ANNUAL REPORT 2005 - 06€¦ · 2 Annual Report 2005-06 Contents

Annual Report2005-2006
Annual Report2005-2006
Annual Report2005-2006
Annual Report2005-2006

The Annual Report is an opportunity to take stock of theachievements of the last year and look forward to theimprovements we will be making for our patients and staff,without whom there would be no hospital service.Over the last year we have been concentrating on furtherreducing waiting times for our patients and as such we arenow one of the best performing hospitals in the WestMidlands for fast access to emergency care.
The hospital is also aiming to make further improvementsin service by reviewing processes in all hospitaldepartments. More details of these improvements arecontained within the report, together with our plans forthe year ahead.
2006 is a particularly exciting year for the Trust as due tomeeting all of the key NHS standards for the care ourpatients receive and our track record of balancing thebooks, we are able to apply for Foundation Trust status.NHS Foundation Trusts are a new kind of organization,remaining part of the NHS whilst being run locally and moreclearly accountable to patients and the public.
Our aim is to continue to provide and develop excellentservices that are local and sustainable. We will faceincreasing competition from within and outside the NHSand believe that by becoming an NHS Foundation Trust wewill be able to build on our current strength whilst alsohaving the flexibility to meet the challenges and graspopportunities.
Being a Foundation Trust will enable us to:
• Deliver improvements in patient care by having thefreedom to make all our decisions locally
• Be more accountable by consulting with local people onkey decisions affecting the hospital
• Strengthen our links with the community , developing aculture of involvement by building a firm membershipbase representative of the people we serve
• Use our finances more flexibly to improve patient care
• Attract and retain high quality staff by being able toprovide unrivalled benefits and working environment
Whether you are reading this as a patient, member of staffor indeed a member of the public interested in your localhospital, we hope you will continue to support the hospitaland our plans for the future. We are keen to ensure thatHereford County Hospital continues to provide high qualityhealthcare for the people of Herefordshire and thesurrounding areas and need your support and feedback tobe able to do so.
We would like to pay tribute to the effort, dedication andcare shown by all those working at the hospital, whetherthey are hospital staff, volunteers or support staff. We allwork under a great deal of pressure to ensure we candeliver the standards required and in our capacity asChairman and Chief Executive we wish to congratulate thehospital team for their drive and commitment in achievingmarked service improvements in addition to maintainingthese standards. Well done to all and we look forward tothe year ahead.
2
A few words from the Chairman and Chief Executive
Cessa Moore David RoseChairman Chief Executive
Our vision:As an aspiring Foundation Trust hospital,
“Our vision is excellence in the delivery of hospitaland integrated healthcare services to our localpopulation through partnership with patients, thepublic and other organizations”.
To achieve this we will:
• Provide high quality , innovative and mostimportantly, patient centered services
• Ensure that as a result of our reputation forquality, patients and healthcare commissioners(GP’s) continue to choose our services
• Be an employer of choice in the county

About the TrustHerefordshire is predominantly a rural county of 842 squaremiles in the south-west corner of the West Midlands regionbordering Wales. Hereford Hospital NHS Trust is the mainacute service provider across Herefordshire and works inclose partnership with 5 community hospitals (4 of whichprovide Minor Injury Units) managed by HerefordshirePrimary Care Trust (PCT).
The Trust provides the majority of health services for acatchment population of 230,000, the majority of whomare resident within Herefordshire (170,000) and the balancemainly in Mid-Powys and North and East Monmouthshire.
The Trust has operated from a new PFI build since 2002with 23 years left to run on the scheme. Turnover(2005/06) was £85m, with a bed compliment of 314.
Main services provided at Hereford Hospital NHS Trust are:A&E, Geriatric Medicine, Cardiology, Respiratory Medicine,Dermatology, Diabetic Medicine, Ear Nose and Throat,Gastroenterology, General Medicine, General Surgery,Gynaecology, Haematology, Neurology, Obstetrics,Oncology, Ophthalmology, Oral Surgery, Orthodontics,Paediatrics, Palliative Medicine, Plastic Surgery,Rheumatology, SCBU, T&O, Urology.
Hereford Primary Care Trust (PCT)The Trust’s principal relationship is with HerefordshirePCT, which not only commissions healthcare on behalfof patients but also provides a range of communityservices which interface closely with those provided bythe Trust.
Herefordshire PCT has invested significantly in the Trustin recent years, both to enable continued delivery
against targets and to strengthen key services likecardiology, respiratory medicine and diabetology.
The PCT has supported the introduction of practicebased commissioning, a key challenge for 2006/07being new measures to curtail the growth in demandfor emergency services.
Powys Local Health Board (LHB)The Trust’s second most significant relationship is withPowys Local Health Board, which commissions servicesfrom the Trust for residents living in the south and eastof the county. Consultants from the Trust also provideout patient clinics and minor surgery sessions in anumber of community hospitals in Powys.
Clinical PartnershipsThe Trust has well established arrangements to supportclinical specialities that would otherwise not be viablein a local district general hospital. University HospitalBirmingham NHS Foundation Trust provides regularoutpatient consultant clinics for a range of specialitiesincluding: Neurology, Nephrology and Cardio Thoracicsurgery. Joint services with Worcester Acute Trust arealso well established in vascular surgery, ENT and Oralsurgery.
The Trust also provides on-site Cancer services inpartnership with Gloucestershire Hospitals FoundationNHS Trust as part of the Three Counties CancerNetwork.
3
About the Trust and our Partners

The table below demonstrates the Trust’s track recordin achieving key national targets. The Trust has metand exceeded national access targets for several yearsand has been an exemplar site for cancer waits.
Description KPI 2003/04 2004/05 2005/06
Patients with suspected 100% 99% 99.9%cancer seen within 2 weeks
Elective patients waiting Nil over Nil over Nil over longer than standard 12 months 9 months 6 months
Outpatient waiting longer Nil over Nil over Nil overthan the standard 21 weeks 17 weeks 13 weeks
Total time in A&E: four hours or less 90% 98% 98%
Outpatient & elective booking 67% 86.6% 100%
Cancer waiting time from N/A N/A 100%decision to Treat (31 days)
Total cancer waiting time from N/A N/A 89% referral to treatment (62 days)
The Trust expects to achieve compliant performanceagainst the Healthcare Commission’s AnnualHealthcheck for 2005-06 and forecasts continuedcompliance over the next five years.
The Trust complies with the requirements of the NHSnational information system enhancements andimplementation programme (known as NPfIT). Clinicaladvancements and improvements are constantlyoccurring in departments such as Radiology, Pathology,Anesthetics and Oncology.
Number of patients treatedThe table below highlights the profile of the Trust’sactivity over the last three years and in particular theunprecedented level of growth in 2005/06.
Activity 2004/05 2005/06 Increase 05/06on 04/05
%
Elective Spells 4,350 4,960 +14%
Day Case Spells 9,070 9,130 +1%
Emergency Spells 16,160 17,870 +11%
Outpatient Attendances 108,440 122,750 +13%
A & E Attendances 41,400 44,400 +7%
4
Our performance
Improving Performance in the Future In preparation for Foundation Trust status, the Trust isworking on its future development plans, takingaccount of the impact of Practice BasedCommissioning, independent sector competition andpatient choice:
• Opportunities have been identified to work inpartnership with the private and voluntary sectors,contest services outside the hospital, do more workfor Welsh commissioners and improve operationalefficiency
• The Trust has drafted its Service Development Plansto reflect 8 key themes. Detailed plans underpinnedby Business Cases for each proposal will bedeveloped by September 2006
• The Trust has developed a clear estates strategyfocused on maximising the utilisation of the mainPFI hospital and reducing reliance on the liability ofthe retained estate
• A detailed capital investment plan to supportdelivery of individual Service Development plans willbe developed by September 2006
• The Trust’s IT strategy is well defined andunderpinned by clear plans to develop both clinicaland business systems

There have been many developments in Cancer servicesat HHT over the last year which will improve patientcare.
Technological achievements have been key to recentsuccesses, a key development being the chemotherapyscheduler. This electronic scheduler replaces a paper-based system to schedule chemotherapy and pre-chemotherapy assessment appointments. The mainbenefit being more effective management ofappointments, helping staff improve patientthroughput and enabling more people to be treated atHereford who would otherwise have to travel toCheltenham.
The scheduler has been designed by Nick Exon, ServiceImprovement Facilitator, and many improvements havebeen added thanks to the active involvement ofchemotherapy nurses and pharmacy staff. Dr LisaRobinson commented
“This is a great achievement and ALL the staff involvedshould feel very proud.”
Peter Davies (lead cancer nurse) stated “theinvolvement of service improvement staff alongsideclinical staff facilitated effective innovation that willgreatly improve patient care. Congratulations to allinvolved”
The Trust is delighted to welcome 2 new clinicaloncologists, Dr Sam Guglani and Dr Nick Reed to theteam at the Charles Renton Unit. They are bothclinical oncologists based at Cheltenham. Samspecialises in breast cancer and brain tumours andNick specialises in the gastrointestinal tract and lungcancers. The great news for patients is that they areboth young, dynamic and highly motivated. Theirappointment has enabled HHT to offer a wider rangeof cytotoxic treatments as well as further additional
treatments. They have already shown themselves tobe excellent team players, focused on providing thebest care possible for patients.
Planned Developments We are working togetherwith Macmillan CancerSupport to raise funds fora new build cancer unithere on site. This decisionfollows 18 months ofdetailed preparatory workby the Trust and Macmillan,who are keen to worktogether to improve cancerservices in Herefordshire.
David Rose, Chief Executive, stated “This is fantasticnews for the hospital and we are delighted to beworking together with Macmillan Cancer Support on aproject which will make a huge difference to localpeople”.
The new unit will offer superb facilities for thediagnosis, treatment and support of local cancerpatients and will also allow the majority of patients toreceive chemotherapy treatment on site, preventinglengthy travels to the Cancer Centre at Cheltenham.
It is anticipated that local fund raising, commencing inJune 2006, will take in the order of 18 months to 2years and that the build will be completed within thistime schedule or shortly afterwards. The site for thebuild is yet to be finalized but it is hoped that it will bein close proximity to the PFI build to allow greatercollaboration of linked services.
5
Cancer services

Geriatric MedicineOrthogeriatrics A new service currently is being developed to improvecare received by older people. All frail elderly patientsadmitted under the orthopaedic surgeons are assessedpre and post operatively to optimise medicalconditions with consultant lead from Dr Alner. Thisincludes comprehensive medical assessment, fallsassessment, rehabilitation and osteoporosis treatmentby the multidisciplinary team to minimise risk for olderpeople.
Falls service – We have gone green!The Hospital now has its own dedicated fallsprevention programme aimed at preventing andreducing falls by improving balance and advisingpeople about safety, particularly at home. Patientsundergo multidisciplinary assessment based on NICEguidelines to identify and treat risk factors for falls.Patients “at risk” of falling are now identified withGreen Wristbands. Staff are extra vigilant whendealing with these patients and additional precautionsare taken to prevent falls.
PathologyThis year the pathology team have used some simpleapproaches to improve the turnaround times for testresults. This has helped improve dischargearrangements and further reduce length of stay.Working together with the hospital “ServiceImprovement Team”, the “Lean approach” has beenused in the department leading to:• Reduced time taken to get results back on blood
tests by 40% with no extra resources• Quicker patient discharge• Improved staff productivity and motivation
No extra money was used to implement these changes
Lean is an approach used by world class companieslike Tesco and Toyota to improve flow and eliminatewaste in their processes. It is increasingly being appliedto healthcare. More Lean improvements will beimplemented throughout the hospital over the nextyear, improving patient flow, reducing waste andhelping to lower costs whilst improving the quality ofcare.
6
Service improvements

Developments in DiabetesWe are particularly proud of the Diabetes service atHereford Hospital NHS Trust, which continues todevelop from strength to strength. One of the serviceimprovements is the introduction of Insulin PumpTherapy over the last 6 months. This improves qualityof life for patients by reducing the number ofinjections necessary.
The Diabetes service has also been complemented withnew appointments to the team, a new in-patientDiabetes Specialist Nurse has been appointed, togetherwith a second Consultant Diabetologist, due to start inOctober 06. The latter will be undertaking communitysessions in conjunction with GP’s and the PCT,allowing the hospital service to concentrate on treatingpatients with more complex needs.
The Paediatric Diabetes Specialist Nurse service has alsoexpanded. The Paediatric Diabetes Nurs specialist willbecome full time from the beginning of September2006. This will help to deal with the increasingnumber of young people with diabetes and providebetter education and support for them and theirfamilies.
The Diabetes eye screening service will also beintroduced in summer 2006 for all adolescents over 12to apply with NICE guidelines.
The Diabetes team are also involved in the expertPatient Education Programme (Diabetes nurse) and areworking with Trust and PCT colleagues to implementthe government’s National Service Framework forDiabetes.
RadiologyDuring the last year the Radiology department havecontinued to focus on improving and modernisingservices and the experience for patients and users.Achievements include,
• Desktop x-ray and imaging reports now availabledirectly to GPs and Community hospitals, followingthe roll out of the Radiology Information ComputerSystem into the Community.
• Improving patient access to MRI and CT diagnostictests (this work went on to form the pilotdemonstrator site case study as part of the NationalCancer Waits Project 2005/06).
• Continuing with our plans to modernise radiologyappointments and bookings, which included asuccessful pilot study for direct “open access”ultrasound examinations for patients.
• Working in partnership with the cardiology team toachieve significant reductions in waiting times fornuclear cardiology imaging tests.
In October 2005 we also welcomed Michael O'Connorto the department, Senior Improvement Consultantworking at the Juran Institute in USA, an expert inunderstanding systems and improving processperformance. Radiology shall continue to focus onways to improve the service for patients and staff andreduce waiting times.
Significant reductions in waiting times for manyimaging examinations over the last year, is a credit toall the improvement work already implemented bystaff.
7
Developments

Car Parking – Pay-on–FootDuring 2005 plans were put in place to launch thenew Pay on Foot system in July 06. This is to improveparking for our patients and visitors, key benefitsbeing:
• Drivers will pay for the time they use rather thanbeing encouraged to use the time they have paid for
• Those not visiting the hospital are discouraged fromusing the car park
• Increase turnover of spaces
• Improved traffic flow
• Improved driver and pedestrian safety.
The Trust, in negotiation with its service provider,Sodexho, and with Controlled Parking Plus, hasendeavored to keep the cost of parking to anacceptable level. The new arrangements (and tariffs)are designed to make “long-term” parking on theHospital site unattractive to city-centre workers andshoppers, relative to other public car parking optionsnearby. However, the Trust does not wish to penaliselong-stay patients and visitors so as such concessionsare available.
This scheme is not about creating an income for theTrust, it is part of our response to meeting patients’needs, balanced with our commitment to operate in aresponsible manner in respect of the environment.
We will continue to look at other alternatives todevelop more integrated travel arrangements with ourLocal Authority colleagues and public transportproviders. In addition as we develop additional oralternative options for our staff, who also need to beconsidered within the overall plan, furtherimprovements to visitor parking may also be possible.
HHT – Smoke Free!The Department of Health seeks to promote a smoke-free NHS and the British Medical Association haspressed for a ban on smoking in public places, whichincludes NHS premises. Evidence on the detrimentaleffects of smoking on the health of smokers and onpeople exposed to second-hand smoke (i.e. ‘passivesmokers’) is widely available and as such the Trust tookthe decision to go completely smoke free throughoutall of its premises from 3rd April 2006.
“Hereford Hospitals NHS Trust has a responsibility tothe patients or clients it provides care to, its staff andto all people visiting its premises for any purpose, toprovide a safe and healthy environment.”
We are constantly seeking ways to improve theenvironment for patients, staff and visitors alike andare encouraged by the support received from staff forimprovement initiatives.
8
Site improvements

There are now 3 Matrons at Hereford Hospital NHSTrust, fully committed to improving the patientexperience. As such, Matrons focus on key issues ofdirect importance to patients, such as:
Protected Meal TimesThis principle was introduced in April 2005 to ensurethat patients meals are not interrupted and thatpatients are allowed times to rest and receivetreatment. It has been a success with patients andstaff alike.
CleanlinessCleanliness is a priority at Hereford Hospital NHS Trust.We are consistently looking at ways to improvecleanliness on the wards, in turn improving the qualityof care for patients. Visitors are encouraged toconsider the following guidelines:• Please do not sit or lie on patients’ beds, use the
chairs provided.
• Children should be discouraged from crawling onthe floor and must be supervised at all times.
• Please talk to the ward staff if you have concernsabout the cleanliness of the environment.
Infection ControlWe have a dedicated Infection Control team at thehospital who focus on reducing infections within the
Trust. Consequently, cases of hospital acquired MRSAhave reduced over the last year and the introduction ofalcohol based gel at the ward entrances is provingeffective. Infection Control is everyones responsibility.Visitors are encouraged to:
• Always use the alcohol gel provided or carefullywash hands with facilities provided. The mosteffective way to protect patients and yourselves is touse the alcohol gel provided when entering andleaving the ward.
• Never touch patients’ wounds, drips, tubes etc. Ifyou do so accidentally, please wash your handsimmediately.
• If you are visiting more than one patient, pleaseperform hand hygiene in between them and visitnon-infectious patients first.
It is hoped that through working together to achievethe same high standards we can make the hospital abetter place for patients, staff and visitors alike.
9
Message from the matrons
Ethnic Origins Staff In Post as at 31 March 2006
156
12 4 15 4 1 5 1 1 4 1 28 3 2
1508
2 26
0
200
400
600
800
1000
1200
1400
1600
Asian Bangladeshi/BritB
an
Asian Indian/Brit
Indian
Asian Other
Asian Pakistani/Brit
Pak
Black African
Black Caribbean
Black Other
Chinese
Mixed Other
Mixed White
/Asian
Mixed White
/Blk African
Mixed White
/Blk Caribbean
Not Stated
Other Specifie
d
Other Stated Orig
in
White Briti
sh/Mxd British
White Iri
sh
White Other
Ethnic Origins
Numb
er of
Staf
f
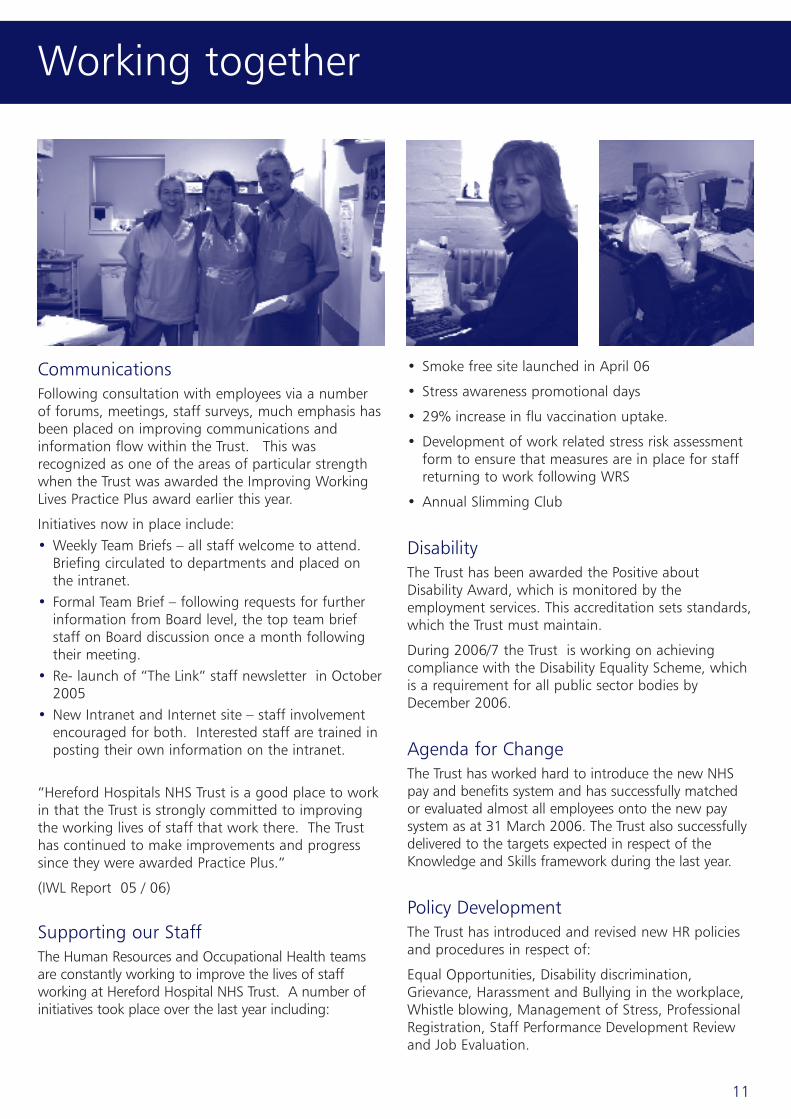
As at 31 January 2006 the Trust employed 1,686 staffequating to 1,357 WTE.
The increase in staff over the last 3 years reflects:
• The additional resources that have been allocated inline with the NHS Plan to develop improved servicesfor patient care. (DOH 2000)
• Commitment to reduce our reliance on Agency andBank staff
• Bed and Ward closure plans suspended andtherefore corresponding additional staff numbersrequired
• Requirement to increase staffing numbers torespond the New Deal for Junior Doctors Initiativeand working towards the European Working TimeDirective 2009
• The number of doctors working in the trust hasincreased in the last year
• The number of nurses working in the trust hasincreased in the last year
• The number of other support roles aligned to carehas remained overall relatively static
Ethnic OriginsThe Trust is participating in a number of initiatives toimprove the employment experience of Black andMinority Ethnic groups (BME):
• Working jointly with other public sector bodies onthe employment aspects of the Race RelationsScheme.
• Establishing a BME network group across the healtheconomy in Herefordshire (inaugural meeting Sept.2006).
• The Professional Development Department providesdiversity training, support for the BME forum andEquality Impact Assessment training and ongoingmonitoring.
• An Equality of Opportunity Policy is being reviewedin 2006/7, which will cover Managing Diversity.
We do not currently have representation from anyethnic minorities in senior management positions andactions within the BME groups will assess whatmeasures can be put in place to address this issue.
10
Our staff
Ethnic OriginsStaff In Post as at 31 March 2006
CommunicationsFollowing consultation with employees via a numberof forums, meetings, staff surveys, much emphasis hasbeen placed on improving communications andinformation flow within the Trust. This wasrecognized as one of the areas of particular strengthwhen the Trust was awarded the Improving WorkingLives Practice Plus award earlier this year.
Initiatives now in place include:• Weekly Team Briefs – all staff welcome to attend.
Briefing circulated to departments and placed onthe intranet.
• Formal Team Brief – following requests for furtherinformation from Board level, the top team briefstaff on Board discussion once a month followingtheir meeting.
• Re- launch of “The Link” staff newsletter in October2005
• New Intranet and Internet site – staff involvementencouraged for both. Interested staff are trained inposting their own information on the intranet.
“Hereford Hospitals NHS Trust is a good place to workin that the Trust is strongly committed to improvingthe working lives of staff that work there. The Trusthas continued to make improvements and progresssince they were awarded Practice Plus.”
(IWL Report 05 / 06)
Supporting our StaffThe Human Resources and Occupational Health teamsare constantly working to improve the lives of staffworking at Hereford Hospital NHS Trust. A number ofinitiatives took place over the last year including:
• Smoke free site launched in April 06
• Stress awareness promotional days
• 29% increase in flu vaccination uptake.
• Development of work related stress risk assessmentform to ensure that measures are in place for staffreturning to work following WRS
• Annual Slimming Club
DisabilityThe Trust has been awarded the Positive aboutDisability Award, which is monitored by theemployment services. This accreditation sets standards,which the Trust must maintain.
During 2006/7 the Trust is working on achievingcompliance with the Disability Equality Scheme, whichis a requirement for all public sector bodies byDecember 2006.
Agenda for ChangeThe Trust has worked hard to introduce the new NHSpay and benefits system and has successfully matchedor evaluated almost all employees onto the new paysystem as at 31 March 2006. The Trust also successfullydelivered to the targets expected in respect of theKnowledge and Skills framework during the last year.
Policy DevelopmentThe Trust has introduced and revised new HR policiesand procedures in respect of:
Equal Opportunities, Disability discrimination,Grievance, Harassment and Bullying in the workplace,Whistle blowing, Management of Stress, ProfessionalRegistration, Staff Performance Development Reviewand Job Evaluation.
11
Working together

In order to continue to provide the right balance ofservices for our patients and in order to keep up withdevelopments in healthcare provision, it is key for us toregularly look at the demands placed on our servicesby our patients. As a result of doing this we haveobserved the following:
• We will continue to treat patients from Wales andtherefore need to keep in touch with the needs ofWelsh patients and the views of their Local HealthBoard, who will continue to provide funds for theWelsh patients which we treat.
• Herefordshire already has a proportionately largeelderly population and we must continue to monitorgrowth of this population. Particular attention mustbe paid to the predicted increase in the +85population over the next 10-15 years, which is likelyto have a significant impact on the demand for theTrust’s services.
• In view of many advancements in medicaltechnology, the Trust needs to plan for investmentsin new equipment / techniques in order to keeppace with best practice
• The Trust needs to focus on recruiting effectively,building relationships with local schools and collegesand trying to illustrate to young people the range ofopportunities for development there are at the Trust.
• The Trust also needs to be aware of the continuedand significant influx of migrant workers to
Herefordshire, particularly as some of thispopulation choose to stay in the County on a morepermanent basis.
• Taking all of the above into consideration, the Trustwill need to focus increasingly on making sure theservices we provide are clinically effective, managingfunds effectively in order to continue to providethem.
In an environment of patient choice, where patientsare increasingly able to chose where they receivetreatment, subject to the necessary services beingavailable, the Trust needs to ensure that we continueto provide the best service possible in the area. Weare keen to ensure that Hereford County Hospital is“the provider of choice” for healthcare in the County.Our dedicated team of staff and partnerorganisations are constantly striving to maintain thehigh standards that make this possible. We alsoneed to ensure that:
• GP’s support the services we provide and are keenfor their patients to come to Hereford
• We work closely with Powys Local Health Board tocontinue to treat Welsh patients
• Diagnostic Services are developed
• Non-Clinical Services are offered
• We work together to retain the provision ofCommunity Hospitals
12
Demand for our services
1 We will be responsive to thebalance of views of patients, thepublic, GPs and other stakeholdersas we seek to develop our servicesand to attract more patients touse them, leading to:
• A 15% increase in patients over 5 years
• Minimum 1.3% increase in elective patients whochose to come to the hospital each year
• GP’s, patients and other organizations continuing tosupport the work of the hospital
• Including the views of often “hard to reach” groupsin our development plans
2 We will ensure consistentapplication of best clinical practicein the care and treatment weprovide to patients, developingactive clinical partnerships whereappropriate through:
• 100% implementation of audited recommendationsof NICE and NCEPOD
• Consistent compliance with the core Standards forBetter Health
• Adopting new technology where appropriate toensure safe and effective care
• Achieving year on year reductions in the incidenceof hospital acquired infections
• Reducing emergency admissions by 1% from2008/09, supported by active partnership workingto manage appropriate patients with long termconditions in their homes
• 8% of our staff working under long-term contractarrangements with a range of health and social careand independent sector organisations.
3 We will be flexible in where weprovide care ensuring services areeasily accessible, safe, reliable and
affordable and make a significantcontribution to reducing healthinequalities and improving thequality of life for our local citizens,ensuring that:
• All services meet and exceed Government accesstargets, including the 18 week maximum wait fromreferral to treatment by 2008
• Increased proportion of out patient and day caseservices provided in a primary care or communitysetting
• The number of patients readmitted to hospital isreduced from the current level of 7.85% to less than5% within 5 years
• At least 40% of patients leave the hospital with aHealthy Living Plan;
4 We will build a reputation as anexcellent employer, ensuring that:
• Staff from within the local economy activelyrecruited retained and developed
• Level attained above Improving Working LivesPractice Plus (yet to be announced)
• Sickness rate reduced to less than 3% within 2 yearsand sustained at that level
• Proportion of employees aged between 18 and 24increased from 5% to 10% within 3 years
5 We will continually improve theproductivity and cost effectivenessof our services, achieving:
• Financial surplus of 1% of turnover by 2009/10
• Average length of stay for non elective adultadmissions reduced by 1 day by 2008/09
• Bed complement reduced by between 5-10% by2008
• Year on year reductions achieved in the unit cost perbed
13
Principal objectives

Risk Management ArrangementsKey risks are identified by the Trust and categorisedinto Strategic; Operational; Financial; InformationTechnology and Human Resources risk areas. Theserisks are assessed in terms of their impact on achievingthe overall business plan.
Potential ‘showstoppers’ include: the effect of externalcompetition; potential repatriation of activity to Wales;continuing pressures on emergency activity and failureto achieve productivity and cost improvement gains.
In practice, the key risks facing the organisation arerecorded in the Trust’s Risk Register with those deemedto be strategic (and therefore potentially impacting ondelivery of corporate objectives) also identified in theTrust Assurance Framework. Individual service oroperational risks are managed at CareGroup/departmental level and monitored throughquarterly performance reviews whilst high levelstrategic risks are tracked and managed by the TrustBoard.
Major Incident Plan (MIP)The Trust is currently undertaking a review of its MIP toensure full compliance with Department of HealthEmergency Planning guidance issued in 2005. Thereview will be completed by the autumn of 2006.
EnvironmentThe Trust has an Environmental Policy adoptedDecember 2004 but no formal Social and Community
policy. The Trust acknowledges that the protectionand enhancement of the environment is of importanceto assist patients' recovery and we recognise our role inprotecting the environment of our local community.
The County Hospital was built as part of the PrivateFinance Initiative (PFI) and the Trust and our PFIpartners are committed to improve the environmentalperformance of the organisation, to eliminate orreduce pollution and to comply with all legislation,present and future that will impact upon theenvironmental position of the Trust.
AuditThe Audit Commission is the Trust's external auditor.The audit fee for the year amounted to £118,500 ofwhich £40,900 was in respect of national use ofresource initiative reviews required by the Departmentof Health; Audit Local Evaluation (ALE), Payments byResults implementation, Emergency Admissions andConsultant Contracts .No non-audit services wereprovided.
The Audit Committee is chaired by Mr Mark Curtis;other Non -Executive members are Mrs CarolineBrown, Mr Sebastian Bowen, Mr Stephan Ludwig andMrs Joanna Whitlock.
Statement of Internal ControlThis can be found on the Trust Website, together withother key Trust documents.
14
Public interest and other

The Remuneration Committee is a formal committee ofthe Trust Board composed of all Non-ExecutiveDirectors with the Chief Executive in attendance asappropriate.
The Committee is responsible to the Board for theremuneration of the Chief Executive and ExecutiveDirectors. However, the Chief Executive is not part ofthe meeting when the Chief Executive’s remunerationis discussed.
The Chairman of the Committee is the Chairman of theBoard, with secretarial support provided by the TrustSecretary.
The key purpose of the committee is to review thereward structure of the Chief Executive and ExecutiveDirectors. Although there is no formal remunerationpolicy, Directors’ salaries and benefits are decided afterconsideration of market forces, performance andindividual contribution based upon the advice andrecommendations of the Chief Executive.
The Chief Executive and Executive Directors arepermanent employees, under local Trust contract termsand conditions, with three monthly notice by theDirector and six months notice by the Trust with theexception of Mr P Mogg (retired April 2005) and Mr MJohnson with six monthly notice by the Director andtwelve months notice by the Trust. There are noarrangements for additional performance relatedpayments.
In the event of an early contract termination by theTrust Directors are eligible for full payment in respectof the Trust notice period.
The salaries and allowances of the Chairman, ChiefExecutive, Non Executive and Executive Directors, inrespect of their work for the Trust, are given in a tablefollowing the Financial Review.
The Remuneration Committee has over the past yearundertaken the following activities:-
• Reviewed and approved the Chief Executive’sremuneration, and Executive Directors remunerationin line with cost of living increases determinednationally by the Department of Health.
• Agreed the starting salaries and approved jobdescriptions of new Executive Directors andseconded senior managers.
• Approved policies in relation to the functioning ofthe Remuneration Committee.
Mr David Rose
Chief Executive and Accounting Officer Hereford Hospitals NHS Trust
15
Remuneration report

The Trust has a good financial track record, achievingfinancial balance in 4 of the last 5 years andconsistently achieving its External Financing Limit (thelimit regulating what it can spend). However it doeshave a underlying deficit which has been bridged byone-off measures.
The Trust has a well defined financial strategy based ongenerating surpluses, improving cost effectiveness andoptimising cash-flow. The financial forecasts for thenext five years demonstrate that the Trust couldeliminate its underlying deficit by the end of 2007/08,realising surpluses from 2008/09 onwards, providedthat it delivers recurrent savings of £7.3m over thisperiod.
The key to financial success lies in consolidating clinicalservices into the main PFI hospital, enabling the huttedwards to be closed, and improving workforceproductivity. Benchmarking information illustrates thatthere is clear opportunity to improve productivitywithout impacting on patient care.
The Trust has three principal financial objectives: -
1. To generate surpluses for investment in improvinghealthcare
2. To improve the cost effectiveness and productivity ofthe Trust’s services
3. To optimise the cash flow of the organisation insupport of healthcare delivery
The financial position of the Trust is dependent on theelimination of the underlying deficit, the achievementof cost improvement/productivity programmes andthe successful introduction of Payment by Results,where each hospital is paid for every patient treated.The achievement of Foundation Trust status wouldrequire even greater financial discipline.
Accounting PoliciesThe Trust follows the Accounting Policies prescribed inthe NHS Trust Manual for Accounts.
The Trust has a 30 year agreement to provide andoperate the PFI hospital. This incorporates quarterlypayments in advance which require up frontborrowings.
The Trust pays a full-term PDC payment to theDepartment of Health based on its net relevant assets.This is currently payable based on 3.5% interest. Thisfinancial regime would change on reaching
Foundation Trust status where different borrowingrules are in place.
Eligible Trust Directors and employees are covered bythe provisions of the NHS pensions scheme which is anunfunded defined benefit scheme. It is accounted foras a defined contribution scheme and the costrepresents the contributions payable to the scheme forthe accounting period.
Significant Contractual ArrangementsIn addition to its contracts for the provision ofhealthcare services, the Trust has significant contractualarrangements with Herefordshire PCT for financialservices and IT provision, Mercia Healthcare for the PFIhospital provision and services and NHS logistics andother major NHS suppliers for clinical supplies.
Cash FlowThe optimization of cash flow is a vital component inthe work of the Finance Department which requiresdetailed daily management. The large quarterlypayment in advance of the PFI Unitary paymentrequires careful planning and the achievement ofIncome and Expenditure balance is crucial to theavoidance of cash pressures.
16
Long term objectives – financial

2005/06 was another challenging but ultimatelysuccessful year in financial terms for the Trust as wemanaged to treat the highest number of patients everwhilst still meeting our statutory financial targets. Thiswas in large part due to the skilled and prudent use ofresources by front line clinical and other staff.
The headline statutory financial achievements for theyear, which as a Trust we should rightly be proud ofwere as follows: -
• we successfully achieved a balanced Income andExpenditure position in relation to our day to dayactivities as a hospital, generating a small surplus of£2,000 ( this compares with a surplus of £20,000 in2004/05).
• we exactly hit the External Financing Limit ( in effecta cash limit for all our activities) set by Governmentof £2,062,000.
• we achieved a Capital Cost Absorption Rate ( ineffect a return on capital employed) of 2.4%. Thisfell outside the acceptable range of the officialtarget of 3.0% to 4.0% because of the late fixedasset adjustments in respect of bringing PFI schemeland and buildings onto the Trust balance sheet at31st March 2005 occurred after the 2005/06 PublicDividend Capital was arranged.
• our capital spending (i.e. expenditure on newbuildings and equipment etc) was within theGovernment set Capital Resource Limit of£3,482,000 by £433,000.
In order to fund the hospital services (secondary care) weprovide as a Trust, we secure the majority of our incomefrom NHS commissioner organisations (Primary CareTrusts in England and Local Health Boards in Wales). In2005/06, of our total income of £84,808,000,£72,921,000 came from NHS commissioners and otherIncome from Activities with the remainder being£2,798,000 funding for the Education and Training ofour staff and £9,089,000 for Other Operating Income.The chart below provides a breakdown of our incomefrom commissioners in 2005/06:
17
Financial review of 2005/2006
Income from Commissioners in 2005/2006

In 2005/06 we spent £84,324,000 on the directprovision of services, an increase of £7,296,000 or 9.5%over the previous year, reflecting the fact that withadditional funding of £2m from Herefordshire PCT wewere able significantly to continue expansion orimprovement to a range of services includingOrthopaedics, Accident and Emergency and Cardiology.As a result patients can expect to wait for a shorter timefor treatment and to receive a higher quality service.
Not surprisingly, the bulk of our day to day spendinggoes on front line services and in particular medical andnursing staff as is demonstrated in the chart above:-
During the year we were also able to commit capitalexpenditure (building construction/improvement andequipment items over £5,000) of £3,062,000, anincrease of £482,000 over the previous year. Amongstother things, this enabled us to continue therefurbishment of our Pathology laboratories and tomake a significant investment in clinical equipmentand IT for front line service areas. A breakdown of ourcapital expenditure programme is provided below:-
£KPFI Tariff – Capital Element 1,274Medical Equipment 514IT HIS development 458IT Replacement Programme 217Pathology refurbishment 208Retained Estate 158Digital Hearing Aids 105A&E Development 85Other 43TOTAL 3,062
These achievements aside, the financial experiencesand challenges of 2005/06 again sound a cautionarynote for the future because in essence we were onlyable to balance Income and Expenditure last yearthrough one off gains totaling some £2.4m (primarilythrough a debt in respect of PFI sculpted payments nolonger being required by the PCT).
Looking ahead to 2006/07 when we expect to treat aneven greater number of patients as we strive to reducewaiting times, we are estimating that we will need tofind increased operational savings through improvedefficiency of some £5.2m to achieve break even onceagain. We are presently heavily involved in thegovernance and rigorous financial diligenceconsequences arising from our bid to become aFoundation Trust in 2006/2007.
A summary of the Trust’s Annual Accounts for2005/06, as audited and signed off by our externalauditors (the Audit Commission), follow at the end ofthis section. A complete set of accounts can beobtained by contacting Martin Woodford, TrustDirector of Finance, on 01432 364428.
18
Analysis of Revenue Expenditure 2005/2006

BA
LAN
CE
SHEE
T A
S A
T 31
Mar
ch 2
006
2004
/05
£000
£000
FIX
ED A
SSET
SIn
tang
ible
ass
ets
487
275
Tang
ible
ass
ets
27,9
7726
,277
Inve
stm
ents
00
28,4
6426
,552
CU
RR
ENT
ASS
ETS
Stoc
ks a
nd w
ork
in p
rogr
ess
1,03
888
1D
ebto
rs15
,173
15,3
47In
vest
men
ts0
0Ca
sh a
t ba
nk a
nd in
han
d45
61,
760
16,6
6717
,988
CR
EDIT
OR
S:A
mou
nts
falli
ng d
ue w
ithin
one
yea
r(8
,001
)(7
,196
)N
ET C
UR
REN
T A
S SET
S (L
IAB
ILIT
IES)
8,66
610
,792
TOTA
L A
SSET
S LE
SS C
UR
REN
T LI
AB
ILIT
IES
37,1
3037
,344
CR
EDIT
OR
S:A
mou
nts
falli
ng d
ue a
fter
mor
e th
an o
ne y
ear
(6,8
63)
(9,1
75)
PRO
VIS
ION
S FO
R L
IAB
ILIT
IES
AN
D C
HA
RG
ES(5
46)
(632
)
TOTA
L A
SSET
S EM
PLO
YED
29,7
2127
,537
FIN
AN
CED
BY:
TAX
PAYE
RS'
EQ
UIT
YPu
blic
div
iden
d ca
pita
l9,
660
7,61
2Re
valu
atio
n re
serv
e12
,149
11,9
10D
onat
ed a
sset
res
erve
4,23
54,
713
Gov
ernm
ent
gran
t re
serv
e0
0O
ther
res
erve
s0
0In
com
e an
d ex
pend
iture
res
erve
3,67
73,
302
TOTA
L TA
XPA
YER
S EQ
UIT
Y29
,721
27,5
37
Sign
ed:
(C
hief
Exe
cutiv
e)D
ate:
3rd
Jul
y 20
06
INC
OM
E A
ND
EX
PEN
DIT
UR
E A
CC
OU
NT
FOR
TH
E YE
AR
EN
DED
31
Mar
ch 2
006
2004
/05
£000
£000
Inco
me
fro
m a
ctiv
itie
s72
,921
68,7
17
Oth
er o
per
atin
g in
com
e11
,887
8,71
1
Op
erat
ing
exp
ense
s(8
4,32
4)(7
7,02
8)
OPE
RA
TIN
G S
UR
PLU
S (D
EFIC
IT)
484
400
Cost
of
fund
amen
tal r
eorg
anis
atio
n/re
stru
ctur
ing
00
Prof
it (lo
ss)
on d
ispo
sal o
f fix
ed a
sset
s0
(4)
SUR
PLU
S (D
EFIC
IT)
BEF
OR
E IN
TER
EST
484
396
Inte
rest
rec
eiva
ble
126
102
Inte
rest
pay
able
00
Oth
er f
inan
ce c
osts
- u
nwin
ding
of
disc
ount
(7)
(11)
Oth
er f
inan
ce c
osts
- c
hang
e in
dis
coun
t ra
te o
n pr
ovis
ions
(47)
0
SUR
PLU
S (D
EFIC
IT)
FOR
TH
E FI
NA
NC
IAL
YEA
R55
648
7
Publ
ic D
ivid
end
Capi
tal d
ivid
ends
pay
able
(554
)(4
67)
RET
AIN
ED S
UR
PLU
S (D
EFIC
IT)
FOR
TH
E YE
AR
220
All
inco
me
and
expe
nditu
re is
der
ived
fro
m c
ontin
uing
ope
ratio
ns.
19
Ann
ual a
ccou
nts
20
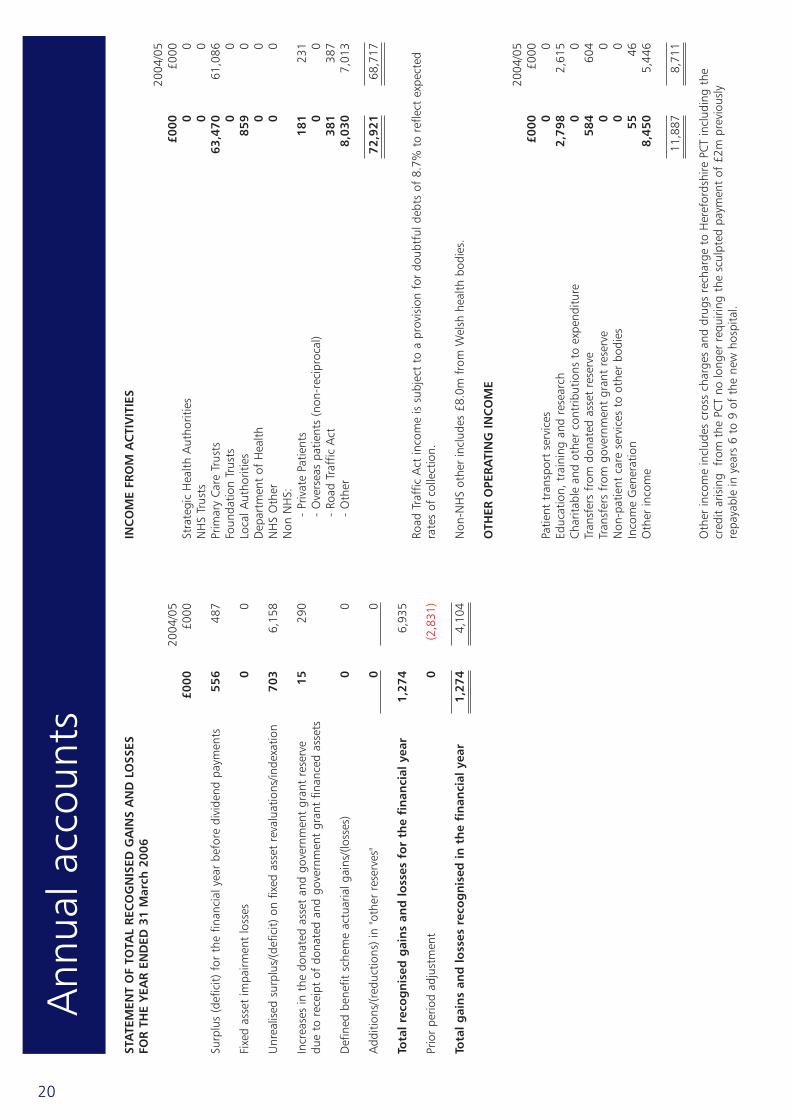
STA
TEM
ENT
OF
TOTA
L R
ECO
GN
ISED
GA
INS
AN
D L
OSS
ES
FOR
TH
E YE
AR
EN
DED
31
Mar
ch 2
006
2004
/05
£000
£000
Surp
lus
(def
icit)
for
the
fin
anci
al y
ear
befo
re d
ivid
end
paym
ents
556
487
Fixe
d as
set
impa
irmen
t lo
sses
00
Unr
ealis
ed s
urpl
us/(d
efic
it) o
n fix
ed a
sset
rev
alua
tions
/inde
xatio
n70
36,
158
Incr
ease
s in
the
don
ated
ass
et a
nd g
over
nmen
t gr
ant
rese
rve
1529
0du
e to
rec
eipt
of
dona
ted
and
gove
rnm
ent
gran
t fin
ance
d as
sets
Def
ined
ben
efit
sche
me
actu
aria
l gai
ns/(l
osse
s)
00
Add
ition
s/(r
educ
tions
) in
"oth
er r
eser
ves"
00
Tota
l rec
og
nis
ed g
ain
s an
d lo
sses
fo
r th
e fi
nan
cial
yea
r1,
274
6,93
5
Prio
r pe
riod
adju
stm
ent
0(2
,831
)
Tota
l gai
ns
and
loss
es r
eco
gn
ised
in t
he
fin
anci
al y
ear
1,27
44,
104
INC
OM
E FR
OM
AC
TIV
ITIE
S
2004
/05
£000
£000
Stra
tegi
c H
ealth
Aut
horit
ies
00
NH
S Tr
usts
00
Prim
ary
Care
Tru
sts
63,4
7061
,086
Foun
datio
n Tr
usts
00
Loca
l Aut
horit
ies
859
0D
epar
tmen
t of
Hea
lth0
0N
HS
Oth
er0
0N
on N
HS:
- Pr
ivat
e Pa
tient
s18
123
1-
Ove
rsea
s pa
tient
s (n
on-r
ecip
roca
l)0
0-
Road
Tra
ffic
Act
381
387
- O
ther
8,03
07,
013
72,9
2168
,717
Road
Tra
ffic
Act
inco
me
is s
ubje
ct t
o a
prov
isio
n fo
r do
ubtf
ul d
ebts
of
8.7%
to
refle
ct e
xpec
ted
rate
s of
col
lect
ion.
Non
-NH
S ot
her
incl
udes
£8.
0m f
rom
Wel
sh h
ealth
bod
ies.
OTH
ER O
PER
ATI
NG
IN
CO
ME
2004
/05
£000
£000
Patie
nt t
rans
port
ser
vice
s0
0Ed
ucat
ion,
tra
inin
g an
d re
sear
ch2,
798
2,61
5Ch
arita
ble
and
othe
r co
ntrib
utio
ns t
o ex
pend
iture
00
Tran
sfer
s fr
om d
onat
ed a
sset
res
erve
58
460
4Tr
ansf
ers
from
gov
ernm
ent
gran
t re
serv
e0
0N
on-p
atie
nt c
are
serv
ices
to
othe
r bo
dies
00
Inco
me
Gen
erat
ion
5546
Oth
er in
com
e8,
450
5,44
6
11,8
878,
711
Oth
er in
com
e in
clud
es c
ross
cha
rges
and
dru
gs r
echa
rge
to H
eref
ords
hire
PCT
incl
udin
g th
ecr
edit
aris
ing
fro
m t
he P
CT n
o lo
nger
req
uirin
g th
e sc
ulpt
ed p
aym
ent
of £
2m p
revi
ousl
yre
paya
ble
in y
ears
6 t
o 9
of t
he n
ew h
ospi
tal.
Ann
ual a
ccou
nts

21
OPE
RA
TIN
G E
XPE
NSE
S
Op
erat
ing
exp
ense
s co
mp
rise
:
2004
/05
£000
£000
Serv
ices
fro
m o
ther
NH
S Tr
usts
00
Serv
ices
fro
m o
ther
NH
S bo
dies
743
432
Serv
ices
fro
m F
ound
atio
n Tr
usts
00
Purc
hase
of
heal
thca
re f
rom
non
NH
S bo
dies
00
Dire
ctor
s' co
sts
699
856
Staf
f co
sts
51,3
2347
,150
Supp
lies
and
serv
ices
– c
linic
al11
,868
10,4
77Su
pplie
s an
d se
rvic
es –
gen
eral
340
273
Esta
blis
hmen
t92
199
7Tr
ansp
ort
7784
Prem
ises
2,40
62,
354
Bad
debt
s25
27D
epre
ciat
ion
and
amor
tizat
ion
1,85
31,
932
Fixe
d as
set
impa
irmen
ts a
nd r
ever
sals
0(7
22)
Aud
it fe
es13
912
7O
ther
aud
itor's
rem
uner
atio
n0
0Cl
inic
al n
eglig
ence
1,10
951
3N
ew H
ospi
tal d
evel
opm
ent
(not
e 25
.1)
11,2
3810
,651
Am
bula
nce
and
othe
r pa
tient
tra
vel
329
367
Nur
ses
cont
inui
ng e
duca
tion
cont
ract
0(5
5)W
aitin
g lis
t in
itiat
ives
2728
Cons
ulta
ncy
fees
229
190
Inte
rnal
Aud
it fe
es71
75In
sura
nce
154
164
Redu
ndan
cy0
41Co
urse
fee
s22
118
7A
mor
tizat
ion
of d
efer
red
asse
ts74
18O
ther
478
862
84,3
2477
,028
Man
agem
ent
cost
s
£000
020
04/2
005
Man
agem
ent
cost
s3,
565
3,25
3
Inco
me
84,8
0877
,428
Man
agem
ent
cost
s ar
e de
fined
as
thos
e on
the
man
agem
ent
cost
s w
ebsi
te a
t w
ww
.dh.
gov.
uk/P
olic
yAnd
Gui
danc
e/O
rgan
isat
ionP
olic
y/Fi
nanc
eAnd
Plan
ning
/NH
SMan
agem
entC
osts
/fs/
en..
Pub
lic S
ecto
r Pa
ymen
t Po
licy
Bett
er P
aym
ent
Prac
tice
Code
- m
easu
re o
f co
mpl
ianc
e
No
.£0
00
Tota
l N
on-N
HS
trad
e in
voic
es p
aid
in t
he y
ear
30,7
9132
,156
Tota
l N
on-N
HS
trad
e in
voic
es p
aid
with
in t
arge
t24
,739
28,5
09Pe
rcen
tage
of
Non
-NH
S tr
ade
invo
ices
pai
d w
ithin
tar
get
80%
89%
Tota
l N
HS
trad
e in
voic
es p
aid
in t
he y
ear
1,07
519
,975
Tota
l N
HS
trad
e in
voic
es p
aid
with
in t
arge
t74
211
,946
Perc
enta
ge o
f N
HS
trad
e in
voic
es p
aid
with
in t
arge
t69
%60
%
The
Bett
er P
aym
ent
Prac
tice
Code
req
uire
s th
e Tr
ust
to a
im t
o pa
y al
l val
id n
on-N
HS
invo
ices
by
the
due
date
or
with
in 3
0 da
ys o
f re
ceip
t of
goo
ds o
r a
valid
invo
ice,
whi
chev
er is
late
r.
Ann
ual a
ccou
nts

CASH FLOW STATEMENT FOR THE YEAR ENDED31 March 2006
2004/05£000 £000
OPERATING ACTIVITIESNet cash inflow/(outflow) from operating activities 1,590 (941)
RETURNS ON INVESTMENTS AND SERVICING OF FINANCE:Interest received 121 106Interest paid 0 0Interest element of finance leases 0 0
Net cash inflow/(outflow) from returns on investments and servicing of finance 121 106
CAPITAL EXPENDITURE(Payments) to acquire tangible fixed assets (3,113) (2,165)Receipts from sale of tangible fixed assets 0 260(Payments) to acquire intangible assets (85) (157)Receipts from sale of intangible assets 0 32(Payments to acquire)/receipts from sale of fixed asset investments 0 0
Net cash inflow/(outflow) from capital expenditure (3,198) (2,030)
DIVIDENDS PAID (554) (467)
Net cash inflow/(outflow) before management of liquid resources and financing (2,041) (3,332)
MANAGEMENT OF LIQUID RESOURCES(Purchase) of current asset investments 0 0Sale of current asset investments 0 0
Net cash inflow/(outflow) from management of liquid resources 0 0
Net cash inflow/(outflow) before financing (2,041) (3,332)
FINANCING
Public dividend capital received 4,050 3,069Public dividend capital repaid (not previously accrued) (2,002) 0Public dividend capital repaid (accrued in prior period) 0 0Loans received 0 0Loans repaid 0 0Other capital receipts 15 290Capital element of finance lease rental payments 0 0Cash transferred (to)/from other NHS bodies 0 0
Net cash inflow/(outflow) from financing 2,063 3,359
Increase/(decrease) in cash 22 27
22
Cash flow statement

The accumulated funds of the Charity amounted to£1.130m at 31 March 2006. They are invested ondeposit with Cazenove Fund Management andBarclays Business Premium Account. In 2005/2006£294,000 additional charitable income was received,including interest of £51,000. £349,000 was spent onpatients’ and staff welfare, amenities and hospitalbuilding and equipment. Management andadministration costs were £31,000. An annual reportof the activities of the Funds held in Trust is sent to theCharity Commission and is available on request fromthe Director of Finance (Tel: 01432 364000).
Directors’ Interests and Trust umbrellacharity trustee interests as at March2006
Mrs Cessa Moore, ChairmanPresident St John Ambulance Brigade, HerefordshireTrustee and Chairman, Support for the Sick Newbornand their Parents, John Radcliffe Hospital, OxfordTrustee, Sick Newborn Education and Research Trust,John Radcliffe Hospital, OxfordPatron of Herefordshire Muheza Link Society
Mr David Rose, Chief ExecutiveNone
Mrs Sharon Beamish, Director of Service DeliveryNone
Mr Peter Harper, Medical DirectorNone
Mr Michael Johnson, Director of Planning andDevelopmentNone
Mrs Helen Blanchard, Director of Nursing andQualityMember of the Investigating Committee of the Nursingand Midwifery Council
Mr Martin Woodford, Director of FinanceDirector of Golf Psychology LtdDirector Monmouthshire Consultancy Co Ltd
Mr Stephan Ludwig, Non-Executive DirectorNone
Cllr Sebastian Bowen, Non-Executive DirectorElected Member of Herefordshire Council
Mrs Caroline Brown, Non-Executive DirectorNone
Mr Mark Curtis, Non-Executive DirectorNone
Mrs Joanna Whitlock, Non-Executive DirectorNone
23
Funds held in trust
Directors
It should be noted that the Independent Auditor’sReport on page 26 does not cover the narrative in thissection. A separate external audit opinion is obtainedon Funds Held in Trust and reported within a separateAnnual Report.

24
Ann
ual a
ccou
nts
25
Ann
ual a
ccou
nts

Independent auditor’s report to the Directors of the Board of Hereford Hospitals NHS Trust
I have examined the summary financial statements set out on pages x to y.
This report is made solely to the Board of Hereford Hospitals NHS Trust in accordance with Part II of the AuditCommission Act 1998 and for no other purpose, as set out in paragraph 36 of the Statement of Responsibilitiesof Auditors and of Audited Bodies prepared by the Audit Commission.
Respective responsibilities of directors and auditors
The directors are responsible for preparing the Annual Report. My responsibility is to report to you my opinionon the consistency of the summary financial statements within the Annual Report with the statutory financialstatements. I also read the other information contained in the Annual Report and consider the implications formy report if I become aware of any misstatements or material inconsistencies with the summary financialstatements.
Basis of opinion
I conducted my work in accordance with Bulletin 1999/6 ‘The auditor’s statement on the summary financialstatement’ issued by the Auditing Practices Board.
Opinion
In my opinion the summary financial statements are consistent with the statutory financial statements of the Trustfor the year ended 31 March 2006.
Signature........................................................................ Date: 23rd August 2006
Name: Mark StocksDistrict Auditor
Address: Audit CommissionFriarsgate1011 Stratford RoadSolihullB90 4EB
26
The independent auditor’s report


8 www.herefordhospital.nhs.uk
) 01432 364000
* FT ConsultationTrust HQThe County HospitalUnion WalkHerefordHR1 2ER
www.herefordhospital.nhs.uk
How to contact us
desi
gn +
prin
t Re
prod
ux P
rinte
rs L
td. 0
1432
269
341