
ANNALS Influenza
16
in the clinic in the clinic Influenza Prevention page ITC5-2 Diagnosis page ITC5-9 Treatment page ITC5-12 Practice Improvement page ITC5-14 CME Questions page ITC5-16 Section Editor Christine Laine, MD, MPH Sankey Williams, MD Physician Writer Margaret Trexler Hessen, MD The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), including PIER (Physicians’ Information and Education Resource) and MKSAP (Medical Knowledge and Self-Assessment Program). Annals of Internal Medicine editors develop In the Clinic from these primary sources in collaboration with the ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIER and MKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org and other resources referenced in each issue of In the Clinic. CME Objective: To provide information on the prevention, diagnosis, and treatment of influenza The information contained herein should never be used as a substitute for clinical judgment. © 2009 American College of Physicians Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
Transcript of ANNALS Influenza
inthe
clinicin the clinic
InfluenzaPrevention page ITC5-2
Diagnosis page ITC5-9
Treatment page ITC5-12
Practice Improvement page ITC5-14
CME Questions page ITC5-16
Section EditorChristine Laine, MD, MPHSankey Williams, MD
Physician WriterMargaret Trexler Hessen, MD
The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), includingPIER (Physicians’ Information and Education Resource) and MKSAP (MedicalKnowledge and Self-Assessment Program). Annals of Internal Medicineeditors develop In the Clinic from these primary sources in collaboration withthe ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIER andMKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org and otherresources referenced in each issue of In the Clinic.
CME Objective: To provide information on the prevention, diagnosis, and treatmentof influenza
The information contained herein should never be used as a substitute for clinicaljudgment.
© 2009 American College of Physicians
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

What are the different types ofinfluenza and what do we knowabout their cause?The 3 main types of influenza virusare A, B, and C. Influenza A issubtyped according to its main sur-face glycoprotein components,hemagglutinin and neuraminidase.There are at least 15 different kindsof hemagglutinin and 9 types ofneuraminidase and a multitude ofpossible combinations. Since 1977,the circulating influenza A strainshave been primarily of the H1N1and H3N2 subtypes.
Influenza A viruses have great capa-city for mutational change, and minor antigenic changes periodicallyoccur in either the hemagglutinin orthe neuraminidase component orboth. This phenomenon, called“antigenic drift,” introduces virusesthat are different enough from preceding strains that previously ac-quired immunity is not fully effec-tive. Thus “drift” contributes to thepattern of yearly seasonal epidemics,and is the basis for the yearly changein vaccine formulations.
More-dramatic antigenic change (a“shift”) results in a virus of distinct-ly different antigenic character towhich most or all of the populationis susceptible. Generally, such shiftsoccur only every few decades, andare the basis for influenza pan-demics. Influenza viruses also infectother species, including birds andpigs. Under circumstances notcompletely understood, these ani-mal strains sometimes adapt to infect humans and spread fromperson to person. For example, despite the H1N1 designation, thecurrently circulating “novel” strainof H1N1 (also known as 2009H1N1 or swine flu), which seems
to have originated in swine, is en-tirely different from the H1N1strains of recent years, and thus hastriggered a pandemic (1).
Influenza B viruses also mutate periodically, but less dramatically;they drift but do not shift, and thusare associated with seasonal epi-demics but not with pandemics. Influenza C viruses are of littleclinical significance.
What is the difference betweenseasonal epidemics and pandemicsof influenza?Seasonal epidemics of influenza Aand B cause substantial morbidityand mortality, disproportionatelyaffecting elderly persons, veryyoung persons, and those withcertain underlying medical condi-tions. The average yearly toll inthe United States is 51 000 deathsand more than 500 000 hospital-izations due to influenza infectionand its complications (2).
Pandemic disease may differ fromseasonal influenza in some features.Unlike yearly epidemics during thecold-weather months, pandemicsmay begin and persist during thewarmer months. Although pan-demic disease is widespread by def-inition, morbidity and mortalityvary depending on the virulence ofthe pandemic strain. The popula-tions hardest hit may be atypicalfor seasonal disease. The 1918 pan-demic was notable for rapid anddevastating disease in young,healthy adults. Although the cur-rent pandemic seems to causemilder disease in general, both thefrequency and severity of infectionhave been greatest in those youngerthan 24 years (3).
© 2009 American College of Physicians ITC5-2 In the Clinic Annals of Internal Medicine 3 November 2009
1. Novel Swine-OriginInfluenza A (H1N1)Virus InvestigationTeam. Emergence ofa novel swine-origininfluenza A (H1N1)virus in humans. NEngl J Med.2009;360:2605-15.[PMID: 19423869]
2. Glezen WP. Clinicalpractice. Preventionand treatment of sea-sonal influenza. NEngl J Med.2008;359:2579-85.[PMID: 19073977]
3. Novel H1N1 Flu Factsand Figures. Centersfor Disease Control,Atlanta, GA, August 4,2009. Accessed atwww.cdc.gov/h1n1flu/surveillanceqa.htmon 10 September2009.
4. Centers for DiseaseControl and Preven-tion. Prevention andcontrol of seasonalinfluenza with vac-cines: recommenda-tions of the AdvisoryCommittee on Im-munization Practices(ACIP), 2009. MMWRRecomm Rep.2009;58:1-52.[PMID: 19644442]
5. Jefferson T, Rivetti A,Harnden A, et al. Vac-cines for preventinginfluenza in healthychildren. CochraneDatabase Syst Rev.2008:CD004879.[PMID: 18425905]
6. Jefferson TO, Rivetti D,Di Pietrantonj C, et al.Vaccines for prevent-ing influenza inhealthy adults.Cochrane DatabaseSyst Rev.2007:CD001269.[PMID: 17443504]
7. Nichol KL, Nordin J,Mullooly J, et al. In-fluenza vaccinationand reduction in hos-pitalizations for car-diac disease andstroke among theelderly. N Engl J Med.2003;348:1322-32.[PMID: 12672859]
With a pandemic currently in progress, influenza has maintained aprominent place in the medical and lay news cycles. The comingseason promises to be challenging for clinicians, who must sort
through strategies for prevention, diagnosis, and treatment for both seasonalinfluenza and influenza due to the novel H1N1 strain.
Prevention
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

© 2009 American College of PhysiciansITC5-3In the ClinicAnnals of Internal Medicine3 November 2009
Which patients should cliniciansimmunize against influenza andwhen during the year is theoptimal timing for vaccination?Current guidelines for vaccinationagainst seasonal influenza, updatedyearly by the Centers for DiseaseControl and Prevention (CDC) fo-cus on providing universal immu-nization for children aged 6 monthsto 18 years and for adults aged 50years or older. The CDC also rec-ommends vaccinating all personswith conditions that place them athigh risk for complications of influenza and their close contacts,including out-of-home caregiversand health care workers. Immu-nization is also encouraged for any-one who wants to prevent becom-ing infected with influenza orspreading it to others, as long assupplies are adequate and the per-son has no contraindications (4).
These recommendations are basedon public health considerations andthe CDC’s assessment of risk andbenefit, guided by existing data. Vaccine efficacy studies have exam-ined populations of different agesand underlying health status andmany end points, including serologicconversion, laboratory-confirmed influenza, influenza-like illness, andsuch complications as hospitalizationand death. Efficacy varies with age,baseline health, and immune func-tion and with the degree of matchbetween vaccine strains and circulat-ing strains. Recent systematic reviewsfound vaccine to be effective in redu-cing laboratory-confirmed influenzain healthy children older than 2 yearsand in healthy adults (5, 6).
Efficacy in elderly patients and inhigh-risk populations has been lessclear. Few trials have focused on thesepopulations, and selection bias maylead to healthier patients being morelikely to be vaccinated. Several largecohort studies have shown a reduc-tion in respiratory and cardiovascularcomplications as well as hospitaliza-tion and death in elderly persons
living in the community and in otherpersons with chronic medical condi-tions (7–11).
A large study of community-dwelling eld-erly persons conducted during 10 influen-za seasons (713 872 person-seasons)showed a 27% reduction in the risk for hos-pitalization for pneumonia and a 48% re-duction in the risk for death among recipi-ents of the influenza vaccine comparedwith those who had not been immunizedagainst influenza (12).
In a cluster randomized, controlled trialduring 2 influenza seasons in 44 nursinghomes in the United Kingdom, vaccinationwas offered to staff in 22 facilities. In the2003 to 2004 influenza season, acceptanceby staff in these “intervention” homes was48.2% compared with 5.9% in the 22 nurs-ing homes in which vaccination was notoffered; in the 2004 to 2005 season, therates were 43.2% and 5.9%, respectively.During periods of influenza activity in 2003to 2004, the decrease in mortality in inter-vention facilities was significant comparedwith control facilities (rate difference, −5.0per 100 residents [95% CI, −7.0 to −2.0]). Nodifferences were found in 2004 to 2005,when the national incidence of influenzawas unusually low (13).
Pregnant women (and their infants)are at high risk for severe influenzaand complications, and vaccinationis recommended for women whoare or will be pregnant during theinfluenza season. Live vaccine iscontraindicated and inactivatedvaccine is classed by the U.S. Foodand Drug Administration as preg-nancy category C, so data are lim-ited. However, available evidencesuggests that inactivated vaccineconfers benefit to both mother andinfant. Transplacental transfer ofmaternal antibody against influen-za has been documented (14).
A prospective study of 340 pregnantwomen randomly assigned to influenzavaccine or pneumococcal vaccine (control)showed reduction in febrile respiratory ill-nesses among women vaccinated againstinfluenza during pregnancy and amongtheir infants, as well as a reduction in docu-mented influenza in the infants, comparedwith women in the control group and their infants. Vaccine effectiveness against
8. Mangtani P, Cumber-land P, Hodgson CR,et al. A cohort studyof the effectivenessof influenza vaccinein older people, per-formed using theUnited Kingdomgeneral practice re-search database. J In-fect Dis. 2004;190:1-10. [PMID: 15195237]
9. EPIVAC Study Group.Effects of annual in-fluenza vaccinationon winter mortality inelderly people withchronic heart disease.Eur Heart J.2009;30:209-16.[PMID: 18997178]
10. Ciszewski A, BilinskaZT, Brydak LB, et al.Influenza vaccina-tion in secondaryprevention fromcoronary ischaemicevents in coronaryartery disease: FLU-CAD study. Eur HeartJ. 2008;29:1350-8.[PMID: 18187561]
11. Hak E, Buskens E,van Essen GA, et al.Clinical effectivenessof influenza vaccina-tion in personsyounger than 65years with high-riskmedical conditions:the PRISMA study.Arch Intern Med.2005;165:274-80.[PMID: 15710789]
12. Nichol KL, Nordin JD,Nelson DB, et al. Ef-fectiveness of in-fluenza vaccine inthe community-dwelling elderly. NEngl J Med.2007;357:1373-81.[PMID: 17914038]
13. Hayward AC, HarlingR, Wetten S, et al. Ef-fectiveness of an in-fluenza vaccine pro-gramme for carehome staff to pre-vent death, morbidi-ty, and health serv-ice use amongresidents: clusterrandomised con-trolled trial. BMJ.2006;333:1241.[PMID: 17142257]
14. Puck JM, Glezen WP,Frank AL, et al. Pro-tection of infantsfrom infection withinfluenza A virus bytransplacentally ac-quired antibody. JInfect Dis.1980;142:844-9.[PMID: 7462695]
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
15. Zaman K, Roy E, Ar-ifeen SE, et al. Effec-tiveness of maternalinfluenza immuniza-tion in mothers andinfants. N Engl JMed. 2008;359:1555-64. [PMID: 18799552]
16. King JC Jr, StoddardJJ, Gaglani MJ, et al.Effectiveness ofschool-based in-fluenza vaccination.N Engl J Med.2006;355:2523-32.[PMID: 17167135]
© 2009 American College of Physicians ITC5-4 In the Clinic Annals of Internal Medicine 3 November 2009
laboratory-confirmed influenza in the in-fants was 63% (CI, 5% to 85%). Reduction infebrile respiratory illness was 36% (CI, 4% to57%) (15).
Recommendations for immunizationof children have been expanded fromthose at highest risk (age >5 years)to all children aged 6 months to 18years. Several studies show thatvaccination of school-aged childrenresults in fewer reports of flu-likesymptoms by household members,suggesting the occurrence of “herdimmunity” and potential benefit tothe community at large (16, 17).
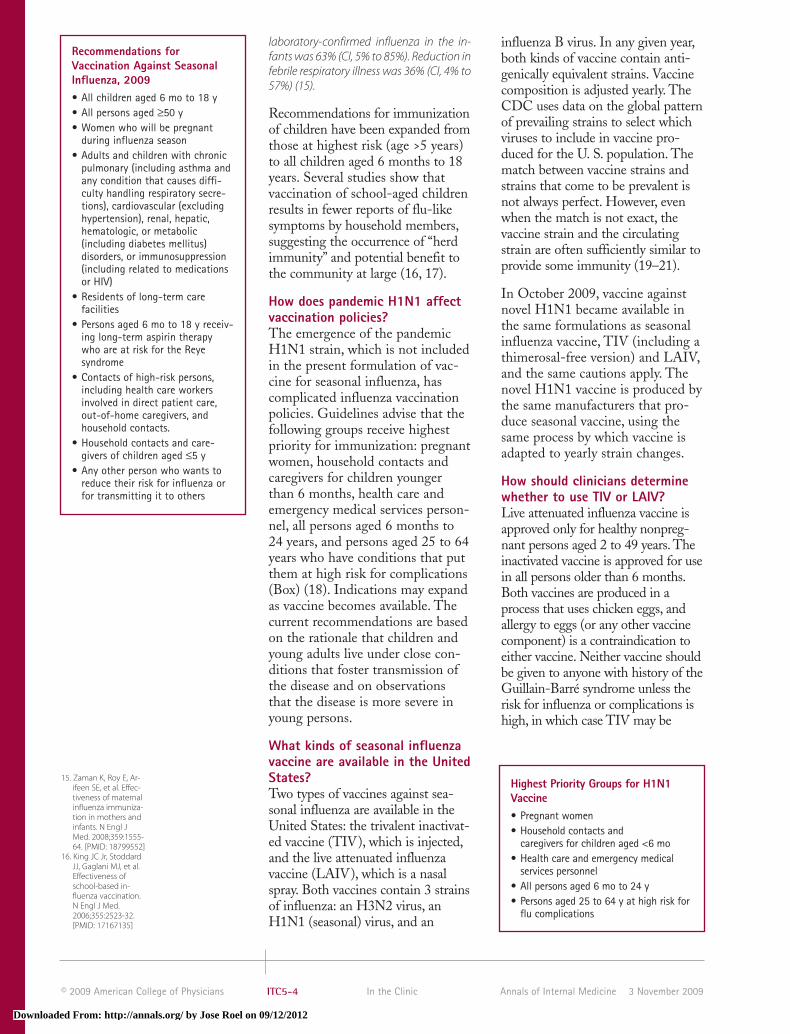
How does pandemic H1N1 affectvaccination policies?The emergence of the pandemicH1N1 strain, which is not includedin the present formulation of vac-cine for seasonal influenza, hascomplicated influenza vaccinationpolicies. Guidelines advise that thefollowing groups receive highestpriority for immunization: pregnantwomen, household contacts andcaregivers for children youngerthan 6 months, health care andemergency medical services person-nel, all persons aged 6 months to24 years, and persons aged 25 to 64years who have conditions that putthem at high risk for complications(Box) (18). Indications may expandas vaccine becomes available. Thecurrent recommendations are basedon the rationale that children andyoung adults live under close con-ditions that foster transmission ofthe disease and on observationsthat the disease is more severe inyoung persons.
What kinds of seasonal influenzavaccine are available in the UnitedStates?Two types of vaccines against sea-sonal influenza are available in theUnited States: the trivalent inactivat-ed vaccine (TIV), which is injected,and the live attenuated influenzavaccine (LAIV), which is a nasalspray. Both vaccines contain 3 strainsof influenza: an H3N2 virus, anH1N1 (seasonal) virus, and an
influenza B virus. In any given year,both kinds of vaccine contain anti-genically equivalent strains. Vaccinecomposition is adjusted yearly. TheCDC uses data on the global patternof prevailing strains to select whichviruses to include in vaccine pro-duced for the U. S. population. Thematch between vaccine strains andstrains that come to be prevalent isnot always perfect. However, evenwhen the match is not exact, thevaccine strain and the circulatingstrain are often sufficiently similar toprovide some immunity (19–21).
In October 2009, vaccine againstnovel H1N1 became available inthe same formulations as seasonalinfluenza vaccine, TIV (including athimerosal-free version) and LAIV,and the same cautions apply. Thenovel H1N1 vaccine is produced bythe same manufacturers that pro-duce seasonal vaccine, using thesame process by which vaccine isadapted to yearly strain changes.
How should clinicians determinewhether to use TIV or LAIV?Live attenuated influenza vaccine isapproved only for healthy nonpreg-nant persons aged 2 to 49 years. Theinactivated vaccine is approved for usein all persons older than 6 months.Both vaccines are produced in aprocess that uses chicken eggs, andallergy to eggs (or any other vaccinecomponent) is a contraindication toeither vaccine. Neither vaccine shouldbe given to anyone with history of theGuillain-Barré syndrome unless therisk for influenza or complications ishigh, in which case TIV may be
Recommendations forVaccination Against SeasonalInfluenza, 2009• All children aged 6 mo to 18 y• All persons aged ≥50 y• Women who will be pregnant
during influenza season• Adults and children with chronic
pulmonary (including asthma andany condition that causes diffi-culty handling respiratory secre-tions), cardiovascular (excludinghypertension), renal, hepatic,hematologic, or metabolic (including diabetes mellitus) disorders, or immunosuppression(including related to medicationsor HIV)
• Residents of long-term care facilities
• Persons aged 6 mo to 18 y receiv-ing long-term aspirin therapywho are at risk for the Reye syndrome
• Contacts of high-risk persons, including health care workers involved in direct patient care,out-of-home caregivers, andhousehold contacts.
• Household contacts and care-givers of children aged ≤5 y
• Any other person who wants toreduce their risk for influenza orfor transmitting it to others
Highest Priority Groups for H1N1Vaccine• Pregnant women• Household contacts and
caregivers for children aged <6 mo• Health care and emergency medical
services personnel• All persons aged 6 mo to 24 y• Persons aged 25 to 64 y at high risk for
flu complications
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

17. Hurwitz ES, Haber M,Chang A, et al. Effec-tiveness of influenzavaccination of daycare children in re-ducing influenza-re-lated morbidityamong householdcontacts. JAMA.2000;284:1677-82.[PMID: 11015798]
18. National Center forImmunization andRespiratory Diseases,CDC. Use of influen-za A (H1N1) 2009monovalent vaccine.Recommendationsof the AdvisoryCommittee on Im-munization Practices(ACIP), 2009. MMWR.2009;58:1-8.
19. Ohmit SE, Victor JC,Rotthoff JR, et al.Prevention of anti-genically drifted in-fluenza by inactivat-ed and liveattenuated vaccines.N Engl J Med.2006;355:2513-22.[PMID: 17167134]
20. Nichol KL, Mendel-man PM, Mallon KP,et al. Effectiveness oflive, attenuated in-tranasal influenzavirus vaccine inhealthy, workingadults: a randomizedcontrolled trial.JAMA. 1999;282:137-44. [PMID: 10411194]
21. New Vaccine Surveil-lance Network. Vac-cine effectivenessagainst laboratory-confirmed influenzain children 6 to 59months of age dur-ing the 2003-2004and 2004-2005 in-fluenza seasons. Pe-diatrics.2008;122:911-9.[PMID: 18977968]
22. Monto AS, Ohmit SE,Petrie JG, et al. Com-parative efficacy ofinactivated and liveattenuated influenzavaccines. N Engl JMed. 2009;361:1260-7. [PMID: 19776407]
23. Piedra PA, GaglaniMJ, Kozinetz CA, etal. Trivalent live at-tenuated intranasalinfluenza vaccineadministered duringthe 2003-2004 in-fluenza type A(H3N2) outbreakprovided immediate,direct, and indirectprotection in chil-dren. Pediatrics.2007;120:e553-64.[PMID: 17698577]
© 2009 American College of PhysiciansITC5-5In the ClinicAnnals of Internal Medicine3 November 2009
preferable to LAIV. Neither vaccineshould be given to persons with sig-nificant febrile illness; minor acute ill-ness without significant fever is not acontraindication, although when sig-nificant nasal congestion is presentand may impede delivery of LAIV,vaccine should be postponed or sub-stituted with TIV. In addition, LAIVshould not be given to anyoneyounger than 2 years or older than 49years; to persons with asthma, reactiveairways disease, or other chronic dis-orders of the pulmonary or cardiovas-cular systems; to persons with otherunderlying medical conditions, suchas diabetes mellitus, renal dysfunc-tion, hemoglo bino pathies, or immunedeficiency; to children or adolescentsreceiving long-term aspirin therapy;to pregnant women; or to persons re-ceiving antiviral drugs active againstinfluenza. Because of the theoreticalrisk for spreading live (albeit attenu-ated) virus to severely immunocom-promised patients (for example, stemcell transplant recipients in protec-tive isolation), health care workerscaring for these patients and otherclose contacts should be immunizedwith TIV. Acquisition of LAIV byunimmunized children through viralshedding has been reported, but noserious illness is known to have beencaused by unvaccinated personsthrough infection by LAIV due toaccidental environmental exposure or shedding of LAIV by vaccinatedcontacts (4).
Not all TIV formulations are licensedfor children. TIV is classified aspreg nancy category C. However, data from the Vaccine Adverse Event Reporting System (VAERS)and other sources show no signifi-cant adverse events to pregnantwomen or to their fetuses attributa-ble to influenza vaccine (4).
Among healthy nonpregnant per-sons aged 2 to 49 years, the CDCguideline states no preference foreither LAIV or TIV (4). Few stud-ies have been designed specificallyto compare the 2 vaccines.
A randomized trial enrolled 1952 healthyadults during the 2007 to 2008 influenzaseason and assigned them to placebo orTIV or LAIV. Absolute efficacy was 68% [CI,46% to 81%] for TIV and 36% [CI, 0% to 59%]for LAIV. Both vaccines prevented influenza,but LAIV was less effective than TIV (22).
LAIV may also offer a protectiveadvantage by eliciting respiratorymucosal as well as systemic immuni-ty. Some authors also cite more-rapid acquisition of antibody withLAIV than with TIV (2, 23). Table 1summarizes differences in indica-tions for TIV and LAIV.
When during the year is theoptimal timing of vaccination?Ideally, persons living in the UnitedStates should receive vaccination inOctober and November, but vaccineshould be offered throughout the
Table 1. Comparison of Inactivated TIV with LAIVCharacteristic TIV LAIV
Approved age ≥6 mo 2 to 49 yIndicated for persons with medical risk factors for influenza complications? Yes NoIndicated for close contacts of immunosuppressed persons not requiring a Yes Yes
protected environment?Indicated for close contacts of immunosuppressed persons who require a Yes No
protected environment (for example, stem cell transplant patients)?Indicated for close contacts of persons at high risk for influenza complications Yes Yes
but not immunosuppressed?Indicated for pregnant women? Yes (Pregnancy category No
C, but no VAERS or other data showing harm to mother or fetus)
LAIV = live attenuated influenza vaccine; TIV = trivalent influenza vaccine; VAERS = Vaccine Adverse Event Reporting System.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

24. Jefferson T, Foxlee R,Del Mar C, et al. In-terventions for theinterruption or re-duction of thespread of respiratoryviruses. CochraneDatabase Syst Rev.2007:CD006207.[PMID: 17943895]
25. World Health Organ-ization WritingGroup. Non-pharma-ceutical interven-tions for pandemicinfluenza, nationaland communitymeasures. Emerg In-fect Dis. 2006;12:88-94. [PMID: 16494723]
26. Cowling BJ, ChanKH, Fang VJ, et al.Facemasks and handhygiene to preventinfluenza transmis-sion in households: arandomized trial.Ann Intern Med.2009. [PMID: 19652172]
27. Khazeni N, BravataD, Holty JEC, et al.Safety and efficacyof extended-dura-tion antiviral chemo-prophylaxis againstpandemic and sea-sonal influenza. AnnIntern Med.2009;151:464-73.
28. Peters PH Jr, Graven-stein S, Norwood P,et al. Long-term useof oseltamivir for theprophylaxis of in-fluenza in a vacci-nated frail olderpopulation. J AmGeriatr Soc.2001;49:1025-31.[PMID: 11555062]
© 2009 American College of Physicians ITC5-6 In the Clinic Annals of Internal Medicine 3 November 2009
winter, because the influenza seasonoften does not peak until Februaryor March. If vaccine is available inSeptember, clinicians should offer itto high-risk patients who presentfor routine appointments or at thetime of hospital discharge to avoiddelayed or missed opportunities.Note that 2 doses separated by atleast 4 weeks are recommended forchildren who have not received atleast 1 dose previously; the firstdose should be given as early aspossible to achieve full effect by theonset of influenza season. Nursinghome residents should not be im-munized before October, becauseantibody levels may not lastthrough the influenza season.These recommendations reflect theconsensus of experts, based on theusual chronology of influenza inthe United States and the durationof vaccine-induced antibody.
How does vaccine supply influencevaccination priorities and timing?If difficulties in vaccine productionor distribution result in shortagesor delays, priority should be givento vaccinating persons at high riskfor severe disease or complicationsand their close contacts, includinghealth care workers. Under suchcircumstances in the past, the CDChas provided triage guidelines ontheir Web site (www.cdc.gov/flu/professionals).
What is the role of behavioralstrategies to prevent influenzatransmission?Few studies have evaluated the ef-ficacy of “nonpharmaceutical in-terventions” for the prevention ofinfluenza. Adults may be able tospread influenza from 1 day beforesymptoms develop to 5 days after.Children and persons with im-mune deficiencies can be infec-tious longer. Handwashing andrespiratory etiquette are easy,cheap, common-sense measuresshown in a systematic review tocontain infection caused by respira-tory viruses (24). Based primarily
on what is known about the trans-mission of disease, experts alsorecommend that infected (or po-tentially infected) persons wear asurgical mask when in close con-tact with others, and that they beisolated when hospitalized or con-fine themselves to home untilafebrile for 24 hours. The protec-tive value of facemasks to unin-fected persons in the community isunknown. Other “social distanc-ing” strategies, such as closingschools and prohibiting large gath-erings, have been studied primarilyhistorically, and these observationsseem to indicate that such meas-ures can contribute to controllingor slowing spread of disease (25).
To investigate whether hand hygiene anduse of facemasks prevents householdtransmission of influenza, 407 persons pre-senting to outpatient clinics in Hong Kongwith influenza-like illness and positive rap-id tests for influenza A or B were randomlyassigned by household to lifestyle educa-tion, hand hygiene, or surgical facemasksplus hand hygiene. Hand hygiene andfacemasks seemed to prevent householdtransmission of influenza virus when im-plemented within 36 hours of index pa-tient symptom onset (26).
What is the role of antiviralagents in preventing influenza,and are there special considerationsduring outbreaks of novel H1N1?Antiviral drugs can supplement orreplace vaccine if there is a shortageor if vaccination is contraindicated,and can prevent the spread of dis-ease during outbreaks in institu-tions and in households. Zanamivir,oseltamivir, amantadine, and ri-mantadine are proven efficaciouswhen used for prophylaxis in com-munity or family settings in whichcirculating virus was sensitive to thedrug. This protection extends tohigh-risk patients.
A systematic review of 7 trials involving7021 participants found that neura min -idase chemoprophylaxis for >4 weeks de-creased the frequency of symptomatic influenza (RR, 0.26 [CI, 0.18 to 0.37]), but notasymptomatic influenza infection (RR, 1.03
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

29. Monto AS, RotthoffJ, Teich E, et al. De-tection and controlof influenza out-breaks in well-vacci-nated nursing homepopulations. Clin In-fect Dis.2004;39:459-64.[PMID: 15356805]
30. Oseltamivir Compas-sionate Use ProgramGroup. Use of os-eltamivir during in-fluenza outbreaks inOntario nursinghomes, 1999-2000. JAm Geriatr Soc.2002;50:608-16.[PMID: 11982659]
31. Ambrozaitis A,Gravenstein S, vanEssen GA, et al. In-haled zanamivir ver-sus placebo for theprevention of in-fluenza outbreaks inan unvaccinatedlong-term care pop-ulation. J Am MedDir Assoc.2005;6:367-74.[PMID: 16286057]
32. Rubin MS, Nivin B,Ackelsberg J. Effectof timing of amanta-dine chemoprophy-laxis on severity ofoutbreaks of influen-za a in adult long-term care facilities.Clin Infect Dis.2008;47:47-52.[PMID: 18484879]
© 2009 American College of PhysiciansITC5-7In the ClinicAnnals of Internal Medicine3 November 2009
[CI, 0.81 to 1.30]). Prevention of influenzawas not significantly different withzanamivir than with oseltamivir, but nau-sea and vomiting were associated with oseltamivir (27).
Prophylaxis for the duration of theinfluenza season has been effectivein preventing laboratory-confirmedinfluenza and secondary complica-tions in nursing home patients(28). Substantial evidence exists for the efficacy of prophylactic useof antiviral agents in controlling established outbreaks in nursinghomes (29–32).
During an outbreak, unvaccinatedstaff members and residents shouldreceive vaccine if it is available.Staff members vaccinated at theonset of the outbreak should re-ceive chemoprophylaxis for 2weeks. In nursing homes, the po-tential for high-intensity virus ex-posure and possible suboptimal immune response to vaccine by de-bilitated residents suggest that allresidents, regardless of previousvaccination, should receive chemo-prophylaxis in an outbreak. Anti-viral medications should be continued in residents for at least 2 weeks and for 1 week longer thanthe duration of the outbreak.
In the community, short-term pro-phylaxis for 10 to 14 days is appro-priate for persons (and their closecontacts) who are at high risk andreceived TIV after the seasonal epi-demic has begun, until vaccinationbecomes effective. Postexposureprophylaxis (for example, in ahousehold setting) should be con-sidered for unimmunized high-riskpersons in conjunction with vacci-nation (TIV) if possible, and forhealthy household contacts of thosewith recently diagnosed influenza.
Prophylaxis may be providedthroughout the influenza outbreakto high-risk persons and their closecontacts (including health careworkers) when vaccine is unavail-able or contraindicated, when a
major antigenic difference existsbetween the epidemic strain andthe vaccine strains, or when severeimmunosuppression makes re-sponse to the vaccine unlikely.Should pandemic disease with thenovel H1N1 continue, antiviralprophylaxis may play an importantrole in management, particularly ifvaccine production does not meetdemand.
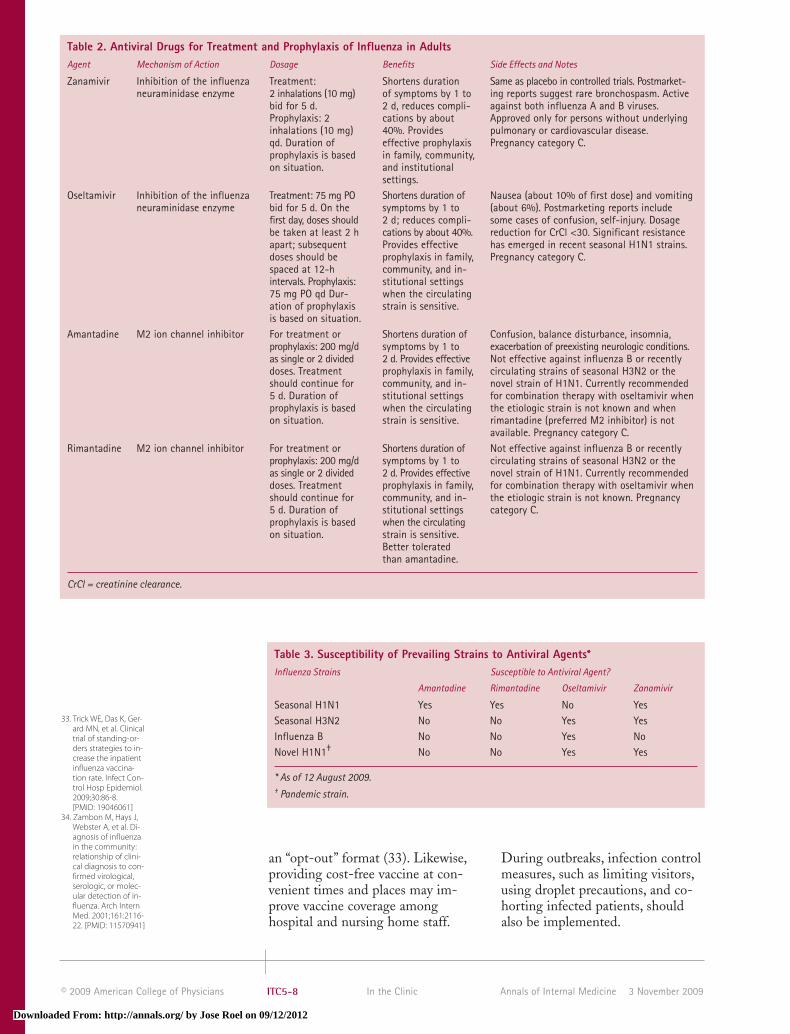
The selection of an appropriate anti-viral regimen has become increas-ingly complex. Various strains havedeveloped resistance to some an-tiviral agents, and no clinicallyavailable tests exist to determineantiviral susceptibility patterns oreven viral subtypes. Table 2 showsavailable agents and Table 3 sum-marizes currently prevailing sensi-tivity patterns, including those seenin the novel H1N1 strain. TheCDC provides periodic updates toguide antiviral use (www.cdc.gov/flu/professionals/index.htm) as wellas weekly surveillance reports thatinclude the geographic distributionof prevailing strains (www.cdc.gov/flu/weekly). At present, zanamiviralone or a combination of os-eltamivir and rimantadine are ap-propriate empirical regimens whenthe specific etiologic strain has notbeen identified.
What measures should clinicianstake to prevent influenza amongpatients and staff in health careinstitutions?All health care personnel should re-ceive influenza vaccination unlessvaccine is contraindicated or un-available. In the latter case, clini-cians should consider prophylaxiswith antiviral medications forthemselves and other health careworkers. The use of standing or-ders, which allow trained healthcare professionals other than physi-cians to identify and vaccinatehigh-risk patients, improves rate ofimmunization of hospital patientsat discharge and of nursing homeresidents, especially if structured in
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
© 2009 American College of Physicians ITC5-8 In the Clinic Annals of Internal Medicine 3 November 2009
an “opt-out” format (33). Likewise,providing cost-free vaccine at con-venient times and places may im-prove vaccine coverage among hospital and nursing home staff.
During outbreaks, infection controlmeasures, such as limiting visitors,using droplet precautions, and co-horting infected patients, shouldalso be implemented.
33. Trick WE, Das K, Ger-ard MN, et al. Clinicaltrial of standing-or-ders strategies to in-crease the inpatientinfluenza vaccina-tion rate. Infect Con-trol Hosp Epidemiol.2009;30:86-8.[PMID: 19046061]
34. Zambon M, Hays J,Webster A, et al. Di-agnosis of influenzain the community:relationship of clini-cal diagnosis to con-firmed virological,serologic, or molec-ular detection of in-fluenza. Arch InternMed. 2001;161:2116-22. [PMID: 11570941]
Table 2. Antiviral Drugs for Treatment and Prophylaxis of Influenza in AdultsAgent Mechanism of Action Dosage Benefits Side Effects and Notes
Zanamivir Inhibition of the influenza Treatment: Shortens duration Same as placebo in controlled trials. Postmarket-neuraminidase enzyme 2 inhalations (10 mg) of symptoms by 1 to ing reports suggest rare bronchospasm. Active
bid for 5 d. 2 d, reduces compli- against both influenza A and B viruses. Prophylaxis: 2 cations by about Approved only for persons without underlying inhalations (10 mg) 40%. Provides pulmonary or cardiovascular disease. qd. Duration of effective prophylaxis Pregnancy category C.prophylaxis is based in family, community, on situation. and institutional
settings.Oseltamivir Inhibition of the influenza Treatment: 75 mg PO Shortens duration of Nausea (about 10% of first dose) and vomiting
neuraminidase enzyme bid for 5 d. On the symptoms by 1 to (about 6%). Postmarketing reports include first day, doses should 2 d; reduces compli- some cases of confusion, self-injury. Dosage be taken at least 2 h cations by about 40%. reduction for CrCl <30. Significant resistance apart; subsequent Provides effective has emerged in recent seasonal H1N1 strains. doses should be prophylaxis in family, Pregnancy category C.spaced at 12-h community, and in-intervals. Prophylaxis: stitutional settings 75 mg PO qd Dur- when the circulating ation of prophylaxis strain is sensitive.is based on situation.
Amantadine M2 ion channel inhibitor For treatment or Shortens duration of Confusion, balance disturbance, insomnia, prophylaxis: 200 mg/d symptoms by 1 to exacerbation of preexisting neurologic conditions.as single or 2 divided 2 d. Provides effective Not effective against influenza B or recently doses. Treatment prophylaxis in family, circulating strains of seasonal H3N2 or the should continue for community, and in- novel strain of H1N1. Currently recommended 5 d. Duration of stitutional settings for combination therapy with oseltamivir when prophylaxis is based when the circulating the etiologic strain is not known and when on situation. strain is sensitive. rimantadine (preferred M2 inhibitor) is not
available. Pregnancy category C.Rimantadine M2 ion channel inhibitor For treatment or Shortens duration of Not effective against influenza B or recently
prophylaxis: 200 mg/d symptoms by 1 to circulating strains of seasonal H3N2 or the as single or 2 divided 2 d. Provides effective novel strain of H1N1. Currently recommended doses. Treatment prophylaxis in family, for combination therapy with oseltamivir when should continue for community, and in- the etiologic strain is not known. Pregnancy 5 d. Duration of stitutional settings category C.prophylaxis is based when the circulating on situation. strain is sensitive.
Better tolerated than amantadine.
CrCl = creatinine clearance.
Table 3. Susceptibility of Prevailing Strains to Antiviral Agents*Influenza Strains Susceptible to Antiviral Agent?
Amantadine Rimantadine Oseltamivir Zanamivir
Seasonal H1N1 Yes Yes No YesSeasonal H3N2 No No Yes YesInfluenza B No No Yes NoNovel H1N1† No No Yes Yes
* As of 12 August 2009.† Pandemic strain.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
35. Monto AS, Graven-stein S, Elliott M, etal. Clinical signs andsymptoms predict-ing influenza infec-tion. Arch InternMed. 2000;160:3243-7. [PMID: 11088084]
36. Boivin G, Hardy I, Tel-lier G, et al. Predict-ing influenza infec-tions duringepidemics with useof a clinical case def-inition. Clin InfectDis. 2000;31:1166-9.[PMID: 11073747]
© 2009 American College of PhysiciansITC5-9In the ClinicAnnals of Internal Medicine3 November 2009
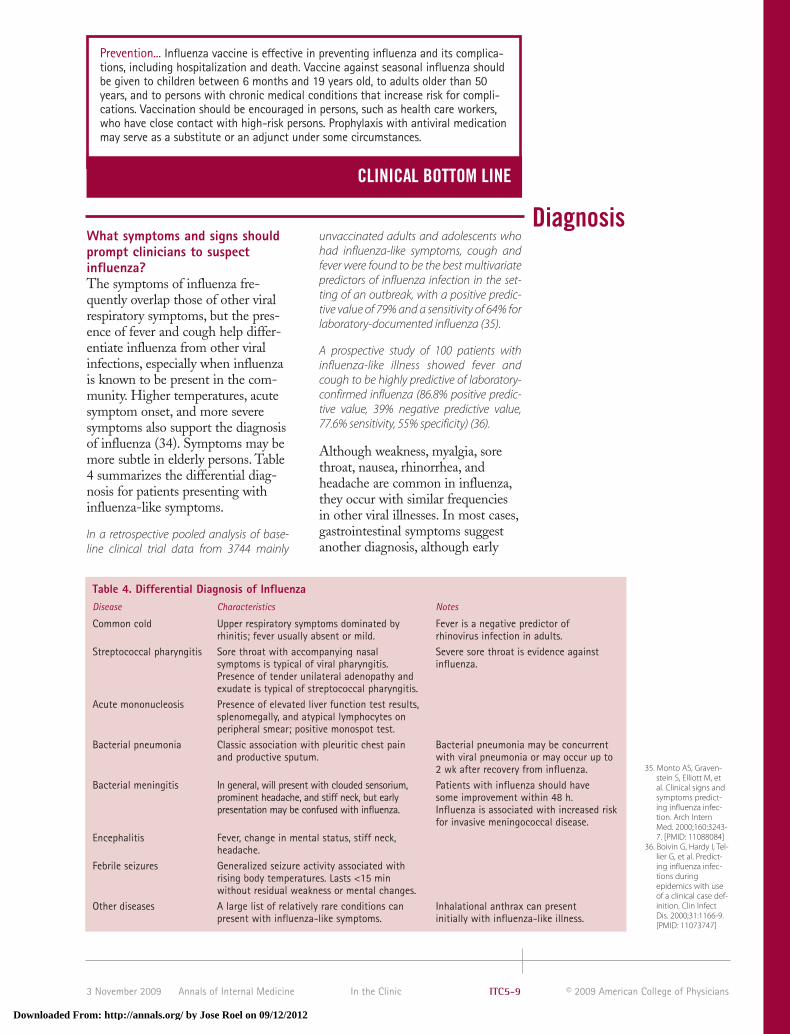
What symptoms and signs shouldprompt clinicians to suspectinfluenza?The symptoms of influenza fre-quently overlap those of other viralrespiratory symptoms, but the pres-ence of fever and cough help differ-entiate influenza from other viral infections, especially when influenzais known to be present in the com-munity. Higher temperatures, acutesymptom onset, and more severesymptoms also support the diagnosisof influenza (34). Symptoms may bemore subtle in elderly persons. Table4 summarizes the differential diag-nosis for patients presenting with influenza-like symptoms.
In a retrospective pooled analysis of base-line clinical trial data from 3744 mainly
unvaccinated adults and adolescents whohad influenza-like symptoms, cough andfever were found to be the best multivariatepredictors of influenza infection in the set-ting of an outbreak, with a positive predic-tive value of 79% and a sensitivity of 64% forlaboratory-documented influenza (35).
A prospective study of 100 patients with influenza-like illness showed fever andcough to be highly predictive of laboratory-confirmed influenza (86.8% positive predic-tive value, 39% negative predictive value,77.6% sensitivity, 55% specificity) (36).
Although weakness, myalgia, sorethroat, nausea, rhinorrhea, andheadache are common in influenza,they occur with similar frequenciesin other viral illnesses. In most cases,gastrointestinal symptoms suggestanother diagnosis, although early
Prevention... Influenza vaccine is effective in preventing influenza and its complica-tions, including hospitalization and death. Vaccine against seasonal influenza shouldbe given to children between 6 months and 19 years old, to adults older than 50years, and to persons with chronic medical conditions that increase risk for compli-cations. Vaccination should be encouraged in persons, such as health care workers,who have close contact with high-risk persons. Prophylaxis with antiviral medicationmay serve as a substitute or an adjunct under some circumstances.
CLINICAL BOTTOM LINE
Diagnosis
Table 4. Differential Diagnosis of InfluenzaDisease Characteristics Notes
Common cold Upper respiratory symptoms dominated by Fever is a negative predictor of rhinitis; fever usually absent or mild. rhinovirus infection in adults.
Streptococcal pharyngitis Sore throat with accompanying nasal Severe sore throat is evidence against symptoms is typical of viral pharyngitis. influenza.Presence of tender unilateral adenopathy and exudate is typical of streptococcal pharyngitis.
Acute mononucleosis Presence of elevated liver function test results, splenomegally, and atypical lymphocytes on peripheral smear; positive monospot test.
Bacterial pneumonia Classic association with pleuritic chest pain Bacterial pneumonia may be concurrent and productive sputum. with viral pneumonia or may occur up to
2 wk after recovery from influenza.Bacterial meningitis In general, will present with clouded sensorium, Patients with influenza should have
prominent headache, and stiff neck, but early some improvement within 48 h. presentation may be confused with influenza. Influenza is associated with increased risk
for invasive meningococcal disease.Encephalitis Fever, change in mental status, stiff neck,
headache.Febrile seizures Generalized seizure activity associated with
rising body temperatures. Lasts <15 min without residual weakness or mental changes.
Other diseases A large list of relatively rare conditions can Inhalational anthrax can present present with influenza-like symptoms. initially with influenza-like illness.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

37. INER Working Groupon Influenza. Pneu-monia and respirato-ry failure fromswine-origin influen-za A (H1N1) in Mexi-co. N Engl J Med.2009;361:680-9.[PMID: 19564631]
38. World Health Organ-ization. Pandemic In-fluenza in PregnantWomen., Geneva,Switzerland. Ac-cessed atwww.who.int/csr/disease/swineflu/notes/h1n1_pregnancy_20090731/en/index.html on 10September 2009.
© 2009 American College of Physicians ITC5-10 In the Clinic Annals of Internal Medicine 3 November 2009
reports of novel H1N1 disease indi-cate that diarrhea is prominent.
In addition to fever, the physical ex-amination may reveal nasal conges-tion and tracheal tenderness. Thepresence of rales or consolidation onchest examination may suggest viralpneumonia or other diagnoses orcomplications, such as bacterialpneumonia or heart failure.
When should clinicians suspectH1N1, avian flu, or otherinfluenza virus infections? Doclinical presentations differ?Other forms of influenza shouldbe considered when a patient withtypical influenza-like symptomspresents outside of the usual in-fluenza season, particularly if they have traveled recently orhave other history that suggestsan unusual form of influenza (forexample, close exposure to birdsor pigs). Very severe disease, par-ticularly in a young, previouslyhealthy person may also suggest anonseasonal strain.
Human infections due to variousavian strains have been reported,and presentations range from verymild upper respiratory symptoms tooverwhelming systemic diseasewith respiratory failure. Reportedcases of H5N1 (avian influenza)from Asia in recent years have beencharacterized by rapid, fulminantdisease and a mortality rate of 50%or more.
Disease due to the novel H1N1pandemic strain has occurredthroughout the northern hemi-sphere during the summer of 2009,but generally has been mild. Somecases of severe, rapidly progressive,often fatal cases have been reportedin young adults with no underlyingdisease. These cases have beencharacterized by dyspnea, cyanosis,hemoptysis, chest pain, confusion,and hypotension. A published de-scription of 18 hospitalized patientsreported markedly elevated levels ofserum lactate dehydrogenase in all;
lymphopenia and elevated creatinekinase levels were also common(37). Factors that might predictsuch an explosive clinical course areas yet unidentified (38).
When should clinicians obtaindiagnostic testing, including rapidtests and tests for novel H1N1, toconfirm influenza diagnosis?Testing should be performed earlyin a suspected outbreak to confirmthe presence of influenza in thecommunity and whenever necessaryto confirm the diagnosis in atypicalcases. It can also be done to investi-gate and monitor outbreaks in hos-pitals and nursing homes.
Although viral cultures on naso-pharyngeal specimens are mostsensitive and specific, results maytake 3 to 10 days or longer, whichlimits clinical usefulness. Rapidtests for seasonal influenza arewidely available and can be helpfulfor individual patients in whomthe results will contribute to treat-ment decisions. Diagnostic testingdoes not need to be done in all pa-tients who present with a typicalclinical picture of influenza whenthe disease is prevalent in thecommunity. In hospitalized pa-tients, rapid confirmation of diag-nosis aids in prompt institution ofappropriate infection-controlmeasures and of antiviral therapyas well as a reduction in the use ofantibacterial antibiotics.
In a published hospital record review, rap-id testing led to a reduction of antibacter-ial antibiotic use in patients who testedpositive for influenza (86% vs. 99%; P = 0.002) and to greater use of antiviralsin patients who tested positive (73% vs.8%; P < 0.001) (39).
In the face of increasing resistanceto antiviral medications, testingthat can differentiate influenza Afrom B may help to determine anappropriate regimen for treatmentor prophylaxis, but none of thecommercially available rapid testsdistinguish between different
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

39. Falsey AR, Murata Y,Walsh EE. Impact ofrapid diagnosis onmanagement ofadults hospitalizedwith influenza. ArchIntern Med.2007;167:354-60.[PMID: 17242309]
40. Centers for DiseaseControl and Preven-tion (CDC). Evalua-tion of rapid influen-za diagnostic testsfor detection of nov-el influenza A(H1N1) Virus - UnitedStates, 2009. MMWRMorb Mortal WklyRep. 2009;58:826-9.[PMID: 19661856]
41. Connolly AM,Salmon RL, Lervy B,et al. What are thecomplications of in-fluenza and can theybe prevented? Expe-rience from the 1989epidemic of H3N2influenza A in gener-al practice. BMJ.1993;306:1452-4.[PMID: 8518643]
© 2009 American College of PhysiciansITC5-11In the ClinicAnnals of Internal Medicine3 November 2009
subtypes of influenza A (seasonalH1N1 or H3N2). No rapid testsare designed specifically to detectthe novel H1N1. Preliminary stud-ies show that some of the rapidtests designed to detect seasonal in-fluenza A also detect novel H1N1,but the sensitivity varies from 40%to 69%, and a positive result doesnot differentiate between seasonaland pandemic strains (40).
In general, CLIA (Clinical Labo-ratory Improvement Act)-waivedtests for physicians’ offices aremore than 70% sensitive andmore than 90% specific for thedetection of seasonal influenza.Sensitivity is higher in childrenthan in adults, higher with nasalsamples than with throat samples,and higher during the first fewdays of illness. The positive pre-dictive value is greatest during in-fluenza season, and the negativepredictive value is greatest outsideof influenza season.
Commercial laboratories can con-firm rapid tests if necessary dur-ing seasonal influenza. If novelH1N1 is suspected and if confir-mation is required (for example,for community surveillance or ina very ill or immunocompromisedpatient), definitive testing may beobtained through public healthauthorities. In either of these cases, clinicians should initiateempirical management withoutawaiting results.
A list of commercially availabletests and their performance charac-teristics can be found at www.cdc.gov/flu/professionals/diagnosis/labprocedures.htm.
When should clinicians suspectbacterial complications in patientsinitially believed to have influenza?Clinicians should consider possiblebacterial complications in patientswho remain ill, worsen, or haveacute onset of high fever andmalaise after initial improvement.Fever in adults with uncomplicat-ed influenza generally lasts about 3 days, by which time most willshow signs of improvement. Al-though it may take 10 to 14 daysfor complete recovery, lack of im-provement or worsening symptomssuggest either a complication or analternative diagnosis.
Acute bronchitis is the most com-monly recognized complication, butothers include sinusitis, pneumonia,and noninfectious sequelae (41).Patients who remain febrile formore than 3 to 5 days, or who develop fever or new symptoms, require evaluation. Symptoms andclinical findings should guide bloodtests, cultures, and imaging studies.Consultation with a specialistshould be considered, especially if the patient is severely ill or immunosuppressed.
Occasionally, serious systemic bac-terial infections, such as pneumonia,staphylococcal bacteremia, menin -gococcal disease, and inhalationalanthrax, can present initially withinfluenza-like symptoms. The dif-ferential diagnosis should be broad-ened in patients whose conditiondeteriorates rapidly, and work-upand treatment should be adjustedaccordingly. Again, consultationwith a specialist might be appropri-ate in such cases.
Diagnosis... Clinical diagnosis of influenza on the basis of fever, cough, rhinor-rhea, and symptom severity is usually reliable when influenza is present in thecommunity. Viral cultures can be useful to determine the cause of an outbreakand rapid testing can guide management decisions in individual patients withan atypical presentation.
CLINICAL BOTTOM LINE
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

42. Hayden FG, Oster-haus AD, Treanor JJ,et al. Efficacy andsafety of the neu-raminidase inhibitorzanamivir in thetreatment of influen-zavirus infections.GG167 InfluenzaStudy Group. N EnglJ Med. 1997;337:874-80. [PMID: 9302301]
43. The MIST (Manage-ment of Influenza inthe Southern Hemi-sphere Trialists)Study Group. Ran-domised trial of effi-cacy and safety ofinhaled zanamivir intreatment of influen-za A and B virus in-fections. Lancet.1998;352:1877-81.[PMID: 9863784]
44. Makela MJ, PauksensK, Rostila T, et al.Clinical efficacy andsafety of the orallyinhaled inhibitorzanamavir in thetreatment of influen-za: a randomized,double-blind, place-bo-controlled Euro-pean study. J InfectDis. 2000;40:42-8[PMID: 10762110]
45. Monto AS, WebsterA, Keene O. Ran-domized, placebo-controlled studies ofinhaled zanamivir inthe treatment of in-fluenza A and B:pooled efficacyanalysis. J Antimi-crob Chemother.1999;44 Suppl B:23-9. [PMID: 10877459]
46. Treanor JJ, HaydenFG, Vrooman PS, etal. Efficacy and safe-ty of the oral neu-raminidase inhibitoroseltamivir in treat-ing acute influenza:a randomized con-trolled trial. US OralNeuraminidaseStudy Group. JAMA.2000;283:1016-24.[PMID: 10697061]
47. Nicholson KG, AokiFY, Osterhaus AD, etal. Efficacy and safe-ty of oseltamivir intreatment of acuteinfluenza: a ran-domised controlledtrial. NeuraminidaseInhibitor Flu Treat-ment InvestigatorGroup. Lancet.2000;355:1845-50.[PMID: 10866439]
48. Jefferson T,Demicheli V, RivettiD, et al. Antivirals forinfluenza in healthyadults: systematic re-view. Lancet.2006;367:303-13.[PMID: 16443037]
© 2009 American College of Physicians ITC5-12 In the Clinic Annals of Internal Medicine 3 November 2009
What is the role of hydration andantipyretics in treating patientswith influenza?Hydration is important to replace thelarge insensible water losses that occurwith fever. In patients with infectiondue to the novel H1N1 strain, diarrhea may also necessitate fluid re-placement. Antipyretics, such as aceta-minophen or ibuprofen, can help toreduce fever and thus prevent furtherinsensible loss. Reduction of fever canprevent other consequences of in-creased metabolic rate, such as tachycardia, and may relieve suchsymptoms as chills and myalgia. Noconvincing evidence exists that anti-pyretic therapy either prolongs orshortens the course of illness. Aspirinand aspirin-containing medicinesshould be avoided, particularly in ado-lescents and children, because of theirassociation with the Reye syndrome.
When should clinicians prescribeantiviral agents for patients withinfluenza and which agents shouldthey prescribe?Clinicians should consider antiviralmedication for people who presentwithin 48 hours of symptom onset, forhospitalized patients, and for those atrisk for severe disease. Pregnantwomen are particularly vulnerable, andespecially in the context of the presentpandemic, prompt antiviral therapy isrecommended. The CDC providesperiodic updates to guide antiviraltherapy based on prevailing strainsand susceptibility patterns of eachstrain. These guidance statements areavailable at www.cdc.gov/flu/professionals/index.htm. Additionally,weekly updates are available atwww.cdc.gov/flu/weekly.
The selection of an appropriate anti-viral drug or combination is difficultdue to the level of resistance that hasemerged. Recently circulating H3N2strains and the pandemic strain ofH1N1 are resistant to the adaman-tanes (amantadine and rimantadine),which also have no inherent activityagainst influenza B. Recent seasonal
strains of H1N1 have become resist-ant to oseltamivir but remain sensitiveto the adamantanes. Table 3 summa-rizes these resistance patterns. Allthese strains remain sensitive tozanamivir, which is the treatment ofchoice for persons who can takeaerosolized medication. In other cas-es, a combination of oseltamivir andrimantadine would be an appropriateempirical regimen. Rapid diagnostictesting (for example, to differentiateinfluenza A and B) and informationfrom public health authorities aboutthe identity of locally prevailingstrains may help refine the selection.
Many studies showed that earlytreatment with either oseltamivir orzanamivir results in earlier resolu-tion of symptoms and a more rapidreturn to normal activities (42–47).
The duration of treatment is 5 days.Table 2 summarizes dosages, benefits,and side effects.
A systematic review that examined trials ofantiviral treatment for influenza concludedthat amantadine and rimantadine useshould be discouraged and that, because oftheir low effectiveness, neuraminidase in-hibitors should be used only in serious epi-demic or pandemic situations rather thanfor control of seasonal influenza (48, 49).
In a meta-analysis of 17 treatment trialsand 7 prevention trials involving childrenyounger than 12 years, healthy adultsaged 12 to 65 years, and high-risk persons,zanamivir reduced the mean duration ofsymptoms by 1.0 day (CI, 0.5 to 1.5), 0.8 day(CI, 0.3 to 1.3), and 0.9 day (CI, 0.1 to 1.9), re-spectively. Oseltamivir reduced symptomsin the same groups by 0.9 day (CI, 0.3 to1.5), 0.9 day (0.3 to 1.4), and 0.4 day (CI,−0.7 to 1.4), respectively. The authors con-cluded that both drugs were effective fortreating influenza, although the evidencewas limited for certain populations (50).
A retrospective pooled analysis of data ex-clusively from 321 high-risk patients with aclinical diagnosis of influenza showed that154 of those patients treated with inhaledzanamivir experienced a reduction in thelength of illness by 2.5 days compared withthose given placebo (P = 0.015). Treated
Treatment
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

49. Jefferson TO,Demicheli V, DiPietrantonj C, et al.Neuraminidase in-hibitors for prevent-ing and treating in-fluenza in healthyadults. CochraneDatabase Syst Rev.2006;3:CD001265.[PMID: 16855962]
50. Cooper NJ, SuttonAJ, Abrams KR, et al.Effectiveness of neu-raminidase inhibitorsin treatment andprevention of in-fluenza A and B: sys-tematic review andmeta-analyses ofrandomised con-trolled trials. BMJ.2003;326:1235.[PMID: 12791735]
51. Lalezari J, CampionK, Keene O, et al.Zanamivir for thetreatment of influen-za A and B infectionin high-risk patients:a pooled analysis ofrandomized con-trolled trials. Arch In-tern Med.2001;161:212-7.[PMID: 11176734]
52. Toronto InvasiveBacterial DiseasesNetwork. Antiviraltherapy and out-comes of influenzarequiring hospital-ization in Ontario,Canada. Clin InfectDis. 2007;45:1568-75.[PMID: 18190317]
53. Lee N, Chan PK, ChoiKW, et al. Factors as-sociated with earlyhospital discharge ofadult influenza pa-tients. Antivir Ther.2007;12:501-8.[PMID: 17668558]
54. Expert Panel of theInfectious DiseasesSociety of America.Seasonal influenza inadults and chil-dren—-diagnosis,treatment, chemo-prophylaxis, and in-stitutional outbreakmanagement: clini-cal practice guide-lines of the Infec-tious DiseasesSociety of America.Clin Infect Dis.2009;48:1003-32.[PMID: 19281331]
55. Centers for DiseaseControl and Preven-tion. Updated Inter-im Recommenda-tions for the Use ofAntiviral Medicationsin the Treatment andPrevention of In-fluenza for the 2009-2010 Season. Accessed atwww.cdc.gov/h1n1flu/recommenda-tions.htm on 10 Sep-tember 2009.
© 2009 American College of PhysiciansITC5-13In the ClinicAnnals of Internal Medicine3 November 2009
high-risk patients returned to normal activities3.0 days earlier (P = 0.022) and had a 43% re-duction in the number of complications requiring antibiotics (P = 0.045) (51).
Fewer studies have been done in hos-pitalized patients, but at least 1 hasshown a reduction in mortality amonghospitalized patients with laboratory-confirmed influenza who were treatedwith antiviral drugs (52). A retrospec-tive cohort study showed decreasedlength of stay in hospitalized patientstreated with oseltamivir (53).
Most studies on the use of antiviralagents are based on initiation oftherapy within 48 hours. However,treatment is generally well-toleratedand, even if started late, may im-prove outcome in critically ill orhigh-risk patients. For this reason,some authorities endorse the use ofantiviral therapy in hospitalized pa-tients and other selected personseven after 48 hours of illness (54).
Although oseltamivir and zanamivirare pregnancy category C drugs, theCDC advises that pregnancy shouldnot be considered a contraindicationto treatment. If H1N1 is suspected,treatment should be given immedi-ately because of the observed severityof disease in pregnant women. Un-der these circumstances, oseltamivirmay be preferred to zanamivir be-cause of its systemic absorption (55).
When should clinicians hospitalizepatients with influenza?Hospitalization should be consideredfor patients who are severely ill be-cause of influenza or its complications.Such conditions as dehydration, inability to maintain adequate intake,respiratory distress, or hypoxemia
should prompt admission. Likewise,an uncertain clinical course or frailbaseline health might prompt admis-sion for close observation.
When should clinicians considerconsultation from an infectiousdisease specialist or public healthauthority?Consultation should be consideredfor help with diagnosis or man-agement as needed. Diagnosticconsultation might be useful in seriously ill patients in whom thediagnosis of influenza is suspectedbut unproven, in patients with anatypical presentation, when a com-plication is suspected, or when thedifferential diagnosis is unusuallybroad (for example, an immuno-suppressed patient with atypicalpneumonia).
Consultation for management shouldbe sought with infectious disease spe-cialists for guidance in the use of antiviral agents and the need for anti-bacterial antibiotics, and with pul-monary or critical care specialists formaintaining oxygenation and obtain-ing specimens for testing.
Consultation with public health au-thorities should be sought if avianinfluenza or another unusual strainis suspected. Public health authori-ties can expedite laboratory identi-fication of the strain and can guidedecisions on antiviral therapy onthe basis of available susceptibilitydata. Also, they are responsible formonitoring disease outbreaks, de-termining the source, evaluatingpossible human-to-human trans-mission, and instituting measures tolimit the spread of disease.
Treatment... The mainstay of influenza treatment is supportive care with hydra-tion and antipyretics. Initiate antiviral treatment in hospitalized patients and inthose at risk for complications. Consider treatment of others who present early inthe course of disease, because early treatment can reduce duration of disease.Hospitalization and subspecialty consultation should be considered for severe ill-ness, uncertain diagnosis, or complications.
CLINICAL BOTTOM LINE
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
Practice Improvement
56. CMS Medicare andMedicaid programs:condition of partici-pation: immuniza-tion standard forlong-term care facili-ties. Final rule. FedRegist2005;70:58833-52
57. Physician Qualityand Reporting Initia-tive. 2009 PQRI Qual-ity Measures List. Ac-cessed atwww.cms.hhs.gov/PQRI/Down-loads/2009_PQRI_Measures-List_030409.pdf on10 September 2009
58. The Joint Commis-sion. Accessed atwww.jointcommis-sion.org on 10 Sep-tember 2009.
inthe
c linicTool Kit
in the clinic
Influenza
PIER Moduleswww.pier.acponline.orgAccess the PIER module on influenza. PIER modules provide evidence-based,updated information on current diagnosis and treatment in an electronic formatdesigned for rapid access at the point of care.
Patient Informationwww.annals.intheclinic/toolkit-flu.htmlDownload copies of the Patient Information sheet that appears on the followingpage for duplication and distribution to your patients.www.nlm.nih.gov/medlineplus/flu.htmlAccess MEDLINE Plus information about influenza for patients, including an interactive tutorial available in both English and Spanish.
Clinical Guidelineswww.cdc.gov/fluCurrent information on seasonal influenza, vaccine and treatment recommenda-tions, vaccine availability, and influenza activity. Includes information for healthprofessionals and patients.www.cdc.gov/h1n1fluCurrent information for clinicians and patients on pandemic influenza due to thenovel H1N1 strain.
Diagnostic Testswww.cdc.gov/flu/professionals/diagnosis/labprocedures.htmAccess information about CLIA-waived tests for rapid diagnosis of influenza.
Quality Measureswww.cms.hhs.gov/pqriAccess information on 2009 Physicians Quality Reporting Initiative measures re-lating to influenza.www.jointcommission.orgAccess information on Joint Commission on the Accreditation of HealthcareOrganizations’ requirements related to influenza vaccination for staff of healthcare organizations.
3 November 2009Annals of Internal MedicineIn the ClinicITC5-14© 2009 American College of Physicians
What measures do stakeholdersuse to measure the quality of carerelated to influenza?Since October 2005, the Centersfor Medicare & Medicaid Services(CMS) has required participatingnursing homes to offer influenzavaccine to all residents (56). TheCMS also includes influenza im-munization of patients 50 yearsand older as a performance meas-ure in its Physician Quality Re-porting Initiative (PQRI) (57).The Joint Commission on the Accreditation of Health Care Or-ganizations ( JCAHO) requiresdocumentation of efforts to vacci-nate independent practitioners andstaff against influenza (58).
What do professionalorganizations recommend forpreventing and treating influenza?The recommendations of most pro-fessional organizations agree with
the CDC’s Advisory Committee onImmunization Practices (ACIP)consensus. ACIP includes represen-tatives from the American Acade-my of Family Physicians, theAmerican Academy of Pediatrics,the American College of Obstetri-cians and Gynecologists, the Amer-ican Medical Association, theAmerican College of Physicians,the American Osteopathic Society,the Infectious Diseases Society ofAmerica, the National Foundationfor Infectious Disease, the Societyfor Healthcare Epidemiology ofAmerica, and numerous other or-ganizations. The Infectious Dis-eases Society of America has alsorecently published a set of clinicalguidelines for prevention, diagnosis,and treatment of seasonal influenza(54). The recommendations listedin this issue of In the Clinic reflectthose guidelines.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012
In the ClinicAnnals of Internal Medicine
Pati
ent
Info
rmat
ion
THINGS YOU SHOULDKNOW ABOUT INFLUENZA
What is influenza?• Influenza (flu) is an illness caused by infection with
the influenza virus.
• Flu symptoms include fever, cough, body aches, tired-ness, sore throat, and runny nose.
• Usually, flu is not serious and persons recover com-pletely. However, older persons, very young children,and persons with long-term conditions can get verysick or even die of flu or its complications.
What is the difference between regularflu and novel H1N1 (swine) flu?• Novel H1N1 (referred to as “swine flu” early on) is a
new influenza virus causing illness in people.
• Novel H1N1 spreads from person to person world-wide, probably in much the same way that regularseasonal influenza viruses spread, but occurs outsidethe regular flu season.
• Although regular flu is most serious in older persons,novel H1N1 seems to affect younger persons morethan older persons.
• Symptoms of novel H1N1 are similar to regular flu,but many patients also have diarrhea, which usuallydoesn’t occur in regular flu.
How can you keep from getting theflu or spreading it to other people?• Get a flu shot every fall if you are aged 6 months to
18 years or 50 years or older; have diabetes, heart orlung disease, or other health problems; or live with ortake care of an older person, someone with healthproblems, or children younger than 5 years.
• Wash your hands often with soap and water and trynot to touch your eyes, nose, or mouth.
• Stay away from people who are sick.
• If you get sick, stay home from work or school.
How will I know if I have the flu orsomething else?• Doctors usually can make the diagnosis without spe-
cial tests, especially when symptoms occur during alocal outbreak.
• Your doctor may need to do tests to rule out other illnesses.
Call your doctor if you have the fluand you:• Have a high fever for more than 3 days
• Are short of breath
• Cannot eat or drink
What can I do for the fever, cough,and aches of the flu?• Fluids and medicines to lower fever are helpful.
• Flu medicines do not cure the flu, but they may short-en the time you are sick. They are most effective whenstarted within 1 to 2 days of the first symptoms.
For More InformationWeb Sites with Good Information about InfluenzaCenters for Disease Control and Preventionwww.cdc.gov/flu
American Lung Associationwww.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=35426
National Institute of Allergy and Infectious Diseaseswww3.niaid.nih.gov/healthscience/healthtopics/Flu/aboutFlu/DefinitionsOverview.htm
American Thoracic Societywww.thoracic.org/sections/education/patient-education/patient-education-materials/patient-information-series/what-is-the-flu.html
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012

5.
4.
3.
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP). Go to www.annals.org/intheclinic/ to obtain up to 1.5 CME credits, to view explanations for correct answers, or to purchase the complete MKSAP program.
CME Questions
3 November 2009Annals of Internal MedicineIn the ClinicITC5-16© 2009 American College of Physicians
A 19-year-old male college student pres-ents in late August with fever of 102°F,chills, body aches, nonproductive cough,loss of appetite, and diarrhea for 4 days.He lives in an apartment with 3 otheryoung adults, 1 of which is currently illwith similar symptoms. He has no under-lying medical conditions. Public healthofficials have identified pandemic H1N1in the southeastern United States com-munity that the patient lives in.
On physical examination, he seems ill. Tem-perature is 101.3°F and blood pressure is120/75 mm Hg in lying position and 120/70mm Hg in standing position. The physicalexamination is otherwise normal.
Which of the following is the most ap-propriate course of action at this time?
A. Hospitalize the patient forobservation because of residencein a community with pandemicH1N1 influenza
B. Make a presumptive diagnosis ofH1N1 influenza and do not obtainlaboratory tests. Prescribe anti-pyretics, oral fluids, and bed rest.Instruct patient to distancehimself from others and remain athome until afebrile off antipyreticsfor 24 hours
C. Obtain nasal swabs to test forH1N1 testing
D. Prescribe oseltamivir
During February, a 37-year-old male res-piratory therapist is seen in your office 1day after developing fever, rigors, gener-alized muscle aches, and mild respiratorysymptoms. He is otherwise in excellenthealth. The patient mentions that he hadnot received an influenza vaccination inthe fall.
Physical examination is normal exceptfor a temperature of 39.4°C (103.0°F)and coryza. Influenza A has been docu-mented in your community, and you haveseen several patients with similar symp-toms this week.
Which of the following is most appropri-ate for managing this patient?
A. Obtain a chest radiograph andblood cultures
B. Obtain a nasopharyngeal culturefor influenza and treat only if theresult is positive
C. Prescribe either zanamivir oroseltamivir
D. Prescribe a fluoroquinoloneantibiotic
E. Administer an intramuscular orintravenous dose of ceftriaxoneand prescribe azithromycin
In January, a 56-year-old woman withchronic obstructive pulmonary diseaseand type 2 diabetes mellitus comes for aroutine office visit. She is currently clini-cally stable and has no new or acutesymptoms. An outbreak of influenza A isoccurring in your community, but the pa-tient failed to receive an influenza vacci-nation last fall.
Which of the following is most appropriatefor preventing influenza in this patient?
A. Administer influenza vaccine andprescribe no new drugs
B. Obtain a nasopharyngeal culturefor influenza and treat only if theresult is positive
C. Administer influenza vaccine andprescribe oseltamivir for 2 weeks
D. Administer influenza vaccine andprescribe amantadine, rimantadine,or oseltamivir for 6 weeks
E. Tell the patient that it is too latefor an influenza vaccination butprescribe amantadine, rimantadine,or oseltamivir for 2 weeks
A 45-year-old man with asthma is eval-uated because of malaise, myalgias,coryza, and a cough. Both influenza Aand B are occurring in the community,and the patient has not been immunizedagainst influenza. Medications includean angiotensin-converting enzyme in-hibitor, an inhaled bronchodilator, and
low-dose aspirin. The patient has nevertraveled outside the United States.
On physical examination, he seems ill.Temperature is 38.3°C (101°F), pulse rateis 95/min, and respiration rate is 24breaths/min. Blood pressure is normal,and the examination is otherwise unre-markable. Chest radiography is normal.
Which of the following antiviral agentsis most appropriate for this patient?
A. ZanamivirB. AmantadineC. OseltamivirD. Rimantadine
The medical director of a primary care prac-tice is developing vaccination policy for thepractice in the setting of anticipating asupply of vaccine for H1N1 influenza.
Which of the following describes thegroups that the Centers for Disease Con-trol (CDC) identifies as highest priorityfor H1N1 vaccine?
A. Pregnant women, householdcontacts and caregivers forchildren younger than 6 months,health care and emergencymedical services personnel, allpersons aged 6 months to 24years, and persons aged 25 to 64years who have conditions thatput them at high risk forcomplications
B. Patients aged 65 years or older, allpersons with chronic conditions,health care workers, and childrenyounger than 12 months
C. Children younger than 12 months,college students living indormitories, patients aged 65 yearsor older, and health care workers
D. Pregnant women and theirhousehold contacts, health careworkers, all persons aged 6 years to24 years, and persons aged 65 yearsor older regardless of the presenceof chronic conditions
1.
2.
Downloaded From: http://annals.org/ by Jose Roel on 09/12/2012


















