Angel Catheter Clinical Evidence Packet
19
CLINICAL EVIDENCE Bio2 Medical, Inc. 4670 Table Mountain Dr., Golden, CO 80403 www.bio2medical.com Toll Free: 866-949-4805 Phone: 303-422-4181 Fax: 303-422-4182 Email: [email protected]
-
Upload
stacy-brewer-mba -
Category
Health & Medicine
-
view
68 -
download
4
Transcript of Angel Catheter Clinical Evidence Packet

CLINICAL EVIDENCEBio2 Medical, Inc.4670 Table Mountain Dr., Golden, CO 80403www.bio2medical.comToll Free: 866-949-4805Phone: 303-422-4181Fax: 303-422-4182Email: [email protected]

CLINICAL NEED
Pulmonary Embolism (PE) Timing After Traumatic Injury .........................................4
VTE Prophylaxis Algorithm for Hospitalized Trauma Patients ..............................5–6
Complications of VTE Prophylaxis in Trauma .............................................................7
Risk and Benefits of IVC Filters ....................................................................................8
IVC Filter Complications ..............................................................................................9
CLINICAL EXPERIENCE
Case Study: Angel® Catheter Pilot Study ................................................................11
The European Angel® Catheter Registry ............................................................12–13
Angel® Catheter Pivotal Study ............................................................................14–18
ANGEL® CATHETERCLINICAL EVIDENCE

CLINICAL NEED
Despite being the most preventable cause of hospital death, PE claims 100,000 lives every year, and it is estimated that 300,000 individuals per year are diagnosed with PE.1 This life-threatening occurrence is exceptionally difficult to diagnose and is often missed; in fact, for every PE that is identified, two can be missed.
Worse yet, due to high risk of bleeding, there is a large population of trauma and ICU patients—nearly 1 million underserved patients in the U.S. annually—contraindicated for anticoagulation, at high risk for PE, and left unprotected from PE.2
Clinical studies show that an effective treatment in PE prophylaxis in these high-risk patients is the inferior vena cava (IVC) filter; however, up to 66% of filters are not retrieved, causing long-term complications such as migration, perforation, and fracture of the filter.3
The unmet clinical need in the treatment of PE is substantial, and the Angel® Catheter addresses this need with ingenuity by providing trauma surgeons with more control, immediacy, and efficacy in PE prophylaxis.
1 Dalen, JE, and Alpert, JS, “Natural History of Pulmonary Embolism,” Prog Cardiovasc Dis 1975;17:257-270.
2 Martinson, M., and Martinson, N., “Pulmonary Embolism Study.” Feb. 2016.3 J Vasc Interv Radiol 2011; 22:1522–1530.

4
PE TIMING AFTER TRAUMATIC INJURY
The American Journal of Surgery (2011) 201, 209–215.
# O
F PA
TIE
NTS
WIT
H
PULM
ON
ARY
EM
BO
LUS
TIME TO PULMONARY EMBOLISM (DAYS)
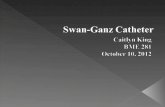
FIGURE 1 The timing of PE after injury.
0
5
20
25
10
15
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
0
2
8
10
12
4
6
0 5 10 15 20 25 30
# O
F PA
TIE
NTS
WIT
H
PULM
ON
ARY
EM
BO
LUS
TIME TO PULMONARY EMBOLISM (DAYS)
FIGURE 2 The timing of PE by injury type.
0
2
8
10
12
4
6
0 5 10 15 20 25 30
• PEs occur within the first 12 days, with peak incidence at day 2
• For 57% of patients, the initiation of chemical prophylaxis was delayed by more than 24 hours
• PEs occur despite current thromboembolic prophylaxis; 74% of patients had chemical prophylaxis before the occurrence of the PE
• 91% of the filters were placed after the diagnosis of PE
Head Injury (AIS>3)
Extremity Fracture

5
VTE RISK FACTORS?YES NO
CONTRAINDICATIONS
FREE AMBULATORY (SEE NEXT PAGE)
“Preventing Venous Thromboembolism | Johns Hopkins Armstrong Institute.” Johns Hopkins Medicine, Web. 14 June 2016.
YESYES
SPECIFIC CONTRAINDICATION TO ENOXAPARIN?
• Use TEDs/SCOs until contraindication no longer present
• Perform serial duplex surveillance
• Consider vena cava (temporary) filter in high-risk trauma patients
HIGH RISK WITH SPECIFIC CONTRAINDICATIONS TO ENOXAPARIN?
• Unfractioned Heparin 5000 units sc q8h
• Plus TEDs/SCDs
• Perform serial duplex surveillance
HIGH RISK WITHOUT SPECIFIC CONTRAINDICATIONS TO ENOXAPARIN?
• Enoxaparin 30 mg sc q12h
• Use TEDs/SCDs
• Perform serial duplex surveillance
• Use TEDs/SCOs until contraindication no longer present
• Perform serial duplex surveillance
• Consider vena cava (temporary) filter in high-risk trauma patients
YES
YESYESYES
NO
NO
HIGH RISK WITHCONTRAINDICATIONS?
HIGH RISK WITHSYSTEMIC ANTICOAGULATION?
VTE PROPHYLAXIS ALGORITHM FOR HOSPITALIZED TRAUMA PATIENTS

6
VTE RISK FACTORS?YES
CONTRAINDICATIONS (SEE PREVIOUS PAGE)
FREE AMBULATORY
*CONTRAINDICATIONS*CONTRAINDICATIONS
NO
• Use TEDs/SCDs until contraindication no longer present
• Perform serial duplex surveillance
• Consider vena cava (temporary) filter in high-risk trauma patients
• No pharmacologic prophylaxis needed
• Use TEDs/SCDs
• No pharmacologic prophylaxis needed
• Use TEDs/SCDs
• No pharmacologic prophylaxis needed
• Use TEDs/SCDs
• Use TEDs/SCDs until contraindication no longer present
• Perform serial duplex surveillance
• Consider vena cava (temporary) filter in high-risk trauma patients
• Unfractionated Heparin 5000 units sc q8h
• Plus TEDs/SCDs• Perform
serial duplex surveillance
• Enoxaparin 30 mg sc q12h
• Use TEDs/SCDs• Perform serial
duplex surveillance
YES YES NO YES YESYES
YES YES
YES
MODERATE RISK, NOT FREELY AMBULATORY
WITH SYSTEMIC ANTICOAGULATION?
FREELY AMBULATORY, MODERATE RISK WITH SYSTEMIC
ANTICOAGULATION?
MODERATE RISK, NOT FREELY
AMBULATORY WITH CONTRAINDICATIONS?
MODERATE RISK, NOT FREELY
AMBULATORY WITH SPECIFIC
CONTRAINDICATIONS TO ENOXAPARIN?
MODERATE RISK, NOT FREELY
AMBULATORY AND WITHOUT SPECIFIC
CONTRAINDICATIONS TO ENOXAPARIN?
FREELY AMBULATORY, MODERATE RISK WITH CONTRAINDICATIONS?
*SPECIFIC CONTRAINDICATION TO ENOXAPARIN?
FREELY AMBULATORY, MODERATE
RISK WITHOUT CONTRAINDICATIONS?
YESYES
NO
“Preventing Venous Thromboembolism | Johns Hopkins Armstrong Institute.” Johns Hopkins Medicine, Web. 14 June 2016.
YES
VTE PROPHYLAXIS ALGORITHM FOR HOSPITALIZED TRAUMA PATIENTS
NONO

7
*344 patients randomized and assessed for bleeding, whereas only 265 patients had venograms adequate for DVT analysis ISS, Injury Severity Score; SCD, Sequential Compression Device; IPC, Intermittent Pneumatic Compression
Datta, et al. Journal of Trauma Management & Outcomes 2010. 4:1.
SUMMARY OF RANDOMIZED LMWH TRAUMA STUDIES THAT REPORT BLEEDING COMPLICATIONS
The following chart summarizes the complication rates of anticoagulants when used for VTE prophylaxis in trauma patients.
COMPLICATIONS OF VTE PROPHYLAXIS IN TRAUMA
STUDY DESIGN TYPE OF LMWH NUMBER OF PATIENTS NON-FATAL BLEEDING FATAL BLEEDING
Geerts, et al. 1996 [10]
Randomized
UH 5,000 U SC BID vs. LMWH 30 mg SC BID
Multi-system trauma & ISS ≥ 9
Enoxaparin 171* 5 (2.9%) 0
Knudson, et al. 1996 [20]
Randomized
LMWH 30 mg SC BID vs. SCD or AVI bilaterally
Multi-system trauma & AIS ≥ 3 with ISS >10
Enoxaparin 120 6 (5%) 0
Ginzburg, et al. 2003 [19]
Randomized
LMWH 30 mg BID vs. IPC bilaterally
Multi-system trauma & ISS ≥ 9
Enoxaparin 218 13 (6%) 0
Green, et al. 1990 [17]
Randomized
UH 5,000 U SC TID vs. LMWH 3500 U SC QD
Spinal cord trauma & complete motor paralysis Logiparin 20 0 0
Spinal Cord Injury Thromboprophylaxis Investigators 2003 [18]
Randomized
UH 5,000 U SC TID + IPC vs. LMWH 30 mg SC BID
Spinal cord trauma
Enoxaparin 230 6 (2.6%) 0
Kortoglu, et al. 2004 [13]
Randomized
LMWH 40 mg QD vs. IPC bilaterally
Head and spinal traumaEnoxaparin 60 2 (3.3%) 0
MULTISYSTEM TRAUMA BLEEDING RISK 24/509 (4.7%) 0%
SPINAL CORD TRAUMA BLEEDING RISK 8/310 (2.6%) 0%COMBINED TOTAL BLEEDING RISK 32/819 (3.9%) 0%

8
Prophylactic Indication:
Pulmonary Embolism:
Mean Insertion
Time:
Mean Retrieval
Time:
Filters Retrieved:
JVIR
JVIR
JVIR
JVIR
JVIR
57%1.3%7 DAYS
52 DAYS
34%
RISK AND BENEFITS OF IVC FILTERS
J Vasc Interv Radiol. 2011; 22:1522-1530.
CLINICAL STUDY
Systematic Review of the Use of Retrievable Inferior Vena Cava Filters
Luis F. Angel, MD, Victor Tapson, MD, Richard E. Galgon, MD, MS, Marcos I. Restrepo, MD, MS, John Kaufman, MD
ABSTRACT
Purpose To review the available literature on retrievable inferior vena cava (IVC) filters to examine the effectiveness and risks of these devices.
Materials and Methods Investigators searched MEDLINE for clinical trials evaluating retrievable filters and reviewed the complications reported to the Manufacturer and User Facility Device Experience (MAUDE) database of the U.S. Food and Drug Administration (FDA).
Results Eligibility criteria were met by 37 studies comprising 6,834 patients. All of the trials had limitations, and no studies were randomized. There were 11 prospective clinical trials; the rest were retrospective studies. Despite the limitations of the evidence, the IVC filters seemed to be effective in preventing pulmonary embolism (PE); the rate of PE after IVC placement was 1.7%. The mean retrieval rate was 34%. Most of the filters became permanent devices. Multiple complications associated with the use of IVC filters were described in the reviewed literature or were reported to the MAUDE database; most of these were associated with long-term use (> 30 days). At the present time, the objective comparison data of different filter designs do not support superiority of any particular design.
Conclusions In high-risk patients for whom anticoagulation is not feasible, retrievable IVC filters seem to be effective in preventing PE. Long-term complications are a serious concern with the use of these filters. The evidence of the effectiveness and the risks was limited by the small number of prospective studies.

9
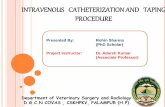
IVC FILTER COMPLICATIONS
• Significant complications associated with traditional IVC filter designs
- Complications include: deployment issues, migration, perforation, fracture, and lack of retrieval
- 66% of retrievable IVC filters are never retrieved—mean implantation time of removed filters is approximately 52 days
Deployment 79.7%
Perforation 9.1%
Migration 7.3%
Other 3.9%
7% OF COMPLICATIONS OCCUR IN FIRST 30 DAYS
Fracture27.3%Retrieval
16.0%
Other 10%
Migration24.6%
Perforation21.6%
93% OF COMPLICATIONS OCCUR AFTER 30 DAYS
J Vasc Interv Radiol. 2011; 22:1522–1530.

CLINICAL EXPERIENCE

11
CASE STUDY:ANGEL® CATHETER PILOT STUDY
INTRODUCTION: The objective of this pilot study was to assess the safety of a new device for pulmonary embolism (PE) prophylaxis. The device, the Angel® Catheter, was placed in eight patients who were in the intensive care unit and were at high risk for PE. The device was inserted at the bedside without fluoroscopic guidance via a femoral venous approach.
RESULT: In subject #7, a significant venous thrombo-embolism (VTE) was captured by the Angel® Catheter and pulled into the left iliac vein. The Angel® Catheter was successfully removed and documented as providing excellent performance.
CONCLUSION: In conclusion, the Angel® Catheter successfully provided protection from a life-threatening VTE while providing access to the central venous system for administration of therapeutic agents, blood withdrawal, and monitoring of central venous pressure.
Thrombus Burden Seen Extending Proximally From Filter (Left Iliac Vein)
Thrombus Captured in the Angel® Catheter Filter
Vena Cava Clear of Thrombus After Angel® Catheter Removal
Significant VTE Captured in Filter, Withdrawn to Iliac Vein
Commercial Filter Placed in Supra-Renal Location
CAPTURE OF SIGNIFICANT THROMBUS

12
Averted-PE rate of approximately 5–23%*
ORIGINAL ARTICLE
THE EUROPEAN ANGEL® CATHETER REGISTRY
A new device for the prevention of pulmonary embolism in critically ill patients: Results of
the European Angel Catheter RegistryFabio S. Taccone, MD, PhD; Nicholas Bunker, MD; Carl Waldmann, MA, MB, BChir;
Daniel De Backer, MD, PhD; Karim Brohi, MD; Robert G. Jones, MRCP; and Jean-Louis Vincent, MD, PhD, Brussels, Belgium
BACKGROUND:
METHODS:
RESULTS:
CONCLUSION:
LEVEL OF EVIDENCE:
KEY WORDS:
Pulmonary embolism (PE) is a potentially life-threatening complication of critical illness. In trauma and neurosurgical patients with contraindications to anticoagulation, inferior vena cava (IVC) filters have been used to prevent PE, but their associated long-term complication rates and difficulties associated with filter removal have limited their use. The Angel catheter is a temporary device, which combined an IVC filter with a triple-lumen central venous catheter (IVC filter–catheter) and is intended for bedside placement and removal when no longer indicated.
This study presents data from a European Registry of 60 critically ill patients in whom the IVC filter–catheter was used to prevent PE. The patients were all at high risk of PE development or recurrence and had contraindications to anticoagulation. The primary end points of this study were to evaluate the safety (in particular, the presence of infectious or thrombotic events) and effectiveness (the numbers of PEs and averted PEs) of the IVC filter–catheter.
The main diagnosis before catheter insertion was major trauma in 33 patients (55%), intracerebral hemorrhage or stroke in 9 (15%), a venous thromboembolic event in 9 (15%), and active bleeding in 6 (10%). The IVC filter–catheter was placed as prophylaxis in 51 patients (85%) and as treatment in the 9 patients (15%) with venous thromboembolic event. The devices were inserted at the bedside without fluoroscopic guidance in 54 patients (90%) and within a median of 4 days after hospital admission. They were left in place for a mean of 6 days (4–8 days). One patient developed a PE, without hemodynamic compromise; two PEs were averted. No serious adverse events were reported.
Early bedside placement of an IVC filter–catheter is possible, and our results suggest that this is a safe, effective alternative to short-term PE prophylaxis for high-risk patients with contraindications to anticoagulation. (J Trauma Acute Care Surg. 2015;79: 456–462. Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.)
Therapeutic study, level V.
Pulmonary embolism; venous thromboembolism; inferior vena cava filter; heparin hematologic.
Active Bleeding 10%
Severe Trauma
55%
Intracerebral Bleeding or
Stroke 15%
VTE 15%
Burns 2% Not Reported 3%
ANGEL® CATHETER PATIENT TYPES N=60
*Clot detection before retrieval range ≥2 cm – ≤2 cm, 5% and 23%, respectively.

13
THE EUROPEAN ANGEL® CATHETER REGISTRY
J Trauma Acute Care Surg. 2015: 79:3. 456-462.
*No filter detachment and was a result of catheter movement
REGISTRY EVENTS WITH ANGEL® CATHETER ANGEL® CATHETER (N=60)
Adverse Events (AEs) Total Occurrence Occurrence related to the Angel® Catheter
None 43/60 (71.7%) 0 (0%)
Catheter Related Blood Stream Infection (CRBSI) 0 in 381 catheter days 0 in 381 catheter days
Death 12/60 (20.0%) 0 (0%)
Guidewire kinked 1/60 (1.7%) 0 (0%)
Migration > 2 cm* 2/60 (3.3%) 2/60 (3.3%)
Inadvertent removal of the Angel® Catheter 4/60 (6.7%) 0 (0%)
Unable to visualize IVC filter during KUB 1/60 (1.7%) 0 (0%)
Pulmonary Embolism 1/60 (1.7%) 0 (0%)
Sepsis 1/60 (1.7%) 0 (0%)

14
ANGEL® CATHETER PIVOTAL STUDY
PRIMARY ENDPOINTS • Freedom from clinically significant PE or fatal PE at
the time of discharge or up to 72 hours after device removal, whichever is first
• Freedom from fatal PE: Unexpected death within 24 hours of onset of the acute event
SECONDARY ENDPOINTS • Incidence of acute proximal deep vein thrombosis• Incidence of catheter-related thrombosis• Incidence of catheter-related bloodstream infections• Incidence of major bleeding event • Incidence of PEs averted
1. Cooper Health Hospital—Camden, NJ2. University of Texas Health Science Center
at San Antonio—San Antonio, TX3. Ben Taub Hospital—Houston, TX4. Medical Center of the Rockies—
Loveland, CO5. Regional One Health—Memphis, TN6. Mercy Hospital—St. Louis, MO7. Broward Health Medical Center—
Fort Lauderdale, FL8. University of New Mexico Hospital—
Albuquerque, NM9. Delray Medical Center—
Delray Beach, FL10. St. Mary’s Medical Center—
West Palm Beach, FL11. Cedars-Sinai Medical Center—
Los Angeles, CA12. University of California, San Diego—
San Diego, CA13. Wake Forest Baptist Medical Center—
Winston-Salem, NC
14. Medical University of South Carolina—Charleston, SC
15. John Peter Smith Hospital—Fort Worth, TX16. UF Health Shands Hospital—Gainesville, FL17. Mount Sinai Hospital—New York, NY18. St. Luke’s University Hospital—
Bethlehem, PA19. University of Miami Hospital—Miami, FL20. Vanderbilt University Medical Center—
Nashville, TN21. Los Angeles County and University of
Southern California Medical Center— Los Angeles, CA
22. University of Mississippi Medical Center—Jackson, MS
23. University of Maryland Medical Center—Baltimore, MD
24. HonorHealth Scottsdale Osborn Medical Center—Scottsdale, AZ
25. Indiana University Health Methodist Hospital—Indianapolis, IN
26. Boston Medical Center—Boston, MA
PRIMARY OBJECTIVEThe primary objective of this clinical trial was to evaluate the safety and effectiveness of the Angel® Catheter in subjects at high risk of PE and with recognized contraindications to standard pharmacological therapy.
STUDY INFORMATION • Single-arm, multicenter, prospective study• 26 Level I and Level II research trauma centers across the United States • A total of 172 subjects were consented across the U.S. The device was
successfully placed in 163 eligible subjects [intention-to-treat (ITT) population]; 151 of these subjects had the device in place for at least 48 hours [per-protocol (PP) population]
• The most common indication for placement of the device was recognized contraindication to the use of anticoagulation in 160/163 (98.2%) of subjects

15
ANGEL® CATHETER 510(k) CLEARANCE
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
Food and Drug Administration 10903 New Hampshire Avenue Document Control Center - WO66-G609 Silver Spring, MD 20993-0002
July 28, 2016
Bio2 Medical, Inc. Ms. Julie Ross Director, Quality Assurance and Regulatory Affairs 4670 Table Mountain Drive Golden, CO 80403
Re: K160747
Trade/Device Name: Angel Catheter Regulation Number: 21 CFR 870.3375 Regulation Name: Cardiovascular Intravascular Filter Regulatory Class: Class II Product Code: PNS Dated: June 24, 2016 Received: June 27, 2016 Dear
Ms. Ross:
We have reviewed your Section 510(k) premarket notification of intent to market the device referenced above and have determined the device is substantially equivalent (for the indications for use stated in the enclosure) to legally marketed predicate devices marketed in interstate commerce prior to May 28, 1976, the enactment date of the Medical Device Amendments, or to devices that have been reclassified in accordance with the provisions of the Federal Food, Drug, and Cosmetic Act (Act) that do not require approval of a premarket approval application (PMA). You may, therefore, market the device, subject to the general controls provisions of the Act. The general controls provisions of the Act include requirements for annual registration, listing of devices, good manufacturing practice, labeling, and prohibitions against misbranding and adulteration. Please note: CDRH does not evaluate information related to contract liability warranties. We remind you, however, that device labeling must be truthful and not misleading.
If your device is classified (see above) into either class II (Special Controls) or class III (PMA), it may be subject to additional controls. Existing major regulations affecting your device can be found in the Code of Federal Regulations, Title 21, Parts 800 to 898. In addition, FDA may publish further announcements concerning your device in the Federal Register.
Please be advised that FDA's issuance of a substantial equivalence determination does not mean that FDA has made a determination that your device complies with other requirements of the Act or any Federal statutes and regulations administered by other Federal agencies. You must comply with all the Act's requirements, including, but not limited to: registration and listing (21 CFR Part 807); labeling (21 CFR Part 801); medical device reporting (reporting of medical device- related adverse events) (21 CFR 803); good manufacturing practice requirements as set forth in
Page 2 - Ms. Julie Ross the quality systems (QS) regulation (21 CFR Part 820); and if applicable, the electronic product radiation control provisions (Sections 531-542 of the Act); 21 CFR 1000-1050.
If you desire specific advice for your device on our labeling regulation (21 CFR Part 801), please contact the Division of Industry and Consumer Education at its toll-free number (800) 638-2041 or (301) 796-7100 or at its Internet address http://www.fda.gov/MedicalDevices/ResourcesforYou/Industry/default.htm. Also, please note the regulation entitled, "Misbranding by reference to premarket notification" (21 CFR Part 807.97). For questions regarding the reporting of adverse events under the MDR regulation (21 CFR Part 803), please go to http://www.fda.gov/MedicalDevices/Safety/ReportaProblem/default.htm for the CDRH's Office of Surveillance and Biometrics/Division of Postmarket Surveillance.
You may obtain other general information on your responsibilities under the Act from the Division of Industry and Consumer Education at its toll-free number (800) 638-2041 or (301) 796-7100 or at its Internet address http://www.fda.gov/MedicalDevices/ResourcesforYou/Industry/default.htm.
Sincerely yours,
Brian D. Pullin -S
for Bram D. Zuckerman, M.D. Director Division of Cardiovascular Devices Office of Device Evaluation Center for Devices and Radiological Health
Enclosure
INTENDED USEThe Angel® Catheter is intended to provide the combined functions of an inferior vena cava (IVC) filter and a multi-lumen central venous catheter.
The Angel® Catheter is intended for short-term use for the prevention of clinically significant Pulmonary Embolism (PE) in critically ill patients at high risk for PE or recurrent PE, and recognized contraindications to standard pharmacological thromboprophylaxis therapy.
The Angel® Catheter is also intended to provide access to the central venous system.
CONTRAINDICATIONS• Patients with a known IVC with a diameter of >30 mm (megacava)• Patients with a known IVC with a diameter of <15 mm• Patients with risk of septic embolism• Patients with known allergic reactions to nickel
Angel® Catheter is the first and only IVC filter to receive 510(k) clearance from the FDA for a prophylactic use indication in critically ill patients.

16
Type of Trauma: Head Injury/Spinal
85.4% Active or High Risk of
Bleeding 95.6%
Multiple VTE Risk Factors
Hypercoagulable Patients
Baseline DVT 11.0%
High Injury Severity Score
(ISS)27.7 +/- 11.9
Immobile Patients
PIVOTAL STUDY
SUBJECT CHARACTERISTICS
ITT Population (N=163)
(160/163)
(8/163)
(10/162)
98.2%
4.9%
6.2%
Patient has contraindications to standard pharmacological thromboprophylaxis
Subject has a confirmed acute proximal lower extremity DVT or a confirmed acute PE
Subject requires a temporary interruption of pharmacological thromboprophylaxis for a surgical or medical procedure
Angel® Catheter Pivotal Study.
ANGEL® CATHETER PIVOTAL STUDYPATIENT CHARACTERISTICS
WHO BENEFITS FROM PE PROTECTION?

17
0 2120191817161514131211109876543210
0.2
0.4
0.6
0.8
1.0
PRO
POR
TIO
N F
RE
E F
RO
M D
VT
TIME (DAYS) TO EVENT
95% Confidence Limits
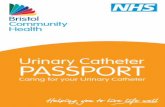
ANGEL® CATHETER PIVOTAL STUDY CLINICAL ENDPOINT ANALYSIS
Angel® Catheter (N=163) 0 Days 1 Day 2 Days 3 Days 4 Days 5 Days 6 Days 7 Days 14 Days 21 Days
Number of Patients At Risk 163 163 161 157 150 138 124 111 93 15
Proportion Free From DVT 1.000 1.000 1.000 0.994 0.967 0.946 0.931 0.881 0.703 0.574
Number of New DVT Events 0 0 0 1 4 3 2 6 12 2
Number of Patients Exited Without a New DVT Event 0 2 4 6 8 11 11 12 66 13
TIME TO ACUTE PROXIMAL DEEP VEIN THROMBOSIS—FREEDOM FROM DVT ANALYSIS, ITT POPULATION
Kaplan-Meier curve shows the timing to event of a new acute proximal DVT and the risk-benefit opportunity for the Angel® Catheter.

18
Angel® Catheter Pivotal Study.
ANGEL® CATHETER PIVOTAL STUDY RESULTS
PATIENT BENEFITS (ITT)
SafeSafety Endpoints
0 CRBSI
• Acute proximal DVT (18.4%, 30/163)
• CRBSI (0%, 0/163)
• Major bleeding events (3.1%, 5/163)
• Catheter-related DVT (12.3%, 20/163)
EfficientPlacement | Retrieval
EASE OF USE
• Duration of ICU placement (avg. 14 min)
• Duration of removal (avg. 14 min)
EffectiveClinical Benefits
AVERTS PULMONARY EMBOLISM
• Averted PE (11%, 14/129 in patients with cavogram)• Freedom from clinically significant PE (100%, 163/163)• Freedom from fatal PE (100%, 163/163)
CLINICAL BENEFIT OF THE ANGEL® CATHETER—ITT POPULATION

AD-056 Rev C
Learn more about Bio2 Medical and the Angel® Catheter by visiting
www.Bio2Medical.com/angel-catheter.
bio2medical.com
Reference the full Instructions For Use (IFU).
Catalog Number AC3930A is commercially available only in the U.S.©2016 Bio2 Medical Inc. All rights reserved. Bio2 Medical® and Angel® trademarks are registered and owned by Bio2 Medical, Inc.
For information on patents covering Bio2 Medical® products, please visit www.bio2medical.com/patents