Angiography in Man
8
Evaluation of Hepatic Regeneration by Scintillation Scanning, Cholangiography and Angiography in Man K. F. ARONSEN, B. ERICSSON, B. NossuN, G. NYLAmNDh, B. PIHL, B. WALDESKOG From the Department of Surgery, Malmo General Hospital, Malmd, Sweden Hepatic resections for primary carci- noma of the liver, unilobar metastases, can- cer of the gallbladder, benign tumors and traumatic liver injury are performed with increasing frequency. From both experi- mental 2 and clinical studies 1, 3, 8, 12, 13, 15 metabolic changes following partial hepa- tectomies are well evaluated. Regeneration of the liver following major resection in man has occasionally been studied by second-look operations16 and by liver scanning.', 12, 13, 17 This paper reports follow-up studies after resections of the liver with scanning, cholangiography and angiography, respec- tively. Material and Methods Of 28 patients subjected to hepatic re- sections of varying extension (subseg- mental) resection to extended right lobec- tomy) it was possible to perform postopera- tive follow-up studies in seven. The ob- servation period varied from 14 days to 2%2 years after the operations. Liver scanning was performed either as memonucleography 4 following injection of 200 uCi. colloidal 198Au, or as photoscan- ning after injection of 200 /Ci. 131I-rose bengal or 3 mCi. 99mTc sulphur colloid. The size of the projected area of the liver in scale 1:1 was estimated planimetri- cally in two patients. All areas calculated after operation were given as a percentage of the preoperative value. Cholangiography was performed by in- jecting contrast medium into the biliary duct system via a T-tube left in the com- mon duct at operation. The T-tube was re- moved 6 months after operation. Direct portography was performed by direct injection of contrast medium into the portal vein via a polyethylene catheter connected to a high pressure syringe. The technic, which has been described else- where,5' 6 includes operative introduction of a polyethylene catheter (Seldinger No. 160) into the portal vein via a small mesen- teric tributary. Selective celiacography was performed by the Seldinger technic, percutaneous catheterization of the femoral artery, and the Odman technic for selective catheteri- zation of the celiac artery.'8 The contrast medium (Urografin 60%, Schering), 0.5 ml./Kg. of body weight, was injected by a high pressure injection syringe. Hepatic blood flow was measured by the method of Bradley et al.9 and Bradley.10 Case Reports Case 1. N. N., a 44-year-old man was operated upon for cancer of the sigmoid colon in February 1963. A solitary metastasis which was localized in the upper convexity of the right lobe of the liver was removed by wedge excision. Two years later the patient complained of pain in the right hypochondrium. Celiacography showed a normal arterial vascular pattem within the liver, but di- 567 Submitted for publication July 14, 1969.
-
Upload
truongphuc -
Category
Documents
-
view
229 -
download
0
Transcript of Angiography in Man

Evaluation of Hepatic Regeneration by ScintillationScanning, Cholangiography and
Angiography in Man
K. F. ARONSEN, B. ERICSSON, B. NossuN, G. NYLAmNDh,B. PIHL, B. WALDESKOG
From the Department of Surgery, Malmo General Hospital, Malmd, Sweden
Hepatic resections for primary carci-noma of the liver, unilobar metastases, can-cer of the gallbladder, benign tumors andtraumatic liver injury are performed withincreasing frequency. From both experi-mental 2 and clinical studies 1, 3, 8, 12, 13, 15metabolic changes following partial hepa-tectomies are well evaluated. Regenerationof the liver following major resection inman has occasionally been studied bysecond-look operations16 and by liverscanning.', 12, 13, 17
This paper reports follow-up studiesafter resections of the liver with scanning,cholangiography and angiography, respec-tively.
Material and MethodsOf 28 patients subjected to hepatic re-
sections of varying extension (subseg-mental) resection to extended right lobec-tomy) it was possible to perform postopera-tive follow-up studies in seven. The ob-servation period varied from 14 days to2%2 years after the operations.
Liver scanning was performed either asmemonucleography 4 following injection of200 uCi. colloidal 198Au, or as photoscan-ning after injection of 200 /Ci. 131I-rosebengal or 3 mCi. 99mTc sulphur colloid.The size of the projected area of the
liver in scale 1:1 was estimated planimetri-cally in two patients. All areas calculated
after operation were given as a percentageof the preoperative value.Cholangiography was performed by in-
jecting contrast medium into the biliaryduct system via a T-tube left in the com-mon duct at operation. The T-tube was re-moved 6 months after operation.
Direct portography was performed bydirect injection of contrast medium intothe portal vein via a polyethylene catheterconnected to a high pressure syringe. Thetechnic, which has been described else-where,5' 6 includes operative introductionof a polyethylene catheter (Seldinger No.160) into the portal vein via a small mesen-teric tributary.
Selective celiacography was performedby the Seldinger technic, percutaneouscatheterization of the femoral artery, andthe Odman technic for selective catheteri-zation of the celiac artery.'8 The contrastmedium (Urografin 60%, Schering), 0.5ml./Kg. of body weight, was injected bya high pressure injection syringe.
Hepatic blood flow was measured by themethod of Bradley et al.9 and Bradley.10
Case ReportsCase 1. N. N., a 44-year-old man was operated
upon for cancer of the sigmoid colon in February1963. A solitary metastasis which was localizedin the upper convexity of the right lobe of theliver was removed by wedge excision. Two yearslater the patient complained of pain in the righthypochondrium. Celiacography showed a normalarterial vascular pattem within the liver, but di-
567Submitted for publication July 14, 1969.

FIG. 1. Illustration of liver scanning with '"'Aupreoperatively and 1, 6 and 22 months after ex-
tended right lobectomy (Case 1). Arrow indicatesresection line.
rect portogratphv and liver scanning revealed a
solitary tumor in the imedial pairt of the right liverlobe. Extended right lobectomy was performedl.The operative specimein weighed 1,350 Gim. His-tological exaamination showed a solitary' metastasisof colonic carinoimia. The patient recovered fromthis operation uneventfully and was discharged.
Liver scanning with "9'Au was done pre-
operatively and at 1, 2, 3, 6, 18 and 22 monthspostoperatively. Scans miade preoperatively andat 1, 6 and 22 months are shown in Figure 1.One month after operation the liver remnant hadincreased considerably' in size and at 6 months a
further increase was seen. In the scan made 22monthis after operation there was a slight addi-tional increase in size. The planimetrically calcu-lated areas of the scans for all the examiiinationsperformed (Fig. 2) show a very rapid initial in-crease in size, later followed by less rapid growth.The calculated preoperative liver size ws'as almostreached at 22 months.
MIesenterico-celiacography 5 moinths after op-
eration showed the left hepatic artery and itsbranches to be elongated and distributed to a con-
siderably larger area than was seen preoperatively(Fig. 3a). Direct portography performed 6 monthsafter operation showed the portal ramifications ofthe remaining part of the liver to be distributedto a larger area than before operation; these ves-
sels were also dilated and elongated. No outgrowthof new vessels from the resection surface was seen
(Fig. 3b). Mesenterico-celiacography 23 years
'D OTHERS Annals of SurgeryApril 1970
after operation slhowe(l the saiie findings that weresene 5 mnontlhs postop. (Fig. 3c).
Case 2. H. A., a 62-year-old man was admittedto the hlospital in Felhruary 1965 with a historyfor 7 years of abdominal colic, diarrhea and grad-iial loss of weiglht. Celiaeography revealed richlyXvasctilarized tuiinors occupying most of the rightlobe of the liver. Direct portography confirmedthe dilagnosis. AIn extended right lobectomy Wasperformed. The operative specimiiein weighed 1,450Gim. Histological examiiination suggested metastasesfroin carcinoid tumiior. Except for biliary perito-Initis, drained oIn the 8tlh postoperative day, thepostoperative course was uneventfuil. Six monthsafter operation the patient died from a bleedinggastric uilcer. Necropsy showed a medullary cancerof the thvroid and para-aortal metastases withthe samiie histological appearance as the tuimorpreviously removed from the liver. At auitopsy theweight of the remaininig liver was 1,480 Gm.
Liver scans made with "AiAu preoperativelyand at 1 and 5 months postoperatively are shownin Figure 4. An impressive increase in size of theliver remiinant was seen 1 month after operation.After 4 mo. a less impressive increase was seen.
Five months postoperati-vely direct portog-raphy showed enlargement of the remaining partof the liver, the lateral segiment of the left lobe,aIs evidenced by elongation and stretching of itsportal branches. No outgrowth of new vesselsfrom the resection surface was noted (Fig. 5).
AREANORMALIZED
1.0 -
0.9
0.8-
0.7-
0.6 -
0.5 -
0.4 -
0.3-
T 3 6 9 12 15 18 21 24 27
OP MONTHS AFTER OPERATION
FIG. 2. Liver areas calculated from scans with..8Au during the postoperative period after ex-tended right lobectomy (Case 1).
568 ARONSEN AN
P R E O P
6 MONTHS POSTOP 2 MUNOIHS USTUOP
EVALUATION OF HEPATIC REGENERATION
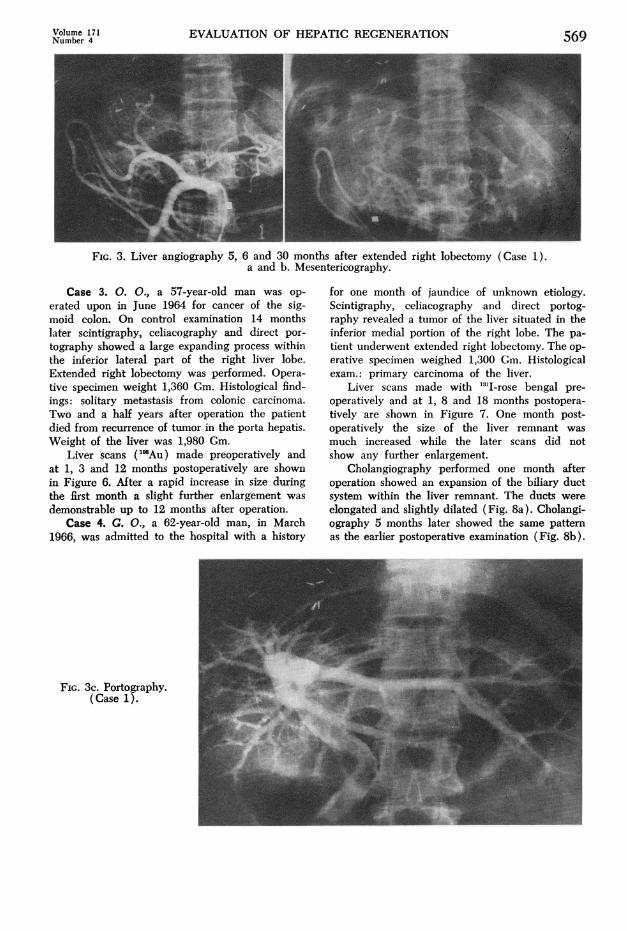
FIG. 3. Liver angiography 5, 6 and 30 months after extended right lobectomy (Case 1).a and b. Mesentericography.
Case 3. 0. O., a 57-year-old man was op-
erated upon in June 1964 for cancer of the sig-moid colon. On control examination 14 monthslater scintigraphy, celiacography and direct por-
tography showed a large expanding process withinthe inferior lateral part of the right liver lobe.Extended right lobectomy was performed. Opera-tive specimen weight 1,360 Gm. Histological find-ings: solitary metastasis from colonic carcinoma.Two and a half years after operation the patientdied from recurrence of tumor in the porta hepatis.Weight of the liver was 1,980 Gm.
Liver scans ("'Au) made preoperatively andat 1, 3 and 12 months postoperatively are shownin Figure 6. After a rapid increase in size duringthe first month a slight further enlargement was
demonstrable up to 12 months after operation.Case 4. G. O., a 62-year-old man, in March
1966, was admitted to the hospital with a history
for one month of jaundice of unknown etiology.Scintigraphy, celiacography and direct portog-raphy revealed a tumor of the liver situated in theinferior medial portion of the right lobe. The pa-
tient underwent extended right lobectomy. The op-
erative specimen weighed 1,300 Gm. Histologicalexam.: primary carcinoma of the liver.
Liver scans made with "3'I-rose bengal pre-
operatively and at 1, 8 and 18 months postopera-tively are shown in Figure 7. One month post-operatively the size of the liver remnant was
much increased while the later scans did notshow any further enlargement.
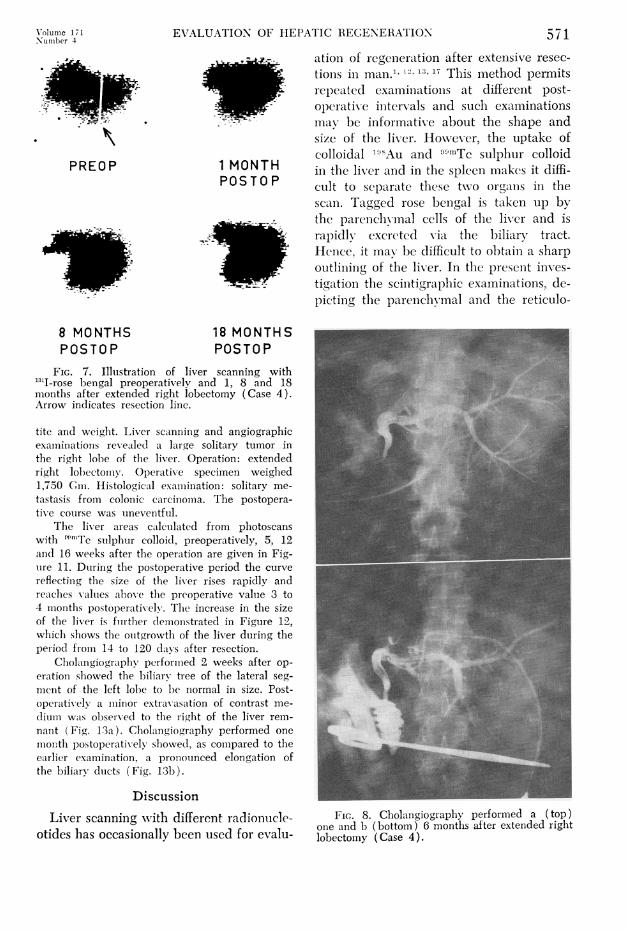
Cholangiography performed one month afteroperation showed an expansion of the biliary ductsystem within the liver remnant. The ducts were
elongated and slightly dilated (Fig. 8a). Cholangi-ography 5 months later showed the same patternas the earlier postoperative examination (Fig. 8b).
FIG. 3c. Portography.(Case 1).
Volume 171Number 4 569

570 ARONSEN AND OTHERS
PR EQ P
lI'i,;.,,:,,. 1 MONTH
_ S&_ POSTOP
_I"o',. 5MONTHS.* .* . 1 ] POS TOP
FIG. 4. Illustration of liver scanning with "98Aupreoperatively and 1 and 5 months after extendedright lobectomy (Case 2). Arrow indicates resec-tion line.
Case 5. J. 0. N., a 23-year-old man sustained ablow against the left inferior part of the chest andwas admiiitted to the hospital. Celiacography per-formed on suspicion of splenic rupture, revealeda normal spleen but a vascular hepatic tumor (5cm. in diameter) in the upper right ventro-lateralportion of the liver (Fig. 9a). The tumor was sup-plied by a feeding branch from the right hepaticartery. Hepatic blood flow estimiation revealed anarterio-venous shunt within the liver. A subseg-mental resection was performed. Histological ex-aminatioin: nodular cirrhosis in otherwise normalliver tissue. Eight months after operation the ar-teriographic pattern was normal (Fig. 9b).
Case 6. T. A., a 56-year-old man was admittedto the hospital in MIay 1966 with a history for 6months of pain in the upper part of the abdomen,gradual loss of appetite and weight. Preoperative
Annals of SurgeryApril 1970
FIG. 5. Portography 5 months after extended rightlobectomy (Case 2).
celiacography showed a large tumor in the rightlobe of the liver. Right lobectomy was performed.The operative specimlen weighed 1,100 Gm. His-tological examination: primary carcinoma of thelixer. The postoperative course was uneventful.
Celiacography 6 months postoperatively showedthe arterial twigs of the left lobe to be distributedto a larger area than preoperatively. Otherwise thearterial structure was normlal ( Fig. 10).
Case 7. A. K., a 65-year-old man was operatedupon for carciniomiia of the sigmoid colon in June1965. Tw,ro Ne.ars later he was readiniitted to thelhospital witlh a history of 4 to 5 imioinths of paiininl the right hypochondrium, gradcual loss of appe-
PREOP 1 MONTH POSTOP
3 MONTHS POSTOP 12 MONTHS POSTOP
FIcG. 6. Illustration of liver scanniing witlh "'Aupreoperatively and 1, 3 and 12 moinths after ex-tended right lobectomy (Case 3). Arrow indicatesresection line.
XVolume 171 EVALUATION OF HEPATIC REGENERATION 57 1Nu-,mber 4
,-.,, ationl of regeneration after extensive resec-
tioIls in man.1 2, 13, 17 This method permitsII' trepeated examiniationis at different post-
F7.: operative initervals and such examinationsmav be informative about the shape andsize of the lixver. Hoowever, the uptake ofcolloidal 1"3Au and "u1Tc sulphur colloid
PREO0P 1 MO0NPTOH in the liver and in the spleen makes it diffi-P0 S TO0 P cult to separate these twvo orgaIns in the
scain. Tagged rose bengial is taken up bythe parenchvimal cclls of the liver and israpidly excreted via the biliary tract.Hence, it max- be difficult to obtain a sharpoutliining of the liver. In the present inves-tigation the sciintigraphic examinations, de-picting the parenchbymal and the reticulo-
8 MONTHS 18 MONTHSPOSTOP POSTOP
FIG. 7. Illustration of liver scanning with"3'I-rose bengal preoperatively and 1, 8 and 18months after extended right lobectomy (Case 4).Arrow indicates resection line.
tite and weight. Liver scanning and angiographicrexa.minations revealed a large solitary tumor inthe right lobe of the liver. Operation: extendedright lohectomv. Operative specimen weighed1,750 Gim. Histological examiiination: solitary me-tastasis from colonic carcinomiia. The postopera-tive course was uneventful.
The liver areas calculated from photoscanswith 'n'Tc sulphur colloid, preoperatively, 5, 12anid 16 weeks after the operation are given in Fig-uire 11. During the postoperative period the curvereflecting the size of the liv-er rises rapidly andreaches valtues ahove the preoperative value 3 to4 montlhs postoperatively. The increase in the sizeof the liver is fuirther clemoinstrated in Figure 12,whiclh shows the outgrowtlh of the liver during theperiod from 14 to 120 days after resection.
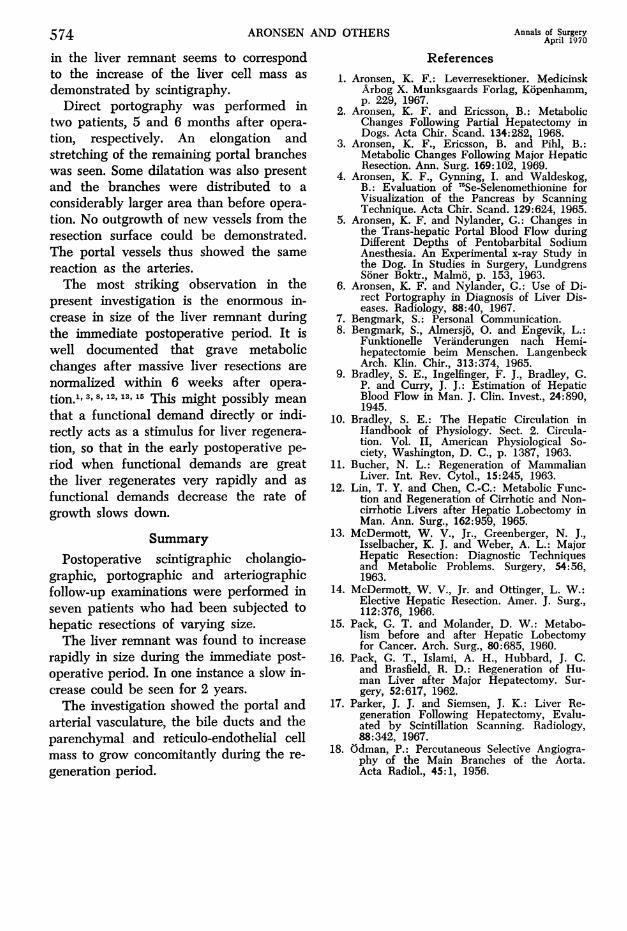
Cholangiography perforimied 2 weeks after op-eration showed the biliarv tree of the lateral seg-mient of the left lobe to be normal in size. Post-operatively a mlinor extravasation of contrast rme- .
dium was observed to the right of the liver reml-naint (Fig. 13a). Cholangiography performed one 4n.
month postoperatively showed, as compared to theearlier examination, a pronotunced elongation ofthe biliarv duicts (Fig. 13b).
DiscussionLiver scanning xvith different radionucle- FIG. 8. Chollngiography performed a (top)
otides has occasionally been used for evaiu-one and b (bottom) 6 months after extended rightlobectomy (Case 4).I .

ARONSEN AND OTHERS
FIG. 10. Mesenterico-celiacography of Case 6, per-formed 6 months after right side lobectomy.
crease in size could be registered for as
long as 2 years in Case 1. In Case 7 theliver was larger than preoperatively 4months after operation. This can be ex-
plained by a recurrence of tumor in theliver, demonstrable at this time.
Parker and Siemsen state that regenera-
tion takes the formn of an outgrowth of newlobes. Other investigators 12, 13, 16 stress that
AREANORMALIZED
1.11
FIG. 9. Celiacography of Case 5. a. (top)Preoperatively and b. (bottom) 8 months aftersubsegmental liver resection.
endothelial cells, respectively, show thatthe liver remnants grow very rapidly dur-ing the first postoperative months. Such a
rapid regeneration has also been reportedby Lin et al.,2 McDermott et al.,3 Packet al.l' and Parker et al.17McDermott et al.13 and Pack et al.'6 feel
that the regeneration was completed within6 months after extended right lobectomywhile Parker and Siemsen reported a re-
generation time of only 2 months. In thepresent investigation, however, a slow in-
1.0 -
0.9 -
0.8 -
0.7-
0.6 -
0.5 -
0.4 -
T 2 4 6 8 10 12 14 16OP WEEKS AFTER OPERATION
FIG. 11. Calculated liver areas from scan with99mTc sulphur colloid during the postoperativeperiod (Case 7).
Annals of SurgeryApril 1970572

EVALUATION OF HEPATIC REGENERATION
FIG. 12. Superimposed photoscannings with9mTc sulphur colloid (14 and 120 days) afterextended right lobectomy. Gray-the liver rem-nant 14 days after operation. White-increase inthe liver remnant size 106 days later. Black-out-lining of the spleen.
the liver regenerates as an enlargement ofthe liver remnant. This is in agreementwith the results of the present investigation.Pack et al.'5 1962 estimated liver weight
at an exploratory laparotomy 21 monthsafter extended right lobectomy to be 1,200Gm. In Case 2 in the present investigationthe patient died 6 months after extendedright lobectomy and at autopsy the liverweight was 1,480 Gm. There was an iso-lated hepatic metastasis measuring 1 x 1
cm.
FIG. 13. Cholangiog-raphy performed. a.(left) 14 and b. (right)30 days after extendedright lobectomy (Case7).
From the case reports it is clear that thebiliary duct system grows very rapidly dur-ing the first postoperative month but there-after grows more slowly. Cholangiographicfindings thus correspond very well with thescintigraphic results.
In the literature we have found only one
report of arteriography after hepatic re-
section.'4 The authors did not commentupon the pictures. It is however evidentthat resection of the dorso-caudal segmentof the right lobe had been performed. The
remaining branches of the right hepaticartery, i.e., the branches to the ventro-cranial segment, are stretched and elon-gated and distributed to a larger area thannormally seen.
In one patient (Case 5) who underwentsubsegmental resection of the right lobe an
arteriogram, 8 months later showed a nor-
mal vascular pattern.After lobectomy (Cases 1, 6) arteriog-
raphies performed 5, 6 and 30 months post-operatively showed an elongation of theintrahepatic arteries of the liver remnant.The vessels were also distributed to a con-
siderably larger area than before operation.No outgrowth of new vessels from the re-
section surface could be seen. Thus thearteriographic pattern after hepatic resec-
tion depends on the extent of resection.The growth of the arterial vascular bed
Volume 171Number 4 573
574 ARONSEN AND OTHERS Annals of SurgeryApril 1970
in the liver remnant seems to correspondto the increase of the liver cell mass asdemonstrated by scintigraphy.
Direct portography was performed intwo patients, 5 and 6 months after opera-tion, respectively. An elongation andstretching of the remaining portal brancheswas seen. Some dilatation was also presentand the branches were distributed to aconsiderably larger area than before opera-tion. No outgrowth of new vessels from theresection surface could be demonstrated.The portal vessels thus showed the samereaction as the arteries.The most striking observation in the
present investigation is the enormous in-crease in size of the liver remnant duringthe immediate postoperative period. It iswell documented that grave metabolicchanges after massive liver resections arenormalized within 6 weeks after opera-tion.1, 3, 8, 12,13,15 This might possibly meanthat a functional demand directly or indi-rectly acts as a stimulus for liver regenera-tion, so that in the early postoperative pe-riod when functional demands are greatthe liver regenerates very rapidly and asfunctional demands decrease the rate ofgrowth slows down.
SummaryPostoperative scintigraphic cholangio-
graphic, portographic and arteriographicfollow-up examinations were performed inseven patients who had been subjected tohepatic resections of varying size.The liver remnant was found to increase
rapidly in size during the immediate post-operative period. In one instance a slow in-crease could be seen for 2 years.The investigation showed the portal and
arterial vasculature, the bile ducts and theparenchymal and reticulo-endothelial cellmass to grow concomitantly during the re-generation period.
References1. Aronsen, K. F.: Leverresektioner. Medicinsk
Arbog X. Munksgaards Forlag, Kopenhamm,p. 229, 1967.
2. Aronsen, K. F. and Ericsson, B.: MetabolicChanges Following Partial Hepatectomy inDogs. Acta Chir. Scand. 134:282, 1968.
3. Aronsen, K. F., Ericsson, B. and Pihl, B.:Metabolic Changes Following Major HepaticResection. Ann. Surg. 169:102, 1969.
4. Aronsen, K. F., Gynning, I. and Waldeskog,B.: Evaluation of 7'Se-Selenomethionine forVisualization of the Pancreas by ScanningTechnique. Acta Chir. Scand. 129:624, 1965.
5. Aronsen, K. F. and Nylander, G.: Changes inthe Trans-hepatic Portal Blood Flow duringDifferent Depths of Pentobarbital SodiumAnesthesia. An Experimental x-ray Study inthe Dog. In Studies in Surgery, LundgrensSoner Boktr., Malmo, p. 153, 1963.
6. Aronsen, K. F. and Nylander, G.: Use of Di-rect Portography in Diagnosis of Liver Dis-eases. Radiology, 88:40, 1967.
7. Bengmark, S.: Personal Communication.8. Bengmark, S., Almersjo, 0. and Engevik, L.:
Funktionelle Veranderungen nach Hemi-hepatectomie beim Menschen. LangenbeckArch. Klin. Chir., 313:374, 1965.
9. Bradley, S. E., Ingelfinger, F. J., Bradley, G.P. and Curry, J. J.: Estimation of HepaticBlood Flow in Man. J. Clin. Invest., 24:890,1945.
10. Bradley, S. E.: The Hepatic Circulation inHandbook of Physiology. Sect. 2. Circula-tion. Vol. II, American Physiological So-ciety, Washington, D. C., p. 1387, 1963.
11. Bucher, N. L.: Regeneration of MammalianLiver. Int. Rev. Cytol., 15:245, 1963.
12. Lin, T. Y. and Chen, C.-C.: Metabolic Func-tion and Regeneration of Cirrhotic and Non-cirrhotic Livers after Hepatic Lobectomy inMan. Ann. Surg., 162:959, 1965.
13. McDermott, W. V., Jr., Greenberger, N. J.,Isselbacher, K. J. and Weber, A. L.: MajorHepatic Resection: Diagnostic Techniquesand Metabolic Problems. Surgery, 54:56,1963.
14. McDermott, W. V., Jr. and Ottinger, L. W.:Elective Hepatic Resection. Amer. J. Surg.,112:376, 1966.
15. Pack, G. T. and Molander, D. W.: Metabo-lism before and after Hepatic Lobectomyfor Cancer. Arch. Surg., 80:685, 1960.
16. Pack, G. T., Islami, A. H., Hubbard, J. C.and Brasfield, R. D.: Regeneration of Hu-man Liver after Major Hepatectomy. Sur-gery, 52:617, 1962.
17. Parker, J. J. and Siemsen, J. K.: Liver Re-generation Following Hepatectomy, Evalu-ated by Scintillation Scanning. Radiology,88:342, 1967.
18. Odman, P.: Percutaneous Selective Angiogra-phy of the Main Branches of the Aorta.Acta Radiol., 45:1, 1956.