ANESTHETIC MANAGEMENT OF PRE-INDUCTION SUBACUTE …
6
ANESTHETIC MANAGEMENT OF PRE-INDUCTION SUBACUTE LEFT VENTRICULAR WALL RUPTURE: A CASE REPORT Soniya R Sulhyan 1 *, Anand T Vagarali 1 , Sharangouda S Patil 1 and Mahadev D Dixit 1 Case Report Rupture of the free wall of the Left Ventricle (LV) is a fatal complication of acute myocardial infarction (AMI). The clinical presentation varies from the acute form which has a high mortality rate to the formation of a pseudoaneurysm. Sudden electromechanical dissociation in the Operating Room (OR) has many clinical possibilities and it warrants rapidious surgical intervention in a hemodynamically unstable patient. This rare case report discusses the challenges faced by the anaesthetist in the diagnosis and management of a subacute form of left ventricular free wall rupture (LVFWR) before the induction of anaesthesia in the OR. Keywords: Subacute left ventricular wall rupture, Anesthetic management, Acute myocardial infarction, Electromechanical dissociation *Corresponding Author: Soniya R Sulhyan [email protected] INTRODUCTION Left ventricular free wall rupture (LVFWR) is a fatal, infrequent and serious complication of acute myocardial infarction (AMI) occurring in 2-4% of patients (Palwasha Sahibzada et al., 2009). It is the second most common cause of death after AMI (James Figueras et al., 1997) and accounts for approximately 20% of infarct related deaths (Luis Raposo et al., 2006). Rupture generally occurs between 1-7 days after the AMI (Nicholas T Kouchoukos et al., 2013). An acute LV wall rupture leads to sudden extravasation of blood from the ventricle into the pericardial cavity, causing acute cardiac tamponade. This event ISSN 2278 – 5221 www.ijpmbs.com Vol. 3, No. 2, April 2014 © 2014 IJPMBS. All Rights Reserved Int. J. Pharm. Med. & Bio. Sc. 2014 1 Department of Cardiothoracic and Vascular Anesthesia and Surgery, KLE University’s Jawaharlal Nehru Medical College, Krishna floor, Near ITU (Intensive Therapy Unit), Dr. Prabhakar Kore’s Hospital and Medical Research Centre, Nehrunagar, Belgaum-590010, Karnataka, India. leads to decrease in the circulating blood volume in the body producing signs and symptoms of shock. It also significantly compromises the diastolic filling of the left ventricle due to LV compression by the enormous amount of blood in pericardial cavity thereby decreasing the perfusion to all organs. The present rare case report is of subacute LVFWR leading to electromechanical dissociation occuring just before induction of anesthesia. CASE PRESENTATION A female patient aged 76 years, who had recent anterior wall myocardial infarction (AWMI) and was thrombolysed with Inj. Streptokinase, was
Transcript of ANESTHETIC MANAGEMENT OF PRE-INDUCTION SUBACUTE …

40
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
ANESTHETIC MANAGEMENT OF PRE-INDUCTION
SUBACUTE LEFT VENTRICULAR WALL RUPTURE:
A CASE REPORT
Soniya R Sulhyan1*, Anand T Vagarali1, Sharangouda S Patil1 and Mahadev D Dixit1
Case Report
Rupture of the free wall of the Left Ventricle (LV) is a fatal complication of acute myocardialinfarction (AMI). The clinical presentation varies from the acute form which has a high mortalityrate to the formation of a pseudoaneurysm. Sudden electromechanical dissociation in theOperating Room (OR) has many clinical possibilities and it warrants rapidious surgical interventionin a hemodynamically unstable patient. This rare case report discusses the challenges facedby the anaesthetist in the diagnosis and management of a subacute form of left ventricular freewall rupture (LVFWR) before the induction of anaesthesia in the OR.
Keywords: Subacute left ventricular wall rupture, Anesthetic management, Acute myocardialinfarction, Electromechanical dissociation
*Corresponding Author: Soniya R Sulhyan � [email protected]
INTRODUCTION
Left ventricular free wall rupture (LVFWR) is a
fatal, infrequent and serious complication of acute
myocardial infarction (AMI) occurring in 2-4% of
patients (Palwasha Sahibzada et al., 2009). It is
the second most common cause of death after
AMI (James Figueras et al., 1997) and accounts
for approximately 20% of infarct related deaths
(Luis Raposo et al., 2006). Rupture generally
occurs between 1-7 days after the AMI (Nicholas
T Kouchoukos et al., 2013). An acute LV wall
rupture leads to sudden extravasation of blood
from the ventricle into the pericardial cavity,
causing acute cardiac tamponade. This event
ISSN 2278 – 5221 www.ijpmbs.com
Vol. 3, No. 2, April 2014
© 2014 IJPMBS. All Rights Reserved
Int. J. Pharm. Med. & Bio. Sc. 2014
1 Department of Cardiothoracic and Vascular Anesthesia and Surgery, KLE University’s Jawaharlal Nehru Medical College, Krishna floor, Near
ITU (Intensive Therapy Unit), Dr. Prabhakar Kore’s Hospital and Medical Research Centre, Nehrunagar, Belgaum-590010, Karnataka, India.
leads to decrease in the circulating blood volume
in the body producing signs and symptoms of
shock. It also significantly compromises the
diastolic filling of the left ventricle due to LV
compression by the enormous amount of blood
in pericardial cavity thereby decreasing the
perfusion to all organs. The present rare case
report is of subacute LVFWR leading to
electromechanical dissociation occuring just
before induction of anesthesia.
CASE PRESENTATION
A female patient aged 76 years, who had recent
anterior wall myocardial infarction (AWMI) and
was thrombolysed with Inj. Streptokinase, was

41
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
admitted to the hospital for ongoing chest pain
and shortness of breath. She was a known
hypertensive and was euthyroid and therefore
was not on thyroid supplement for hypothyroidism.
She underwent coronary angiography which
revealed critical Left Main (LM) artery stenosis
with thrombus in the LM extending to proximal
left anterior descending artery (LAD) and proximal
left circumflex artery (LCX). In addition, she had
plaque in mid LAD. Her right coronary artery
(RCA) was normal. Her transthoracic
echocardiography (TTE) revealed LV dysfunction
with ejection fraction (EF) of 40%. Her distal
Interventricular Septum (IVS), apex, and anterior
wall were a kinetic. Mild pericardial effusion was
present.
Because of her ongoing chest pain, she was
taken up for emergency coronary artery bypass
grafting (CABG). After shifting her to OR and while
the electrocardiography (ECG) electrodes were
being applied, she had sudden cardiac arrest.
She was immediately intubated with 8 mm portex
cuffed endotracheal tube under vision without any
inducing drugs or muscle relaxants. A peripheral
venous cannula of 16 G was inserted immediately
and Inj. Adrenaline given IV. Emergency
sternotomy was done, only to find the pericardium
full of fresh blood and clots, which had lead to
cardiac tamponade. A rent was seen in the
infarcted anterior region of LV. Emergency
cardiopulmonary bypass (CPB) was set up with
right atrial cannulation with arterial cannulation to
ascending aorta after adequate heparinization.
Patient was cooled to 28oC. The rent in the LV,
i.e., the ruptured akinetic portion of LV was excised
and surgical restoration of LV was done using
polytetrafluroethylene (PTFE) felt on either side
of ruptured LV edges and double layer
approximation of PTFE felt and refashioned LV
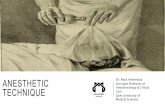
edges using 1 no. Ethicon 30 mm needle (Figure
1). CABG x 3 grafts were done, anastomosing
Saphenous Vein Grafts (SVG) to LAD, Obtuse
Marginal 2 (OM2) and Posterior Descending (PD)
arteries. A 7.5 Fr 16 cm triple lumen central venous
catheter was inserted into the right subclavian vein.
Patient was then rewarmed and successfully
weaned off with inotropic support and intraaortic
balloon pump (IABP) support. However, chest wall
closure was deferred and patient shifted to ITU.
Figure 1: Intraoperative Photograph of LVFree Wall Showing the Extensive RupturedPortion Secured with PTFE Felt on EitherSide of Ruptured LV Edges and DoubleLayer Approximation of PTFE Felt and
Refashioned LV Edges Using 1No. Ethicon 30 mm Needle
On 2nd postoperative day, the chest was
closed. Patient continued to do well and on 5th
postoperative day her IABP was removed.
Her renal parameters were deranged in the
postoperative period. She had to be reintubated
and her renal failure progressed and she went
into low cardiac output. Hemodialysis was not
possible because of hypotension. She had
cardiac arrest on 8th postoperative day and inspite
of all resusciative measures, she died.

42
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
DISCUSSION
The time of occurrence classifies post AMI
LVFWR into two subtypes, early and late;
occurring 48 hours before and after the episode
of acute MI (Figueras et al., 2000).
There are 3 forms of post- AMI LVFWR
classified according to the time of occurrence and
form of presentation. The acute form of ventricular
rupture is the most common form usually
occuring on the first day of AMI and is fatal. Acute
LVFWR leads to acute cardiac tamponade due
to rapid development of massive hemopericardium
and compromises diastolic filling of both left and
right ventricles leading to decreased stroke
volume and cardiac output. This leads to rapid
electromechanical dissociation and sudden
death. The “oozing type” or subacute form is
marked by small leak through a friable myocardial
tissue leading to pericardial effusion without
significant cardiac tamponade. As in our case,
acute blowout rupture can occur in the subacute
form after initial AMI if left untreated (Figueras et
al., 2000; Qiping Chenet al., 2004; and James W
Bard, 2000). The third type is the “chronic type”
which leads to the pseudoanerysm formation
(Qiping Chen et al., 2004; and James W Bard,
2000).
LV ruptures are also classified into 4 patterns.
Type I has an almost direct trajectory with little
dissection. Type II has a multicanalicular trajectory
with extensive myocardial dissection and bloody
infiltration. Type III has the orifice of rupture
protected either by a thrombus or by a pericardial
symphysis. Type IV is an incomplete rupture such
that the trajectory does not extend completely
through the muscle (Hasan Ekim et al., 2009).
Risk factors for ventricular free wall rupture
after an acute MI include female gender, older age,
hypertension, single vessel disease, and
transmural infarctions with relatively good
ventricular function and AWMI (Qiping Chenet al.,
2004; and Hasan Ekim et al., 2009).
Sudden hypotension and bradycardia with
cyanosis and loss of consciousness is an
indicator of impending rupture (Hasan Ekim et
al., 2009). LVFWR should be suspected in
patients who have recurrent or persistent chest
pain after an acute transmural infarction,
hemodynamic instability, syncope, signs of
pericardial tamponade-neck vein distension,
cyanosis, pallor, shock with hypotension, pulsus
paradoxus, elevated venous pressure, quiet heart
sounds, diastolic equalization of central venous
pressure (CVP), pulmaonary artery pressure and
pulmonary capillary wedge pressure, steep X
descent and blunted Y descent on CVP, sinus
bradycardia, nodal rhythm or transient
electromechanical dissociation (Nicholas T
Kouchoukos et al., 2013; Figueras et al., 2000;
James W Bard, 2000; and Hasan Ekim et al.,
2009).
ECG shows low voltage QRS complex,
electrical alterans, T wave changes.
Echocardiogram shows pericardial effusion with
or without evidence of cardiac tamponade.
Pericardiocentesis may be useful for establishing
the diagnosis of hemopericardium and therapeutic
for relieving the tamponade (James W Bard,
2000).
Successful medical management of subacute
LVFWR has been reported. Percutaneous
intrapericardial fibrin-glue injection therapy (PIFIT)
has been tried as an alternative for LVFWR
instead of surgical repair and has found to be quite
effective (Masayoshi Terashim et al., 2008).
Extracorporeal Membrane Oxygenation (ECMO)

43
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
can also be used as a bridge to recovery or for
safer surgery after 7 to 10 days (Golbarg Abedi-
Valugerdi et al., 2012). But surgical therapy
appears to be the definite therapy (Figueras et
al., 2000; and James W Bard, 2000). Surgical
repair can be achieved by 3 surgical techniques.
Direct closure with suture reinforced by Teflon
felt is used for small lacerations. Infarctectomy
and Teflon felt–reinforced suture closure is
possible in small infarctions. A rent can be closed
with a felt sandwich, bovine pericardium or
prosthetic patch using various novel techniques
like double patch sealing method secured by
glues, sutures or both (James W Bard, 2000; and
Hideki Amano et al., 2002). Sutureless techniques
have also been used, for example in slow
leakages (Golbarg Abedi-Valugerdi et al., 2012).
PTFE felt, polyester or pericardial patches can
be placed over the site of rupture and sutured
with various glues like Gelatin-Resorcin-
Formaldehyde-Glutaraldehyde (GRF), fibrin,
cyanoacrylate (Nicholas T Kouchoukoset al.,
2013).
This is a case of subacute LVFWR which
progressed to acute blow out rupture. There are
two possibilities, either it is a case of acute on
subacute rupture, and not a case of acute rupture
because it occurred on the 9th day after AWMI
because Kirklin et al. say that acute rupture
usually occurs between 1- 7 days of acute MI
(Nicholas T Kouchoukoset al., 2013), or it is a
delayed form of acute rupture. Diagnosis of acute
on subacute rupture of the LV free wall is difficult
in the OR, mainly because of the differential
diagnoses like acute massive pulmonary
embolism, acute anaphalactoid reaction to
antibiotics because these are usually given before
induction and spontaneous tension pneumothorax
because of ruptured emphysematous bullae
(Qiping Chen et al., 2004). The diagnosis of
subacute LVFWR is mostly made from diagnosis
of hemopericardium and cardiac tamponade by
two dimensional echocardiography (James Slater
et al., 2000), cardiac catheterisation or
pericardiocentesis and the signs associated
thereof (Augusto Purcaro et al., 1997). To the
authors’ best knowledge, there are no reported
cases of spontaneous subacute LVFWR on the
operating table in the OR just before induction of
anaesthesia. Such a condition, provides even no
time for placement of intravenous and intra-arterial
lines. Immediate institution of CPR with rapidious
placement of intravenous line for IV bolus of
resuscitation drugs is the key.
Role of IABP is very well established in
ventricular septal rupture secondary to AMI. But
its role in LVFWR is controversial (Nicholas T
Kouchoukos et al., 2013; James W Bard, 2000;
and Hasan Ekim et al., 2009). Placement of an
IABP by one part of the surgical team provides
afterload reduction and may buy time before
insertion of arterial and venous cannulae before
going on CPB. In this case, IABP was inserted
for optimizing coronary perfusion while
simultaneous sternotomy and manual direct
cardiac compressions were given.
Rapid infusion of blood and blood products is
very crucial in such case. On the cardiopulmonary
bypass, 3 packed cell volume units and 2 whole
blood units were added.
The post bypass anesthetic management is
very crucial in this case. Optimal hemodynamics
with mean arterial pressures to maintain adequate
perfusion pressures but to avoid excess strain
on the sutured LV wall is extremely important. The
spherical shape of the LV cavity changes from
spherical. Also, the LV volume is reduced. It also

44
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
requires the use of inotropes to support the
contractility of the heart but to maintain the same
perfusion pressures and a urine output of 1 mL/
kg/h. In our case, high dosage of inotrope infusion
was required to maintain adequate pressures, IV
Dobutamine 10 mcg/ kg/ min, IV Adrenaline 0.15
mcg/kg/min and IV Vasopressin 1 U/hr. IV
Milrinone 0.5 mg/kg/min was also started later in
the postoperative period while decreasing the
Dobutamine dose. Fluid overloading must be
avoided.
Achieving optimal hemostasis in this case is
a challenge. The patient was on IV Heparin since
9 days. CPB also is a known cause for platelet
dysfunction and a trigger for initiation of a complex
cascade of coagulation, firinolysis and
inflammatory pathways. Heparin infusion was
needed to maintain ACT between 130-160 s due
to the presence of IABP. Chest closure was
deferred in our case because of unstable
hemodynamics.
Because of the rapid sterile cleaning and
draping of the patient, followed by deferred chest
closure postoperatively, IV Meropenem 1 g thrice
a day (TID) was started. IV Metronidazole 500
mg TID was started for covering anaerobic
infection.
Immediate recognition of subacute LVFWR is
a challenge and requires high degree of suspicion.
The immediate institution of CPR with immediate
insertion of IABP with emergency sternotomy,
followed by manual cardiac compressions and
rapidious institution of CPB with maintenance of
adequate perfusion pressures is a must. All these
measures were done to increase the perfusion
pressures. Since the patient hemodynamically
collapsed before placing any intravenous or
intraarterial catheters, recognition of arterial
pressures was not possible. Placement of
intravenous and one intraarterial catheter,
preferably radial should be encouraged
preoperatively in the preoperative room. There
was no evidence of cardiac tamponade or
pericardial effusion on the preoperative chest
radiograph. However, the TTE had revealed mild
pericardial effusion.
REFERENCES
1. Augusto Purcaro, Carlo Constantini, Nino
Ciarrpani et al. (1997), “Diagnostic criteria
and management of subacute ventricular
free wall rupture complicating acute
myocardial infarction”, American Journal of
Cardiology, Vol. 80, No. 4, pp. 397-405.
2. Golbarg Abedi-Valugerdi, Anders Gabrielsen,
Thomas Fux et al. (2012), “Management of
left ventricular rupture after myocardial
infarction solely with ECMO”, Circ Heart
Fail, pp. 65-67.
3. Hasan Ekim, Mustafa Tuncer and Halil Basel
(2002), “Repair of ventricular free wall
rupture after acute myocardial infarction: a
case report”, Cases Journal, Vol. 2, p. 9099.
4. Hideki Amano, Kuniyoshi Ohara, Masaki Nie
et al. (2002), “New surgical technique of left
ventricular free wall rupture: Double patch
sealing method”, Ann Thorac Cardiovasc
Surg, Vol. 8, No. 6, pp. 389-392.
5. Figueras J, Cortadellas J and Soler-Soler J
(2000), “Left ventricular free wall rupture:
case presentation and management”,
Heart, Vol. 83, pp. 499-504.
6. James Figueras, Josefa Cortadellas, Arturo
Evangelista et al. (1997), “Medical
management of selected patients with left
ventricular free wall rupture during acute

45
Int. J. Pharm. Med. & Bio. Sc. 2014 Soniya R Sulhyan et al., 2014
myocardial infarction”, JCVA, Vol. 29, No.
3, pp. 512-518.
7. James Slater, Robert J Brown, Tracy A
Antonelli et al. (2000), “Cardiogenic shock
dur to cardiac free-wall rupture or
tamponade after acute myocardial
infarction: Areport from the SHOCK trial
registry”, JACC, Vol. 36, No. 3, Suppl A
September, pp. 1117-22.
8. James W Bard (2000),“ Anesthetic
implications of subacute left ventricular
rupture following acute myocardial
infarction: A case report”, AANA Journal, Vol.
68, No. 5, pp. 415-419.
9. Luis Raposo, Maria Joao Andrade, Jorge
Ferreria et al. (2006), “Subacute left
ventricular rupture after acute myocardial
infaction: awareness of the clinical signs
and early use of echocardiography may be
life-saving”, Cardiovascular Ultrasound, Vol.
4, p. 46.
10. Masayoshi Terashima, Satomi Fujiwara,
Gen-ya Yaginuma et al. (2008), “Outcome
of percutaneous intrapericardial fibrin-glue
injection therapy for left ventricular free wall
rupture secondary to acute myocardial
infarction”, American Journal of Cardiology,
Vol. 101, No. 4, pp. 419-421.
11. Nicholas T Kouchoukos, Eugene H
Blackstone, Frank L Hanley et al. (2013),
“Kirklin/ Barratt-Boyes Cardiac Surgery”,
Chapter 8: Left ventricular aneurysm,
Philadelphia, PA Elsevier Saunders, pp. 441-
442.
12. Palwasha Sahibzada, Niaz Ali, Zahidullah M
et al. (2009), “Ventricular free wall rupture”,
J Ayub Med Coll Abbottabad, Vol. 21, N o.
2, pp. 22-26.
13. Qiping Chen, Bharathi H Scott, Thomas V
Bilfinger et al. (2004), “Pulseless electrical
activity after induction of anesthesia: A
witnessed cardiac rupture”, JCVA, Vol. 18,
No. 6, pp. 767-768.