
Angiotensin-I Converting Enzyme Gene Polymorphisms and the ... · factors.1,2...
7
Genetics Angiotensin-I Converting Enzyme Gene Polymorphisms and the Risk of Venous Thromboembolism in an Ethnically Chinese Population Living in Taiwan Chien-An Hsieh, 1 Yu-Lin Ko, 2 Tsu-Shiu Hsu, 1 Chi-Jen Chang, 1 Ming-Sheng Teng, 2 Semon Wu 2 and Lung-An Hsu 1 Background: There have been conflicting reports of the association between the insertion/deletion (I/D) polymorphism of the angiotensin-converting enzyme (ACE) gene, and the risk of venous thromboembolism (VTE). We sought to investigate the association between ACE I/D polymorphism, and the risk of VTE in a Chinese population living in Taiwan. Methods: 176 patients with VTE and 321 age and sex-matched controls were analyzed for the ACE I/D polymorphism by polymerase chain reaction. Results: The genotype distribution of the ACE I/D polymorphism was not statistically different between the VTE affected subjects and the group of unaffected subjects (p = 0.057). Notably, the frequency of ACE D allele in patients with VTE were significantly lower than that in the control group (28% vs. 35%, p = 0.018). After adjusting for age, gender, smoking, hypertension, diabetes and body mass index (BMI), the ACE D allele carriers remained significantly associated with a decreased risk of VTE. Further meta-analysis by pooling data from 15 studies revealed that neither the DD, nor the II genotype, was found to be associated with VTE (pooled unadjusted odds ratio were 1.167, 95% confidence intervals, 0.927-1.470, p = 0.189 for DD, and 1.085, 95% confidence intervals, 0.875-1.345 p = 0.460 for II). Conclusion: Our results suggest that the presence of the D allele may confer protection against the development of VTE in an ethnically Chinese population in Taiwan. Further meta-analysis did not support a relationship between the ACE I/D polymorphism and the risk of VTE. Key Words: Angiotensin converting enzyme · Polymorphism · Genetics · Venous thromboembolism INTRODUCTION Venous thromboembolism (VTE) is a multifactorial disease influenced by both genetic and environmental factors. 1,2 Angiotensin-converting enzyme (ACE) has some biological effects that could be involved in the pathogenesis of VTE, in that ACE converts angiotensin I to angiotensin II, which is a potent vasoconstrictor and can inhibit fibrinolysis, as well as enhance the activation and aggregation of platelets. 3 This enzyme also degrades bradykinin, which is a powerful vasodilator and inflam- matory mediator. 4 Previous studies have suggested that these factors are important in VTE pathogenesis, 5,6 thus Acta Cardiol Sin 2011;27:252 -8 252 ACE Polymorphism and Venous Thromboembolism Original Article Acta Cardiol Sin 2011;27:252-8 Received: October 12, 2010 Accepted: March 3, 2011 1 First Cardiovascular Division, Department of Internal Medicine, Chang Gung Memorial Hospital, Chang Gung University College of Medicine; 2 The Division of Cardiology, Department of Internal Medicine, Buddhist Tzu Chi General Hospital Taipei Branch, Taipei, Tzu Chi University School of Medicine, Hualian, Taiwan. Address correspondence and reprint requests to: Dr. Lung-An Hsu, First Cardiovascular Division, Department of Internal Medicine, Chang Gung Memorial Hospital, Chang Gung University College of Medicine, No. 199, Tung-Hwa North Road, Taipei, Taiwan. Tel: 886-3-328-1200 ext. 8162, Fax: 886-3-327-1192, E-mail: hsula@ adm.cgmh.org.tw
Transcript of Angiotensin-I Converting Enzyme Gene Polymorphisms and the ... · factors.1,2...

Genetics
Angiotensin-I Converting Enzyme Gene
Polymorphisms and the Risk of Venous
Thromboembolism in an Ethnically Chinese
Population Living in Taiwan
Chien-An Hsieh,1 Yu-Lin Ko,2 Tsu-Shiu Hsu,1 Chi-Jen Chang,1 Ming-Sheng Teng,2 Semon Wu2 and Lung-An Hsu1
Background: There have been conflicting reports of the association between the insertion/deletion (I/D)
polymorphism of the angiotensin-converting enzyme (ACE) gene, and the risk of venous thromboembolism (VTE).
We sought to investigate the association between ACE I/D polymorphism, and the risk of VTE in a Chinese
population living in Taiwan.
Methods: 176 patients with VTE and 321 age and sex-matched controls were analyzed for the ACE I/D
polymorphism by polymerase chain reaction.
Results: The genotype distribution of the ACE I/D polymorphism was not statistically different between the VTE
affected subjects and the group of unaffected subjects (p = 0.057). Notably, the frequency of ACE D allele in patients with
VTE were significantly lower than that in the control group (28% vs. 35%, p = 0.018). After adjusting for age, gender,
smoking, hypertension, diabetes and body mass index (BMI), the ACE D allele carriers remained significantly associated
with a decreased risk of VTE. Further meta-analysis by pooling data from 15 studies revealed that neither the DD, nor the
II genotype, was found to be associated with VTE (pooled unadjusted odds ratio were 1.167, 95% confidence intervals,
0.927-1.470, p = 0.189 for DD, and 1.085, 95% confidence intervals, 0.875-1.345 p = 0.460 for II).
Conclusion: Our results suggest that the presence of the D allele may confer protection against the development of
VTE in an ethnically Chinese population in Taiwan. Further meta-analysis did not support a relationship between
the ACE I/D polymorphism and the risk of VTE.
Key Words: Angiotensin converting enzyme � Polymorphism � Genetics � Venous thromboembolism
INTRODUCTION
Venous thromboembolism (VTE) is a multifactorial
disease influenced by both genetic and environmental
factors.1,2 Angiotensin-converting enzyme (ACE) has
some biological effects that could be involved in the
pathogenesis of VTE, in that ACE converts angiotensin I
to angiotensin II, which is a potent vasoconstrictor and
can inhibit fibrinolysis, as well as enhance the activation
and aggregation of platelets.3 This enzyme also degrades
bradykinin, which is a powerful vasodilator and inflam-
matory mediator.4 Previous studies have suggested that
these factors are important in VTE pathogenesis,5,6 thus
Acta Cardiol Sin 2011;27:252�8 252
ACE Polymorphism and Venous ThromboembolismOriginal Article Acta Cardiol Sin 2011;27:252�8
Received: October 12, 2010 Accepted: March 3, 20111First Cardiovascular Division, Department of Internal Medicine,
Chang Gung Memorial Hospital, Chang Gung University College of
Medicine; 2The Division of Cardiology, Department of Internal
Medicine, Buddhist Tzu Chi General Hospital Taipei Branch, Taipei,
Tzu Chi University School of Medicine, Hualian, Taiwan.
Address correspondence and reprint requests to: Dr. Lung-An Hsu,
First Cardiovascular Division, Department of Internal Medicine,
Chang Gung Memorial Hospital, Chang Gung University College of
Medicine, No. 199, Tung-Hwa North Road, Taipei, Taiwan. Tel:
886-3-328-1200 ext. 8162, Fax: 886-3-327-1192, E-mail: hsula@
adm.cgmh.org.tw

implying that the serum ACE level may be associated
with the risk of developing VTE.
The ACE gene, located on chromosome 17q23, con-
tains an insertion/deletion (I/D) polymorphism in intron
16, which is characterized by the presence or absence of
a 287-bp fragment. This polymorphism accounts for
50% of the inter-individual serum ACE level variation,
with the DD genotype reported to have a higher serum
ACE level than the ID or II variants.7,8
Several studies previously investigated the relation-
ship between ACE I/D polymorphism and VTE,9-25 but
their findings have been controversial. This may have re-
sulted from ethnic differences between study popula-
tions. Among them, only one study was comprised of
Chinese subjects, and reported an association between
the DD genotype and the risk of pulmonary embolism.
Therefore, this study attempted to extend and confirm
their results for an ethnically Chinese population living
in Taiwan.
MATERIALS AND METHODS
Subjects
A total of 186 consecutive and unrelated Taiwanese
VTE patients, 87 males and 99 females, were referred to
the first cardiovascular division of Chang Gung Memo-
rial Hospital, Lin Kou, Taiwan, for venous Doppler
study. Those patients diagnosed with deep vein throm-
bosis (DVT) and/or pulmonary embolism were enrolled.
The mean age of VTE patients was 58.5 � 15.1 years.
Impedance plethysmography and ultrasonographic study
confirmed the diagnosis of deep vein thrombosis in all
such cases. Of the patients with VTE, 25 had pulmonary
embolism. The diagnosis of pulmonary embolism was
supported by one of the following confirmatory imaging
modalities: ventilation/perfusion radionuclide lung scan,
spiral pulmonary computed tomographic scan, or pulmo-
nary angiography. In 40 cases, VTE was associated with
cancer (n = 19), pregnancy (n = 5), oral contraceptives
(n = 1); or VTE occurred postoperatively (5 cardiac
catheterization, 10 surgery). In these cases, VTE was
classified as a secondary event. In the other 146 cases,
VTE was classified as a primary event. There were 360
control subjects, matched with VTE patients for age
(within two years) and sex, randomly selected from
among 718 subjects who underwent health examina-
tions, with no known history of major systemic and car-
diovascular diseases, including VTE, with mean age of
57.9 � 14.7 years, including 171 males and 189 females.
The demographic details of the VTE patients and their
control subjects have been described previously.26 Each
subject provided informed consent. The ethics commit-
tee at Chang Gung Memorial Hospital approved this
study.
Genomic DNA extraction and genotyping of
the ACE I/D polymorphism
Genomic DNA of patients and controls was isolated
from the peripheral blood leukocytes by standard me-
thod using proteinase K digestion of nuclei. The D and I
alleles were identified based on polymerase chain reac-
tion amplification (PCR) of the respective segments
from intron 16 of the ACE gene, as described pre-
viously.27 For quality control purposes, approximately
10% of the samples were re-genotyped using a blinded
procedure, with the same results. Further, in order to
confirm genotyping, a random sample of subjects was
re-genotyped by direct sequence analysis using a com-
mercial sequencing service and the primers previously
used for PCR amplification.
Statistical analysis
Clinical characteristics of continuous variables are
expressed as means � standard deviations (SDs), and
were tested using a two-sample t test. The chi-square test
was used to examine the differences in categorical vari-
ables, and to compare the allelic and genotype frequen-
cies. Odds ratios (OR) were calculated as a measure of
the association of the ACE I/D genotype with the VTE,
with the effects of the D allele assumed to be dominant
(which compares a combination of genotypes ID and DD
to the homozygous II), recessive (which compares a
combination of genotypes ID and II to the homozygous
DD), or additive (which compares a combination of
genotypes DD and ID with weights 2 and 1 respectively,
to the homozygous II). For each odds ratio, we calcu-
lated 2-tailed p values and 95% confidence intervals
(CI). A multivariable logistic regression analysis was
used to evaluate the independent effect of investigated
parameters on the risk of VTE. We used Metanalysis
software (version 1.2.0, 2004; Technopharma Srl, Italy)
253 Acta Cardiol Sin 2011;27:252�8
ACE Polymorphism and Venous Thromboembolism

for the meta-analysis. First, the within- and between-
study variation or heterogeneity was examined by Co-
chrane’s Q test. If a significant Q statistic (p < 0.05) in-
dicated heterogeneity across the studies, the DerSi-
monian and Laird method in the random effects model
was used for meta-analysis. Otherwise, the Mantel-
Haenszel method in the fixed effect model was selected.
Quantification of heterogeneity was also determined by
the I2 metric, which is independent of the number of
studies in the meta-analysis.28 Since not all studies per-
formed and reported the adjusted analysis, and there was
also no uniform set of confounders adjusted for by all
the studies, we used raw genotype data to yield pooled
unadjusted OR (which may be susceptible to confound-
ing). The sample size of our study could determine a
relative risk of > 38% for the D allele being a risk factor
for VTE with a power of 80% at an alpha level of 0.05
in a population with an incidence of D allele of 34%.
RESULTS
In this study, the genotyping of the ACE I/D poly-
morphism could not be determined in 10 cases in the
case group and 39 cases in the control group because of
a shortage of DNA sample. Table 1 lists the baseline
characteristics of the cases and control subjects. BMI
was significantly higher in VTE patients than in con-
trols. A substantially higher percentage of VTE patients
than controls were also diabetics. No significant devia-
tion from Hardy-Weinberg equilibrium was detected for
these two polymorphisms in either VTE patients or con-
trols (p = 0.34, and 0.62, respectively). The D allele fre-
quency of the ACE gene in the control group was 35%,
and consistent with findings obtained by our previous
works.27,29 The genotype frequencies in the study sam-
ples are shown in Table 2 according to whether the sub-
ject has VTE or not. The genotype distribution of the
ACE I/D polymorphism was not statistically different
between the VTE-affected subjects and the group of un-
affected subjects (p = 0.057). In contrast, the ACE D
allele frequencies of cases was significantly lower than
that in the control group (28% vs. 35%, p = 0.018, Table
2). As shown in Table 3, subjects carrying the ACE D
allele were significantly associated with a decreased risk
of VTE compared with those with homozygous II geno-
type in dominant and additive models. Although the
clinical profiles for the study population were incom-
plete, the association was also analyzed with a multi-
variable logistic regression analysis. After adjusting for
age, gender, smoking, hypertension, diabetes and BMI,
the ACE D allele carriers were significantly associated
with a decreased risk of VTE in all studied genetic
models (Table 3). Similar results were obtained when
cases with pulmonary embolism were compared to con-
trols (data not shown). Moreover, sub-classification of
VTE patients into primary or secondary subgroups
found no significant difference of the ACE genotype dis-
tribution when compared to controls (Table 2). Never-
theless, the ACE D allele carriers were still significantly
Acta Cardiol Sin 2011;27:252�8 254
Chien-An Hsieh et al.
Table 1. Baseline characteristics of study population
Controls VTE patients p
Numbers 321 176
Sex (M/F) 149/172 81/95 0.933
Age, years 57.2 � 15.1 59.3 � 15.1 0.142
BMI, kg/m2 (n) 24.4 � 3.8 (309) 26.0 � 4.2 (139) < 0.001
Smoking, % (n) 33.2 (316) 29.1 (148) 0.369
Hypertension, % (n) 29.1 (316) 29.0 (155) 0.985
Diabetes, % (n) 06.6 (316) 12.3 (155) 0.040
* (n) represented case numbers without missing data; totally, 49
subjects had missing data on BMI status, 26 on hypertension
status, 33 on smoking status, and 26 subjects had missing data
on diabetes status.
Table 2. Genotype and allele frequencies of the ACE I/D polymorphism in the study population
Genotype Allele
II ID DDp
I D
Controls 138 (0.43)0 142 (0.44)0 41 (0.13) 0.65 0.35
VTE 95 (0.54) 65 (0.37) 16 (0.09) 0.057 0.72 0.28 0.018
Primary VTE 72 (0.52) 52 (0.38) 14 (0.10) 0.190 0.71 0.29 0.081
Secondary VTE 24 (0.60) 13 (0.33) 03 (0.07) 0.120 0.76 0.24 0.047
All p values are vs. controls.

associated with a decreased risk of VTE compared with
those with homozygous II genotype in secondary sub-
group (Table 2). Figure 1 shows the results of the meta-
analysis of our findings, together with 14 previous re-
ports.30 In total, this meta-analysis comprised 3624 cases
and 3812 controls. Cochrane’s Q test was statistically
significant (p < 0.001) and I2 was 77%, thus indicating
heterogeneity across the studies. Overall, the meta-
analysis demonstrated no statistically significant as-
sociation between the DD genotype and the risk of VTE
(DD versus ID + II, the pooled unadjusted OR = 1.167,
95% CI, 0.927-1.470, p = 0.189 by random effect). As
shown in Figure 2, similar results were obtained when
the effects of the D allele were assumed to be dominant
(which compares a combination of genotypes DD and ID
to the homozygous II) (pooled unadjusted OR = 1.085,
255 Acta Cardiol Sin 2011;27:252�8
ACE Polymorphism and Venous Thromboembolism
Table 3. Odds ratio (OR) and 95% confidence interval (CI) for venous thromboembolism (VTE) in subjects carrying the ACE I/D
polymorphism
model Genotype Control VTE OR (95% CI) p OR (95% CI)* p*
Dominant II 138 (43%) 95 (54%) 1.00 0.019 1.00 0.012
ID + DD 183 (57%) 81 (46%) 0.64 (0.44-0.93) 0.58 (0.37-0.89)
Recessive II + ID 280 (87.2%) 160 (90.9%) 1.00 0.218 1.00 0.02
DD 041 (12.8%) 16 (9.1%) 0.68 (0.37-1.26) 0.40 (0.18-0.92)
Additive II 138 (43%)0. 95 (54%) 1 0.020 1 0.003
ID 142 (44.2%) 065 (36.9%) 0.72 (0.54-0.95) 0.61 (0.44-0.86)
DD 041 (12.8%) 16 (9.1%)
* Multivariable logistic regression analysis with adjustments for age, gender, smoking, hypertension, diabetes and BMI.
Figure 1. Angiotensin-I Converting Enzyme (ACE) DD versus ID and II genotypes and the risk of venous thromboembolism (VTE).
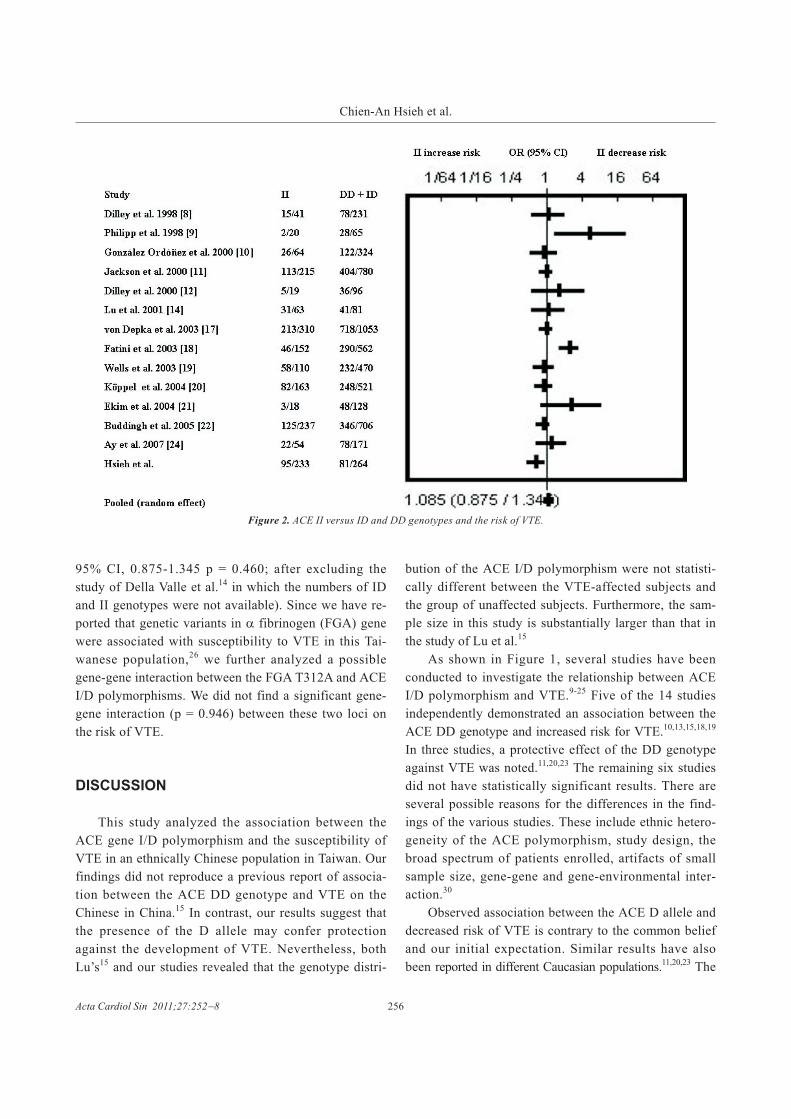
95% CI, 0.875-1.345 p = 0.460; after excluding the
study of Della Valle et al.14 in which the numbers of ID
and II genotypes were not available). Since we have re-
ported that genetic variants in � fibrinogen (FGA) gene
were associated with susceptibility to VTE in this Tai-
wanese population,26 we further analyzed a possible
gene-gene interaction between the FGA T312A and ACE
I/D polymorphisms. We did not find a significant gene-
gene interaction (p = 0.946) between these two loci on
the risk of VTE.
DISCUSSION
This study analyzed the association between the
ACE gene I/D polymorphism and the susceptibility of
VTE in an ethnically Chinese population in Taiwan. Our
findings did not reproduce a previous report of associa-
tion between the ACE DD genotype and VTE on the
Chinese in China.15 In contrast, our results suggest that
the presence of the D allele may confer protection
against the development of VTE. Nevertheless, both
Lu’s15 and our studies revealed that the genotype distri-
bution of the ACE I/D polymorphism were not statisti-
cally different between the VTE-affected subjects and
the group of unaffected subjects. Furthermore, the sam-
ple size in this study is substantially larger than that in
the study of Lu et al.15
As shown in Figure 1, several studies have been
conducted to investigate the relationship between ACE
I/D polymorphism and VTE.9-25 Five of the 14 studies
independently demonstrated an association between the
ACE DD genotype and increased risk for VTE.10,13,15,18,19
In three studies, a protective effect of the DD genotype
against VTE was noted.11,20,23 The remaining six studies
did not have statistically significant results. There are
several possible reasons for the differences in the find-
ings of the various studies. These include ethnic hetero-
geneity of the ACE polymorphism, study design, the
broad spectrum of patients enrolled, artifacts of small
sample size, gene-gene and gene-environmental inter-
action.30
Observed association between the ACE D allele and
decreased risk of VTE is contrary to the common belief
and our initial expectation. Similar results have also
been reported in different Caucasian populations.11,20,23 The
Acta Cardiol Sin 2011;27:252�8 256
Chien-An Hsieh et al.
Figure 2. ACE II versus ID and DD genotypes and the risk of VTE.

reasons, however, remain unclear. It could be due to
chance fluctuation, or other unknown gene-gene and
gene-environmental interactions. VTE is a multifactorial
disease influenced by genetic and environmental fac-
tors.1 Primary or idiopathic VTE was defined as a VTE
event without any triggering factors such as trauma,
surgery, immobilization, pregnancy, or the postpartum
period. It is possible that the presence of environmental
risk factors alters the association between ACE I/D poly-
morphism and VTE. Wells et al.20 postulated that the
ACE I/D polymorphism has a protective effect for idio-
pathic VTE, but this theory is weakened or even re-
versed if a transient condition is present (such as surgery
or cancer). Although our exploratory subgroup analysis
was underpowered, we did not find this gene and envi-
ronmental interaction. Nevertheless, the possibility that
ACE I/D polymorphism has differential effects in pa-
tients with primary versus secondary VTE still cannot be
excluded.
Our study has some limitations. First, the sample
size is relatively small. To overcome this limitation on
sample size, we incorporated our data into the pooled
data from a recent meta-analysis study by Hsiao and
Hsu,30 wherein the combined results still demonstrated
no association between VTE and either the DD or the II
genotype (the pooled unadjusted odds ratio was 1.167,
and 1.085, respectively). Second, there was a lack of in-
formation on serum ACE levels. Therefore, whether
ACE levels actually contribute directly to VTE cannot
be clearly determined. In addition, a positive association
between serum ACE levels and VTE has not yet been
established.30 Third, undiagnosed asymptomatic VTE in
the controls may be subject to some degree of error.
Other limitations included incomplete clinical profiles,
and lack of information for use of drugs such as ACE in-
hibitors and statins. Finally, because we did not assess
the influence of the ACE I/D polymorphism on the pre-
sence of other genetic thrombophilia factors with the
exception of FGA gene, we cannot exclude a possible
role of gene-gene interaction.
CONCLUSION
In conclusion, our results suggest that the presence
of the D allele may confer protection against the deve-
lopment of VTE to a limited extent, but further meta-
analysis does not support any association between the
ACE I/D polymorphism and the risk of VTE. A larger
prospective and longitudinal study, stratifying patients
by etiology and plasma ACE activity, would be neces-
sary to fully assess the significance of this polymor-
phism in the risk of VTE.
REFERENCES
1. Hirsh J, Hull RD, Raskob GE. Epidemiology and pathogenesis of
venous thrombosis. J Am Coll Cardiol 1986;8:104B-13B.
2. Ngow HA, Khairina W. A case of successful thrombolysis in pul-
monary embolism with tenecteplase during peripartum period.
Acta Cardiol Sin 2011;27:52-5.
3. Brown NJ, Vaughan DE. Prothrombotic effects of angiotensin.
Adv Intern Med 2000;45:419-29.
4. Dzau VJ. Cell biology and genetics of angiotensin in cardio-
vascular disease. J Hypertens 1994;12:S3-10.
5. Wakefield TW, Myers DD, Henke PK. Mechanisms of venous
thrombosis and resolution. Arterioscler Thromb Vasc Biol 2008;
28:387-91.
6. Poredos P, Jezovnik MK. The role of inflammation in venous
thromboembolism and the link between arterial and venous
thrombosis. Int Angiol 2007;26:306-11.
7. Rigat B, Hubert C, Alhenc-Gelas F, et al. An insertion/deletion
polymorphism in the angiotensin I-converting enzyme gene
accounting for half the variance of serum enzyme levels. J Clin
Invest 1990;86:1343-6.
8. Tiret L, Rigat B, Visvikis S, et al. Evidence, from combined seg-
regation and linkage analysis, that a variant of the angiotensin
I-converting enzyme (ACE) gene controls plasma ACE levels.
Am J Hum Genet 1992;51:197-205.
9. Dilley A, Austin H, Hooper WC, et al. Relation of three genetic
traits to venous thrombosis in an African-American population.
Am J Epidemiol 1998;147:30-5.
10. Philipp CS, Dilley A, Saidi P, et al. Deletion polymorphism in the
angiotensin-converting enzyme gene as a thrombophilic risk fac-
tor after hip arthroplasty. Thromb Haemost 1998;80:869-73.
11. González Ordóñez AJ, Fernández Carreira JM, Medina Rodríguez
JM, et al. Risk of venous thromboembolism associated with the
insertion/deletion polymorphism in the angiotensin-converting
enzyme gene. Blood Coagul Fibrinolysis 2000;11:485-90.
12. Jackson A, Brown K, Langdown J, et al. Effect of the angio-
tensin-converting enzyme gene deletion polymorphism on the
risk of venous thromboembolism. Br J Haematol 2000;111:
562-4.
13. Dilley A, Austin H, El-Jamil M, et al. Genetic factors associated
with thrombosis in pregnancy in a United States population. Am J
Obstet Gynecol 2000;183:1271-7.
257 Acta Cardiol Sin 2011;27:252�8
ACE Polymorphism and Venous Thromboembolism

14. Della Valle CJ, Issack PS, Baitner A, et al. The relationship of the
factor V Leiden mutation or the deletion-deletion polymorphism
of the angiotensin converting enzyme to postoperative throm-
boembolic events following total joint arthroplasty. BMC Mus-
culoskelet Disord 2001;2:1.
15. Lu Y, Hui R, Zhao Y. Insertion/deletion polymorphsim of the
angiotensin I converting enzyme gene and pulmonary throm-
boembolism in Chinese population. Zhonghua Jie He He Hu Xi
Za Zhi 2001;24:265-8.
16. Dowling NF, Hooper WC, Austin H, et al. The effect of gene
polymorphisms of the rennin-angiotensin system on risk of
venous thromboembolism: the GATE study. Blood 2001;98:264a.
17. Hooper WC, Dowling NF, Wenger NK, et al. Relationship of
venous thromboembolism and myocardial infarction with the
renin-angiotensin system in African-Americans. Am J Hematol
2002;70:1-8.
18. von Depka M, Czwalinna A, Wermes C, et al. The deletion poly-
morphism in the angiotensin-converting enzyme gene is a mo-
derate risk factor for venous thromboembolism. Thromb Hae-
most 2003;89:847-52.
19. Fatini C, Gensini F, Sticchi E, et al. ACE DD genotype: an inde-
pendent predisposition factor to venous thromboembolism. Eur J
Clin Invest 2003;33:642-7.
20. Wells PS, Rodger MA, Forgie MA, et al. The ACE D/D genotype
is protective against the development of idiopathic deep vein
thrombosis and pulmonary embolism. Thromb Haemost 2003;
90:829-34.
21. Köppel H, Renner W, Gugl A, et al. The angiotensin-convert-
ing-enzyme insertion/deletion polymorphism is not related to ve-
nous thrombosis. Thromb Haemost 2004;91:76-9.
22. Ekim N, Oguzulgen IK, Demir N, et al. The role of angiotensin-
converting enzyme gene polymorphism in pulmonary thrombo-
embolism. Thromb Haemost 2004;92:432-3.
23. Buddingh EP, Van Hylckama Vlieg A, Rosendaal FR. The angio-
tensin-converting enzyme gene insertion/deletion polymorphism:
insufficient evidence for a role in deep venous thrombosis. J
Thromb Haemost 2005;3:403-4.
24. Ozbek N, Ataç FB, Yildirim SV, et al. Analysis of prothrombotic
mutations and polymorphisms in children who developed throm-
bosis in the perioperative period of congenital cardiac surgery.
Cardiol Young 2005;15:19-25.
25. Ay C, Bencur P, Vormittag R, et al. The angiotensin-converting
enzyme insertion/deletion polymorphism and serum levels of
angiotensin-converting enzyme in venous thromboembolism.
Data from a case control study. Thromb Haemost 2007;98:777-
82.
26. Ko YL, Hsu LA, Hsu TS, et al. Functional polymorphisms of
FGA, encoding alpha fibrinogen, are associated with susceptibil-
ity to venous thromboembolism in a Taiwanese population. Hum
Genet 2006;119:84-91.
27. Ko YL, Ko YS, Wang SM, et al. Angiotensinogen and angio-
tensin-I converting enzyme gene polymorphisms and the risk of
coronary artery disease in Chinese. Hum Genet 1997;100:210-4.
28. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-
analysis. Stat Med 2002;21:1539-58.
29. Chang YC, Wu WM, Chen CH, et al. Association between the
insertion/deletion polymorphism of the angiotensin I-converting
enzyme gene and risk for psoriasis in a Chinese population in Tai-
wan. Br J Dermatol 2007;156:642-5.
30. Hsiao FC, Hsu LA. Meta-analysis of association between inser-
tion/deletion polymorphism of the angiotensin i-converting en-
zyme gene and venous thromboembolism. Clin Appl Thromb
Hemost 2011;17:51-7.
Acta Cardiol Sin 2011;27:252�8 258
Chien-An Hsieh et al.


















