Anesthetic Management of Pediatric Liver Transplantation ...
6
경희의학 : 제 32 권 제 1 호 □ 증 례 □ J Kyung Hee Univ Med Cent : Vol. 32, No. 1, 2017 - 52 - Anesthetic Management of Pediatric Liver Transplantation for Langerhans Cell Histiocytosis with Central Diabetes Insipidus : A Case Report Seung-Ah Ryu 1 , Jae-Hyuk Lee 1 , Chan-Hee Lee 1 , Sun-Key Kim 2 1 Department of Anesthesiology and Pain Medicine, Seoul Medical Center, Seoul, 2 Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Corresponding author: Sun-Key Kim, Clinical Instructor, Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpagu, Seoul 05505, Korea Tel: +82-2-3010-3876, Fax: +82-2-3010-6790 E-mail: [email protected] INTRODUCTION Langerhans cell histiocytosis (LCH) is a rare immu- nologic disorder occurring mainly in childhood. It involves the abnormal proliferation of histiocytes, genotypically similar to Langerhans cells, in single or multiple organs. Liver involvement manifests with clinical, biochemical, and radiological features of sclerosing cholangitis, and may progress to end-stage chronic liver disease.(1) The presence of a large volume of ascites in end-stage chronic liver disease can cause intravascular volume depletion during anesthesia. Central diabetes insipidus (DI) is characterized by polyuria and elevation in serum sodium and osmolality. Correction of hypernatremia requires replacement of both water and electrolyte deficits, and it is important to assess the patient’s plasma volume status as in the setting of significant hypovolemia. It is also important to determine the rate of correction, as there is a risk of cerebral edema if the sodium level is corrected too rapidly. We report a case of a 3-year-old girl with LCH and central DI, who underwent liver transplantation under general anesthesia. We present details of the successful management of the volume status and sodium level. To our knowledge, this is the first report of pediatric liver transplantation in a patient with LCH in Korea. CASE REPORT The female patient, born at 38 weeks gestation weighing 3.02 kg, had no remarkable previous develop- mental episode. She presented as a 2-year-old with dermatitis seborrheica, polydipsia, polyuria, and abdominal distention, and was diagnosed with LCH, liver disease (classified as Child-Pugh class C and with a pediatric end-stage liver disease score of 22) and central DI (Fig. 1). The patient was treated with chemotherapy for the LCH, and desmopressin for the central DI. Her sodium level was poorly controlled between the range of 131 to 159 mmol/L, and she experienced seizure with drowsy mentality several times due to the abrupt decrease in sodium level. She
Transcript of Anesthetic Management of Pediatric Liver Transplantation ...

경희의학 : 제 32 권 제1 호 □ 증 례 □
J Kyung Hee Univ Med Cent : Vol. 32, No. 1, 2017
- 52 -
Anesthetic Management of Pediatric Liver Transplantation for Langerhans Cell Histiocytosis with Central Diabetes Insipidus
: A Case Report
Seung-Ah Ryu1, Jae-Hyuk Lee1, Chan-Hee Lee1, Sun-Key Kim2
1Department of Anesthesiology and Pain Medicine, Seoul Medical Center, Seoul, 2Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Corresponding author: Sun-Key Kim, Clinical Instructor, Department of Anesthesiology and Pain Medicine, Asan Medical
Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpagu, Seoul 05505, KoreaTel: +82-2-3010-3876, Fax: +82-2-3010-6790
E-mail: [email protected]
INTRODUCTION
Langerhans cell histiocytosis (LCH) is a rare immu-
nologic disorder occurring mainly in childhood. It
involves the abnormal proliferation of histiocytes,
genotypically similar to Langerhans cells, in single or
multiple organs. Liver involvement manifests with
clinical, biochemical, and radiological features of
sclerosing cholangitis, and may progress to end-stage
chronic liver disease.(1) The presence of a large
volume of ascites in end-stage chronic liver disease can
cause intravascular volume depletion during anesthesia.
Central diabetes insipidus (DI) is characterized by
polyuria and elevation in serum sodium and osmolality.
Correction of hypernatremia requires replacement of
both water and electrolyte deficits, and it is important
to assess the patient’s plasma volume status as in the
setting of significant hypovolemia. It is also important
to determine the rate of correction, as there is a risk of
cerebral edema if the sodium level is corrected too
rapidly.
We report a case of a 3-year-old girl with LCH and
central DI, who underwent liver transplantation under
general anesthesia. We present details of the successful
management of the volume status and sodium level. To
our knowledge, this is the first report of pediatric liver
transplantation in a patient with LCH in Korea.
CASE REPORT
The female patient, born at 38 weeks gestation
weighing 3.02 kg, had no remarkable previous develop-
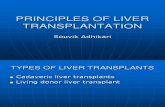
mental episode. She presented as a 2-year-old with
dermatitis seborrheica, polydipsia, polyuria, and
abdominal distention, and was diagnosed with LCH,
liver disease (classified as Child-Pugh class C and with
a pediatric end-stage liver disease score of 22) and
central DI (Fig. 1). The patient was treated with
chemotherapy for the LCH, and desmopressin for the
central DI. Her sodium level was poorly controlled
between the range of 131 to 159 mmol/L, and she
experienced seizure with drowsy mentality several
times due to the abrupt decrease in sodium level. She
− Seung-ah Ryu, et al:Anesthetic Management of Pediatric Liver Transplantation for Langerhans Cell Histiocytosis with Central Diabetes Insipidus −
- 53 -
Fig. 1. The whole body magnetic resonance imaging
showed Langerhans cell histiocytosis involve-
ment in both distal femurs, liver cirrhosis with
large amount of ascites
had several episodes of variceal bleeding in the
gastrointestinal tract. The medical team considered her
suitable for orthotopic liver transplantation after achie-
ving complete remission from the LCH. However, the
LCH was refractory, and as the patient developed
severe jaundice during the chemotherapy, finally the
chemotherapy ceased. She was admitted for liver trans-
plantation workup and her abdominal circumference
was found to have increased by about 18 cm since she
was last discharged from our medical center. During
the workup, desmopressin treatment was interrupted
due to acute renal failure, which required continuous
renal replacement therapy; desmopressin was repeatedly
resumed for a few days to combat polyuria and
increased sodium levels, but was finally stopped.
Ascites were drained continuously via the peritoneal
dialysis catheter for 2 days before the operation to
avoid abrupt volume depletion during surgery.
At preanesthetic assessment, the patient’s weight was
14.5 kg and height was 89 cm. She was severely
jaundiced, with hepatosplenomegaly. Laboratory test
results were as follows: hemoglobin, 10.4 g/dL; white
blood cell count, 17.1 x 109/L; platelets, 66 x 10
9/L;
sodium, 156 mmol/L; potassium, 4.2 mmol/L; glucose,
97 mg/dL; creatinine, 0.31 mg/dL; albumin, 3.7 g/dL;
aspartate transaminase, 186 IU/L; alanine transaminase,
83 IU/L; total bilirubin, 112.4 mg/dL; ammonia, 765
mol/L; and troponin-I, 0.018 ng/mL. On imaging,
there was no evidence of a pituitary mass; there were,
however, right frontal and left parietal parenchymal
lesions, and brain involvement of LCH could not be
excluded, and there was evidence of sclerosing
cholangitis caused by involvement of LCH. Her mental
status was alert.
In the operating room, electrocardiograph, pulse
oximetry, cerebral oximetry, and bispectral index
monitors were applied. We also monitored arterial
blood pressure and central venous pressure by placing
intravascular catheters into the right femoral artery and
left internal jugular vein, respectively. Her vital signs
were as follows: systolic/diastolic arterial blood pressure,
71/43 mmHg; heart rate, 125 beats/min; and central
venous pressure, 9 mmHg. Arterial blood gas analysis
results as follows: pH, 7.50; PaCO2, 34 mmHg; PaO2,

− 경희의학 제32 권 제1 호 2017 −
- 54 -
Table 1. Cahnges of Electrolytes and Vital Signs during Liver Transplantation Surgery in a 3-year-old Child with
Langerhans Cell Histiocytosis and Central Diabetes Insipidus
Before induction Preanhepatic phase Anhepatic phase After reperfusion
Electrolytes
Na+ (mmol/L) 148 149 148 148
K+ (mmol/L) 4.6 3.9 3.4 3.6
Ca2+ (mg/dL) 9.4 7.8 8.5 7.7
Vital sings
SBP/DBP (mmHg) 68/42 62/39-95/52 75/44-85/50 65/40-96/54
Heart rate (beats/min) 125 112-123 115-120 110-121
SBP: systolic arterial blood pressure, DBP: diastolic arterial blood pressure
87 mmHg; HCO3-, 22.6 mEq/L; SaO2, 97%. Electro-
lytes were as follows: sodium, 146 mmol/L; potassium,
4.0 mmol/L; calcium, 1.20 mmol/L; and glucose, 65
mg/dL. Hemoglobin was 9.9 g/dL and the hematocrit
was 29%.
General anesthesia was induced with thiopental 75
mg, rocuronium 20 mg, and fentanyl 15 g, and endo-
tracheal intubation was performed. Both breathing
sounds were equal and without rales. Anesthesia was
maintained with sevoflurane in 50% oxygen/air and
continuous fentanyl infusion.
The duration of the operation was 10 hours and 10
minutes, and the duration of anesthesia was 12 hours
and 15 minutes. The prehepatic, anhepatic, and neo-
hepatic phases were 7 hours and 10 minutes, 1 hour
and 5 minutes, and 4 hours, respectively. Postreper-
fusion syndrome did not develop.
After the induction of anesthesia, 600 mL of ascites
were drained via the peritoneal dialysis catheter. A
flow of ascites was observed in the operative field
throughout the operation. About 30 minutes after the
start of the operation, the patient’s systolic/diastolic
arterial blood pressure slowly dropped to 53/33 mmHg;
we therefore started a continuous infusion of norepi-
nephrine at a dose of 0.1 g/kg/min. Her systolic arterial
blood pressure rose within a few minutes and was then
stable at 80 mmHg for most of the operation. The
mean central venous pressure during the prehepatic,
anhepatic, and neohepatic phase was 4, 3, and 5
mmHg, respectively. Urine output during the pre-
hepatic, anhepatic, and neohepatic phase was 48 mL
(6.7 mL/h), 17 mL (16 mL/h), and 300 mL (75 mL/hr),
respectively. The total estimated ascites volume during
the entirety of the operation was 2 L. The level of
sodium during the prehepatic, anhepatic, and neohepatic
phase was 149, 148, and 148 mmol/L, respectively
(Table 1). The volumes of crystalloids administered
were as follows: 170 mL of 5% DNK3, 285 mL of
10% dextrose water, and 1.2 L of plasma solution. The
volume of 5% albumin administered was 2.5 L. Trans-
fused blood products were as follows: red blood cells,
250 mL; fresh frozen plasma, 40 mL; cryoprecipitate, 4
units; and platelet concentrates, 4units.
After the operation, the patient was transferred with
an endotracheal tube to the pediatric intensive care
unit; her weight had dropped by about 4 kg. She
developed polyuria and an elevated sodium level, and
therefore desmopressin treatment was commenced,
which restored normal urination and sodium levels. She
was extubated 2 days after the operation, and imaging
1 month later showed that there was no stenosis at the
portal vein anastomosis site. The patient developed no
new neurologic findings, and resumed oral feeding
without any problem. She was well at discharge.

− Seung-ah Ryu, et al:Anesthetic Management of Pediatric Liver Transplantation for Langerhans Cell Histiocytosis with Central Diabetes Insipidus −
- 55 -
DISCUSSION
LCH is a rare disorder and most commonly charac-
terized by single or multiple osteolytic bone lesions of
infiltrated histiocytes with bean-shaped nuclei evident
at biopsy. These cells, along with lymphocytes, macro-
phages, and eosinophils, may infiltrate nearly every
organ (notably the skin, lymph nodes, lung, thymus,
liver, spleen, bone marrow, or central nervous system,
but not the heart and kidneys). The clinical presen-
tation of patients with LCH varies depending upon the
sites and extent of involvement. Acute disseminated
multisystem disease is most commonly seen in children
less than 3 years of age, while a more indolent disease
involving a single organ is more common in older
children and adults.(2) Liver disease has been reported
to occur in 16–36% of patients with LCH,(3) and
presents with histologically acute hepatitis with abnormal
histiocytes or severe, progressive cholestasis with a bile
duct lesion, and sclerosing cholangitis.(1) The cause of
liver cirrhosis in LCH is not well defined as several
mechanisms have been implicated; these include
histiocytic infiltration, extrinsic compression of the
common bile duct by adenopathy in the hepatic hilus,
histiocytic infiltration of the extrahepatic bile ducts,
drug-induced injury, total parenteral nutrition, and
primary sclerosing cholangitis.(4) Liver transplantation
in patients with LCH is controversial because of the
risk of recurrence of the underlying disease, which can
manifest as a viral, neoplastic, or autoimmune disease.(5)
However, one study asserts that liver transplantation is
the treatment of choice for LCH patients with
progressive sclerosing cholangitis, and that liver
transplantation should be performed as early as possible
in patients with severe hepatic damage.(6)
Central DI is rare in children and characterized by
decreased release of antidiurectic hormone, resulting in
a variable degree of polyuria. Central DI is a disease
caused by idiopathic DI most commonly,(7) and by
primary or secondary tumors or infiltrative diseases
(such as LCH),(8) neurosurgery, and trauma. During
the natural course of LCH, central DI occurs in about
one quarter of patients.(9) It is a syndrome charac-
terized clinically by excretion of abnormally large
volumes of free water,(10) resulting in solute-free
water loss in the urine and hypernatremia. Hyper-
natremia, especially, can cause severe perioperative
morbidity and mortality, and complications range from
headaches, weakness, neuromuscular irritability and
confusion, seizures, coma, or death.(11) Correction of
hypernatremia requires the administration of dilute
fluids to both correct the water deficit and replace
ongoing water losses, and also, when appropriate,
interventions to limit further water loss. In any child
with significant volume depletion, first management
steps should be directed toward ensuring cardiovascular
stability. It is recommended that the rate of correction
should not exceed a fall in sodium of greater than 0.5
mEq/L per hour.(12)
Ascites is defined as the pathologic accumulation of
fluid in the peritoneal cavity.(11) Also ascites is the
most common complication of cirrhosis, which is the
most common cause of ascites, accounting for approxi-
mately 85 percent of cases in the United States.(13)
The formation of ascites is governed by the same
principles as edema formation at other sites, including
net capillary permeability and hydraulic and oncotic
pressure gradients. Portal hypertension and the conse-
quences of vasodilatation are determining factors for
ascites formation in liver cirrhosis.(14)
It is important for the anesthesiologist to carefully
monitor the intravascular volume status and electrolyte
levels. In this case, the patient had liver cirrhosis
caused by LCH with central DI, and central DI results
in excretion of free water. Ascites accumulation is
wasting state of body water. Our patient required

− 경희의학 제32 권 제1 호 2017 −
- 56 -
replacement of both water and electrolyte deficits. To
monitor and control the intravascular volume and
sodium level, we measured arterial blood pressure and
central venous pressure, and received electrolyte
readings from the laboratory, monitoring input and
output frequently. Systolic arterial blood pressure was
maintained at 80 ± 10 mmHg throughout the operation.
Central venous pressure fell suddenly at the start of the
operation, probably because the preoperative central
venous pressure was overestimated due to the ascites.
During the operation, central venous pressure was
maintained constantly at 4 ± 1 mmHg.
We had to consider which of several kinds of fluids
we would administer to the patient. The fluid we used
in anesthesia was plasma solution, 5% DNK3, 10%
dextrose water, 5% albumin; 5% DNK3 and 10%
dextrose water are used for controlling serum glucose
and potassium levels. Plasma solution is a balanced
crystalloid solution (containing sodium at 136 mEq/L)
that is used for volume replacement, but in our patient,
because of her central DI, a crystalloid solution alone
would not effectively increase the circulatory volume,
and would instead lead to generalized edema and cause
too rapid a correction of the sodium level. Albumin is
a colloid prepared from human venous plasma and the
sodium content in the 5% solution is 145±15 mEq/L,
with the usual concentration being 154 mEq/L. The
sodium level we administered, which was evaluated
just before induction of anesthesia, was 146 mmol/L,
and the range in sodium level of the patient’s
measurements during the operation was 142–148
mmol/L. Thus, the regimen that we used of crystalloid
with colloid was able to both correct the water deficit
and control the sodium level.
In conclusion, as demonstrated by this report, it is
very important to optimize the intravascular volume in
cases of water deficit caused by central DI and ascites.
Furthermore, it is also important to strictly control
elevated sodium levels by the administration of various,
well considered fluids.
ABSTRACT
Anesthetic Management of Pediatric Liver
Transplantation for Langerhans Cell
Histiocytosis with Central Diabetes
Insipidus
: A Case Report
Seung-Ah Ryu1, Jae-Hyuk Lee1,
Chan-Hee Lee1, Sun-Key Kim2
1Department of Anesthesiology and Pain Medicine,
Seoul Medical Center, Seoul, 2Department of Anesthesiology and Pain Medicine,
Asan Medical Center, University of Ulsan College of Medicine,
Seoul, Korea
A 3-year-old girl with Langerhans cell histiocytosis
and central diabetes insipidus underwent liver
transplantation under general anesthesia. On arrival at
the operating room, she has severe ascites and
hypernatremia. During the operation, she showed signs
of intravascular volume depletion due to third spacing
by ascites and an excessive urine output caused by the
central diabetes insipidus. The anesthesiologists ende-
avored to administer appropriate fluids to optimize the
volume status and inhibit too rapid correction of the
sodium level. The intraoperative sodium level range
was 142-148 mmol/L, and the central venous pressure
range was 3-5 mmHg. The operation was completed
without complications. Several days after the operation,
she was discharged without any significant problem.
Key Words: Central diabetes insipidus, Langerhans
cell histiocytosis, Liver transplantation

− Seung-ah Ryu, et al:Anesthetic Management of Pediatric Liver Transplantation for Langerhans Cell Histiocytosis with Central Diabetes Insipidus −
- 57 -
REFERENCES
1. Thompson HH, Pitt HA, Lewin KJ, Longmire WP,
Jr. Sclerosing cholangitis and histiocytosis X. Gut
1984;25:526-30.
2. Martin A, Macmillan S, Murphy D, Carachi R.
Langerhans cell histiocytosis: 23 years' paediatric
experience highlights severe long-term sequelae.
Scott Med J 2014;59:149-57.
3. Nezelof C, Frileux-Herbet F, Cronier-Sachot J.
Disseminated histiocytosis X: analysis of prog-
nostic factors based on a retrospective study of 50
cases. Cancer 1979;44:1824-38.
4. Leblanc A, Hadchouel M, Jehan P, Odievre M,
Alagille D. Obstructive jaundice in children with
histiocytosis X. Gastroenterology 1981;80:134-9.
5. Van Thiel DH, Gavaler JS. Recurrent disease in
patients with liver transplantation: when does it
occur and how can we be sure? Hepatology 1987;
7:181-3.
6. Braier J, Ciocca M, Latella A, de Davila MG,
Drajer M, Imventarza O. Cholestasis, sclerosing
cholangitis, and liver transplantation in Langerhans
cell histiocytosis. Med Pediatr Oncol 2002;38:
178-82.
7. Rose BD, Post TW. Clinical physiology of
acid-base and electrolyte disorders. 5th ed. New
York: McGraw-Hill. 2001.
8. Grois N, Fahrner B, Arceci RJ, Henter JI, McClain
K, Lassmann H, et al. Central nervous system
disease in Langerhans cell histiocytosis. J Pediatr
2010;156:873-81, 81.e1.
9. Marchand I, Barkaoui MA, Garel C, Polak M,
Donadieu J. Central diabetes insipidus as the inau-
gural manifestation of Langerhans cell histiocytosis:
natural history and medical evaluation of 26
children and adolescents. J Clin Endocrinol Metab
2011;96:E1352-60.
10. Robertson GL. Diabetes insipidus. Endocrinol
Metab Clin North Am 1995;24:549-72.
11. Adrogue HJ, Madias NE. Hypernatremia. N Engl J
Med 2000;342:1493-9.
12. Fang C, Mao J, Dai Y, Xia Y, Fu H, Chen Y, et
al. Fluid management of hypernatraemic de-
hydration to prevent cerebral oedema: a retro-
spective case control study of 97 children in
China. J Paediatr Child Health 2010;46:301-3.
13. Runyon BA. Management of adult patients with
ascites due to cirrhosis: an update. Hepatology
2009;49:2087-107.
14. Cardenas A, Arroyo V. Mechanisms of water and
sodium retention in cirrhosis and the pathogenesis
of ascites. Best Pract Res Clin Endocrinol Metab
2003;17:607-22.