Mr S Eames - Chief Executive 0.0-2.5 5.0-7.5 80-85 250-255 1,654 1,755 -63 0
Mrs S Jacques - Director of Finance 0.0-2.5 5.0-7.5 30-35 100-105 431 472 -26 0
Ms L Robson - Director of Nursing 0.0-2.5 2.5-5.0 40-45 130-135 872 922 -31 0
Mr RT McEwan - Director of Ops and Bus. Devt. 0.0-2.5 2.5-5.0 15-20 55-60 312 323 -6 0
Mr T Hunt - Project Director TCS from 1 Feb 2011 0 0 0 0 0 0 0 0
Mr W Headley - Director of Estates & Facilities 0.0-2.5 5.0-7.5 25-30 85-90 550 545 3 0
Mr A Ali - Divisional Director to 30 Sep (7.5)-(10.0) (22.5)-(25.0) 40-45 130-135 0 1,464 -451 0
Mr IM Bain - Divisional Director (2.5)-(5.0) (12.5)-(15.0) 45-50 145-150 753 946 -120 0
Dr RWD Mitchell - Divisional Director to 30 Sep, Acting MD from 17 January 2011 0-(2.5) 0-(2.5) 60-65 180-185 1,243 1,375 -41 0
Dr NC Munro - Divisional Director 2.5-5.0 10.0-12.5 50-55 155-160 933 962 -18 0
Dr P Moncur - Medical Director 5.0-7.5 17.5-20.0 25-30 75-80 314 291 14 0
Dr S Cronin - Divisional Director from 1 October 2010 2.5-5.0 10.0-12.5 45-50 135-140 857 793 20 0
Dr S Dabner - Divisional Director from 1 October 2010 0.0-2.5 2.5-5.0 25-30 85-90 350 387 -12 0
Total 7.5-10.0 30.0-32.5 515-520 1560-1565 8,269 10,235 (736) 0
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 126

127Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
A Cash Equivalent Transfer Value (CETV) isthe actuarially assessed capital value of thepension scheme benefits accrued by amember at a particular point in time. Thebenefits valued are the member's accruedbenefits and any contingent spouse's pensionpayable from the scheme. A CETV is apayment made by a pension scheme, orarrangement to secure pension benefits inanother pension scheme or arrangementwhen the member leaves a scheme andchooses to transfer the benefits accrued intheir former scheme. The pension figuresshown relate to the benefits that theindividual has accrued as a consequence of their total membership of the pensionscheme, not just their service in a seniorcapacity to which the disclosure applies. The CETV figures, and from 2004-05 theother pension details, include the value ofany pension benefits in another scheme orarrangement which the individual hastransferred to the NHS pension scheme. They also include any additional pensionbenefit accrued to the member as a result of their purchasing additional years of pensionservice in the scheme at their own cost.CETVs are calculated within the guidelinesand framework prescribed by the Instituteand Faculty of Actuaries.
Real Increase in CETV - This reflects theincrease in CETV effectively funded by theemployer. It takes account of the increase inaccrued pension due to inflation,contributions paid by the employee (includingthe value of any benefits transferred fromanother pension scheme or arrangement)and uses common market valuation factorsfor the start and end of the period. In October 2008 the Occupational PensionScheme (Transfer Value Amendment)regulations changed the way in whichschemes are required to calculate transfervalues. The pension entitlement of schememembers however remained consistent withprevious years.
NotesIn the 2010 Budget the Chancellorannounced that the uprating (annualincrease) of public sector pensions wouldchange from the Retail Prices Index (RPI) tothe Consumer Prices Index (CPI) with thechange expected from April 2011. As a resultthe Government Actuaries Departmentundertook a review of all transfer factors. Thenew CETV factors have been used in thesecalculations and are lower than the previousfactors used. As a result the value of theCETVs for some senior managers has fallensince 31/03/2010.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 127

128 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Mr A Ali retired and called on his pensionduring 2010/2011. There is therefore no cashequivalent value at 31 March 2011
The pension and lump sum for severaldivisional directors has reduced during theyear. Pensionable pay was inflated in2009/2010 when it was agreed that due to clinical senior managers should bepensionable, backdated to 2008/2009.
Pensionable pay has reduced in 2010/2011as the effect of this backdating has sessionalpayments
Mr T Hunt received no pension from hisemployment with the Trust during2010/2011.
Staff recognised for their hard work and dedication at the Annual Awards Ceremony
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 128

129Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Events after the end of the Reporting PeriodThe Trust is in the process of acquiringCDDCHS which due to its turnover relative to CDDFT’s requires the Trust to submit theproposal to Monitor’s risk evaluation process,the outcome of which is expected in earlyMay, following a board to board meeting on4th May. In the interim, CDDFT has signed acontract with NHS County Durham to providecommunity health services for a period of 3months commencing on 1 April 2011, in theexpectation that Monitor’s risk rating will besuch as to enable the board to approve thetransaction on a permanent basis.
The impact of the transaction is expected to increase annual turnover by c£120m and to increase its asset base by £1.1m
Related Party TransactionsCounty Durham and Darlington NHSFoundation Trust is a body corporateestablished by order of the Secretary of State for Health.
During the year there were transactionsbetween parties related to two of the Board Members and County Durham and Darlington NHS Foundation Trust, the values of which are listed below:
Payments to Receipts from Amounts owed Amounts dueRelated Party Related Party to Related Party from Related Party
£ - p £ - p £ - p £ - p
Board Members
Ms K Larkin-Bramley - 136,549 60,738 0 417Non Executive Director
Mrs S Jacques - Chief Operating 6,574 0 0 0Officer and Director of Finance
143,123 60,738 0 417
Ms K Larkin-Bramley is a tutor at Durham University and an Independent member of the Police Authority. The amountsshown are receipts and payments to both organisations.
Mrs S Jacques is a director of the Healthcare Financial Management Association and payments relate to their programmemembership and various training events.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 129

130 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
We have examined the summaryfinancial statement of County Durhamand Darlington NHS Foundation Trustfor the year ended 31 March 2011 whichcomprises primary financial statementssuch as the Statement of ComprehensiveIncome, the Statement of FinancialPosition, the Cash Flow Statement, theStatement of Changes in TaxpayersEquity and the related notes.
This report is made solely to the Board ofGovernors and Board of Directors (“theBoards”) of County Durham and DarlingtonFoundation Trust, as a body, in accordancewith paragraph 4 of Schedule 10 of theNational Health Service Act 2006. Our auditwork has been undertaken so that we mightstate to the Boards those matters we arerequired to state to them in an auditors’report and for no other purpose. To thefullest extent permitted by law, we do not, in giving our opinion, accept or assumeresponsibility to anyone other than the Trustand the Boards, as a body, for this report, or for the opinions we have formed.
Respective responsibilities ofdirectors and auditorsThe directors are responsible for preparingthe Annual Report. Our responsibility is toreport to you our opinion on the consistencyof the summary financial statements withinthe Annual Report with the statutory
financial statements. We also read the otherinformation contained in the Annual Reportas described in the content section andconsider the implications for our report if we become aware of any misstatements ormaterial inconsistencies with the summaryfinancial statements.
Basis of opinionWe conducted our work in accordance withBulletin 2008/3 ‘The auditor’s statement on the summary financial statement in theUnited Kingdom’ issued by the AuditingPractices Board. Our report on the statutoryfinancial statements describes the basis ofour audit opinion on those financialstatements.
OpinionIn our opinion the summary financialstatements are consistent with the statutoryfinancial statements of the Trust for the yearended 31 March 2011.
Paul Thomson (Senior Statutory Auditor)For on and behalf of Deloitte LLPLeeds, UK
Independent Auditor’s Report to the Board ofGovernors and Board of Directors of CountyDurham and Darlington NHS Foundation Trust
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 130
131Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Glossary of Terms
Accident and Emergency (A&E) - hospitaldepartment that assesses and treats people withserious injuries and those in need of emergencytreatment (also known as Emergency Departments).
Acute – describes a disease of rapid onset, severesymptoms and brief duration.
Agenda for Change (AfC) – NHS system of paythat reflects job content, and the skills andknowledge of staff.
Benchmarking – process that helps professionals totake a structured approach to the development ofbest practice.
BME – Abbreviation used to refer to Black andMinority Ethnic groups
Board of Directors – the powers of a trust areexercised by the Board of Directors. In a foundationtrust, the Board of Directors is accountable togovernors for the performance of the trust.
CDDFT – County Durham and Darlington NHSFoundation Trust
CHKS Limited – a private company which providescomparative information on the NHS.
Care Quality Commission (CQC) – theindependent regulator of health and social care inEngland.
Clostridium Difficle (C.Difficile or CDIFF) – ahealth care associated intestinal infection that mostlyaffects elderly patients with underlying diseases.
Commissioning for Quality and Innovation(CQUIN) – a payment framework developed toensure that a proportion of a providers’ income isdetermined by their work towards quality andinnovation.
Community based health services – servicesprovided outside of a hospital setting, usually inclinics, surgeries or in the patient’s own home.
Community hospitals - local hospitals providing arange of clinical services.
DH – Abbreviation used for the Department ofHealth
ED – Abbreviation used for Emergency Department
Foundation Trust (FT) – NHS hospitals that are runas independent public benefit corporations and arecontrolled and run locally.
Freedom of Information Act (FOI) – legislationgiving a general right of access to information heldby public authorities.
Healthcare Associated Infection (HCAI) –infections such as MRSA or Clostridium Difficile thatpatients or health workers may acquire from ahealthcare environment such as a hospital or carehome.
HDU – Abbreviation used for a High DependencyUnit
IR1s – Abbreviation used for Incident ReportingProcess in the Trust
Infection Control – the practices used to preventthe spread of communicable diseases.
Intensive Therapy Unit (ITU) – specialised hospitaldepartment delivering life support therapies topatients who are critically ill.
LINKs - Local Involvement Networks
Methicillin-Resistant Staphyloccus Aureus(MRSA) – bacterium responsible for several difficultto treat infections.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 131

132 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
MHRA – Medicines in Healthcare ProductsRegulatory Agency, a government agency withresponsibility for standards of safety quality andperformance.
Monitor – the independent regulator of NHSfoundation trusts that is responsible for authorising,monitoring and regulating them.
National tariff (tariff) – centrally agreed list ofprices for particular procedures; linked to thePayment by Results policy.
NCEPOD - National Confidential Enquiry into PatientOutcome and Death
NHSCDD - NHS County Durham and Darlington
NHS Constitution – establishes the principles andvalues of the NHS. It sets out the rights andresponsibilities of public, patients and staff to ensurethat the NHS operates fairly and effectively.
NIHR – National Institute for Health Research.
Non-Executive Directors (NEDs) of foundationtrusts – lay people appointed by the Governors tosit on the Board of Directors. The Chair of thefoundation trust will be a Non-Executive Director.
NPSA - National Patient Safety Agency
NRES – National Research Ethics Service
OSC - Overview and Scrutiny Committee
Quality, Innovation, Productivity andPrevention (QIPP) – a framework adopted by theNHS to deliver quality and efficiency improvements.
Patient Advice and Liaison Services (PALS) –services that provide information, advice and supportt help patients, families and their carers.
PAS - Patient Administration System
PBR - Payment by Results
Payment by Results (PbR) – the rules based systemused for paying trusts that links the allocation of fundsto hospitals to the activity they undertake.
PPI - Patient and Public Involvement
Practice-based commissioning (PBC) – governmentpolicy designed to give GPs, nurses and other primarycare professionals the power to decide how NHSfunds are spent.
Primary care – the collective term for family healthservices that are usually the patient’s first point ofcontact with the NHS; includes general medical anddental practices, community pharmacy andoptometry.
Primary Care Trusts (PCTs) – NHS bodies responsiblefor the planning and securing of health services in alocal area.
QIPP - Quality, Innovation, Productivity and Prevention
RfPB – Research for Patient Benefit, a nationalprogramme to generate high quality clinical research.
Secondary care – care provided in hospitals.
SMR - Standard Mortality Rate
Standardised Mortality Ratio – the number ofdeaths in a given year as a percentage of thoseexpected.
Strategic Health Authorities (SHAs) – regionalauthorities tasked with providing strategicmanagement support to primary care trusts andhospitals as they improve and develop their services.
UKCRN – United Kingdom Clinical Research Network.
UTI - Urinary Tract Infection
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 132

133Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
Contact the Trust Secretary at the address, emailor telephone numbers listed below forinformation about the Board of Directors or theGoverning Council or if you would like to:
• become a member of the County Durhamand Darlington NHS Foundation Trust;
• view the register of Directors’ or Governors’interests;
• contact the Chairman or a member of theBoard Directors or one of the Governors;
• receive detailed information about those ofour Board of Directors’ meetings which areopen to the public;
• receive detailed information about theGoverning Council meetings which are opento the public. Details of all our publicmeetings are displayed within the Trust’shospitals and are published on the Trust’swebsite;
• receive further copies of this report.
Write to: Foundation Trust Office County Durham and Darlington NHS Foundation TrustExecutive CorridorDarlington Memorial HospitalHollyhurst RoadDarlingtonDL3 6HX
Telephone: 01325 743 625Email: [email protected]: www.cddft.nhs.uk
How to find out more
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 133

134 Annual Report and Summary Financial Statements 1 April 2010 – 31 March 2011
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
................................................................................................................................................................................
Notes
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 134

This report is also available, on request,in alternative languages and formatsincluding large print and Braille.
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 135

County Durham and Darlington NHS Foundation TrustTrust HeadquartersDarlington Memorial HospitalHollyhurst RoadDarlingtonCounty DurhamDL3 6HXSwitchboard: 01325 380 100Email: [email protected]: www.cddft.nhs.uk
Quality Care Respect
County Durham and DarlingtonNHS Foundation Trust
32868_AR_Public_32868_AR_Public 30/06/2011 15:00 Page 136









![SUMMARY OF FINANCIAL STATEMENTS [IFRS ...SUMMARY OF FINANCIAL STATEMENTS [IFRS] (CONSOLIDATED) Financial Results for the Fiscal Year Ended March 31, 2014 May 8, 2014 Takeda Pharmaceutical](https://static.fdocuments.in/doc/165x107/5ece4cbfb1af104f892b6602/summary-of-financial-statements-ifrs-summary-of-financial-statements-ifrs.jpg)








