An#microbial resistance and stewardship: Naonal landscape...
42
An#microbial resistance and stewardship: Na#onal landscape and what’s happening in Yorkshire & Humber Philip HOWARD Consultant An#microbial Pharmacist , Leeds THT NHS-Improvement AMR Project Lead [email protected] Vice President BSAC @An#bio#cLeeds
Transcript of An#microbial resistance and stewardship: Naonal landscape...

An#microbialresistanceandstewardship:Na#onallandscapeandwhat’shappeningin
Yorkshire&HumberPhilipHOWARD
ConsultantAn#microbialPharmacist,LeedsTHTNHS-ImprovementAMRProjectLead
[email protected]@An#bio#cLeeds

FlemingwarnedaboutAMRin1945NobelPrizespeech


Highincomecountries,AMRisrelateddirectlytoconsump#on.Theyusemorean#bio#csthanLMIC

noinfec#on=
noneedforan#bio#cs
#safeHANDS

6


AMRisoneofbiggestthreatstohumanity
21stSept2016193countriesinUnited
Na#onsagreedalandmarkdeclara#ontoridtheworldofdrug-resistantinfec#ons
or"superbugs“!Reportbackwithin2years

ECDC
UKAn#bio#cuse
NoUKhospitalleveldatasubmidedtoECDCun#l2013

2013:UK5yearAMRStrategy

Scotland,WalesandNorthernIrelanddevelopedtheirowncountrylevelplans
http://gov.wales/docs/dhss/publications/160330amr-dplanen.pdf
https://www.health-ni.gov.uk/sites/default/files/publications/dhssps/arac-strategy-for-tackling-antimicrobial-resistance-star-2012-17.pdf
http://www.gov.scot/Resource/0045/00456736.pdf

UK5yearAMRStrategy:7keyareas

An#microbialStewardship:layeredapproach
Type Features(Mendelson.NatureMay-17.AMRhasalanguageproblem)
Individual Systema#capproachtakenbytheprescribertoopAmiseABusetoimprovepa#entoutcome,ensurepa#entsafety&limitemergenceofAMR
MulA-disciplinary
Combina#onofID,micro,non-specialistDr,pharmacists,IPCNsetcworkinginateamtoop#miseoneormoreABforapa#entorpa#ents
Hospital Involvesoneormoreteams,usuallyco-ordinatedbyacommidee
Community Atprimaryhealthclinic,singleorgroupofprac#ces,long-termcarefacili#es.
NaAonal Ac#vi#esencompassbroaderissues,usinglegisla#onandregula#ontodefineaccesstomedicinesandwhomayprescribethem
GlobalLinkedtodevelopment,thiswillexpandonna#onalprogrammes,toco-ordinateindividualna#ons,country®ionalnetworks&con#nentalac#vi#es.WHO.

Na#onalAn#microbialStewardshipToolkits:collabora#onwithseveralorganisa#ons

TARGET:pa#entinforma#onleaflet–standardapproachforrespiratoryinfec#ons
Adaptedversionforcommunitypharmacists&OOH.Mul#plelanguages&pictorialversion.UTIversionbeingpilotedforGPs&communitypharmacy

ImprovedAMSinDen#stry• Dentalan#microbialstewardshiptoolkithasbeendevelopedand
rolledoutbythedentalsubgroupofESPAURincollabora#onwithFacultyofGeneralDentalPrac#ceandBri#shDentalAssocia#on
• www.gov.uk/guidance/dental-an#microbial-stewardship-toolkit:• Resources,Guidance,EducaAonandtrainingtools,Audittool
andacAonplanning
16

Improvedan#microbialstewardship• AMSincludedinHealth&SocialCareAct2008IPCCodeof
Prac#cesince2015.AllhealthcareprovidersareregisteredbyCQCagainstthisAct
• NICEguidelines&qualitystandardsforallhealthcareprovidersonan#microbialstewardship– NICEAMS:processes&systemsguideline&standards(NG15&QS121)–AMSneedstoexistinallsectors
– NICEAMS:changingriskrelatedbehaviouringeneralpopula#on(NG63):localpriority,$ABdemand&use,preven#ng&$spreadofinfec#ons(handwashing),#knowledgeinchildren&youngpeople,safety-neqng.
– FromJul-17,NICEcommoninfec#onguidelinesforallsectorsevery6-8wk–sinusi#swillbefirst

PilotAMRcampaigninNWEnglandonTV&radio.Resultswillinforma£10mna#onalcampaign
hdps://youtu.be/mu7qsi0y4Mc?list=PLluZEep8m3PAh2b2vJO7_szdtAnRb-IPo
Longervideo1:56forGPprac#ces,communitypharmacies,hospitals.
hdps://youtu.be/zTbLai2GaQM?list=PLluZEep8m3PAh2b2vJO7_szdtAnRb-IPo
30sTVadvert/videoonAMR

HastheUKan#bio#cconsump#onimprovedsince2013(1stUKdata)to2015?Hospitals–UK2ndhighest&noimprovementsince
Hospitals+community–averageforEurope
Moved3countriestorightsince2013
NotclearwhyhospitalABusageperpopula#onissohigh

Good Progress on Reducing Antibiotic (AB) Use in Primary Care Across UK: 2011-2015 ABuseinprimarycare(excludingdental) Items/1000/day 2011 2012 2013 2014 2015 Changelastyear Scotland 2.14 2.21 2.09 2.05 2.00 -2.4%England 1.92 2.01 1.92 1.92 1.79 -6.8%NorthernIreland 2.90 3.06 2.88 2.84 2.76 -2.8%Wales 2.32 2.45 2.33 2.30 2.19 -4.8%
NHSNa#onalServicesScotland.An#microbialuseandresistanceinhumans2015publica#onreport.Availablefrom:hdps://isdscotland.scot.nhs.uk/Health-Topics/Prescribing-and-Medicines/Publica#ons/2016-08-30/AMR_2016.xlsx.LastaccessedOctober2016.
UseofbroadAB(CDIassociated)inprimarycare(excludingdental) Items/100,000/day 2011 2012 2013 2014 2015 Changelastyear Scotland 22.9 20.5 17.9 17.0 16.0 -5.9%England 24.9 23.5 22.1 21.4 18.6 -13.1%NorthernIreland 36.1 37.0 34.7 34.6 32.2 -6.9%Wales 34.6 31.7 28.7 26.2 22.3 -14.9%

ImprovedAMRsurveillanceanddrug-bugoutputs • Tenkeydrug-bugAMRmonitored
&10shadowcombina#ons• 2ndGenera#onSurveillance
Scheme(SGSS)rolledoutformonitoringAMR• IncreasedcoveragefromNHS
laboratoriesfrom30%to98%• Increaseddailyrepor#ngfrom10%
to82%• Increasedautomatedrepor#ngfrom
0%to78%

What’shappeningtoAMR?
ESPAUR2016report
AMRisstableinVREand$inpneumococcalandPseudomonasBSI,but• MRSABSIrate14%#since
2013• MSSABSIrate31%#since2011• E.coliBSI#5%from2015-6• Pip-tazo-R2016-7
• E.coli12%to16%• K.pneum20%to22%
• Co-amoxiclav-R2016-7• E.coli42%to45%
Klebpneum
E.coli

IsY&HAMRdifferentfromEngland?Y&HlowerthanEnglandfor:• E.coli–pip-tazo(same10.1%)• Pseudaeruginosa–pip-tazo4.2%&
meropenem4.8%• Streppneum–penicillin6.3%• Haeminf–co-amoxiclav6.3%
Klebpneum–pip-tazo
Pip-tazoresistanceinKlebpneumwasaproblembutnowimprovingasEngQ122%

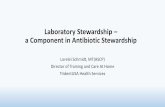
Urinary E.coli resistance to trimethoprim & nitrofurantoin in Y&H CCGs Q3 2016-7
Probablyanover-es#mateofAMRasonlysamplesfromcomplicatedUTIor1stlinefailuresaretested.ChinJAC2016

NaAonalincenAveschemesinEnglandQualityPremiumforPrimaryCare(QP)£90mQPisaboutrewardingCCGsforimprovementsinthequalityoftheservicestheycommission,&toimprovepa#enthealthoutcomesandreduceinequali#esinhealthoutcomesandimproveaccesstoservices.Paidinfollowingyearifallelementsachieved.(~50p/pa#ent)CommissioningforQualityandInnovaAon(CQUIN)£350mCQUINschemeisintendedtodeliverclinicalqualityimprovementsanddrivetransforma#onalchangeinhospitals.Thesewillimpactonreducinginequali#esinaccesstoservices,theexperiencesofusingthemandtheoutcomesachieved.Paidin-yearagainstperformance.LinkedtoPBRac#vity.

CommissioningforQualityandInnovaAon(CQUIN)2016-7
Didthe2016-7sepsisandAMRschemesworkagainsteachother,orcomplementeachother?
NHSEngland.CommissioningforQualityandInnova#on(CQUIN).Guidancefor2016/17.March2016.Availablefrom:hdps://www.england.nhs.uk/wp-content/uploads/2016/03/cquin-guidance-16-17-v3.pdf.LastaccessedOctober2016.

Sepsis AMR

Incen#veschemestoimprovean#bio#cprescribingPrimarycare(QualityPremium)£90m• 2015-6:1%$ABRx&broadspectrumAB<10%.Achieved7%$&13%$• 2016-7:datatoFeb-16:totalnochangebut9%$broadABHospitals(CQUINClinicalQualityIndicators)£350m• 2015-6:sepsisscreening&treatment.4.5%$mortality(21%#EDIVAB)• 2016-7:1%$DDD/admvsFY1314• totalIP&OPAB(12%#in4y)=target2.4%$vsprevyearAchieved2.4%$• carbapenems(36%#/4y&CRE#)=target3.9%$Achieved7%$• piperacillin-tazo(55%#/4y&K.pneum-R36%#E.coli-R31%#)=target16%$Achieved9%$• Q3>75%documenta#oninnotesofday3reviewofempiricAB=98%.• Unintendedconsequence:9%$inC.difficileinfecAoncasesvsprevyr 28

Y&HCCGsperformanceCCG
Achievement
AntibacterialItems/STAR-PU
AntibacterialItems/STAR-PU
QPTargetValueFY2015/16tobeequal
toorlessthan
Co-Amoxiclav,CephalosporinsandQuinolones%Items
Co-Amoxiclav,CephalosporinsandQuinolones%ItemsQPTargetValueFY2015/16tobeequal
toorlessthan
AIREDALE,WHARFEDALEANDCRAVEN Bothmet 1.036 1.161 6.53 10.00BARNSLEY Both met 1.148 1.259 6.51 10.00BASSETLAW Bothmet 1.119 1.161 4.63 10.00BRADFORDCITY Antibacterial items NOT met 1.164 1.161 5.15 10.00BRADFORDDISTRICTS Bothmet 1.168 1.176 5.73 10.00CALDERDALE AntibacterialitemsNOTmet 1.235 1.232 6.04 10.00DONCASTER Both met 1.205 1.315 5.91 10.00EASTRIDINGOFYORKSHIRE Bothmet 1.121 1.161 6.25 10.00England England 1.071 8.92GREATERHUDDERSFIELD Bothmet 1.182 1.213 6.75 10.00HAMBLETON,RICHMONDSHIREANDWHITBYBoth met 0.976 1.161 9.53 12.10HARROGATEANDRURALDISTRICT Bothmet 0.913 1.161 6.31 10.00HULL Bothmet 1.175 1.288 4.60 10.00LEEDSNORTH Bothmet 1.021 1.161 6.11 10.00LEEDSSOUTHANDEAST Both met 1.134 1.207 6.82 10.00LEEDSWEST Bothmet 0.995 1.161 6.32 10.00LINCOLNSHIREEAST Bothmet 1.227 1.241 10.13 10.60LINCOLNSHIREWEST Bothmet 1.088 1.161 10.47 10.60NORTHEASTLINCOLNSHIRE Bothmet 1.107 1.279 8.04 10.00NORTHKIRKLEES Both met 1.215 1.326 6.98 10.00NORTHLINCOLNSHIRE Both met 1.172 1.176 9.74 10.00ROTHERHAM Antibacterial items NOT met 1.250 1.187 7.06 10.00SCARBOROUGHANDRYEDALE Both met 1.196 1.199 5.33 10.00SHEFFIELD Bothmet 1.110 1.161 9.42 11.50VALEOFYORK Bothmet 0.953 1.161 4.37 10.00WAKEFIELD Bothmet 1.181 1.285 5.64 10.00

Widevaria#onwithinprimarycareinYH
Excellentperformanceonbroad-spectrumbutmixedontotalan#bio#cs

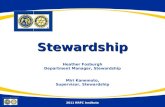
Year end position for YH using RX-info data (PHE AMR from 4th July)
31
DDD/1000Admissions(incDayCase) TrustName
Totalelementsachieved
YH AIREDALENHSFOUNDATIONTRUST 2896.3 2815.8 -2.78% 28.1 23.8 -15.30% 88.2 104 17.91% 2YH BARNSLEYHOSPITALNHSFOUNDATIONTRUST 4801.7 3956 -17.61% 43.2 29.9 -30.79% 73 85.9 17.67% 2YH DONCASTERANDBASSETLAWHOSPITALSNHSFOUNDATIONTRUST3914 3585.4 -8.40% 22.1 24.1 9.05% 38.5 36.6 -4.94% 2YH LEEDSTEACHINGHOSPITALSNHSTRUST 5044.9 4380.2 -13.18% 129.8 114.5 -11.79% 128 127.8 -0.16% 2YH HARROGATEANDDISTRICTNHSFOUNDATIONTRUST 2811.5 2683.1 -4.57% 11.7 17.9 52.99% 38.6 72.7 88.34% 1YH HULLANDEASTYORKSHIREHOSPITALSNHSTRUST 2493 3209.1 28.72% 49.8 38.5 -22.69% 43.5 47.2 8.51% 1YH MIDYORKSHIREHOSPITALSNHSTRUST 3676.5 3625.2 -1.40% 37.4 60.7 62.30% 74.5 111.6 49.80% 1YH THEROTHERHAMNHSFOUNDATIONTRUST 3293.4 3868 17.45% 35.8 30.9 -13.69% 55 66.2 20.36% 1YH YORKTEACHINGHOSPITALNHSFOUNDATIONTRUST 2717.4 2628 -3.29% 17.5 20.8 18.86% 60.9 90.7 48.93% 1YH BRADFORDTEACHINGHOSPITALSNHSFOUNDATIONTRUST2505.6 3189.9 27.31% 32.7 37.8 15.60% 88.8 134 50.90% -YH CALDERDALEANDHUDDERSFIELDNHSFOUNDATIONTRUST3334.1 3535.6 6.04% 40.1 45.5 13.47% 96.4 137.2 42.32% -YH NORTHERNLINCOLNSHIREANDGOOLEHOSPITALSNHSFOUNDATIONTRUST3446.4 3810.9 10.58% 73.2 100.3 37.02% 70.2 110.9 57.98% -YH SHEFFIELDTEACHINGHOSPITALSNHSFOUNDATIONTRUST 3240.1 3269.7 0.91% 69.4 77.4 11.53% 94 97.8 4.04% -
J01-Allantibacterials J01DH-CarbapenemsJ01CR05-Piperacillinand
Tazobactam
NoYHTrustmetall3reduc#onelementsofAMR-CQUINthoughsomeprobablydidwithlocalvaria#ons

Widevaria#ononCQUINperformance
32
Trusts(dots)belowthe0%horizontalgrowthlinemetAMR-CQUIN.Dotstorightofredver#calmedianline=2%↓target&thosetole|=1%↓forFY1718CQUIN


Outcomeofday3reviewofempirican#bio#cs&linkingtomodelhospitalefficiencies(RMOC)Outcomeofday3review(Q1+2)(n=126(81%)trustsenteredvoluntarydata):• Con#nue63%,Stop10%,IVOS16%,switchAB12%,OPAT0.5%
• IVtooralswitch$LOSby6days,£32/pt=massivebedreduc#ons• IVanAbioAcstakeuplotsofnursing#me&costmore=6.5shi|s/day&£450k/yr
(per1000bedhospital)• C.difflinkedtolongercoursesofALLbroadspectrumAB(inclpip-tazo&
carbapenems).Cdiffmortalityis~20%at28d&30%at90d.£4.5k&3-18LOS#/pt• Lessphlebi#s(&probablylessMSSA/MRSABSIas15%devicerelated)• OPAT(home/OPIVAB)freesupbeds&$HCAI.OVIVAstudy:oral=IVfor
osteomyeli#s.OPATneedstobeinallSTPplans• Netherlands:only37%con#nue.Allptsseenat48hbyA-team.0.1wte/ward.€475
savedperconsulta#on6xReturnoninvestment(Diketal.,PLoSOne.2015;10(5):e0126106)• RegMedOpCommifees:AMSwillbeanearlyfocus

Singleinforma#onsourceupdatedmonthlyforAMR&AMU(openaccess)PHEAMRFinger#ps
hfp://fingerAps.phe.org.uk/profile/amr-local-indicators

UKGovernmentAMR2020ambi#ons• ReducehealthcareassociatedGram-nega#ve
bloodstreaminfec#onsinEnglandby50%by2020
• Reduceinappropriatean#bio#cprescribingby50%,withtheaimofbeingaworldleaderinreducingprescribingby2020.
• Seqnganoveralltargetforan#bio#cuseinlivestockandfishfarmedforfood.Strictoversightoncri#calABforhumanuse.
GovtresponsetoReviewonAMR.Sep-16www.gov.uk/government/uploads/system/uploads/adachment_data/file/553471/Gov_response_AMR_Review.pdf.

2017-18AMRIncenAveSchemesReduc#oninGramnega#vebloodstreaminfec#ons• Wholehealtheconomy10%reduc#oninallEcoliBSI• DecreaseinappropriateABRxforUTIinprimarycare.
– 10%$trimethoprim:nitrofurantoinprescribingra#o– 10%$intrimethoprimRx>70yr
• Sustainedreduc#onofinappropriateprescribinginprimarycareReducingimpactfromseriousinfec#onsCQUINforhospitals• Sepsisscreening&IVABtreatmentwithin60minsofdiagnosis• EmpiricIVABreview.%BC+ve.OutcomeofD3review.EvidenceofIVOS.
Jus#fica#onforcon#nuingsameIVAB• 1%or2%$inAB(DDD/adm)fortotalAB,carbapenemandpiperacillin-tazo

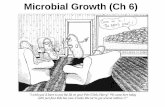
Interventions to Reduce Gram-Negative Bloodstream Infections Gram-negative bacteria are a common cause of urinary tract and intra-abdominal infections. They can also cause surgical site infections, pneumonia and infections of intravascular devices. Gram negative bacteria include E. coli, Klebsiella, Pseudomonas and Enterobacter.
Ulcers and wounds should be minimised using preventative policies based on current guidance, participation in surveillance and auditVentilator-associated pneumonia should be minimised by monitored systems as part of a validated care bundle
Staff should follow guidance and ensure safe aseptic insertion and care of intravascular devicesAll clinical staff required to insert, use, or look after vascular catheters must have adequate training
Medium and long term vascular access devices must only be accessed by people with documented competency in their use and always following aseptic techniquePatients with medium/long term vascular access and carers should be educated in the care of their lines by a healthcare worker trained in the insertion and care of such lines.
Poor hydration is known to increase the risk of urinary tract infections. All hospital patients should have their state of hydration checked and recorded during each nursing shift. This should also be observed in residential careAntibiotic treatment of urinary infection should follow treatment guidelines and not be stopped prematurelyDoes the patient need a catheter? Only insert a catheter if it is essential
All clinical staff required to insert, use, or look after urinary catheters must have adequate training
Bladder scanners should be available in all inpatients areas to aid decisions on catheterisation
Patients leaving hospital with an urinary catheter in situ, and those catheterised in the community, should be provided with a catheter passport giving details of the catheterisation
The date of insertion, expected date of removal, and justification for insertion of any urinary catheter must be recorded in the clinical notes
Good Infection Prevention and Control practice should be adhered to by all staff Staff should adhere to the World Health Organisation’s 5 Moments for Hand Hygiene
References: Tacconelli E et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clinical microbiology and infection. 2014; 20 Suppl 1:1-55. Wilson APR et al. Prevention and control of multi-drug-resistant Gram-negative bacteria. Journal of Hospital Infection. 92:S1-S44.

PHEAMRFingerApsdashboardforYHprimarycare
39

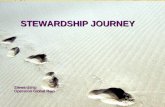
TacklingAMR2017onwards
Interna#onalambi#ontopromotethedevelopmentofan#bio#cs
Ambi#ontohalveinappropriateprescribingby2020
Ambi#ontohalveGram-vebloodstreaminfec#onsby2020
Infection Prevention
and control *
Immunisation programmes and vaccine development
R&
D
Surveillance
DiagnosAcs
Thethreemainprinciples-prevent,protectandpromote-applytohumans,animals,agricultureandtheenvironment.ThisOne-HealthapproachappliesintheUKandglobally.Thediagramiden#fiesthecomponentsthataddressAMRandshowshowtheUKstrategymapstothosecomponents.
SEPSIS
Domestic work on drug reimbursement
Training
Protectthedrugswehave
Promotedevelopmentofnewdrugs,
diagnos#csandalterna#vetreatments
Preventinfec#ons
GIRFT#
AnAbioAcstewardshipprogrammes
*IPC–awholesystemsapproachincludesstandardprecau#ons-handhygiene,environmentalcleaningandinstrumentdecontamina#on.
Ambi#ontoreduceanimaluseto50mg/kgby2018
#GIRFT-Geqngitrightfirst#mewww.geqngitrigh�irsqme.co.uk

SummaryforNa#onalAMR&YHUK5yearAMRstrategyhasbeenabigleverformakingimprovementsquickly• ImprovedAMRandusagerepor#ngforUK&YH• Seqngtargets(andseeingearlyreduc#on)inan#microbialusage
butlidleimpactonAMRsofar• GivingAMSahigherpriorityalongsideIPC• WideningthefocusfromjustC.difficile&MRSA• GoodAMSsaveslives,$HCAI,bed-days,nursing#me,LOS,£££• Needtoworktogethertoreduceanyinappropriatevaria#onin
primary&secondarycare• WeALLneedtobeAn#bio#cGuardians

ThankstoLaraUtsi(YHPHE),DrDianeAshiru-Oredope(PHE),ElizabethBeech(NHS-Imp),MohammedSadak(HEE),Jacqui
Sneddon(SAPG),ColinRichman(RX-info),UKCPA-PIN
PhilipHOWARDConsultantAn#microbialPharmacist,LeedsTHT
[email protected]@An#bio#cLeeds