Basic Principles of Anesthesiology Department of Anesthesiology and Pain Control.

Anesthesia Protocols for Surgery during Neuromonitoring
Anesthesiology, University of Colorado Denver: [email protected] April 1, 2009
A variety of anesthesia methods can be used during surgery where intraoperative neurophysiological
monitoring is used. Clearly the anesthesia must be titrated to each patient to adjust for the various comorbidities, including the degree of neural compromise that may impact monitoring, as well as searching to find an anesthetic that allows an adequate monitoring signal while keeping the patient adequately anesthetized. In general, with respect to monitoring, the choice of anesthesia depends on the particular monitoring modalities being used. The major limitations are when techniques are sensitive to inhalational agents (IH) and when they are sensitive to neuromuscular blocking agents (NMB). Some modalities are insensitive to both (e.g. ABR), others are sensitive to muscle relaxants only (e.g. EMG), or inhalational agents only (e.g. cortical SSEP), and some are sensitive to both inhalational agents and muscle relaxants (e.g. transcranial motor evoked potentials (MEP)). The most restrictive techniques among the techniques used for a specific surgery define the overall anesthetic approach and the protocols below are the protocols which I usually start with for various types of monitoring. I have also mentioned some alternatives to the approach I use. These protocols are for adults; children may require different doses or approaches. Monitoring During Posterior Fossa Surgery
When surgery in the posterior fossa involves only the Auditory Brainstem Response (ABR), there are no anesthetic considerations since this is neither sensitive to inhalational agents or muscle relaxants; any anesthetic technique is fine with respect to monitoring and should be guided to the patient and surgery. In the unlikely event that the Eustacean tube is blocked then Nitrous Oxide could cause a middle ear tension that would make its use a problem.
Anesthesia for ABR (techniques insensitive to IH or NMB) Induction as usual Maintenance as usual (IH and NMB as desired)
The most common addition to ABR is monitoring using EMG of various cranial nerves, especially the
facial nerve. As such the monitoring then becomes sensitive to muscle relaxants. For some EMG techniques where the nervous system is stimulated (e.g. MEP, Pedicle screws), partial muscle relaxation is often acceptable (see below), but when monitoring is designed to be sensitive to mechanical stimulation of the nerves (as is usually the case with cranial nerves) muscle relaxants reduce the EMG amplitude and make the monitoring less sensitive to impending neural injury. For this reason I try to avoid muscle relaxation during the case. In surgeries where ABR is combined with EMG, since there is no inhalational agent restriction, I usually use a balanced anesthetic (e.g. some opioids and inhalational agents) and allow the muscle relaxants that were used with intubation to wear off. Since higher doses of inhalational agents can be used, this anesthetic works fine. The situation gets a bit more complex when the SSEP is used as in cortical surgery.
Anesthesia for ABR with EMG (insensitive to IH sensitive to NMB) Induction as usual Maintenance as usual (IH as desired) Let NMB wear off after induction

Monitoring the Cerebral Cortex
A variety of procedures involve monitoring for potential neural compromise to the cerebral cortex. A good example is Carotid Endarterectomy. If the only monitoring modality is EEG, the anesthesia is made rather easy since it is insensitive to muscle relaxants and only sensitive to high doses of inhalational agents. Hence the choice of anesthesia is usually designed to produce a rhythmic EEG in the alpha range (8‐12 Hz) that is associated with light to moderate anesthesia with inhalational agents. Higher doses will produce burst suppression or electrical silence which impairs monitoring so inhalational doses in the 1 MAC or lower range is usually fine and can be titrated to the EEG. This usually produces excellent anesthesia provided that additional opioids are used to supplement the analgesia (with the inhalational agents producing amnesia and sedation). A processed EEG monitor may be used to help insure adequate sedation in most patients if the IH dose is low (less than ½ MAC). The opioids have the additional advantage of slowing the heart rate and blunting hypertensive episodes which are important in reducing the cardiac risk in these patients. This technique also allows maintenance of the blood pressure in the patient’s usual range and is excellent for TCD monitoring. For this reason I usually load these patients with 1 ug/kg or more of fentanyl (or a similar dose of another opioid) with induction and run a balanced anesthetic with inhalational agents.
Anesthesia for EEG (moderately sensitive to IH insensitive to NMB) Induction as usual Balanced Maintenance (6% Des ~ 1 MAC) Opioids and NMB as needed
Anesthesia comes a bit more difficult if SSEP is used with the EEG for cortical monitoring as would be
done in intracranial aneurysm surgery. Here the inhalational agent must be kept low enough to keep the cortical SSEP responses monitorable. In general, cortical SSEP amplitudes will be acceptable with inhalational agent concentrations between ½ and 1 MAC, however the effect is non‐linear; there is usually a concentration “threshold” in that range above which the cortical SSEP response is markedly reduced in amplitude. The problem is that each patient may have a different threshold so the inhalational agent must be titrated to effect. My approach is to plan a balanced anesthetic with some opioid, muscle relaxants as needed, and adjust the inhalational agent, observing the response. I use Desflurane or Sevoflurane when possible because their insolubility allows rapid increase and decrease of effect. For young, healthy patients with minimal neurological debility I usually start at 1 MAC and titrate down, and for older and neurologically compromised patients I start at ½ MAC and titrate up. Recall that inhalational doses in excess of 1 MAC may produce brain swelling from increased cerebrovascular arterial volume (as well as amplitude depression of the SSEP) so I don’t go above 1 MAC with intracranial cases. If the dose of inhalational agents must be kept low to allow monitoring, I often will add a propofol infusion to insure adequate sedation and opioids as needed. A processed EEG monitor is often helpful with this, provided the electrode contacts with the brain are not altered by the craniotomy and the brain does not move away from the frontal bone. For intracranial surgery this additional infusion of propofol to prevent awareness and sedation is often not necessary (it something about operating on the brain), but there is a high possibility of this in spinal surgery where SSEP is used since awareness appears to be more common.
Anesthesia for Cortical Surgery with SSEP (sensitive to IH insensitive to NMB) Induction as usual, preferably Propofol Balanced Maintenance (3‐6% Des ½‐1 MAC) Opioids and NMB as needed Propofol infusion if needed by EEG

Monitoring during Spinal Surgery using the SSEP
When I am providing anesthesia for spinal surgery where only the SSEP is used (such as spinal corrective surgery below L2), I approach the choice as above – a balanced anesthetic using opioids and muscle relaxation as needed and ½ to 1 MAC inhalational agent (Des) as acceptable to acquire a cortical response (titrating as described above). As opposed to intracranial surgery, I find I usually need a supplemental infusion of propofol and usually use an infusion of opioid. The propofol usually runs at 60‐120 ug/kg/min (often titrated with the help of a processed EEG). For the opioid I usually use sufentanil (unless it’s an elderly frail patient where I bolus fentanyl to effect). Sufentanil infusions usually run 0.15‐0.3 ug/kg/hr, but can be higher depending on the patient’s tolerance from preoperative analgesic use. Note the sufentanil infusion needs to be turned off about 30 minutes before ending. Note that fentanyl (infusion 4‐5 ug/kg/hr) can be used as can remifentanil (0.2‐0.5 ug/kg/min). Fortunately the inhalational agents help a lot with the anesthetic.
Anesthesia for Spinal Surgery with SSEP (sensitive to IH insensitive to NMB) Induction as usual (preferable Propofol) Balanced Maintenance (3‐6% Des ½‐1 MAC) Opioids – sufentanil bolus as needed than 0.15‐0.3 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (60‐120 ug/kg/min) NMB as needed if EMG not monitored
An alternative approach here is to use dexmeditomidine instead of, or supplementary to the
propofol. Some individuals use Dex infusions of 0.2‐0.5 ug/kg/hr. I usually don’t load the Dex (which cuts the cost) if it’s started at the beginning of the case. The infusion of Propofol will be a lower dose due to the sedation from the Dex. Because the mechanism of action is not opioid like (it’s a central alpha2 stimulant), it appears to be helpful in opioid tolerant patients.
Alternate anesthesia for Spinal Surgery with SSEP (sensitive to IH insensitive to NMB) Induction as usual (preferable Propofol) Balanced Maintenance (3‐6% Des ½‐1 MAC) Opioids – sufentanil bolus as needed than 0.15‐0.3 ug/kg/hr turn off 30 minutes before end Dexmeditomidine (0.2‐0.5 ug/kg/hr) Propofol infusion (60‐100 ug/kg/min) NMB as needed if no EMG
If EMG is also monitored with the SSEP (which is usually the case with our surgeries), the muscle
relaxants must be restricted. I prefer to let the muscle relaxants wear off after the beginning of surgery. After the baseline recordings are done, sometimes we will use some relaxation for the opening of a large spinal surgery to reduce the muscle activity or assist in the exposure of an anterior abdominal case. Although I prefer to use no relaxation during the monitoring portion of the procedure, acceptable EMG monitoring can be done with 2 twitches in a train of four, optimally using a titrated infusion of an intermediate acting drug such as rocuronium (5‐10 ug/kg/min) or vecuronium (0.5‐0.8 ug/kg/min). Data suggests that a deeper block (only 1 twitch), may artificially increase the pedicle screw threshold which could reduce the ability to signal the need for repositioning of the screws. In addition, the detection of nerve root compromise from mechanical means might be reduced similar to facial nerve monitoring above, such that no relaxation is desirable. In general, since the sensitivity of muscle groups to muscle relaxants varies, where the TOF is monitored is important. Since distal muscles are most sensitive (and frequently where monitoring is done), if we monitor the TOF using the ulnar nerve and hand response is probably best since more proximal muscles (such as on the face) may underestimate the effect in the
periphery. The best neuromuscular monitoring of TOF will be done by the monitoring team in the muscles they are monitoring (note they need to use the same technique as anesthesia with a TOF at 2 Hz).
Anesthesia for Spinal Surgery with SSEP & EMG (sensitive to IH & NMB) Induction as usual (preferable Propofol) Balanced Maintenance (3‐6% Des ½‐1 MAC) Opioids – sufentanil bolus as needed than 0.15‐0.3 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (50‐150 ug/kg/min) NMB as needed for induction, possibly for muscle dissection then none (acceptable 2+/4 twitches in TOF in muscles monitored for monitoring nerve stimulation)
Monitoring the SSEP when a Reduction or Elimination of the Inhalational Agents is Needed
In general, the ability to use inhalational agents and partial muscle relaxation is very helpful in anesthetizing the spine surgery patients (particularly if they are opioid tolerant). The situation becomes much more difficult when the responses are so poor that the inhalational agent must be reduced or eliminated. In this case the anesthesia becomes a total intravenous anesthetic (TIVA) with the sedation being provided by propofol (75‐150 ug/kg/min, usually titrated to processed EEG) with an opioid infusion (e.g. sufentanil 0.3‐0.5 ug/kg/hr). If the SSEP remains too small for monitoring, an infusion of etomidate (0.6 mg/kg/hr) can be used instead of the propofol (as etomidate enhances the cortical SSEP at low doses). Alternatively a ketamine infusion (1‐2 mg/kg/hr) can be used with the opioid infusion (see below for our approach to ketamine) since ketamine also increases the cortical SSEP response. Since our spine surgeries most often use transcranial motor evoked responses when we need to eliminate the inhalational agents, we take the TIVA approach described below when low dose of inhalational agents are not acceptable for MEP. Monitoring when Motor evoked Potentials are used
The most challenging anesthetic is required during monitoring of surgery when motor evoked potentials are being used because both the inhalational agents and neuromuscular blocking agents must be severely restricted or not used. With these cases SSEP and EMG are also usually being monitored, but the MEP defines the major restrictions. For a medically healthy patient who is without marked neurological problems (i.e. usually presents with severe pain that prompts surgery), I usually start with a TIVA technique supplemented with ½ MAC of inhalational agent (e.g. 3% Des). Some folks start with pure TIVA, but frequently a small amount of Des or Sevo is acceptable and I believe it is helpful, especially with patients who are opioid tolerant. Hence, after a standard induction with propofol and a short or intermediate acting muscle relaxant (which I let wear off), I will use 3% Des, a sufentanil infusion (0.3‐0.5 ug/kg/hr) and a propofol infusion (75‐150 ug/kg/min titrated to processed EEG). Note that some individuals would prefer to use 50‐60% nitrous oxide instead of the Des (but not both IH and N2O together at the same time since they are synergistic and the effect is usually too much). This works similarly but I prefer to not have my FiO2 restricted by nitrous oxide and that when turning the nitrous off in a time of concern may cause an abrupt change in anesthesia and monitoring.
This technique usually works well, but occasionally the MEP responses are too small which necessitates turning off the Des and adjusting the Propofol and sufentanil infusions as needed. It’s important to note that moderate doses of benzodiazepines and barbiturates have been reported to reduce the MEP response and that this may last a long time (much longer than the drug duration of action). It is not clear how this pertains to the modern multipulse technique; however, small doses of midazolam appear quite acceptable such as those that are customarily used for preinduction or occasionally during the case.

Anesthesia for Spinal Surgery with MEP & EMG (very sensitive to IH & NMB) Induction as usual (preferable Propofol) Low dose IH (3% Des) Opioids – sufentanil bolus as needed than 0.15‐0.3 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (75‐150 ug/kg/min) NMB as needed for induction, possibly for muscle dissection then none (acceptable 2+/4 twitches in TOF in muscles monitored for monitoring nerve stimulation)
Monitoring MEP with Opioid Tolerant Patients or Who have Significant Neurological Disability
In patients who are not young and healthy or have moderate neural disability or where turning off the Des is required in the above technique, I usually use pure TIVA using propofol and sufentanil.
Anesthesia for Spinal Surgery with MEP & EMG (very sensitive to IH & NMB) Induction as usual (preferable Propofol) Pure TIVA – no IH Opioids – sufentanil bolus as needed than 0.15‐0.3 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (75‐175 ug/kg/min) NMB as needed for induction, possibly for muscle dissection then none (acceptable 2+/4 twitches in TOF in muscles monitored for monitoring nerve stimulation)
If this isn’t sufficient to allow monitoring, or in patients who are very opioid tolerant or who have
significant neurological debility where the responses are likely to be poor I use TIVA enhanced with ketamine. In this case I use ketamine to supplement the analgesia (recall it has NMDA action that the opioids do not). It also supplements the sedation which allows a reduction in the propofol infusion rate (and a reduction in the depressant effect of the propofol). The notable thing about ketamine is that it is metabolized slower than propofol so that the infusion must be turned down earlier than the propofol. One approach is to run a separate infusion of ketamine (1‐2 mg/kg/hr), but since we currently titrate the sedation to the processed EEG, it’s more convenient to mix the ketamine with the propofol. As such, we mix ketamine in the propofol for an initial infusion that has 2 mg of ketamine in each cc of propofol (e.g. 100 mg ketamine in a 50 cc syringe of propofol). This infusion is titrated to the EEG (since ketamine can increase the numeric value of the processed EEG, I titrate to the high end of the acceptable processed EEG range). This concentration of ketamine is reduced with each subsequent 50 cc syringe of propofol. For a shorter case I usually go 2, then 1.5, then 1, then 0.5 mg of ketamine per cc and use no ketamine in the final syringes. For a much longer case I taper more slowly. Note that the ketamine will increase the SSEP amplitude so you may see a slow decline in SSEP amplitude over the case (often to 50%) and this is expected and must be differentiated from a pathologic change.
Anesthesia for Spinal Surgery with MEP & EMG (very sensitive to IH & NMB) Induction as usual (preferable Propofol) Pure TIVA – no IH Opioids – sufentanil bolus as needed than 0.3‐0.5 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (75‐175 ug/kg/min) Ketamine mixed in the Propofol (initial 2 mg/cc) and tapered to off NMB as needed for induction, possibly for muscle dissection then none (acceptable 2+/4 twitches in TOF in muscles monitored for monitoring nerve stimulation)

The major alternative to this is to use dexmeditomidine as described above. Hence some individuals use <0.5 ug/kg/hr Dexmeditomidine instead of the propofol (or with a small dose of Propofol 50‐60 ug/kg/min). However, I must note that many individuals report that MEP are difficult to obtain with Dex. As such the use of Dex is evolving.
Anesthesia for Spinal Surgery with MEP & EMG (very sensitive to IH & NMB) Induction as usual (preferable Propofol) Pure TIVA – no IH Opioids – sufentanil bolus as needed than 0.3‐0.5 ug/kg/hr turn off 30 minutes before end Propofol infusion guided by EEG (60‐100 ug/kg/min) Dexmeditomidine (0.3‐0.5 ug/kg/hr) NMB as needed for induction, possibly for muscle dissection then none (acceptable 2+/4 twitches in TOF in muscles monitored for monitoring nerve stimulation)
Dexmeditomidine would also be an acceptable alternative in patients where propofol is
contraindicated (such as allergy to soy or eggs or a history of propofol infusion syndrome). Similarly, etomidate could be used. Low dose IH or nitrous oxide might also be acceptable as long as the depressant effect was not excessive.
It is also worth mentioning that in patients where an intravenous line is not available for induction a mask induction with sevoflurane with or without nitrous oxide works fine. Usually these can be eliminated after transition to intravenous techniques in time for the need for intraoperative monitoring. Conclusion
In general, I pick the initial anesthetic technique based on the patient comorbidities (choice of anesthesia drugs independent to monitoring), patient tolerance to analgesics used preoperatively, the degree of patient neural disabilities, the actual surgery to be performed, and the specific monitoring modalities to be used. As such the doses above are only approximate and should be verified as appropriate and adjusted for each individual patient. My goal is to get the maintenance anesthetic on board and see how the monitoring responses are doing, making required changes in the technique as rapidly as possible so that I can have a steady state anesthetic effect during the period of the surgery when monitoring needs to focus on changes that might be the result of surgical or physiological changes (hence infusions are extremely valuable).
I uniformly use the processed EEG to titrate/insure sedation (BIS, Sedline, SNAP, etc.), relying on blood pressure and heart rate to guide adequate analgesia. Although I recognize that these devices will not always insure adequate sedation or anmesia, especially when ketamine is present since it increases the processed indices. However, if recall was to occur, I can say in good faith that I did what might be helpful. I most often use sufentanil with bolus doses around induction and then by infusion. Fentanyl and remifentanil work fine when used in a similar fashion. I favor Desflurane because its insolubility allows rapid changes, however Isoflurane, Sevoflurane and Nitrous Oxide will also work. If a mask induction is used then Sevoflurane is preferable. I also prefer propofol for induction so that the patient is loaded for an infusion (ketamine and dexmeditomidine are described as needing loading doses, but do not appear to need them when used as above). Obviously substitutions may be necessary for individual drug sensitivities and some individuals express concern with propofol in children (propofol infusion syndrome). I also favor no muscle relaxation when the technique is sensitive (especially spontaneous EMG). I recognize that there is ample literature showing partial relaxation is acceptable, however, I am concerned about regulating the degree of relaxation leading to an iatrogenic loss of response.

Usually these protocols work quite well, although I occasionally have a patient a couple times a year who I just can’t keep down. My approach is usually to add inhalational agents so that we maintain the SSEP and EMG monitoring, sacrificing the MEP rather than using NMB and losing the EMG and MEP.

“Clinical topic reviews” are an effort to update and inform the practice. In general, the topics pertain to the overall practice of anesthesiology. On occasion, they specifically address departmental education surrounding new or current clinical circumstances in our workplace at Saint John’s. They may serve as a means of demonstrating compliance with regulatory standards or practice awareness of current standards and guidelines. It may also serve as evidence for participation in FFPE (focused professional practice evaluation). FFPE is a requirement for MOCA (Maintenance of Certification in Anesthesiology). An individual’s participation is voluntary. Your input is valued and encouraged. If you identify, in your element of the practice, a clinical topic that you think warrants increased departmental awareness then you are encouraged to submit ideas for a “clinical topic review.” Forward your ideas to the current VP of Clinical Affairs on the Board of Directors of Western Anesthesiology. Please provide explicit information (eg. Video link, journal article, medical or regulatory website). Chosen topics will be distributed via email. Your attestation that you have participated will be documented with the use of “Survey Monkey.” The frequency of distributions of clinical topics will occur regularly or according to necessity. THIS SESSION'S CLINICAL TOPIC REVIEW IS: "SAFE INJECTION PRACTICES FROM THE JOINT COMMISSION". To view the video, click or paste the below link into your web browser. NEXT, press the arrow in the black screen. http://www.oneandonlycampaign.org/videos/Default.aspx After you are done watching the video, click the survey link and give us your input on this months topic. https://www.surveymonkey.com/s.aspx?sm=bPkVYe52YyvKg9oRyNj8qWwpeuhh9vP6R_2fcCTwMG0Lw_3d Thank you. Respectfully, Andrew M. Barnett, MD

� SPECIAL ARTICLESAnesthesiology 2009; 110:459–79 Copyright © 2009, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Practice Advisory on Anesthetic Care for MagneticResonance Imaging
A Report by the American Society of Anesthesiologists Task Force on AnestheticCare for Magnetic Resonance Imaging*
PRACTICE advisories are systematically developed re-ports that are intended to assist decision making inareas of patient care. Advisories are based on a syn-thesis of scientific literature and analysis of expert andpractitioner opinion, clinical feasibility data, open fo-rum commentary, and consensus surveys. Advisoriesdeveloped by the American Society of Anesthesiolo-gists (ASA) are not intended as standards, guidelines,or absolute requirements. They may be adopted, mod-ified, or rejected according to clinical needs and con-straints.
The use of practice advisories cannot guarantee anyspecific outcome. Practice advisories summarize thestate of the literature, and report opinions obtained fromexpert consultants and ASA members. Practice adviso-ries are not supported by scientific literature to the samedegree as standards or guidelines because of the lack ofsufficient numbers of adequately controlled studies.Practice advisories are subject to periodic revision aswarranted by the evolution of medical knowledge, tech-nology, and practice.
The magnetic resonance imaging (MRI) suite is a haz-ardous location because of the presence of a strongstatic magnetic field, high-frequency electromagnetic(radiofrequency) waves, and a time-varied (pulsed) mag-
netic field. Secondary dangers of these energy sourcesinclude high-level acoustic noise, systemic and localizedheating, and accidental projectiles. There may be signif-icant challenges to anesthetic administration and moni-toring capabilities due to static and dynamic magneticfields as well as radiofrequency energy emissions. Directpatient observation may be compromised by noise, dark-ened environment, obstructed line of sight, and othercharacteristics unique to this environment (e.g., distrac-tions). Unlike a conventional operating room, the MRIenvironment frequently requires the anesthesiologist toassume broader responsibility for immediate patient caredecisions.
Methodology
A. Definition of Anesthetic Care for MRI and High-risk ImagingThis Advisory defines anesthetic care for MRI as mod-
erate sedation, deep sedation, monitored anesthesiacare, general anesthesia, or ventilatory and critical caresupport. High-risk imaging refers to imaging in patientswith medical or health-related risks; imaging with equip-ment-related risks; and procedure-related risks, such asMRI-guided surgery, minimally invasive procedures (e.g.,focused ultrasound, radiofrequency ablation), or cardiacand airway imaging studies.
B. PurposeThe purposes of this Advisory are to (1) promote
patient and staff safety in the MRI environment, (2)prevent the occurrence of MRI-associated accidents, (3)promote optimal patient management and reduce ad-verse patient outcomes associated with MRI, (4) identifypotential equipment-related hazards in the MRI environ-ment, (5) identify limitations of physiologic monitoringcapabilities in the MRI environment, and (6) identifypotential health hazards (e.g., high decibel levels) of theMRI environment.
C. FocusThis Advisory focuses on MRI settings where anes-
thetic care is provided, specifically facilities that aredesignated as level II or III (appendix 1). Level IIrefers to facilities that image patients requiring moni-toring or life support. Level III refers to facilities thatare designed for operative procedures. This Advisory
Supplemental digital content is available for this article. DirectURL citations appear in the printed text and are available inboth the HTML and PDF versions of this article. Links to thedigital files are provided in the HTML text of this article on theJournal’s Web site (www.anesthesiology.org).
�
* Developed by the American Society of Anesthesiologists Task Force on Anes-thetic Care for Magnetic Resonance Imaging: Jan Ehrenwerth, M.D. (Co-chair),Madison, Connecticut; Mark A. Singleton, M.D., San Jose, California (Co-chair);Charlotte Bell, M.D., Milford, Connecticut, Jeffrey A. Brown, D.O., Cleveland, Ohio;Randall M. Clark, M.D., Denver, Colorado; Richard T. Connis, Ph.D., Woodinville,Washington; Robert Herfkens, M.D., Stanford, California; Lawrence Litt, M.D., Ph.D.,San Francisco, California; Keira P. Mason, M.D., Wellesley Hills, Massachusetts; CraigD. McClain, M.D., Brookline, Massachusetts; David G. Nickinovich, Ph.D., Bellevue,Washington; Susan M. Ryan, M.D., Ph.D., San Francisco, California; and Warren S.Sandberg, M.D., Ph.D., Boston, Massachusetts.
Submitted for publication October 24, 2008. Accepted for publication Octo-ber 24, 2008. Supported by the American Society of Anesthesiologists under thedirection of James F. Arens, M.D., Chair, Committee on Standards and PracticeParameters. Approved by the House of Delegates on October 22, 2008. Acomplete list of references used to develop this Advisory is available by writingto the American Society of Anesthesiologists.
Address reprint requests to the American Society of Anesthesiologists: 520North Northwest Highway, Park Ridge, Illinois 60068-2573. This Practice Advi-sory, as well as all published ASA Practice Parameters, may be obtained at no costthrough the Journal Web site, www.anesthesiology.org.
Anesthesiology, V 110, No 3, Mar 2009 459
does not apply to level I facilities, where no anestheticcare is provided.
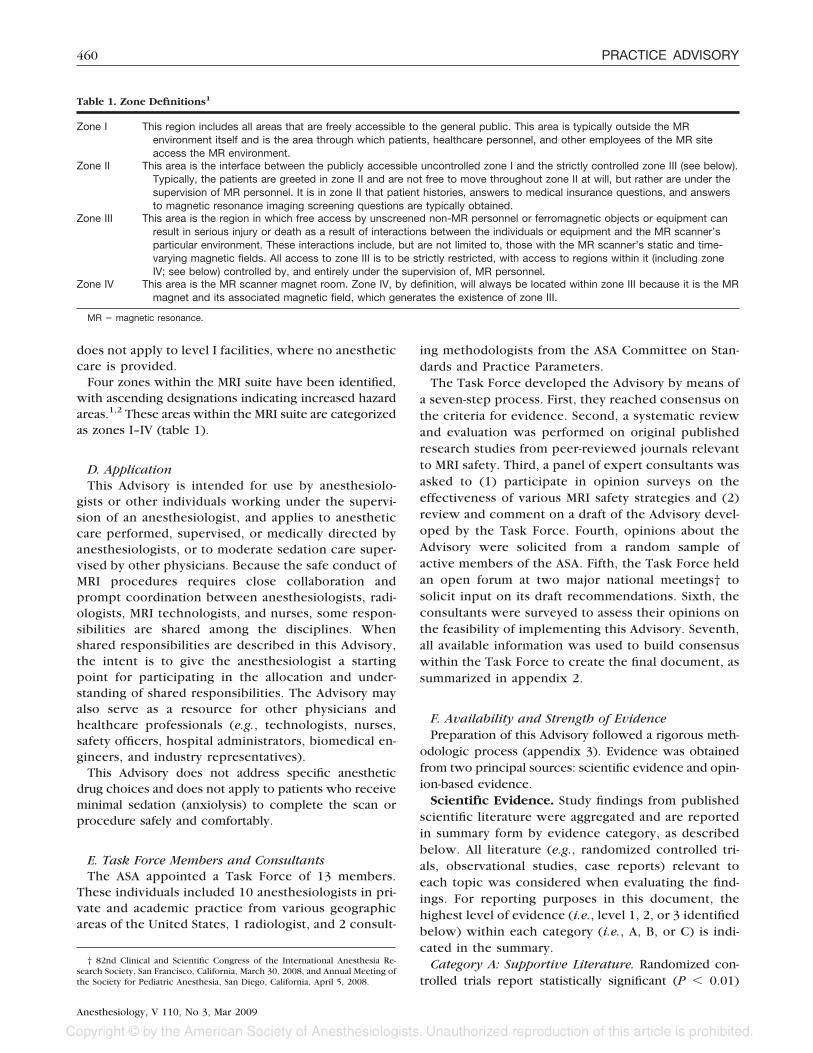
Four zones within the MRI suite have been identified,with ascending designations indicating increased hazardareas.1,2 These areas within the MRI suite are categorizedas zones I–IV (table 1).
D. ApplicationThis Advisory is intended for use by anesthesiolo-
gists or other individuals working under the supervi-sion of an anesthesiologist, and applies to anestheticcare performed, supervised, or medically directed byanesthesiologists, or to moderate sedation care super-vised by other physicians. Because the safe conduct ofMRI procedures requires close collaboration andprompt coordination between anesthesiologists, radi-ologists, MRI technologists, and nurses, some respon-sibilities are shared among the disciplines. Whenshared responsibilities are described in this Advisory,the intent is to give the anesthesiologist a startingpoint for participating in the allocation and under-standing of shared responsibilities. The Advisory mayalso serve as a resource for other physicians andhealthcare professionals (e.g., technologists, nurses,safety officers, hospital administrators, biomedical en-gineers, and industry representatives).
This Advisory does not address specific anestheticdrug choices and does not apply to patients who receiveminimal sedation (anxiolysis) to complete the scan orprocedure safely and comfortably.
E. Task Force Members and ConsultantsThe ASA appointed a Task Force of 13 members.
These individuals included 10 anesthesiologists in pri-vate and academic practice from various geographicareas of the United States, 1 radiologist, and 2 consult-
ing methodologists from the ASA Committee on Stan-dards and Practice Parameters.
The Task Force developed the Advisory by means ofa seven-step process. First, they reached consensus onthe criteria for evidence. Second, a systematic reviewand evaluation was performed on original publishedresearch studies from peer-reviewed journals relevantto MRI safety. Third, a panel of expert consultants wasasked to (1) participate in opinion surveys on theeffectiveness of various MRI safety strategies and (2)review and comment on a draft of the Advisory devel-oped by the Task Force. Fourth, opinions about theAdvisory were solicited from a random sample ofactive members of the ASA. Fifth, the Task Force heldan open forum at two major national meetings† tosolicit input on its draft recommendations. Sixth, theconsultants were surveyed to assess their opinions onthe feasibility of implementing this Advisory. Seventh,all available information was used to build consensuswithin the Task Force to create the final document, assummarized in appendix 2.
F. Availability and Strength of EvidencePreparation of this Advisory followed a rigorous meth-
odologic process (appendix 3). Evidence was obtainedfrom two principal sources: scientific evidence and opin-ion-based evidence.
Scientific Evidence. Study findings from publishedscientific literature were aggregated and are reportedin summary form by evidence category, as describedbelow. All literature (e.g., randomized controlled tri-als, observational studies, case reports) relevant toeach topic was considered when evaluating the find-ings. For reporting purposes in this document, thehighest level of evidence (i.e., level 1, 2, or 3 identifiedbelow) within each category (i.e., A, B, or C) is indi-cated in the summary.
Category A: Supportive Literature. Randomized con-trolled trials report statistically significant (P � 0.01)
† 82nd Clinical and Scientific Congress of the International Anesthesia Re-search Society, San Francisco, California, March 30, 2008, and Annual Meeting ofthe Society for Pediatric Anesthesia, San Diego, California, April 5, 2008.
Table 1. Zone Definitions1
Zone I This region includes all areas that are freely accessible to the general public. This area is typically outside the MRenvironment itself and is the area through which patients, healthcare personnel, and other employees of the MR siteaccess the MR environment.
Zone II This area is the interface between the publicly accessible uncontrolled zone I and the strictly controlled zone III (see below).Typically, the patients are greeted in zone II and are not free to move throughout zone II at will, but rather are under thesupervision of MR personnel. It is in zone II that patient histories, answers to medical insurance questions, and answersto magnetic resonance imaging screening questions are typically obtained.
Zone III This area is the region in which free access by unscreened non-MR personnel or ferromagnetic objects or equipment canresult in serious injury or death as a result of interactions between the individuals or equipment and the MR scanner’sparticular environment. These interactions include, but are not limited to, those with the MR scanner’s static and time-varying magnetic fields. All access to zone III is to be strictly restricted, with access to regions within it (including zoneIV; see below) controlled by, and entirely under the supervision of, MR personnel.
Zone IV This area is the MR scanner magnet room. Zone IV, by definition, will always be located within zone III because it is the MRmagnet and its associated magnetic field, which generates the existence of zone III.
MR � magnetic resonance.
460 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

differences among clinical interventions for a specifiedclinical outcome.
Level 1: The literature contains multiple randomizedcontrolled trials, and the aggregated findings are sup-ported by meta-analysis.‡
Level 2: The literature contains multiple randomizedcontrolled trials, but there is an insufficient number ofstudies to conduct a viable meta-analysis for the purposeof this Advisory.
Level 3: The literature contains a single randomizedcontrolled trial.
Category B: Suggestive Literature. Information fromobservational studies permits inference of beneficial orharmful relations among clinical interventions and clini-cal outcomes.
Level 1: The literature contains observational compar-isons (e.g., cohort, case–control research designs) of twoor more clinical interventions or conditions and indi-cates statistically significant differences between clinicalinterventions for a specified clinical outcome.
Level 2: The literature contains noncomparative obser-vational studies with associative (e.g., relative risk, cor-relation) or descriptive statistics.
Level 3: The literature contains case reports.Category C: Equivocal Literature. The literature can-
not determine whether there are beneficial or harmfulrelations among clinical interventions and clinical out-comes.
Level 1: Meta-analysis did not find significant differ-ences among groups or conditions.
Level 2: There is an insufficient number of studies toconduct meta-analysis and (1) randomized controlledtrials have not found significant differences amonggroups or conditions or (2) randomized controlled trialsreport inconsistent findings.
Level 3: Observational studies report inconsistent find-ings or do not permit inference of beneficial or harmfulrelations.
Category D: Insufficient Evidence from Literature.The lack of scientific evidence in the literature is de-scribed by the following terms.
Silent: No identified studies address the specified rela-tions among interventions and outcomes.
Inadequate: The available literature cannot be used toassess relations among clinical interventions and clinicaloutcomes. The literature either does not meet the crite-ria for content as defined in the “Focus” of the Advisoryor does not permit a clear interpretation of findingsbecause of methodologic concerns (e.g., confounding instudy design or implementation).
Opinion-based Evidence. All opinion-based evi-dence relevant to each topic (e.g., survey data, open-forum testimony, Internet-based comments, letters, edi-torials) is considered in the development of thisAdvisory. However, only the findings obtained from for-mal surveys are reported.
Opinion surveys were developed by the Task Force toaddress each clinical intervention identified in the doc-ument. Identical surveys were distributed to two groupsof respondents: expert consultants and ASA members.
Category A: Expert Opinion. Survey responses fromTask Force–appointed expert consultants are reportedin summary form in the text. A complete listing ofconsultant survey responses is reported in table 2 inappendix 3.
Category B: Membership Opinion. Survey responsesfrom a random sample of members of the ASA are re-ported in summary form in the text. A complete listing ofASA member survey responses is reported in table 3 inappendix 3.
Survey responses are recorded using a 5-point scaleand summarized based on median values.§
Strongly agree: median score of 5 (at least 50% of theresponses are 5)
Agree: median score of 4 (at least 50% of the responses are4 or 4 and 5)
Equivocal: median score of 3 (at least 50% of the responsesare 3, or no other response category or combination ofsimilar categories contain at least 50% of the responses)
Disagree: median score of 2 (at least 50% of the responsesare 2 or 1 and 2)
Strongly disagree: median score of 1 (at least 50% ofthe responses are 1)
Category C: Informal Opinion. Open-forum testi-mony, Internet-based comments, letters, and editorialsare all informally evaluated and discussed during thedevelopment of the Advisory. When warranted, the TaskForce may add educational information or cautionarynotes based on this information.
Advisories
I. EducationMRI safety education includes, but is not limited to,
topics addressing: (1) MRI magnet hazards in zones III andIV, (2) challenges and limitations of monitoring, and (3) long-term health hazards.
There is insufficient published evidence to evaluatethe effect of education regarding magnet hazards, mon-itoring limitations, or long-term health hazards associ-ated with MRI. [Category D evidence] One observationalstudy examined the potential long-term health hazards ofpregnant MRI workers and pregnant non-MRI workers,and found no significant difference in the relative risk of
‡ All meta-analyses are conducted by the ASA methodology group. Meta-analyses from other sources are reviewed but not included as evidence in thisdocument.
§ When an equal number of categorically distinct responses is obtained, themedian value is determined by calculating the arithmetic mean of the two middlevalues. Ties are calculated by a predetermined formula.
461PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

early delivery, low birth weight, or spontaneous abor-tions.3 [Category C evidence]
The consultants and ASA members strongly agree thatall anesthesiologists should have general safety educa-tion on the unique physical environment of the MRIscanner. The ASA members agree and the consultantsstrongly agree that all anesthesiologists should have spe-cific education regarding the features of individual scan-ners within their institution. The ASA members agreeand the consultants strongly agree that anesthesiologistsshould work in collaboration with radiologists, technol-ogists, and physicists within their institutions to developsafety training programs.
Advisory Statements. All anesthesiologists shouldhave general safety education on the unique physicalenvironment of the MRI scanner and specific educationregarding the specific features of individual scannerswithin their institution. Education should emphasizesafety for entering zones III and IV, with special empha-sis on hazards in this environment and effects on moni-toring capabilities. Education should address potentialhealth hazards (e.g., high decibel levels and high-inten-sity magnetic fields) and necessary precautions to dealwith the specific field strength and the safety of the MRIscanners within their institutions. Education should in-clude information regarding ferromagnetic items (e.g.,stethoscopes, pens, wallets, watches, hair clips, nametags, pagers, cell phones, credit cards, batteries) andimplantable devices (e.g., spinal cord stimulators, im-planted objects) that should not be brought into zoneIII or IV of the MRI suite or should be brought in withcaution. Anesthesiologists should work in collabora-tion with radiologists, technologists, and physicistswithin their institutions to ensure that the above top-ics are included in their safety training programs.Finally, education should include how to safely re-spond to code blue situations in zones III and IV, andthis information should be integrated into protocolsfor the designated code blue team.
II. Screening of Anesthetic Care Providers andAncillary Support PersonnelThe MRI medical director or designated technologist is
responsible for access to zones III and IV. Screening ofall individuals entering zone III is necessary to preventaccidental incursions of ferromagnetic materials or inad-vertent exposure of personnel with foreign bodies orimplanted ferromagnetic items.
The literature is silent regarding whether the screeningof anesthesia care providers and ancillary support per-sonnel improves safety in the MRI suite. [Category Devidence] The ASA members agree and the consultantsstrongly agree that the anesthesiologist should work incollaboration with the MRI medical director or designeeto ensure that all anesthesia team personnel enteringzone III or IV have been properly screened.
Advisory Statements. The anesthesiologist shouldwork in collaboration with the MRI medical director ordesignee (e.g., safety officer) to ensure that all anesthesiateam personnel entering zone III or IV have beenscreened for the presence of ferromagnetic materials,foreign bodies, or implanted devices.
III. Patient ScreeningPatient screening consists of determining patient and
equipment-related risks for adverse outcomes associatedwith MRI procedures.
Patient-related Risks: Risks related to the patient mayinclude age-related risks, health-related risks, and risksfrom foreign bodies located in or on the patient orimplanted ferromagnetic items. Age-related risks applyto neonates or premature infants, and elderly patients.Health-related risks include, but are not limited to, (1)the need for intensive or critical care; (2) impaired re-spiratory function (e.g., tonsillar hypertrophy, sleep ap-nea); (3) changes in level of sedation, muscle relaxation,or ventilation; (4) hemodynamic instability and vasoac-tive infusion requirements; and (5) comorbidities thatmay contribute to adverse MRI effects (e.g., burns ortemperature increases in patients with obesity or periph-eral vascular disease). Risks from foreign bodies includenonmedical ferromagnetic items imbedded in the pa-tient (e.g., eyeliner tattoos, metallic intraocular frag-ments) or attached to the patient (e.g., pierced jewelry,magnetic dental keepers). Risk from implanted ferro-magnetic items may include such items as aneurysmclips, prosthetic heart valves, or coronary arterial stents.
One comparative study reports that neonates undergoingMRI demonstrate increased fluctuations in heart rate, bloodpressure, and oxygen saturation levels compared with ne-onates not undergoing MRI.4 [Category B1 evidence] Twoobservational studies report that premature neonates canexperience heart rate fluctuations, decreases in oxygensaturation, and increases in temperature during MRI.5,6
[Category B2 evidence] One case report indicates that achild with a history of previous cardiac arrest experienceda cardiac arrest during MRI.7 [Category B3 evidence] Fourobservational studies8–11 and two case reports12,13 indicatethat patients with impaired renal function are at risk ofnephrogenic systemic fibrosis after gadolinium adminis-tered for MRI. [Category B2 evidence]
Case reports indicate that exposure of iron filings to themagnetic field may result in hemorrhage,7,14 and exposureof eyeliner tattoos may result in image artifacts, burns,swelling, or puffiness.7,15–17 [Category B3 evidence] Nu-merous observational studies and case reports indicate in-teractions with the magnetic field (e.g., movements, dis-placements, image artifacts) and increases in temperatureduring MRI for ferromagnetic items such as aneurysm clips,surgical clips, prosthetic heart valves, intravenous infusionpumps, coronary arterial stents, and implanted dental mag-net keepers.18–43 [Category B2 evidence]
462 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Both the consultants and the ASA members stronglyagree that, for every case, the anesthesiologist shouldcommunicate with the patient and radiologist or refer-ring physician to determine whether the patient has ahigh-risk medical condition. In addition, they bothstrongly agree that if the patient presents with a high-riskmedical condition, the anesthesiologist should collabo-rate with all participants, including the referring physi-cian, radiologist, and technologist, to determine how thepatient will be managed during the MRI procedure. Boththe consultants and the ASA members agree that, forpatients with acute or severe renal insufficiency, theanesthesiologist should not administer gadolinium be-cause of the increased risk of nephrogenic systemicfibrosis.
Equipment-related Risks: Patient equipment-relatedrisks include, but are not limited to, (1) physiologicmonitors; (2) invasive monitors (e.g., intravascular cath-eters); (3) intubation equipment; (4) oxygenation andventilation equipment; and (5) pacemakers, implantedcardiodefibrillators, and other implanted devices (e.g.,deep brain stimulators, vagal or phrenic nerve stimula-tors, middle-ear or cochlear implants).
One case report notes that cardiac monitor leads inter-fered with an MRI scan.7 [Category B3 evidence] Oneobservational study and one case report indicate that fireor burns occurred beneath or near cardiac monitor elec-trodes.44,45 [Category B2 evidence] Five case reportsnote that burns occurred from the looping of a temper-ature probe or pulse oximetry cables.46–50 [Category B3evidence] One observational study reports ferromag-netic components in ventilators51 [category B2 evi-dence], and three case reports describe projectile ni-trous oxide or oxygen tanks52–54 [category B3 evidence].Additional observational studies and case reports indi-cate interactions of pacemakers or implanted cardio-verter–defibrillators with MRI scanning, including, butnot limited to, pacing artifacts, reed switch closure,generator movement or displacement, alterations of pac-ing rate, and temperature increases.7,55–84 [Category B2evidence] Two observational studies report palpitations,rapid heart rate, and discomfort at the pacemaker pocketafter MRI.75,85 [Category B2 evidence] Finally, two casesof cardiac arrest are reported in patients with pacemak-ers during or after an MRI scan; in one case, the patientdied.7,57 [Category B3 evidence]
Two observational studies report image artifacts whenMRI is performed in patients with neurostimulators, infu-sion pumps, or implantable spinal fusion stimulators.86,87
Six observational studies report increased temperatures inpatients with deep brain stimulators, neurostimulators, orspinal cord stimulators,88–93 and three report displacementof leads, pulse generators, or other components of deepbrain stimulators or middle ear prostheses during MRIscans.94–96 [Category B2 evidence]
Both the consultants and the ASA members agree that,for every case, the anesthesiologist should communicatewith the radiologist or referring physician to determinewhether the patient requires equipment that may pose arisk during the scan. In addition, they agree that anes-thesiologists should determine the safety and effective-ness of the equipment needed by the patient during theprocedure for each MRI location. Further, the consult-ants and ASA members strongly agree that anesthesiolo-gists should work with their institutions to properlyidentify and label anesthesia-related equipment accord-ing to convention for each MRI scanner. The ASA mem-bers agree and the consultants strongly agree that careshould be taken to ensure that anesthesia equipmentdoes not interfere with image acquisition or quality.Both the consultants and the ASA members agree that, ingeneral, MRI should not be performed on patients withimplanted electronic devices. Finally, both the consult-ants and the ASA members strongly agree that, whenMRI is considered essential by the referring physicianand consulting radiologist, a plan for managing patientswith implanted electronic devices during the scanshould be developed in collaboration with the referringphysician, medical director or on-site radiologist, andother appropriate consultants.
Advisory Statements for Patient and Equipment-related Risks. For every case, the anesthesiologistshould communicate with the patient, referring physi-cian, and radiologist to determine whether the patient(1) presents with a high-risk medical condition (e.g.,neonatal status or prematurity, intensive or critical carestatus, impaired respiratory function, hemodynamic in-stability and vasoactive infusion requirements, comor-bidities such as obesity and peripheral vascular disease);(2) requires equipment (e.g., physiologic or invasivemonitors; intubation, oxygenation, or ventilation equip-ment); (3) has implanted devices (e.g., pacemakers, car-dioverter–defibrillators, nerve stimulators); (4) has beenscreened for the presence of implanted ferromagneticitems (e.g., surgical clips, prosthetic heart valves); and (5)has been screened for the presence of imbedded foreignbodies (e.g., orbital iron filings, eyeliner tattoos). Finally, theanesthesiologist should communicate with the technolo-gist to ensure that the patient has been screened for thepresence of foreign bodies on the patient (e.g., piercedjewelry, rings) before entering zone III.
If a patient presents with a high-risk medical condition,the anesthesiologist should collaborate with all partici-pants, including the referring physician, radiologist, andtechnologist, to determine how the patient will be man-aged during the MRI procedure. Anticipated changes inlevel of sedation, muscle relaxation, or ventilation mayalso place a patient in a high-risk situation.
For patients with acute or severe renal insufficiency,the anesthesiologist should not administer gadolinium
463PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

because of the increased risk of nephrogenic systemicfibrosis.�
Anesthesiologists should work with their institutions toproperly identify and label anesthesia-related equipmentaccording to convention (safe, unsafe, or conditional) foreach MRI scanner.# For each MRI location, anesthesiolo-gists should determine the safety and effectiveness of theequipment needed by the patient during the procedure. Inaddition, care should be taken to ensure that equipmentdoes not interfere with image acquisition or quality.
The Task Force believes that cardiac pacemakersand implantable cardioverter–defibrillators are generallycontraindicated for MRI. These devices pose an extremehazard in this environment and may be life-threateningwithin the 5 gauss line. When MRI is considered essen-tial by the referring physician and consulting radiologist,a plan for managing these patients during the scanshould be developed in collaboration with the orderingphysician, medical director or on-site radiologist, andother appropriate consultants (e.g., the patient’s pace-maker specialist or cardiologist, the diagnostic radiolo-gist, the device manufacturer).**
Other implanted electronic devices also pose a hazardin the MRI environment. These devices and associatedwiring may transfer energy during the MRI scan, causingtissue damage, malfunction of the device, image arti-facts, and device displacement. MRI may be performedon a limited basis for patients with certain implantedelectronic devices (e.g., deep brain stimulators, vagalnerve stimulators, phrenic nerve stimulators, wire-con-taining thermodilution catheters, cochlear implants). Inconsultation with the referring physician, the radiologistresponsible for the procedure, and the neurosurgeon,the anesthesiologist should ensure that the presence ofthe device has been noted and determined to be MRIsafe/conditional before imaging of these patients.
IV. PreparationPreparation consists of determining and implement-
ing an individualized anesthetic plan before the MRIprocedure begins. In addition to the anesthetic plan,preparation includes a plan for optimal positioning of
equipment and personnel in the MRI suite during theprocedure.
The literature is insufficient to determine whether ac-tive preparation or pre-MRI planning reduces the fre-quency of adverse events. [Category D evidence] Onecase report indicates that misinformation about the typeof aneurysm clip resulted in intracerebral hemorrhageand death,31 and a second case report indicates that alack of communication among physicians caring for apacemaker patient resulted in the death of the patient.97
[Category B3 evidence]Both the consultants and the ASA members strongly
agree that, for every case, the anesthesiologist shouldprepare, with support personnel, a plan for providingoptimal anesthetic care within the special environmentof the MRI suite. They both strongly agree that theanesthesiologist should communicate with the radiologypersonnel to determine the requirements of the scan. TheASA members agree and the consultants strongly agree thatthe anesthesiologist should collaborate with the magneticresonance (MR) technologist and/or facility biomedical en-gineer to determine and demarcate the optimal and safelocation of movable equipment in relation to the gauss lineswithin the MRI suite. They both strongly agree that, be-cause line of sight within the bore will vary depending onthe facility, the anesthesiologist should choose a location orposition for optimal patient observation and vigilance dur-ing delivery of care, whether in zone III or IV. Finally, theyboth strongly agree that the anesthesiologist should pre-pare a plan for rapidly summoning additional personnel inthe event of an emergency.
Advisory Statements. For every case, the anesthesiol-ogist should prepare, with support personnel, a plan forproviding optimal anesthetic care within the special envi-ronment of the MRI suite. In addition to addressing themedical needs of the patient, features of the plan shouldinclude (1) requirements of the scan and personnel needs, (2)positioning of equipment, (3) special requirements or uniqueissues of patient or imaging study, (4) positioning of the anes-thesiologist and the patient, and (5) planning for emergencies.
1. The anesthesiologist should communicate with theradiology personnel to determine the requirementsfor the scan (e.g., duration of the scan, position of thepatient or area of the body in the scanner, positioningof receiver coils, need for periods of paused respira-tion). The anesthesiologist should communicate withother anesthesia team members regarding individualroles for anesthetic care.
2. The anesthesiologist should collaborate with the MRtechnologist and/or facility biomedical engineer todetermine and demarcate the optimal and safe loca-tion of movable equipment in relation to the gausslines within the MRI suite.
3. Because line of sight within the bore will vary de-pending on the facility, the anesthesiologist should
� See US Food and Drug Administration alert. Available at: http://www.fda.gov/CDER/Drug/InfoSheets/HCP/gcca_200705.htm. Accessed October 17, 2008.
# Equipment is categorized as safe, unsafe, or conditional for use in the MRIenvironment. MRI safe equipment is identified by the American Society forTesting and Materials as having no ferromagnetic parts or radiofrequency inter-ference. MRI unsafe equipment is identified as having ferromagnetic parts or beingaffected by radiofrequency interference. MRI conditional equipment may be safe incertain locations of the suite depending on gauss line locations, but cannot beidentified as having no ferromagnetic parts (see American Society for Testing andMaterials Practice Standards F2503, F2119, and F2052, www.astm.org). In the past,equipment was described as MRI compatible, but because the safety of this equip-ment depended on the particular MRI environment, the word conditional nowapplies.
** American Society of Anesthesiologists: Practice advisory for the periopera-tive management of patients with cardiac rhythm management devices: Pace-makers and implantable cardioverter–defibrillators. ANESTHESIOLOGY 2005; 103:186–98.
464 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

choose a location or position for optimal patientobservation and vigilance during delivery of care,whether in zone III or IV. In particular, anesthesiolo-gists should have (1) a clear line of sight of the patientand physiologic monitors, whether by direct observa-tion or by video camera; (2) anesthetic delivery equip-ment located for optimal control of anesthetic depthand rapid intervention; and (3) access to hospitalinformation systems integral to patient care. In pre-paring for positioning, the anesthesiologist shouldtake into account potential electromagnetic and au-ditory hazards.
4. Anesthesiologists should prepare a plan for rapidlysummoning additional personnel in the event of anemergency. Because the MRI suite is frequently lo-cated in an isolated area of the facility, the anesthesi-ologist should ensure that (1) emergency equipmentand drugs are immediately accessible; (2) emergencycommunication (e.g., phone or code button) is imme-diately available; and (3) an evacuation plan is inplace, including an appropriate location outside thescan room (zone IV) for resuscitation. This locationshould be complete with physiologic monitors, oxy-gen, suction, and other appropriate resuscitationequipment. Monitoring requirements, airway man-agement, and emergency preparedness are additionalfeatures that should be included in the preparationand planning for an MRI scan, and are addressed insection V below.
V. Patient Management during MRIFeatures of safe patient management during MRI proce-
dures include (1) monitoring, (2) anesthetic care, (3) air-way management, and (4) management of emergencies.
Monitoring. Safe monitoring conditions include (1)the use of MRI-safe/conditional monitors, (2) remotemonitoring, and (3) compliance with ASA standards.98
Three observational studies indicate that the use ofMRI-compatible monitoring equipment resulted in noradiofrequency interference, interruptions in scanning,or artifacts.99–101 [Category B2 evidence] Five observa-tional studies demonstrate that remote monitoring forheart rate, blood pressure, auscultation, respiration, andchest wall movement can be performed safely and effec-tively.100,102–105 [Category B2 evidence] One observa-tional study reported that compliance with the ASA Stan-dards for Basic Anesthetic Monitoring can be obtained,provided that the monitoring equipment is properlytested before MRI.106 [Category B2 evidence]
The consultants and ASA members both strongly agreethat MRI patients should be monitored in a mannerconsistent with the ASA Standards for Basic AnestheticMonitoring. In addition, they both strongly agree that (1)anesthesiologists should be familiar with the expectedlimitations of available monitoring equipment, (2) theanesthesiologist should make sure that all monitors used
in zone IV are safe/conditional for the scan, and (3) amonitor should be available to view vital signs from zoneIII when the anesthesia care provider is not in zone IV.
Advisory Statements. MRI patients should be moni-tored in a manner consistent with the ASA Standards forBasic Anesthetic Monitoring. Anesthesiologists shouldbe familiar with the expected limitations of availablemonitoring equipment. The Task Force notes that infor-mation from electrocardiograms may be limited becauseof superimposed voltages from blood flow in the highmagnetic field (e.g., ST-segment interpretation may beunreliable, even with highly filtered monitors). The an-esthesiologist should make sure that all monitors used inzone IV are safe/conditional for the scan. A monitorshould be available to view vital signs from zone IIIwhen the anesthesia care provider is not in zone IV.Additional care should be taken in positioning electro-cardiographic and other monitor leads to eliminateburns, even with nonferromagnetic leads.
Anesthetic Care. Observational studies report a highrate of success in imaging of sedated patients or patients towhom light anesthesia is administered.107–112 However,motion artifacts may still occur.113–115 [Category B2 evi-dence] Observational studies and case reports also indicatethat sedation or light anesthesia may be associated withrespiratory depression, oxygen desaturation, bronchos-pasm, drowsiness, agitation, and vomiting.99,108–113,116–128
[Category B2 evidence] The Task Force believes that auto-mated apnea monitoring (by detection of exhaled carbondioxide or other means) may decrease risks during bothmoderate and deep sedation.
Both the consultants and the ASA members stronglyagree that, in general, because MRI is a nonpainful pro-cedure, lighter levels of anesthesia may be appropriate,recognizing that institutional circumstances, patientcharacteristics, and anesthesiologist preference maywarrant more aggressive airway management and deeperanesthetic levels. They both strongly agree that anesthe-siologists should ensure that patients who receive mod-erate or deep sedation are monitored in a manner con-sistent with their institution’s protocol for monitoringsimilarly sedated patients elsewhere in the facility. Inaddition, they both strongly agree that equipment anddrugs for anesthetic care in the MRI suite should mirrorwhat is available in the operating room. Both the con-sultants and the ASA members are equivocal that, whenan MRI-safe/conditional anesthesia machine is not avail-able, inhalation anesthetics may be administered from ananesthesia machine inside zone III via an elongatedcircuit through a wave guide. Finally, both the consult-ants and the ASA members agree that, if total intravenousanesthesia is used, it should be administered by using (1)MRI-safe/conditional pumps in zone IV, (2) traditional(i.e., MRI-unsafe) pumps in zone III with intravenoustubing passed through a wave guide, or (3) periodicbolus injections in zone III or IV.
465PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Advisory Statements. Although lighter levels of an-esthesia may be appropriate during an MRI scan, theanesthesiologist should be aware that these lighter levelsmay result in airway complications (e.g., laryngospasm,coughing, other airway compromise) that may necessi-tate interruption of the scan for urgent treatment and alter-ation of anesthetic depth. Institutional circumstances, pa-tient characteristics, and anesthesiologist preference maywarrant more aggressive airway management and deeperanesthetic levels.
Anesthesiologists should ensure that patients who re-ceive moderate or deep sedation are monitored in amanner consistent with their institution’s protocol formonitoring similarly sedated patients elsewhere in thefacility. Monitoring of exhaled carbon dioxide should beconsidered for all patients receiving deep sedation andfor patients whose ventilation cannot be directly ob-served during moderate sedation.†† The Task Force cau-tions that, because ventilation and oxygenation are sep-arate though related physiologic processes, monitoringoxygenation by pulse oximetry is not a substitute formonitoring ventilatory function.
Equipment and drugs for anesthetic care in the MRIsuite should mirror what is available in other anesthetiz-ing locations, including (1) an integrated anesthesia ma-chine, medical gases, and waste anesthesia gas disposalor gas scavenging, when inhalational anesthesia is ad-ministered; (2) suction; (3) adequate electrical outletsand lighting; and (4) storage areas for equipment anddrugs. The Task Force recognizes that physical plantvariability exists among institutions.‡‡ Equipment usedin the MRI suite should be appropriate for the age andsize of the patient.
Magnetic resonance imaging–safe/conditional anesthe-sia machines are always preferred for use in an MRIfacility.§§ However, when an MRI-safe/conditional anes-thesia machine is not available, inhalational anestheticscan be administered from an anesthesia machine insidezone III via an elongated circuit through a wave guide.��Although this method of anesthetic delivery was com-monplace before the commercial manufacture of MRI-safe/conditional anesthesia machines, this practice is in-herently cumbersome and may be prone to morepossibilities for mishaps than the use of an anesthesiamachine specifically designed for the MRI environment.
Alternatively, if total intravenous anesthesia is used, itshould be administered by using (1) MRI-safe/conditionalpumps in zone IV, (2) traditional (i.e., MRI unsafe) pumpsin zone III with intravenous tubing passed through a waveguide, or (3) periodic bolus injections in zone III or IV.Although an anesthesia machine may not be required forthe administration of total intravenous anesthesia, theremust be equipment immediately available for the adminis-tration of positive-pressure ventilation with oxygen.
Airway Management. Unique features of airway man-agement during an MRI scan include (1) the limitedaccessibility of the patient’s airway and (2) the difficultyof conducting visual and auditory assessments of thepatient. The literature is silent regarding the managementof airway problems (e.g., obstruction, secretions, laryngo-spasm, apnea and hypoventilation) during an MR scan.[Category D evidence] In addition, the literature is silentregarding whether the use of an endotracheal tube orlaryngeal mask airway improves outcomes for patients atrisk of airway compromise during MRI. [Category D evi-dence]
Both the consultants and the ASA members stronglyagree that the anesthesiologist should have an advanceplan in place to deal with instrumentation of the airwayand common airway problems when patients are in anMRI environment. Both the consultants and the ASAmembers strongly agree that, if the patient is at risk forairway compromise, more aggressive airway manage-ment should be instituted because the patient’s airwaymay be less accessible when the patient is in the scan-ner. Both the consultants and the ASA members stronglyagree that (1) complex airway management (e.g., fiber-optic intubation) should be performed in a controlledenvironment outside of zone IV, (2) alternative airwaydevices should be immediately available in the MRI suite,and (3) suction equipment should be immediately acces-sible to the patient’s airway at all times.
Advisory Statements. The anesthesiologist shouldhave an advance plan in place to deal with instrumenta-tion of the airway and common airway problems (e.g.,obstruction, secretions, laryngospasm, apnea and hy-poventilation) when patients are in an MRI environment.If the patient is at risk for airway compromise, moreaggressive airway management (e.g., use of a endotra-cheal tube or laryngeal mask airway) should be institutedbecause the patient’s airway may be less accessiblewhen the patient is in the scanner. Complex airwaymanagement (e.g., fiberoptic intubation) should be per-formed in a controlled environment outside of zone IV.
Alternative MRI-safe/conditional airway devices shouldbe immediately available in the MRI suite. Suction equip-ment should be immediately accessible to the patient’sairway at all times.
Management of Emergencies. Emergencies in theMR suite include (1) medical emergencies (e.g., cardio-pulmonary arrest) and (2) environmental emergencies (e.g.,
†† American Society of Anesthesiologists: Practice guidelines for sedation andanalgesia by non-anesthesiologists: An updated report. ANESTHESIOLOGY 2002; 96:1004–17.
‡‡ When remodeling or building a new facility, input from the anesthesiologistis critical.
§§ An MRI facility that is newly built or that undergoes a major renovationshould have an MRI-safe/conditional anesthesia machine.
�� A wave guide is a copper-lined conduit with a specific length and diameterthat maintains radiofrequency isolation of the magnet room installed duringconstruction of the MRI suite. Wires or conducting material act as an antenna andshould not be passed through a wave guide.
466 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

quench, fire, projectiles). The remote location of the scan-ner within the facility may delay response of support per-sonnel or availability of equipment during an emergency.
The literature is insufficient regarding the manage-ment of medical emergencies (e.g., cardiopulmonaryarrest) or quench in the MR suite. [Category D evi-dence] One case report indicates that a fire occurringon the patient was managed by extinguishing theflames, discontinuing the scan, and immediately re-moving the patient from the bore.45 Two case reportsof projectile nitrous oxide or oxygen tanks indicatethat the emergency was managed by removing pa-tients from zone IV and instituting a controlledquench.53,54 [Category B3 evidence]
Both the consultants and the ASA members stronglyagree that when a patient has a medical emergency inthe MRI scanner, the following should occur: (1) initiatecardiopulmonary resuscitation, when needed, while im-mediately removing the patient from zone IV; (2) call forhelp; and (3) transport the patient to a previously des-ignated safe location in proximity to the MRI suite. Inaddition, they both strongly agree that the designatedsafe location should contain the following resuscitationequipment: (1) a defibrillator; (2) vital signs monitors;and (3) a code cart that includes resuscitation drugs,airway equipment, oxygen, and suction. The consultantsand ASA members both strongly agree that when a fireoccurs in the MRI suite, team members should performtheir preassigned fire management tasks as quickly aspossible, in accordance with the ASA Practice Advisoryfor the Prevention and Management of Operating RoomFires.129 The ASA members agree and the consultantsstrongly agree that, when a quench occurs, team mem-bers should perform their institution’s protocol in reac-tion to this occurrence. In addition, the ASA membersagree and the consultants strongly agree that, when aquench occurs, if possible, (1) the patient should beremoved from zone IV immediately and (2) oxygenshould be administered to the patient immediately. Fi-nally, both the consultants and the ASA members agreethat, because powerful static magnetic fields may persistafter a quench or fire, emergency response personnelshould be restricted from entering zone IV.
Advisory Statements. Medical emergencies may bedifficult to manage while the patient is in the MRI scanner.When a patient has a medical emergency (e.g., cardiopul-monary arrest) in the MRI scanner, the following shouldoccur: (1) immediately remove the patient from zone IVwhile initiating cardiopulmonary resuscitation, if indicated;(2) call for help; and (3) transport the patient to a previ-ously designated safe area for resuscitation that is not inzone IV. This location should be as close to zone IV aspossible so as not to delay resuscitation efforts, and shouldcontain the following resuscitation equipment: a defibrilla-tor; vital signs monitors; and a code cart that includesresuscitation drugs, airway equipment, oxygen, and suction.
When a fire occurs in the MRI suite, team membersshould perform their preassigned fire management taskas quickly as possible, in accordance with the ASA Prac-tice Advisory for the Prevention and Management ofOperating Room Fires. If a team member cannot rapidlyperform his or her task in the predetermined order,other team members should perform their tasks withoutwaiting. When a team member has completed a preas-signed task, he or she should help other members per-form tasks that are not yet complete.
In the case of projectile emergencies, team membersshould perform their institution’s protocol in reactionto this occurrence. If possible, immediately remove thepatient from zone IV and discontinue the scan. If thepatient is injured, proceed with medical emergency man-agement as indicated above. A controlled quench may benecessary to remove the patient from the bore.
A quench occurs when a superconducting magnetturns resistive and catastrophically releases all of thestored energy as heat, boiling off the stored cryogens asgas. The most common cause of quench is an intentionalshutdown of the magnet for a life-threatening emergency.Quench may also be the consequence of an unintentionalshutdown. If not properly vented, a quench can result inthe complete dissipation of oxygen in zone IV, riskinghypoxia to the patient and MRI personnel. In addition,entrance to zone IV may not be possible because of highpressure caused by escaping gases, making it impossible toopen the door into zone IV. When a quench occurs, teammembers should perform their institution’s protocol inreaction to this occurrence. If possible, (1) immediatelyremove the patient from zone IV and (2) immediatelyadminister oxygen to the patient.
Powerful static magnetic fields may persist after aquench, and therefore the usual precautions apply whenentering zone IV. Emergency response personnel shouldbe restricted from entering zone IV during any environ-mental emergency because of the persistent magnetic field.
VI. Postprocedure CareThe literature is insufficient to determine whether
postprocedure care consistent with that provided forother areas of the institution reduces the frequency ofadverse events. [Category D evidence]
The ASA members agree and the consultants stronglyagree that the anesthesiologist should collaborate withthe radiologist and other staff in the postanesthetic careof the patient. Finally, both the consultants and the ASAmembers strongly agree that (1) patients receiving seda-tion or anesthesia within the MRI suite should haveaccess to postanesthetic care consistent with that pro-vided in other areas of the institution; (2) in all situations,intensive care and recovery areas should include accessto vital signs monitors, oxygen, suction, and trainedpersonnel; and (3) patients should be given written dis-charge instructions.
467PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Advisory Statements. The anesthesiologist should col-laborate with the radiologist and other staff in the postan-esthetic care of the patient. Patients receiving sedation oranesthesia within the MRI suite should have access topostanesthetic care consistent with that provided in otherareas of the institution,130 including transport to otherrecovery rooms, dedicated intensive care, or recovery areaswithin the MRI suite. In all situations, intensive care andrecovery areas should include access to vital sign monitors,oxygen, suction, resuscitation equipment, and trained per-sonnel.## Patients should be given oral and written dis-charge instructions.
References
1. Kanal E, Borgstede JP, Barkovich AJ, Bell C, Bradley WG, Felmlee JP,Froelich JW, Kaminski EM, Keeler EK, Lester JW, Scoumis EA, Zaremba LA,Zinninger MD: American College of Radiology white paper on MR safety. AJRAm J Roentgenol 2002; 178:1335–47
2. Kanal E, Barkovich AJ, Bell C, Bradler WG Jr, Froelich JW, Gilk T, Gimbel JR,Gosbee J, Kuhie-Kaminski E, Lester JW Jr, Nuenhuis J, Parag Y, Schaefer DJ,Sebek-Scoumis EA, Weinreb J, Zaremba LA, Wilcox P, Lucey L, Sass N, ACR BlueRibbon Panel on MR Safety: ACR guidance document for safe MR practices: 2007.AJR Am J Roentgenol 2007; 188:1447–74
3. Kanal E, Gillen J, Evans JA, Savitz DA, Shellock FG: Survey of reproductivehealth among female MR workers. Radiology 1993; 187:395–9
4. Philbin MK, Taber KH, Hayman LA: Preliminary report: Changes in vitalsigns of term newborns during MR. AJNR Am J Neuroradiol 1996; 17:1033–6
5. Battin M, Maalouf EF, Counsell S, Herligy A, Hall A, Azzopardi D, EdwardsAD: Physiologic stability of preterm infants during magnetic resonance imaging.Early Hum Dev 1998; 52:101–10
6. Taber KH, Hayman LA, Northrup SR, Maturi L: Vital sign changes duringinfant magnetic resonance examinations. J Magn Reson Imaging 1998; 8:1252–6
7. Gangarosa RE, Minnis JE, Nobbe J, Praschan D, Genberg RW: Operationalsafety issues in MRI. Magn Reson Imaging 1987; 5:287–92
8. Broome DR, Girguis MS, Baron PW, Cottrell AC, Kjellin I, Kirk GA: Gadodia-mide-associated nephrogenic systemic fibrosis: Why radiologists should be con-cerned. AJR Am J Roentgenol 2007; 188:586–92
9. Grobner T: Gadolinium: A specific trigger for the development of nephro-genic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol DialTransplant 2006; 21:1104–8
10. Khurana A, Runge VM, Narayanan M, Greene JF Jr, Nickel AE: Nephro-genic systemic fibrosis: A review of 6 cases temporally related to gadodiamideinjection. Invest Radiol 2007; 42:139–45
11. Marckmann P, Skov L, Rossen K, Dupont A, Damholt MB, Heaf JG,Thomsen HS: Nephrogenic systemic fibrosis: Suspected etiological role of ga-dodiomide used for contrast-enhanced magnetic resonance imaging. J Am SocNephrol 2006; 17:2359–62
12. Dharnidharka VR, Wesson SK, Fennel RS: Gadolinium and nephrogenicfibrosing dermopathy in pediatric patients. Pediatr Nephrol 2006; 22:1395
13. Thakral C, Alhariri J, Abraham JL: Long-term retention of gadolinium intissues from nephrogenic systemic fibrosis patient after multiple gadolinium-enhanced MRI scans: Case report and implications. Contrast Media Mol Imaging2007; 2:199–205
14. Kelly WM, Paglen PG, Pearson JA, San Diego AG, Soloman MR: Ferromag-netism of intraocular foreign body causes unilateral blindness after MR study.AJNR Am J Neuroradiol 1986; 7:243–5
15. Jackson JG, Acker JD: Permanent eyeliner and MR imaging. AJR Am JRoentgenol 1987; 49:1080
16. Lund G, Nelson JD, Wirtschafter JD, Williams PA: Tattooing of eyelids:Magnetic resonance imaging artifacts. Ophthalmol Surg 1986; 17:550–3
17. Wagle WA, Smith M: Tattoo-induced skin burn during MR imaging. AJRAm J Roentgenol 2000; 174:1795
18. Applebaum E, Valvassori G: Further studies on the effects of magnetic reso-nance fields on middle ear implants. Ann Otol Rhinol Laryngol 1990; 99:801–4
19. Barrafato D, Henkelman RM: Magnetic resonance imaging and surgicalclips. Can J Surg 1984; 27:509–12
20. Becker RL, Forfray JF, Teitelbaum GP, Bradley WG Jr, Jacobs JB, WacaserL, Rieman RL: MR imaging in patient with intracranial aneurysm clips. AJNRAm J Neuroradiol 1988; 9:885–9
21. Brown MA, Carden JA, Coleman RE, McKinney R, Spicer LD: Magnetic fieldeffects on surgical ligation clips. Magn Reson Imaging 1987; 5:443–53
22. Chou C-K, McDougall JA, Chan KW: RF heating of implanted spinal fusionstimulator during magnetic resonance imaging. IEEE Trans Biomed Eng 1997;44:367–72
23. Davis PL, Crooks L, Arakawa M, McRii R, Kaufman L, Margulis AR: Potentialhazards of NMR imaging: Heating effects of changing magnetic fields and RFfields on small metallic implants. AJR Am J Roentgenol 1981; 137:857–60
24. Dujovny M, Kossovsky N, Kossowsky R, Valdivia R, Suk JS, Diaz FG,Berman K, Cleary W: Aneurysm clip motion during magnetic resonance imaging:In vivo experimental study with metallurgical factor analysis. Neurosurgery1985; 17:543–8
25. Edwards MB, Taylor KM, Shellock FG: Prosthetic heart valves: Evaluationof magnetic field interaction, heating and artifacts at 1.5 T. J Magn Reson Imaging2000; 12:363–9
26. Gegauff AF, Laurell KA, Thavendrarajah A, Rosenstiel SF: A potential MRIhazard: Forces on dental magnet keepers. J Oral Rehabil 1990; 17:403–10
27. Hartnell GG, Spence L, Hughe LA, Cohen MC, Saouf R, Buff B: Safety of MRimaging in patients who have retained metallic materials after cardiac surgery.Am J Roentgenol 1997; 168:1157–9
28. Hug J, Nagel E, Bornstedt A, Schnackenburg B, Oswald H, Fleck E: Coronaryarterial stents: Safety and artifacts during MR imaging. Radiology 2000; 216:781–7
29. Kaste S, Laningham F, Stazzone M, Brown SD, Emery K, Newman B,Racadio J, Estroff J, Brill P, Mendelson KL, Slovis TL, Frush D: Safety in pediatricMR and cardiac CT: Results of a membership survey of the Society for PediatricRadiology—2006. Pediatr Radiol 2007; 37:409–12
30. Kean DM, Worthington BS, Firth JL, Hawkes RC: The effect of magneticresonance imaging on different types of microsurgical clips. J Neurol NeurosurgPsychiatry 1985; 48:286–7
31. Klucznik R, Carrier D, Pyka R, Haid R: Placement of a ferromagneticintracerebral aneurysm clip in a magnetic field with a fatal outcome. Radiology1993; 187:855–6
32. Konings MK, Bartels LW, Smits HFM, Bakker CJG: Heating around intra-vascular guidewires by resonating RF waves. J Magn Reson Imaging 2000;12:79–85
33. Laakman RW, Kaufman B, Han JS, Nelson AD, Clampitt M, O’page AM,Haaga JR, Alfidi RJ: MR imaging in patients with metallic implants. Radiology1985; 157:711–4
34. Moscatel MA, Shellock FG, Morisoli SM: Biopsy needles and devices:Assessment of ferromagnetism and artifacts during exposure to a 1.5 T MRsystem. J Magn Reson Imaging 1995; 5:369–72
35. Pruefer D, Kalden P, Schreiber W, Dahm M, Buerke M, Thelen M, OelertH: In vitro investigation of prosthetic heart valves in magnetic resonance imag-ing: Evaluation of potential hazards. J Heart Valve Dis 2001; 10:410–4
36. Romner B, Olsson M, Ljunggren B, Holtas S, Saveland H, Brandt L, PerssonB: Magnetic resonance imaging and aneurysm clips. J Neurosurg 1989; 70:426–31
37. Shellock FG: Prosthetic heart valves and annuloplasty rings: Assessment ofmagnetic field interactions, heating, and artifacts at 1.5 tesla. J Cardiovasc MagnReson 2001; 3:317–24
38. Shellock FG: Biomedical implants and devices: Assessment of magneticfield interactions with a 3.0-tesla MR system. J Magn Reson Imaging 2002;16:721–32
39. Shellock F, Crues J: High field strength MR imaging and metallic biomed-ical implants: An ex vivo evaluation of deflection forces. AJR Am J Roentgenol1988; 151:389–92
40. Soulon R, Budinger T, Higgins C: Magnetic resonance imaging of pros-thetic heart valves. Radiology 1985; 154:705–7
41. Teitelbaum GP, Lin MC, Watanabe AT, Norfray JF, Young TI, Bradley WGJr: Ferromagnetism and MR imaging: Safety of carotid vascular clamps. AJNRAm J Neuroradiol 1990; 11:267–72
42. Von Roemeling R, Lanning RM, Eames FA: MR imaging of patients withimplanted drug infusion pumps. J Magn Reson Imaging 1991; 1:77–81
43. Wichmann W, Von Ammon K, Fink U, Weik T, Yasargil GM: Aneurysmclips made of titanium: Magnetic characteristics and artifacts in MR. AJNRAm J Neuroradiol 1997; 18:939–44
44. Dempsey MF, Condon B: Thermal injuries associated with MRI. Clin Radiol2001; 56:457–65
45. Kugel H, Bremer C, Puschel M, Fischbach R, Lenzen H, Tombach B, VanAken H, Heindel W: Hazardous situation in the MR bore: Induction in ECG leadscauses fire. Eur Radiol 2003; 13:690–4
46. Anonymous: ECRI: The safe use of equipment in the magnetic resonanceenvironment. Health Devices 2001; 30:421–44
47. Bashein G, Syrory B: Burns associated with pulse oximetry during mag-netic resonance imaging. ANESTHESIOLOGY 1991; 75:382–3
48. Brown TR, Goldstein B, Little J: Severe burns resulting from magneticresonance imaging with cardiopulmonary monitoring: Risks and relevant safetyprecautions. Am J Phys Med Rehabil 1993; 72:166–7
49. Hall SC, Stevenson GW, Suresh S: Burn associated with temperaturemonitoring during magnetic resonance imaging. ANESTHESIOLOGY 1992; 76:152
50. Shellock FG, Slimp GL: Severe burn of the finger caused by using a pulseoximeter during MR imaging. AJR Am J Roentgenol 1989; 153:1105
51. Williams EJ, Jones NS, Carpenter TA, Bunch CS, Menon DK: Testing ofadult and paediatric ventilators for use in a magnetic resonance imaging unit.Anaesthesia 1999; 54:969–74
52. Anonymous: ECRI hazard report: Patient death illustrates the importance## When remodeling or building a new facility, an attempt should be made to
locate recovery and resuscitation in proximity to the MRI suite.
468 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

of adhering to safety precautions in magnetic resonance environments. HealthDevices 2001; 30:311–4
53. Chaljub G, Kramer LA, Johnson RF III, Singh H, Crow WN: Projectilecylinder accidents resulting from the presence of ferromagnetic nitrous oxide oroxygen tanks in the MR suite. AJR Am J Roentgenol 2001; 177:27–30
54. Colletti PM: Size “H” oxygen cylinder: Accidental MR projectile at 1.5 tesla.J Magn Reson Imaging 2004; 19:141–3
55. Achenbach S, Moshage W, Diem B, Bieberle T, Schibgilla V, Bachmann K:Effects of magnetic resonance imaging on cardiac pacemakers and electrodes.Am Heart J 1997; 134:467–73
56. Anfinsen OG, Berntsen RF, Aass H, Kongsgaard E, Amlie JP: Implantablecardioverter defibrillator dysfunction during and after magnetic resonance imag-ing. Pacing Clin Electrophysiol 2002; 25:1400–2
57. Avery JE: Loss prevention case of the month: Not my responsibility! J TennMed Assoc 1988; 81:523–4
58. Bonnett CA, Elson JJ, Fogoros RN: Accidental deactivation of the automaticimplantable cardioverter defibrillator. Am Heart J 1990; 120:696–7
59. Coman JA, Martin ET, Sandler DA, Thomas JR: Implantable cardiac defi-brillator interactions with magnetic resonance imaging at 1.5 tesla. J Am CollCardiol 2004; 43:138A
60. Erlebacher JA, Cahill PT, Pannizzo F, Knowles JR: Effect of magneticresonance imaging on DDD pacemakers. Am J Cardiol 1986; 57:437–40
61. Fetter J, Aram G, Holmes DR Jr, Gray JE, Hayes DL: The effects of nuclearmagnetic resonance imagers on external and implantable pulse generators. Pac-ing Clin Electrophysiol 1984; 7:720–7
62. Fiek M, Remp T, Reithmann C, Steinbeck G: Complete loss of ICD pro-grammability after magnetic resonance imaging. Pacing Clin Electrophysiol 2000;27:1002–4
63. Fontain JM, Mohammed FB, Gottlieb C, Callans DJ, Marchlinski FE: Rapidventricular pacing in a pacemaker patient undergoing magnetic resonance im-aging. Pacing Clin Electrophysiol 1998; 21:1336–9
64. Garcia-Bolao I, Albaladejo V, Benito A, Alegria E, Zubieta JL: Magneticresonance imaging in a patient with a dual-chamber pacemaker. Acta Cardiol1998; 53:33–5
65. Gimbel JR, Bailey SM, Tchou PJ, Ruggieri PM, Wilcox EL: Strategies for thesafe magnetic resonance imaging of pacemaker-dependent patients. Pacing ClinElectrophysiol 2005; 28:1041–6
66. Gimbel JR, Johnson D, Levine PA, Wilkoff BL: Safe performance of mag-netic resonance imaging on five patients with permanent cardiac pacemakers.Pacing Clin Electrophysiol 1996; 19:913–9
67. Gimbel JR, Kanal E, Schwartz KM, Wilkoff BL: Outcome of magneticresonance imaging (MRI) in selected patients with implantable cardioverterdefibrillators (ICDs). Pacing Clin Electrophysiol 2005; 28:270–3
68. Gimbel JR, Trohman RL, Lindsay WC, Clair WK, Wilkoff BL: Strategies forthe safe performance of magnetic resonance imaging in selected ICD patients.Pacing Clin Electrophysiol 2002; 25:618
69. Hayes DL, Holmes DR Jr, Gray JE: Effect of 1.5 tesla nuclear magneticresonance imaging scanner on implanted permanent pacemakers. J Am CollCardiol 1987; 10:782–6
70. Heatlie G, Pennell DJ: Cardiovascular magnetic resonance at 0.5T in fivepatients with permanent pacemakers. J Cardiovasc Magn Reson 2007; 9:15–9
71. Holmes DR Jr, Hayes DL, Gray JE, Merideth J: The effects of magneticresonance imaging in implantable pulse generators. Pacing Clin Electrophysiol1986; 9:360–70
72. Lauck G, von Smekal A, Wolke S, Seelos KC, Jung W, Manz M, Luderitz B:Effects of nuclear magnetic resonance imaging on cardiac pacemakers. PacingClin Electrophysiol 1995; 18:1549–55
73. Luechinger R, Duru F, Scheidegger MB, Boesiger P, Dandinas R: Force andtorque effects of a 1.5 tesla MRI scanner on cardiac pacemakers and ICDs. PacingClin Electrophysiol 2001; 24:199–205
74. Luechinger R, Zeijlemaker VA, Pederson EM, Mortensen P, Falk E, Duru F,Candinas R, Boesiger P: In vivo heating of pacemaker leads during magneticresonance imaging. Eur Heart J 2005; 26:376–83
75. Martin ET, Coman JA, Shellock FG, Pulling CC, Fair R, Jenkins K: Magneticresonance imaging and cardiac pacemaker safety at 1.5 T. J Am Coll Cardiol 2004;43:1315–24
76. Pavlicek W, Geisinger M, Castle L, Borkowski GP, Meaney TF, Bream BL,Gallagher JH: The effects of nuclear magnetic resonance on patients with cardiacpacemakers. Radiology 1983; 147:149–53
77. Roguin A, Zviman MM, Meininger GR, Rodrigues ER, Dickfeld TM,Bluemke DA, Lardo A, Berger RD, Calkins H, Halperin HR: Modern pacemakerand implantable cardioverter/defibrillator systems can be magnetic resonanceimaging safe: In vitro and in vivo assessment of safety and function at 1.5 T.Circulation 2004; 110:475–82
78. Rozner MA, Burton AW, Kumar AJ: Pacemaker complication during MRI.J Am Coll Cardiol 2005; 45:161–2
79. Schmiedel A, Hackenbroch M, Yang A, Nahle CP, Skowasch D, Meyer C,Schimpf R, Schild H, Sommer T: Magnetic resonance imaging of the brain inpatients with cardiac pacemakers: In vitro and in vivo evaluation at 1.5 tesla [inGerman]. Rofo 2005; 177:731–44
80. Shellock FG, Fieno DS, Thomson LJ, Talavage TM, Berman DS: Cardiacpacemaker: In vitro assessment at 1.5 T. Am Heart J 2006; 2:436–43
81. Shellock FG, Fischer L, Fieno DS: Cardiac pacemakers and implantable
cardioverter defibrillators: In vitro magnetic resonance imaging evaluation at1.5-tesla. J Cardiovasc Magn Reson 2007; 9:21–31
82. Shellock FG, O’Neil M, Ivans V, Kelly D, O’Connor M, Toay L, Crues JV:Cardiac pacemakers and implantable cardioverter defibrillators are unaffected byoperation of an extremity MR imaging system. AJR Am J Roentgenol 1999;172:165–70
83. Sommer T, Vahihaus C, Lauck G, von Smekal A, Reinke M, Hofer U, BlockW, Traber F, Schneider C, Gieseke J, Jung W, Schild H: MR imaging and cardiacpacemakers: In vitro evaluation and in vivo studies in 51 patients at 0.5 T.Radiology 2000; 215:869–79
84. Valhaus C, Sommer T, Lewalter T, Schimpf R, Schumacher B, Jung W,Luderitz B: Interference with cardiac pacemakers by magnetic resonance imag-ing: Are there irreversible changes at 0.5 tesla? Pacing Clin Electrophysiol 2001;24:489–95
85. Gimbel JR, Lorig RJ, Wilkoff BL: Safe magnetic resonance imaging ofpacemaker patients. J Am Coll Cardiol 1995; 25:11A
86. Schueler BA, Parrish TB, Lin JC, Hammer BE, Pangrle BJ, Ritenour ER,Kucharczyk J, Truwit CL: MRI compatibility and visibility assessment of implant-able medical devices. J Magn Reson Imaging 1999; 9:596–603
87. Shellock FG, Hatfield M, Simon BJ, Block S, Wamboldt R, Starewica PM,Punchard WFB: Implantable spinal fusion stimulator: Assessment of MRI safety. JMagn Reson Imaging 2000; 12:214–23
88. Bhidayasiri R, Bronstein JM, Sinha S, Krahl SE, Ahn S, Behnke EJ, CohenMS, Frysinger R, Shellock FG: Bilateral neurostimulation systems used for deepbrain stimulation: In vitro study of MRI-related heating at 1.5 T and implicationsfor clinical imaging of the brain. Magn Reson Imaging 2005; 23:549–55
89. Carmichael DW, Pinto S, Limousin-Dowsey P, Thobois S, Allen PJ, LemieuxL, Yousry T, Thornton JS: Functional MRI with active, fully implanted, deep brainstimulation systems: Safety and experimental confounds. Neuroimage 2007;37:508–17
90. De Andres J, Valıa JC, Cerda-Olmedo G, Quiroz C, Villanueva V, Martinez-Sanjuan V, de Leon-Casasola O: Magnetic resonance imaging in patients withspinal neurostimulation systems. ANESTHESIOLOGY 2007; 106:779–86
91. Finelli DA, Rezai AR, Ruggieri PM, Tkach JA, Nyenhuis JA, Hrdlicka G,Sharan A, Gonzalez-Martinez J, Stypulkowski PH, Shellock FG: MR imaging-related heating of deep brain stimulation electrodes: In vitro study. Am J Neu-roradiol 2002; 23:1795–802
92. Heller J, Brackman D, Tucci D, Nyenhuis J, Chou C: Evaluation of MRIcompatibility of the modified nucleus multichannel auditory brainstem andcochlear implants. Am J Otol 1996; 17:724–9
93. Rezai AR, Finelli D, Nyenhuis JA, Hrdlicka G, Tkach J, Sharan A, Rugieri P,Stypulkowski PH, Shellock FG: Neurostimulation systems for deep brain stimu-lation: In vitro evaluation of MRI-related heating at 1.5 tesla. J Magn ResonImaging 2002; 15:241–50
94. Baker KB, Nyenhuis JA, Hrdlicka G, Rezai AR, Tkach JA, Shellock FG:Neurostimulation systems: Assessment of magnetic field interactions associatedwith 1.5- and 3-tesla MR systems. J Magn Reson Imaging 2005; 21:72–7
95. Utti RJ, Tsuboi Y, Pooley RA, Putzke JD, Turk MF, Wszolek Z, Witte RJ,Wharen RE Jr: Magnetic resonance imaging and deep brain stimulation. Neuro-surgery 2002; 51:1423–31
96. Williams MD, Antonelli PJ, Williams LS, Moorhead JE: Middle ear prosthesisdisplacement in high-strength magnetic fields. Otol Neurotol 2001; 22:158–61
97. Ferris NJ, Kavnoudias H, Thiel C, Stuckey S: The 2005 Australian MRIsafety survey. AJR Am J Roentgenol 2007; 188:1388–94
98. American Society of Anesthesiologists: Standards for basic anestheticmonitoring, Standards, Guidelines and Statements 2006. Available at: http://www.asahq.org/publicationsAndServices/standards/02.pdf. Accessed Octo-ber 17, 2008
99. Holshouser BA, Hinshaw DB, Shellock FG: Sedation, anesthesia, and phys-iologic monitoring during MR imaging: Evaluation of procedures and equipment.J Magn Reson Imaging 1993; 3:553–8
100. Odegard KC, Dinardo JA, Tsai-Goddman B, Powell AJ, Geva T, LaussenPC: Anaesthesia considerations for cardiac MRI in infants and children. PaediatrAnaesth 2004; 14:471–6
101. Salvo I, Colombo S, Capocasa T, Torri G: Pulse oximetry in MRI units.J Clin Anesth 1990; 2:65–6
102. Barnett GH, Ropper AH, Johnson KA: Physiological support and moni-toring of critically ill patients during magnetic resonance imaging. J Neurosurg1988; 68:246–50
103. Henneberg S, Hok B, Wiklund L, Sjodin G: Remote auscultatory patientmonitoring during magnetic resonance imaging. J Clin Monit 1992; 8:37–43
104. Mason KP, Burrows PE, Dorsey MM, Zurakowski D, Krauss B: Accuracyof capnography with a 30 foot nasal cannula for monitoring respiratory rate andend-tidal CO2 in children. J Clin Monit Comput 2000; 16:259–62
105. Roth JLO, Nugent M, Gray JE, Julsrud RR: Patient monitoring duringmagnetic resonance imaging. ANESTHESIOLOGY 1985; 62:80–3
106. Jorgensen NH, Messick JM, Gray J, Nugent M, Berquist TH: ASA moni-toring standards and magnetic resonance imaging. Anesth Analg 1994; 79:1141–7
107. Beebe DS, Tran P, Bragg M, Stillman A, Truwitt C, Belani KG: Trainednurses can provide safe and effective sedation for MRI in pediatric patients. CanJ Anaesth 2000; 47:205–10
108. Hubbard AM, Markowitz RI, Kimmel B, Kroger M, Bartko MB: Sedation forpediatric patients undergoing CT and MRI. J Comput Assist Tomogr 1992; 16:3–6
469PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

109. Manuli MA, Davies L: Rectal methohexital for sedation of children duringimaging procedures. AJR Am J Roentgenol 1993; 160:577–80
110. Slovis TL, Parks C, Reneau D, Becker CJ, Hersch J, Carver CD, Ross RD,Tech K, Towbin RB: Pediatric sedation: Short-term effects. Pediatr Radiol 1993;23:345–8
111. Volle E, Park W, Kaufman HJ: MRI examination and monitoring ofpediatric patients under sedation. Pediatr Radiol 1996; 26:280–1
112. Shorrab AA, Demain AD, Atallah MM: Multidrug intravenous anesthesiafor children undergoing MRI: A comparison with general anesthesia. PaediatrAnaesth 2007; 17:1187–93
113. Greenberg SB, Faerber EN, Aspinall CL, Adams RC: High-dose chloralhydrate sedation for children undergoing MR imaging: Safety and efficacy inrelation to age. AJR Am J Roentgenol 1993; 161:639–41
114. Shepherd JK, Hall-Craggs MA, Finn JP, Bingham RM: Sedation in childrenscanned with high-field magnetic resonance: The experience at the Hospital forSick Children, Great Ormond Street. Br J Radiol 1990; 63:794–7
115. Vangerven M, Van Hemelrijck J, Wouters P, Vandermeersch E, Van Aken H:Light anaesthesia with propofol for paediatric MRI. Anaesthesia 1992; 47:706–7
116. Bloomfield EL, Masaryk TJ, Caplin A, Obuchowski NA, Schubert A,Hayden J, Ebrahim ZY, Ruggieri PM, Goske MJ, Ross JS: Intravenous sedation forMR imaging of the brain and spine in children: Pentobarbital versus propofol.Radiology 1993; 186:93–7
117. Bluemke DA, Breiter SN: Sedation procedures in MR imaging: Safety,effectiveness, and nursing effect on examinations. Radiology 2000; 216:645–52
118. Connor L, Burrows PE, Zurakowski D, Bucci K, Gagnon DA, Mason KP:Effects of IV pentobarbital with and without fentanyl on end-tidal carbon dioxidelevels during deep sedation. AJR Am J Roentgenol 2003; 181:1691–4
119. De Sanctis Briggs V: Magnetic resonance imaging under sedation innewborns and infants: A study of 640 cases using sevoflurane. Paediatr Anaesth2005; 15:9–15
120. Malviya S, Voepel-Lewis T, Eldevik OP, Rockwell DT, Wong JH, Tait AR:Sedation and general anaesthesia in children undergoing MRI and CT: Adverseevents and outcomes. Br J Anaesth 2000; 84:743–8
121. Mason KP, Sanborn P, Zurakowski D, Karian VE, Connor L, Fontaine PJ,Burrows PE: Superiority of pentobarbital versus chloral hydrate for sedation ininfants during imaging. Radiology 2004; 230:537–42
122. Mason KP, Zurakowski D, Connor L, Karian VE, Fontaine PJ, Sanborn PA,Burrows PE: Infant sedation for MR imaging and CT: Oral versus intravenouspentobarbital. Radiology 2004; 233:723–8
123. Merola C, Albarracin C, Lebowitz P, Bienkowski RS, Barst SM: An audit ofadverse events in children sedated with chloral hydrate or propofol duringimaging studies. Paediatr Anaesth 1995; 5:375–8
124. Pershad J, Wan J, Anghelescu DL: Comparison of propofol with pento-barbital/midazolam/fentanyl sedation for magnetic resonance imaging of thebrain in children. Pediatrics 2007; 120:e629–36
125. Sanborn PA, Michna E, Zurakowski D, Burrows PE, Fontaine PJ, ConnorL, Mason KP: Adverse cardiovascular and respiratory events during sedation ofpediatric patients for imaging examinations. Radiology 2005; 237:288–94
126. Sury MRJ, Harker H, Thyomas ML: Sevoflurane sedation in infants under-going MRI: A preliminary report. Paediatr Anaesth 2005; 15:16–22
127. Vade A, Sukhani R, Dolenga M, Habisohn-Schuck C: Chloral hydratesedation of children undergoing CT and MR imaging: Safety as judged by Amer-ican Academy of Pediatrics guidelines. AJR Am J Roentgenol 1995; 165:905–9
128. Woodthorpe C, Trigg A, Alison G, Sury M: Nurse led sedation for paedi-atric MRI: Progress and issues. Paediatr Nurs 2007; 19:14–8
129. American Society of Anesthesiologists: Practice advisory for the preven-tion and management of operating room fires. ANESTHESIOLOGY 2008; 108:786–801
130. American Society of Anesthesiologists: Standards for postanesthesia care,ASA Standards, Guidelines and Statements. October 2007. Available at: http://www.asahq.org/publicationsAndServices/standards/36.pdf. Accessed October17, 2008
Appendix 1: Facility Levels for MRI Suites
This Advisory categorizes MRI facilities into three general levels accord-ing to the anticipated level of patient care required. These levels describethe physical plant, technical infrastructure, and resources needed to de-liver patient care according to standards already established by the ASAand other professional organizations for sedation, anesthesia, and moni-tored care.
Level I: Facilities That Image Patients Who Do NotRequire Medical Support or Physiologic MonitoringThese facilities do not typically have available oxygen supplies,
suction, physiologic monitors, resuscitation equipment, or non-MRImedical support personnel on site, although some level 1 facilities mayprovide such services or equipment. Level 1 facilities do not containsuitable equipment or infrastructure for the care of critical patients,infants, emergency patients, patients needing anesthesia or sedation,or other patients with high-risk medical conditions.
Level II: Facilities That Image Patients RequiringAny Level of Anesthesia or Critical Care, IncludingNoninvasive or Invasive Monitoring and LifeSupportFacilities with this designation provide imaging for patients receiv-
ing sedation or anesthesia; intensive care patients requiring continuousmonitoring, drug infusions, or mechanical ventilation; and patientsneeding emergent scans. Non-MRI personnel (e.g., anesthesiologists,emergency physicians, intensivists, house staff, nurses, nurse practitio-ners) are typically present to provide patient care. Patient monitoringsystems designated as safe/conditional for zone IV are required in thesefacilities. Level II facilities provide medical gases (oxygen, nitrousoxide, air), patient suction, and evacuation of anesthetic gases. Back upoxygen resources in nonferromagnetic (e.g., aluminum) canisters arealso available. Finally, oxygen and suction are readily available in zoneII or III for patients who need to be evacuated from zone IV foremergent resuscitation.
Level III: Facilities That Provide Imaging forOperative ProceduresFacilities with this designation contain all resources (i.e., physical
plant and technical infrastructure) commensurate with level II facilitiesand, in addition, provide an operative team of non-MRI personnel withthe appropriate surgical tools and equipment (e.g., availability of addi-tional gases such as nitrogen to power surgical equipment). All legalcodes and standards for operating rooms (such as air turnover andventilation) apply.
470 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Appendix 2: Primary Findings of theAdvisory Task Force
I. Education● All anesthesiologists should have general safety education on the
unique physical environment of the MRI scanner, and specific edu-cation regarding the specific features of individual scanners withintheir institution.� Education should emphasize safety for entering zones III and IV, with
special emphasis on hazards in this environment and effects on mon-itoring capabilities.
� Education should address potential health hazards (e.g., high decibellevels and high-intensity magnetic fields).
� Education should address necessary precautions to deal with thespecific field strength and the safety of the MRI scanners within theirinstitutions.
� Education should include information regarding ferromagnetic items(e.g., stethoscopes, pens, wallets, watches, hair clips, name tags, pag-ers, cell phones, credit cards, batteries) and implantable devices (e.g.,spinal cord stimulators, implanted objects) that should not be broughtinto zone III or IV of the MRI suite or should be brought in withcaution.
● Anesthesiologists should work in collaboration with radiologists,technologists, and physicists within their institutions to ensure thatthe above topics are included in their safety training programs.
● Education should include how to safely respond to code blue situa-tions in zones III and IV, and this information should be integratedinto protocols for the designated code blue team.
II. Screening of Anesthesia Care Providers andAncillary Support Personnel
● The anesthesiologist should work in collaboration with the MRImedical director or designee (e.g., safety officer) to ensure that allanesthesia team personnel entering zone III or IV have been screenedfor the presence of ferromagnetic materials, foreign bodies, andimplanted devices.
III. Patient Screening● For every case, the anesthesiologist should communicate with the
patient, referring physician, and radiologist to determine whether thepatient:� Presents with a high-risk medical condition (e.g., neonatal status or
prematurity, intensive or critical care status, impaired respiratoryfunction; hemodynamic instability and vasoactive infusion re-quirements; comorbidities such as obesity and peripheral vascu-lar disease)
� Requires equipment (e.g., physiologic or invasive monitors; in-tubation, oxygenation, or ventilation equipment)
� Has been screened for implanted devices (e.g., pacemakers, cardio-verter–defibrillators, nerve stimulators)
� Has been screened for implanted ferromagnetic items (e.g., surgicalclips, prosthetic heart valves)
� Has been screened for the presence of imbedded foreign bodies (e.g.,orbital iron filings, eyeliner tattoos)
● The anesthesiologist should communicate with the technologist to en-sure that the patient has been screened for the presence of foreign bodieson the patient (e.g., pierced jewelry, rings) before entering zone III.
● If a patient presents with a high-risk medical condition, the anesthe-siologist should collaborate with all participants, including the refer-ring physician, radiologist, and technologist, to determine how thepatient will be managed during the MRI procedure.� Anticipated changes in level of sedation, muscle relaxation, or
ventilation may also place a patient in a high-risk situation.● For patients with acute or severe renal insufficiency, the anesthesi-
ologist should not administer gadolinium because of the increasedrisk of nephrogenic systemic fibrosis.
● Anesthesiologists should work with their institutions to properlyidentify and label anesthesia-related equipment according to conven-tion (safe, unsafe, or conditional) for each MRI scanner.
● For each MRI location, anesthesiologists should determine the safetyand effectiveness of the equipment needed by the patient during theprocedure.� Care should be taken to ensure that the patient’s equipment does
not interfere with image acquisition or quality.● Cardiac pacemakers and implantable cardioverter–defibrillators are
generally contraindicated for MRI.� When MRI is considered essential by the referring physician and
consulting radiologist, a plan for managing these patients duringthe scan should be developed in collaboration with the orderingphysician, medical director or on-site radiologist, and other appro-priate consultants (e.g., patient’s pacemaker specialist or cardiolo-gist, diagnostic radiologist, device manufacturer).
● MRI may be performed on a limited basis for patients with certainimplanted electronic devices (e.g., deep brain stimulators, vagalnerve stimulators, phrenic nerve stimulators, wire-containing ther-modilution catheters, cochlear implants).� In consultation with the referring physician, the radiologist respon-
sible for the procedure, and the neurosurgeon, the anesthesiologistshould ensure that the presence of the device has been noted anddetermined to be MRI safe/conditional before imaging of thesepatients.
IV. Preparation● For every case, the anesthesiologist should prepare, with support
personnel, a plan for providing optimal anesthetic care within thespecial environment of the MRI suite.� In addition to addressing the medical needs of the patient, features
of the plan should include (1) requirements of the scan and per-sonnel needs, (2) positioning of equipment, (3) special require-ments or unique issues of patient or imaging study, (4) positioningof the anesthesiologist and the patient, and (5) planning for emer-gencies.
● The anesthesiologist should communicate with the radiology personnelto determine the requirements for the scan (e.g., duration of the scan,position of the patient or area of the body in the scanner, positioning ofreceiver coils, need for periods of paused respiration).
● The anesthesiologist should communicate with other anesthesiateam members regarding individual roles for anesthetic care.
● The anesthesiologist should collaborate with the MR technologistand/or facility biomedical engineer to determine and demarcate theoptimal and safe location of movable equipment in relation to thegauss lines within the MRI suite.
● The anesthesiologist should choose a location or position for optimalpatient observation and vigilance during delivery of care, whether inzone III or IV.� Anesthesiologists should have (1) a clear line of sight of the
patient and physiologic monitors, whether by direct observationor by video camera; (2) anesthetic delivery equipment locatedfor optimal control of anesthetic depth and rapid intervention;and (3) access to hospital information systems integral to patientcare.
� In preparing for positioning, the anesthesiologist should takeinto account potential electromagnetic and auditory hazards.
● Anesthesiologists should prepare a plan for rapidly summoning addi-tional personnel in the event of an emergency.� The anesthesiologist should ensure that (1) emergency equipment and
drugs are immediately accessible; (2) emergency communication (e.g.,phone or code button) is immediately available; and (3) an evacuationplan is in place, including an appropriate location outside the scanroom (zone IV) for resuscitation.- This location should be complete with physiologic monitors, oxy-
gen, suction, and other appropriate resuscitation equipment.
471PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

V. Patient Management during MRI● Monitoring
� MRI patients should be monitored in a manner consistent with theASA Standards for Basic Anesthetic Monitoring.
� The anesthesiologist should be familiar with the expected limitationsof available monitoring equipment.- Information from electrocardiograms may be limited due to super-
imposed voltages from blood flow in the high magnetic field (e.g.,ST-segment interpretation may be unreliable, even with highly fil-tered monitors).
� The anesthesiologist should make sure that all monitors used in zoneIV are safe/conditional for the scan.
� A monitor should be available to view vital signs from zone III whenthe anesthesia care provider is not in zone IV.
� Additional care should be taken in positioning electrocardiogram andother monitor leads to eliminate burns, even with nonferromagneticleads.
● Anesthetic care� Although lighter levels of anesthesia may be appropriate during
an MRI scan, the anesthesiologist should be aware that theselighter levels may result in airway complications (e.g., laryngo-spasm, coughing, or other airway compromise), which maynecessitate interruption of the scan for urgent treatment andalteration of anesthetic depth.- Institutional circumstances, patient characteristics, and anes-
thesiologist preference may warrant more aggressive airwaymanagement and deeper anesthetic levels.
� Anesthesiologists should ensure that patients who receive mod-erate or deep sedation are monitored in a manner consistentwith their institution’s protocol for monitoring similarly sedatedpatients elsewhere in the facility.
� Monitoring of exhaled carbon dioxide should be considered forall patients receiving deep sedation and for patients whoseventilation cannot be directly observed during moderate seda-tion.
� Monitoring oxygenation by pulse oximetry is not a substitute formonitoring ventilatory function.
� Equipment and drugs for anesthetic care in the MRI suite shouldmirror what is available in other anesthetizing locations, includ-ing (1) an integrated anesthesia machine, medical gases, and wasteanesthesia gas disposal or gas scavenging, when inhalational anesthe-sia is administered; (2) suction; (3) adequate electrical outlets andlighting; and (4) storage areas for equipment and drugs.
� Equipment used in the MRI suite should be appropriate for the age andsize of the patient.
� MRI-safe/conditional anesthesia machines are always preferred for usein an MRI facility.- When an MRI-safe/conditional anesthesia machine is not available,
inhalational anesthetics can be administered from an anesthesiamachine inside zone III via an elongated circuit through a waveguide.
- If total intravenous anesthesia is used, it should be administered byusing (1) MRI-safe/conditional pumps in zone IV, (2) traditional (i.e.,MRI unsafe) pumps in zone III with intravenous tubing passedthrough a wave guide, or (3) periodic bolus injections in zone III orIV.
● Although an anesthesia machine may not be required for the admin-istration of total intravenous anesthesia, there must be equipmentimmediately available for the administration of positive pressureventilation with oxygen.
● Airway management� The anesthesiologist should have an advance plan in place to deal
with instrumentation of the airway and common airway problems
(e.g., obstruction, secretions, laryngospasm, apnea and hypoventi-lation) when patients are in an MRI environment.
� If the patient is at risk for airway compromise, more aggressiveairway management (e.g., use of a endotracheal tube or laryngealmask airway), should be instituted because the patient’s airwaymay be less accessible when the patient is in the scanner.
� Complex airway management (e.g., fiberoptic intubation) shouldbe performed in a controlled environment outside of zone IV.
� Alternative airway devices should be immediately available in theMRI suite.
� Suction equipment should be immediately accessible to the pa-tient’s airway at all times.
VI. Management of Emergencies● When a patient has a medical emergency (e.g., cardiopulmonary
arrest) in the MRI scanner, the following should occur: (1) Immedi-ately remove the patient from zone IV while initiating cardiopulmo-nary resuscitation, if indicated; (2) call for help; and (3) transport thepatient to a previously designated safe area for resuscitation that isnot in zone IV.� This location should be as close to zone IV as possible so as not to
delay resuscitation efforts, and should contain the following resus-citation equipment: a defibrillator, vital signs monitors, and a codecart that includes resuscitation drugs, airway equipment, oxygen,and suction.
● When a fire occurs in the MRI suite, team members should performtheir preassigned fire management task as quickly as possible, inaccordance with the ASA Practice Advisory for the Prevention andManagement of Operating Room Fires.� If a team member cannot rapidly perform his or her task in the
predetermined order, other team members should perform theirtasks without waiting.
� When a team member has completed a preassigned task, he orshe should help other members perform tasks that are not yetcomplete.
● In the case of projectile emergencies, team members should performtheir institution’s protocol in reaction to this occurrence.� If possible, immediately remove the patient from zone IV and
discontinue the scan.� If the patient is injured, proceed with medical emergency manage-
ment as indicated above.� A controlled quench may be necessary to remove the patient from
the bore.● When a quench occurs, team members should perform their institu-
tion’s protocol in reaction to this occurrence. If possible, (1) imme-diately remove the patient from zone IV and (2) immediately admin-ister oxygen to the patient.� Powerful static magnetic fields may persist after a quench, and
therefore the usual precautions apply when entering zone IV.● Emergency response personnel should be restricted from entering
zone IV during any environmental emergency because of the persis-tent magnetic field.
VII. Postprocedure Care● The anesthesiologist should collaborate with the radiologist and
other staff in the postprocedure care of the patient.● Patients receiving sedation or anesthesia within the MRI suite should
have access to postanesthetic care consistent with that provided inother areas of the institution, including transport to other recoveryrooms, dedicated intensive care, or recovery areas within the MRIsuite.
● In all situations, intensive care and recovery areas should include accessto vital sign monitors, oxygen, suction, resuscitation equipment, andtrained personnel.
● Patients should be given oral and written discharge instructions.
472 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Appendix 3: Methods and Analyses
For this Advisory, a systematic review and evaluation of the literaturewas conducted, and formal survey opinion data were obtained fromexperts and ASA members. Informal opinion-based information fromother sources (e.g., open forums, Internet postings) was also used inthe development of this document. Both the literature evaluation andthe survey opinion data were based on evidence linkages, or state-ments regarding potential relations between patient care interventionsand safety outcomes in the MRI suite.*** The evidence linkage inter-ventions are listed below.
I. Education1. MRI education for magnet hazards2. MRI education for monitoring limitations3. MRI education for long-term health hazards
II. Screening of Anesthesia Care Providers and Ancillary SupportPersonnel4. Mandatory screening of all personnel entering zone III or IV
III. Patient Screening5. Patient-related risks for adverse outcomes related to MRI6. Equipment-related risks for adverse outcomes related to MRI
IV. Preparation7. Planning for the anesthetic care of the patient for the scan8. Planning for rapidly summoning additional personnel in the
event of an emergency
V. Patient Management during MRI9. Monitoring during MRI
10. Anesthetic care during MRI11. Airway management during MRI
VI. Management of Emergencies12. Medical emergencies13. Environmental emergencies
VII. Postprocedure Care14. Postprocedure care consistent with that provided for other
areas of the institution
A. State of the LiteratureFor the literature review, potentially relevant studies were identified
via electronic and manual searches of the literature. The literaturesearch covered a 36-yr period from 1973 through 2008. More than
1,200 citations were initially identified, yielding a total of 343 articlesthat addressed topics related to the evidence linkages and met ourcriteria for inclusion. After review of the articles, 186 studies did notprovide direct evidence and were subsequently eliminated. A total of157 articles contained direct linkage-related evidence (see Supplemen-tal Digital Content 1, which is a complete list of references used todevelop this Advisory, http://links.lww.com/A623).††† No evidencelinkage contained enough studies with well-defined experimental de-signs and statistical information to conduct a quantitative analysis (i.e.,meta-analysis).
Interobserver agreement among Task Force members and two meth-odologists was established by interrater reliability testing. Agreementlevels using a � statistic for two-rater agreement pairs were as follows:(1) type of study design, � � 0.49–0.85; (2) type of analysis, � �0.54–0.93; (3) evidence linkage assignment, � � 0.77–1.00; and (4)literature inclusion for database, � � 0.78–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav � 0.65, Var(Sav) � 0.009; (2) type of analysis, Sav � 0.69, Var (Sav) � 0.010; (3)linkage assignment, Sav � 0.85, Var (Sav) � 0.004; and (4) literaturedatabase inclusion, Sav � 0.85, Var (Sav) � 0.013. These valuesrepresent moderate to high levels of agreement.
B. Consensus-based EvidenceConsensus was obtained from multiple sources, including (1) survey
opinion from consultants who were selected based on their knowledgeor expertise in MRI, (2) survey opinions solicited from active membersof the ASA, (3) testimony from attendees of a publicly held open forumat two national anesthesia meetings, (4) Internet commentary, and (5)Task Force opinion and interpretation. The survey rate of return was63% (n � 50 of 79) for the consultants, and 989 surveys were receivedfrom active ASA members. Results of the surveys are reported in tables2 and 3 and are reported in summary form in the text of the Advisory.
The consultants were asked to indicate which, if any, of the evi-dence linkages would change their clinical practices if the Advisorywas instituted. The rate of return was 29% (n � 23 of 79). The percentof responding consultants expecting a change in their practice associ-ated with each linkage topic was as follows: (1) education, 30%; (2)screening of anesthesia care providers and ancillary support personnel,13%; (3) patient screening, 26%; (4) preparation,13%; (5) patient man-agement during MRI—monitoring, 4%; (6) patient management duringMRI—anesthetic care, 0%; (7) patient management during MRI—air-way, 0%; (8) patient management during MRI—emergencies, 13%; and(9) postprocedure care, 9%. Seventy-four percent indicated that theirclinical practice would not need new equipment, supplies, or trainingto implement the Practice Advisory. Eighty-five percent indicated thatthe Advisory would not require ongoing changes in their practice thatwould affect costs. Ninety-five percent of the respondents indicated thatthe Advisory would have no effect on the amount of time spent on atypical case, and 5% indicated that there would be a 10-min increase in theamount spent on a typical case with the implementation of this Advisory.
*** Outcomes for the listed interventions refer to the occurrence of safety-based outcomes.
††† A complete list of references used to develop this Advisory is also availableby writing to the American Society of Anesthesiologists.
473PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 2. Consultant Survey Responses
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1. All anesthesiologists should have general safety education on the
unique physical environment of the MRI scanner50 90.0* 10.1 0.0 0.0 0.0
2. All anesthesiologists should have specific education regarding thefeatures of individual scanners within their institutions
50 58.0* 38.0* 2.0 2.0 0.0
3. All anesthesiologists should work in collaboration with radiologists,technologists, and physicists within their institutions to develop safetytraining programs
50 80.0* 16.0 2.0 2.0 0.0
Screening of anesthesia care providers and ancillary support personnel4. The anesthesiologist should work in collaboration with the MRI
medical director or designee to ensure that all anesthesia teampersonnel entering zone III or IV have been properly screened
50 60.0* 34.0 4.0 2.0 0.0
Patient screening5a. For every case, the anesthesiologist should communicate with the
patient and radiologist or referring physician to determine whether thepatient has a high-risk medical condition
58.0* 20.0 10.0 10.0 2.0 58.0*
5b. If the patient presents with a high-risk medical condition, theanesthesiologist should collaborate with all participants, including thereferring physician, radiologist, and technologist, to determine howthe patient will be managed during the MRI procedure
50 58.0* 26.0 4.0 10.0 2.0
5c. For patients with acute or severe renal insufficiency, theanesthesiologist should not administer gadolinium because of theincreased risk of nephrogenic systemic fibrosis
49 34.7 34.7* 26.5 4.1 0.0
6a. For every case, the anesthesiologist should communicate with theradiologist or referring physician to determine whether the patientrequires equipment that may pose a risk during the scan
49 28.6 36.7* 18.4 14.3 2.0
6b. The anesthesiologist should determine the safety and effectiveness ofthe equipment needed by the patient during the procedure for eachMRI location
50 46.0 34.0* 10.0 10.0 0.0
6c. Anesthesiologists should work with their institutions to properlyidentify and label anesthesia-related equipment according toconvention (safe, unsafe, or conditional) for each MRI scanner
50 74.0* 26.0 0.0 0.0 0.0
6d. Care should be taken to ensure that anesthesia equipment does notinterfere with image acquisition or quality
50 68.0* 30.0 2.0 0.0 0.0
7a. In general, MRI should not be performed on patients with implantedelectronic devices
50 22.0 48.0* 14.0 14.0 2.0
7b. When MRI is considered essential by the referring physician andconsulting radiologist, a plan for managing a patient with implantedelectronic devices during the scan should be developed incollaboration with the referring physician, medical director, or on-siteradiologist and other appropriate consultants
50 72.0* 26.0 0.0 2.0 0.0
Preparation8. For every case, the anesthesiologist should prepare, with support
personnel, a plan for providing optimal anesthetic care within thespecial environment of the MRI suite
50 72.0* 26.0 0.0 2.0 0.0
9. The anesthesiologist should communicate with the radiologypersonnel to determine the requirements for the scan (e.g., durationof the scan, position of the patient or area of the body in the scanner,positioning of receiver coils, need for periods of paused respiration)
50 68.0* 30.0 0.0 2.0 0.0
10. The anesthesiologist should collaborate with the MRI technologistand/or facility biomedical engineer to determine and demarcate theoptimal and safe location of movable equipment in relation to thegauss lines within the MRI suite
50 62.0* 34.0 2.0 0.0 2.0
11. Because line of sight within the bore will vary depending on thefacility, the anesthesiologist should choose a location or position foroptimal patient observation and vigilance during delivery of care,whether in zone III or IV
50 64.0* 28.0 8.0 0.0 0.0
12. The anesthesiologist should prepare a plan for rapidly summoningadditional personnel in the event of an emergency
50 82.0* 18.0 0.0 0.0 0.0
(continued)
474 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 2. Continued
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
Patient management during MRIMonitoring
13. MRI patients should be monitored in a manner consistent with theASA “Standards for Basic Anesthetic Monitoring”
50 72.0* 26.0 2.0 0.0 0.0
14. Anesthesiologists should be familiar with the expected limitations ofavailable monitoring equipment
50 84.0* 16.0 0.0 0.0 0.0
15. The anesthesiologist should make sure that all monitors used in zoneIV are safe/conditional for the scan
50 82.0* 12.0 0.0 4.0 2.0
16. A monitor should be available to view vital signs from zone IV whenthe anesthesia care provider is not in zone IV
50 78.0* 16.0 6.0 0.0 0.0
Anesthetic care17. In general, because MRI is a nonpainful procedure, lighter levels of
anesthesia may be appropriate, recognizing that institutionalcircumstances, patient preference, and anesthesiologist preferencemay warrant more aggressive airway management and deeperanesthetic levels
50 58.0* 34.0 2.0 6.0 0.0
18. Anesthesiologists should ensure that patients who receive moderateor deep sedation are monitored in a manner consistent with theirinstitution’s protocol for monitoring similarly sedated patientselsewhere in the facility
50 82.0* 18.0 0.0 0.0 0.0
19. Equipment and drugs for anesthetic care in the MRI suite shouldmirror what is available in the OR
50 76.0* 18.0 4.0 2.0 0.0
20a. When an MRI-safe/conditional anesthesia machine is not available,inhalation anesthetics may be administered from an anesthesiamachine inside zone III via an elongated circuit through a wave guide
50 6.0 30.0 24.0* 34.0 6.0
20b. If total intravenous anesthesia is used, it should be administered byusing (1) MRI-safe/conditional pumps in zone IV, (2) traditional (i.e .,MRI-unsafe) pumps in zone III with the intravenous tubing passedthrough a wave guide, or (3) periodic bolus injections in zone III or IV
50 30.0 58.0* 10.0 2.0 0.0
Airway management21. The anesthesiologist should have an advance plan in place to deal
with instrumentation of the airway and common airway problemswhen patients are in an MRI environment
50 88.0* 12.0 0.0 0.0 0.0
22. If the patient is at risk for airway compromise, more aggressiveairway management (e.g., use of a tracheal tube or LMA) should beinstituted because the patient’s airway may be less accessible whenthe patient is in the scanner
50 58.0* 34.0 6.0 2.0 0.0
23. Complex airway management (e.g., fiberoptic intubation) should beperformed in a controlled environment outside of zone IV
50 76.6* 18.0 6.0 0.0 0.0
24. Alternative airway devices should be immediately available in the MRIsuite
50 78.0* 16.0 4.0 2.0 0.0
25. Suction equipment should be immediately accessible to the patient’sairway at all times
49 91.8* 6.1 0.0 2.1 0.0
Management of emergencies26a. When a patient has a medical emergency (e.g., cardiopulmonary
arrest) in the MRI scanner, the following should occur: (1) InitiateCPR, when needed, while immediately removing the patient fromzone IV; (2) call for help; and (3) transport the patient to a previouslydesignated safe location in proximity to the MRI suite
49 81.6* 18.4 0.0 0.0 0.0
26b. The designated safe location should contain the followingresuscitation equipment: a defibrillator, vital signs monitors, and acode cart that includes resuscitation drugs, airway equipment,oxygen, and suction
49 85.7* 14.3 0.0 0.0 0.0
27. When a fire occurs in the MRI suite, team members should performtheir preassigned fire management task as quickly as possible, inaccordance with the ASA “Practice Advisory for the Prevention andManagement of Operating Room Fires”
49 71.4* 14.3 14.3 0.0 0.0
28a. When a quench occurs, team members should perform theirinstitution’s protocol in reaction to this occurrence
49 65.3* 28.6 6.1 0.0 0.0
(continued)
475PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 2. Continued
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
28b. When a quench occurs, if possible, (1) immediately remove thepatient from zone IV and (2) immediately administer oxygen to thepatient
49 55.1* 22.5 20.4 2.0 0.0
29. Because powerful static magnetic fields may persist after a quench orfire, emergency response personnel should be restricted fromentering zone IV
49 44.9 26.5* 20.4 8.2 0.0
Postprocedure care30. The anesthesiologist should collaborate with the radiologist and other
staff in the postanesthetic care of the patient50 62.0* 28.0 0.0 10.0 0.0
31. Patients receiving sedation or anesthesia within the MRI suite shouldhave access to postanesthetic care consistent with that provided inother areas of the institution
50 82.0* 16.0 0.0 2.0 0.0
32. In all situations, intensive care and recovery areas should includeaccess to vital sign monitors, oxygen, suction, and trained personnel
50 84.0* 14.0 2.0 0.0 0.0
33. Patients should be given written discharge instructions 50 66.6* 32.0 2.0 0.0 0.0
* Median.
ASA � American Society of Anesthesiologists; CPR � cardiopulmonary resuscitation; LMA � laryngeal mask airway; MRI � magnetic resonance imaging; n �number of consultants who responded to each item; OR � operating room.
476 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 3. American Society of Anesthesiologists Membership Survey Responses
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1. All anesthesiologists should have general safety education on the
unique physical environment of the MRI scanner989 73.6* 25.0 1.0 0.2 0.2
2. All anesthesiologists should have specific education regarding thefeatures of individual scanners within their institutions
986 33.7 42.4* 18.4 5.1 0.5
3. All anesthesiologists should work in collaboration with radiologists,technologists, and physicists within their institutions to develop safetytraining programs
989 47.0 41.3* 8.1 3.4 0.2
Screening of anesthesia care providers and ancillary support personnel4. The anesthesiologist should work in collaboration with the MRI medical
director or designee to ensure that all anesthesia team personnelentering zone III or IV have been properly screened
988 43.5 45.5* 8.0 2.8 0.2
Patient screening5a. For every case, the anesthesiologist should communicate with the
patient and radiologist or referring physician to determine whether thepatient has a high-risk medical condition
988 54.7* 30.6 6.7 6.9 1.2
5b. If the patient presents with a high-risk medical condition, theanesthesiologist should collaborate with all participants, including thereferring physician, radiologist, and technologist, to determine how thepatient will be managed during the MRI procedure
983 53.8* 34.2 4.6 6.4 1.0
5c. For patients with acute or severe renal insufficiency, theanesthesiologist should not administer gadolinium because of theincreased risk of nephrogenic systemic fibrosis
981 23.7 29.5* 42.9 3.7 0.3
6a. For every case, the anesthesiologist should communicate with theradiologist or referring physician to determine whether the patientrequires equipment that may pose a risk during the scan
976 36.2 38.1* 10.5 12.9 2.4
6b. The anesthesiologist should determine the safety and effectiveness ofthe equipment needed by the patient during the procedure for eachMRI location
977 46.9 38.4* 6.7 6.4 1.7
6c. Anesthesiologists should work with their institutions to properly identifyand label anesthesia-related equipment according to convention (safe,unsafe, or conditional) for each MRI scanner
981 56.6* 38.8 3.0 1.5 0.1
6d. Care should be taken to ensure that anesthesia equipment does notinterfere with image acquisition or quality
980 46.2 49.4 3.1 1.0 0.3
7a. In general, MRI should not be performed on patients with implantedelectronic devices
982 27.8 42.9* 22.2 6.7 0.4
7b. When MRI is considered essential by the referring physician andconsulting radiologist, a plan for managing a patient with implantedelectronic devices during the scan should be developed incollaboration with the referring physician, medical director, or on-siteradiologist and other appropriate consultants
979 53.7* 41.6 2.8 1.3 0.6
Preparation8. For every case, the anesthesiologist should prepare, with support
personnel, a plan for providing optimal anesthetic care within thespecial environment of the MRI suite
977 63.2* 33.6 1.7 1.1 0.4
9. The anesthesiologist should communicate with the radiology personnelto determine the requirements for the scan (e.g., duration of the scan,position of the patient or area of the body in the scanner, positioning ofreceiver coils, need for periods of paused respiration)
980 64.5* 33.1 1.2 1.2 0.0
10. The anesthesiologist should collaborate with the MRI technologist and/or facility biomedical engineer to determine and demarcate the optimaland safe location of movable equipment in relation to the gauss lineswithin the MRI suite
974 48.8 43.2* 6.7 1.2 0.1
11. Because line of sight within the bore will vary depending on the facility,the anesthesiologist should choose a location or position for optimalpatient observation and vigilance during delivery of care, whether inzone III or IV
982 53.8* 39.3 5.1 1.3 0.5
12. The anesthesiologist should prepare a plan for rapidly summoningadditional personnel in the event of an emergency
978 70.6* 28.0 1.0 0.4 0.0
(continued)
477PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 3. Continued
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
Patient management during MRIMonitoring
13. MRI patients should be monitored in a manner consistent with the ASA“Standards for Basic Anesthetic Monitoring”
977 73.7* 22.5 1.4 1.8 0.5
14. Anesthesiologists should be familiar with the expected limitations ofavailable monitoring equipment
978 71.9* 27.8 0.2 0.0 0.1
15. The anesthesiologist should make sure that all monitors used in zoneIV are safe/conditional for the scan
977 68.3* 27.7 2.4 1.3 0.3
16. A monitor should be available to view vital signs from zone IV when theanesthesia care provider is not in zone IV
976 71.6* 24.7 3.5 0.1 0.1
Anesthetic care17. In general, because MRI is a nonpainful procedure, lighter levels of
anesthesia may be appropriate, recognizing that institutionalcircumstances, patient preference, and anesthesiologist preferencemay warrant more aggressive airway management and deeperanesthetic levels
976 53.3* 43.3 1.6 1.2 0.5
18. Anesthesiologists should ensure that patients who receive moderate ordeep sedation are monitored in a manner consistent with theirinstitution’s protocol for monitoring similarly sedated patients elsewherein the facility
976 66.9* 30.2 1.3 1.1 0.4
19. Equipment and drugs for anesthetic care in the MRI suite should mirrorwhat is available in the OR
980 61.4* 33.3 3.3 2.0 0.0
20a. When an MRI-safe/conditional anesthesia machine is not available,inhalation anesthetics may be administered from an anesthesiamachine inside zone III via an elongated circuit through a wave guide
975 10.3 22.8 31.0* 29.1 6.9
20b. If total intravenous anesthesia is used, it should be administered byusing (1) MRI-safe/conditional pumps in zone IV, (2) traditional (i.e.,MRI-unsafe) pumps in zone III with the intravenous tubing passedthrough a wave guide, or (3) periodic bolus injections in zone III or IV
978 24.0 53.2* 12.0 8.7 2.2
Airway management21. The anesthesiologist should have an advance plan in place to deal with
instrumentation of the airway and common airway problems whenpatients are in an MRI environment
979 79.6* 20.1 0.3 0.0 0.0
22. If the patient is at risk for airway compromise, more aggressive airwaymanagement (e.g., use of a tracheal tube or LMA) should be institutedbecause the patient’s airway may be less accessible when the patientis in the scanner
981 72.8* 23.0 2.6 1.6 0.0
23. Complex airway management (e.g., fiberoptic intubation) should beperformed in a controlled environment outside of zone IV
981 71.9* 24.5 2.7 1.0 0.0
24. Alternative airway devices should be immediately available in the MRIsuite
981 70.2* 26.1 2.5 1.2 0.0
25. Suction equipment should be immediately accessible to the patient’sairway at all times
978 86.4* 12.8 0.7 0.1 0.0
Management of emergencies26a. When a patient has a medical emergency (e.g., cardiopulmonary arrest)
in the MRI scanner, the following should occur: (1) Initiate CPR, whenneeded, while immediately removing the patient from zone IV; (2) callfor help; and (3) transport the patient to a previously designated safelocation in proximity to the MRI suite
976 72.2* 25.7 1.8 0.2 0.0
26b. The designated safe location should contain the following resuscitationequipment: a defibrillator, vital signs monitors, and a code cart thatincludes resuscitation drugs, airway equipment, oxygen, and suction
978 79.4* 19.9 0.5 0.1 0.1
27. When a fire occurs in the MRI suite, team members should performtheir preassigned fire management task as quickly as possible, inaccordance with the ASA “Practice Advisory for the Prevention andManagement of Operating Room Fires”
970 65.4* 30.4 4.5 0.0 0.1
28a. When a quench occurs, team members should perform theirinstitution’s protocol in reaction to this occurrence
967 49.1 29.7* 21.2 0.0 0.0
28b. When a quench occurs, if possible, (1) immediately remove the patientfrom zone IV and (2) immediately administer oxygen to the patient
963 49.0 27.6* 22.5 0.7 0.1
(continued)
478 PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009

Table 3. Continued
Percent Responding to Each Item
nStronglyAgree Agree Uncertain Disagree
StronglyDisagree
29. Because powerful static magnetic fields may persist after a quench orfire, emergency response personnel should be restricted from enteringzone IV
973 22.3 28.7* 41.0 7.2 0.8
Postprocedure care30. The anesthesiologist should collaborate with the radiologist and other
staff in the postanesthetic care of the patient979 41.5 41.5* 4.9 10.5 1.6
31. Patients receiving sedation or anesthesia within the MRI suite shouldhave access to postanesthetic care consistent with that provided inother areas of the institution
981 72.0* 27.1 0.5 0.4 0.0
32. In all situations, intensive care and recovery areas should includeaccess to vital sign monitors, oxygen, suction, and trained personnel
977 77.7* 22.3 0.0 0.0 0.0
33. Patients should be given written discharge instructions 981 53.1* 39.4 5.9 1.5 0.1
* Median.
ASA � American Society of Anesthesiologists; CPR � cardiopulmonary resuscitation; LMA � laryngeal mask airway; MRI � magnetic resonance imaging; n �number of American Society of Anesthesiology members who responded to each item; OR � operating room.
479PRACTICE ADVISORY
Anesthesiology, V 110, No 3, Mar 2009










![Neuromonitoring [PDF, 2.5 MB]](https://static.fdocuments.in/doc/165x107/586f5f371a28abf0508bd912/neuromonitoring-pdf-25-mb.jpg)