Anesthesia and Positioning
76
ANESTHESIA AND POSITIONING by: JOVEN A. OCCEÑA, MD. Anesthesia Chief Resident DAVAO REGIONAL HOSPITAL
Transcript of Anesthesia and Positioning

ANESTHESIA AND
POSITIONINGby:
JOVEN A. OCCEÑA, MD.Anesthesia Chief Resident
DAVAO REGIONAL HOSPITAL

ANESTHESIA

OBJECTIVES

CONSIDERATIONS:
1. Quality
2. Safety
3. Efficiency
4. Cost of drugs
5. Equipment

Anesthetic should:
1. have a rapid and smooth onset of action
2. produce intraoperative amnesia and analgesia
3. good surgical conditions with a short recovery period
4. no side effects.

Standard intraoperative monitoring equipment includes:
A. precordial stethoscopeB. electrocardiogram (ECG)C. blood pressure cuffD. pulse oximeter E. capnograph
Several factors have to be taken into consideration:
1. The technique should anesthetize not only the operative field but also all the areas involved in the surgery (e.g., site of tourniquet placement, sites where skin or bone grafts are to be taken)

Several factors have to be taken into consideration:
2. The adequacy of the duration of the sensory block with the expected duration of postoperative pain
3. The physical condition of the patient

Several factors have to be taken into consideration:
4. The local conditions at the site of puncture
5. The suitability of the position required for performing the block according to the lesions and/or the physical condition of the child

Several factors have to be taken into consideration:
6. The similar importance of anesthetic and surgical techniques (under normal conditions, central blocks have to be avoided for minor surgery)
7. The experience of the anesthesiologist


General Anesthesia
General anesthesia remains the most widely used anesthetic technique because of its popularity with patients, surgeons, and anesthesiologists
Anesthesiologist must consider:1. the recovery characteristics of the
anesthetics 2. the management of postoperative pain
and nausea/vomiting when making the anesthesia plan.

General Anesthesia
BENZODIAZEPINES OPIOIDS MUSCLE RELAXANT (non-depolarizing) LIDOCAINE BARBITURATES MUSCLE RELAXANT (depolarizing) –
intubating dose

General Anesthesia
INGALED ANESTHETICS1. HALOTHANE2. ISOFLURANE3. ENFLURANE4. DESFLURANE5. SEVOFLURANE6. METHOXYFLURANE

RATIONALE FOR THE USE OF EPIDURAL AND SPINAL
ANESTHESIA
1. Metabolic and endocrine alterations
2. Blood loss
3. Thromboembolic complications
4. Cardiopulmonary complications
Continuous epidural analgesia for postoperative pain relief

ANATOMYBony structures
Ligaments
Epidural space – located between the ligamentum flavum and the dura mater
Subdural space
Subarachnoid space

PATIENT EVALUATION AND PREPARATION FOR EPIDURAL
AND SPINAL ANESTHESIA Physical examination of the back and history of back problems Coagulation profile Explanation of technique and perceived advantages Description of the forms of sedation available Tailor preoperative medication to level of anxiety and need for analgesia

CONTRAINDICATIONS FOR EPIDURAL AND SPINAL
ANESTHESIA
ABSOLUTE CONTRAINDICATIONS
1. Patient refusal
2. Infection at the puncture site
3. Uncorrected hypovolemia
4. Severe coagulation abnormalities
5. Anatomic abnormalities

CONTRAINDICATIONS FOR EPIDURAL AND SPINAL
ANESTHESIA
RELATIVE CONTRAINDICATIONS
1. Bacteremia
2. Preexisting neurologic disorders (multiple sclerosis)
3. Minidose heparin

TECHNICAL ASPECTS
LANDMARK:
VERTEBRAL SPINAL PROCESSES (MIDLINE)
ILIAC CREST
( A LINE DRAWN BETWEEN
THE CRESTS CROSSES L4)

EPIDURAL ANESTHESIA
17 or 18 gauge tuohy needle (curved Huber point)
Loss of resistance technique
Catheter placement
Test dose = 3-4cc local anesthetic + 1:200,000 epinephrine
SPINAL ANESTHESIA
Midline approach
Paramedian or lateral approach
The Taylor approach
Continuous spinal anesthesia
PHYSIOLOGIC EFFECTS OF SPINAL AND EPIDURAL
ANESTHESIA A. Spinal anesthesia
1. Sympathetic nervous system blockade
2. Cardiovascular systema) Bradycardiab)Venodilationc) Decreased blood pressure
PHYSIOLOGIC EFFECTS OF SPINAL AND EPIDURAL
ANESTHESIA A. Spinal anesthesia
3. Respiratory system
4. Renal system
5. Gastrointestinal system

PHYSIOLOGIC EFFECTS OF SPINAL AND EPIDURAL ANESTHESIA
B. Epidural anesthesia1. Hemodynamic effects
a. Level of anesthesia (above T5)
b. Systemic absorption of local anesthetic
c. Inclusion of epinephrine (B1 and B2 effects)
d. Intravascular fluid volume
e. Cardiovascualr status of the patient
2. Effects on regional blood flow

PHARMACOLOGIC CONSIDERATIONS
A. Spinal anesthesia
1. Selection of a specific local anesthetic
A. Hyperbaric lidocaine
B. Hyperbaric tetracaine
C. Isobaric bupivacaine

PHARMACOLOGIC CONSIDERATIONS
A. Spinal anesthesia
2. Factors that influence distribution of local anesthetics in the CSF
A. Baricity of the local anesthetic solution
B. Shape of the spinal canal
C. Position of the patient
D. Vasoconstrictors

B. Epidural anesthesia
1. The quality of epidural anesthesia is determined by several factors:
A. Local anesthetic selected
B. Mass of the drug injected
C. Addition of epinephrine
D. Site but not speed of injection or patient position
E. Patients >40 yrs of age
F. Pregnancy

COMPLICATIONS OF SPINAL AND EPIDURAL ANESTHESIA
SPINAL1. Hypotension2. Postdural puncture headache
i. Postural component ii. Frontal or occipitaliii. Tinnitusiv. Diplopiav. Young femalesvi. Use of large gauge needle
COMPLICATIONS OF SPINAL AND EPIDURAL ANESTHESIA
SPINAL3. Extensive spread of spinal anesthesia
i. Agitationii. Hypotensioniii. Nauseaiv. Absent intercostal muscle functionv. Inadequate air movement to generate
an audible voiceBackache
5. Major neurologic injury or infection

COMPLICATIONS OF SPINAL AND EPIDURAL ANESTHESIA
EPIDURAL
1. Toxicity due to local anesthetics
i. Site of injection
ii. Total dose
iii.Vasoconstrictor
iv.Pharmacologic profile of local anesthetic

COMPLICATIONS OF SPINAL AND EPIDURAL ANESTHESIA
EPIDURAL2. Technique related
complications:1) Hypotension2) Accidental Subdural or
subarachnoid injection3) Dural puncture and postdural
headache4) Neural damage5) Catheter complications
POSITIONINGTHE SURGICAL
PATIENTS

OBJECTIVES
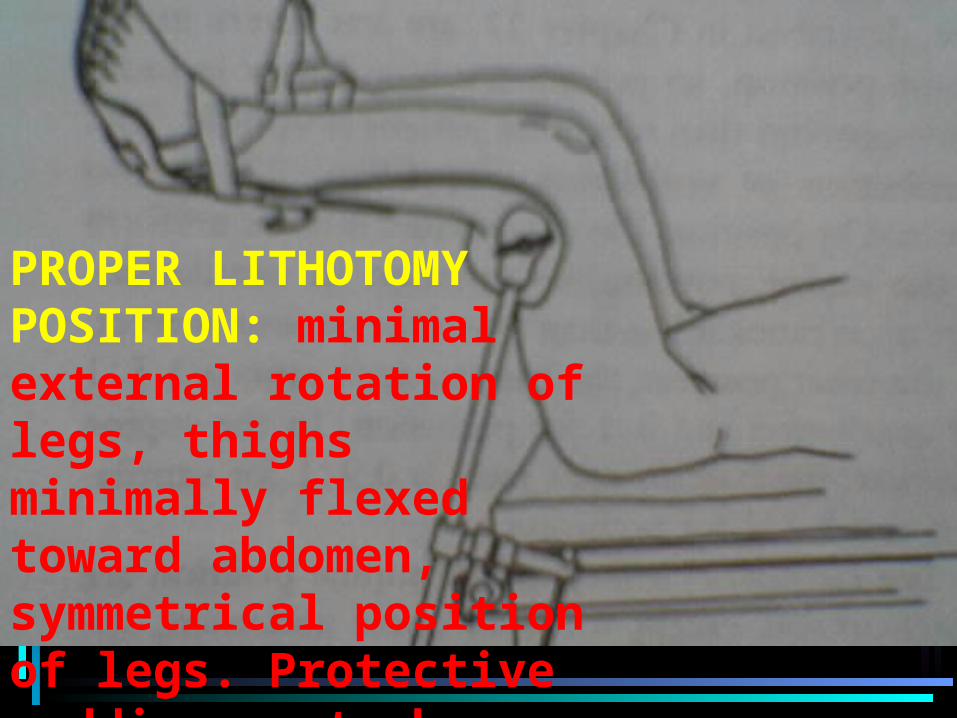
PROPER LITHOTOMY POSITION: minimal external rotation of legs, thighs minimally flexed toward abdomen, symmetrical position of legs. Protective paddings not shown.

CLASSIC PRONE POSITION with arms extended next to head (A), or alongside torso (B). Chest roll placed below clavicle and pillow under iliac crest to along abdomen to hang free. The table is flexed to a variable degree depending on the lumbar lordosis and the needs of the surgeon. With flexion, a subgluteal anchor is needed to prevent caudal slippage of the patient.

CLASSIC PRONE POSITION

The ANDREWS FRAME, which supports the chest and buttocks, with the knees padded. The knees are never flexed more than 90 degrees on the thighs.

ANDREWS FRAME

Methods of avoiding excessive turning of the head in the prone position, A, B, and C are acceptable. Extreme rotation of the neck (D) may be dangerous in patients with cervical spine disease or cerebrovascular disease. The eyes themselves must be free from pressure, since pressure on the globe may reduce flow in the retinal vessels enough to produce permanent retinal blindness.





NEUROSURGICAL SITTING POSITION. The legs are slightly flexed and raised to the level of the heart. The feet are padded to maintained a dorsiflexed position. The sciatic nerve is protected by gluteal padding. The framed of the head holder is clamped to the back section of the table so that the patient head’s head can be lowered in case of air embolism.

NEUROSURGICAL SITTING POSITION

The RIGHT LATERAL DECUBITUS POSITION. (Above) inadequate padding and improper head position. (Below) Padding over bony prominence, chest roll to protect neurovascular bundle in the axilla, and proper alignment of cervical spine. The lower leg is flexed to stabilized the patient.

inadequate padding and improper head position.
Padding over bony prominence, chest roll to protect neurovascular bundle in the axilla, and proper alignment
of cervical spine
FLEXED LATERAL DECUBITUS POSITION. The point of flexion lies beneath the dependent iliac crest to minimize interference with the dependent lung and diaphragm.

FLEXED LATERAL DECUBITUS POSITION

The LAWN CHAIR POSITION with flexion of the hips, minimal knee flexion, and trunk section level.

LAWN CHAIR POSITION

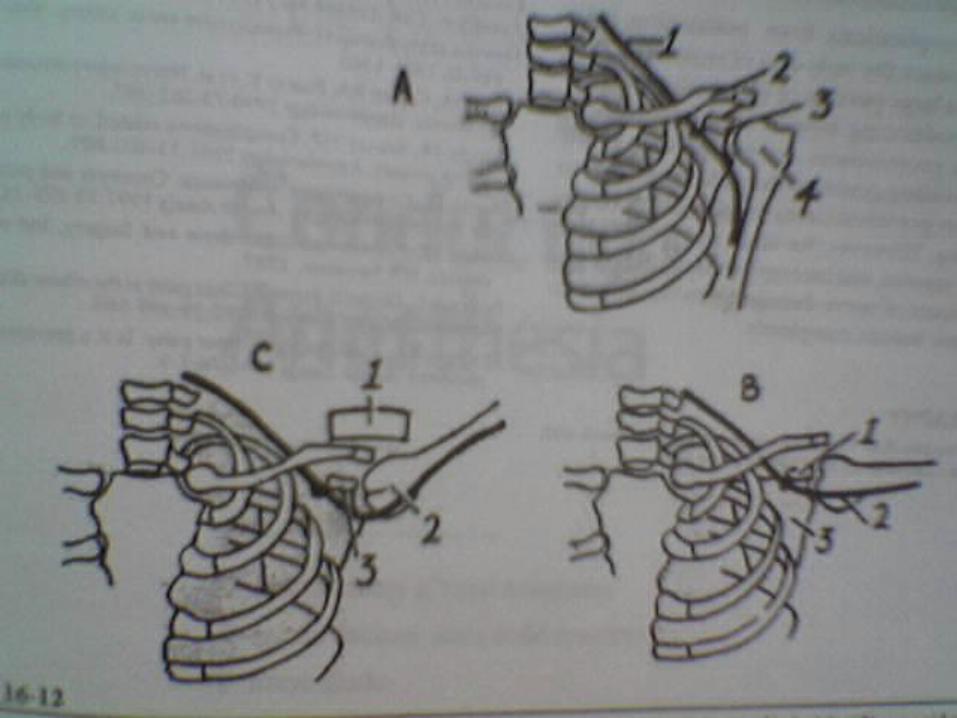
Brachial plexus in relation to surrounding structures. (A) arm at side: 1. Brachial plexus. 2. Clavicle, 3. Coracoid process, and 4. Head of humerus. (B) arm at right angle. (C) arm hyperextended by shoulder brace, depresses scapula, streching brachial plexux beneath coracoid process and around humeral head.

Flexing, then raising of the legs for the lithotomy position

Holding the leg and stirrups for final positioning
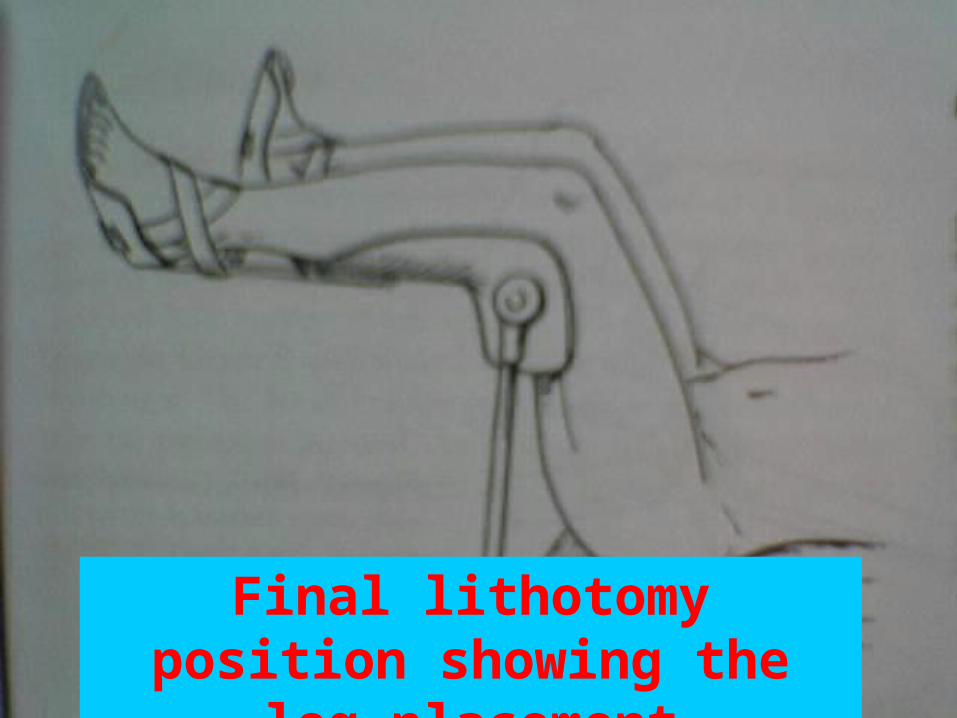
Final lithotomy position showing the leg placement

Lithotomy position with less hip flexion for endoscopic procedures e.g. TURP
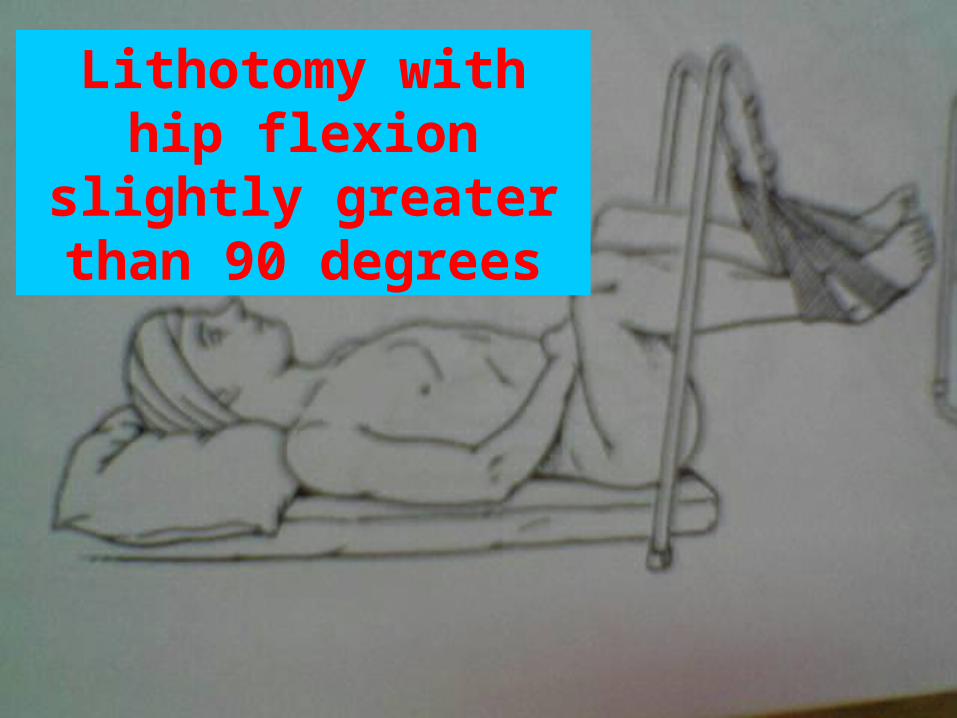
Lithotomy with hip flexion slightly greater
than 90 degrees

Legs do not touch support poles

Straps use instead of stirrups

Risk to fingers when the lower portion of the operating table
is lowered
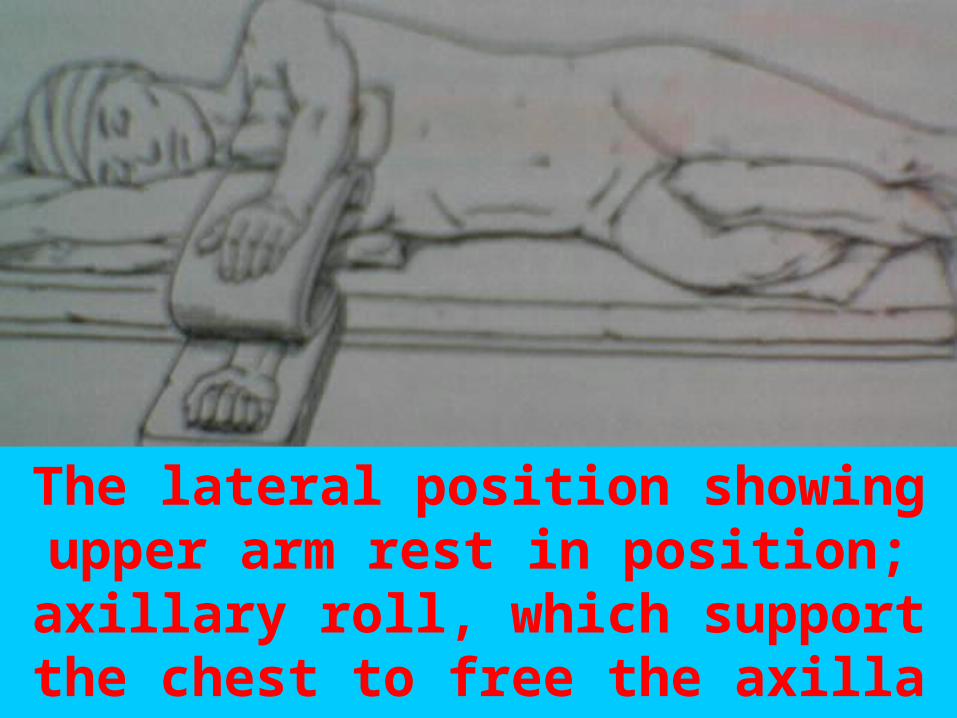
The lateral position showing upper arm rest in position; axillary roll, which
support the chest to free the axilla and 1 type of leg positioning
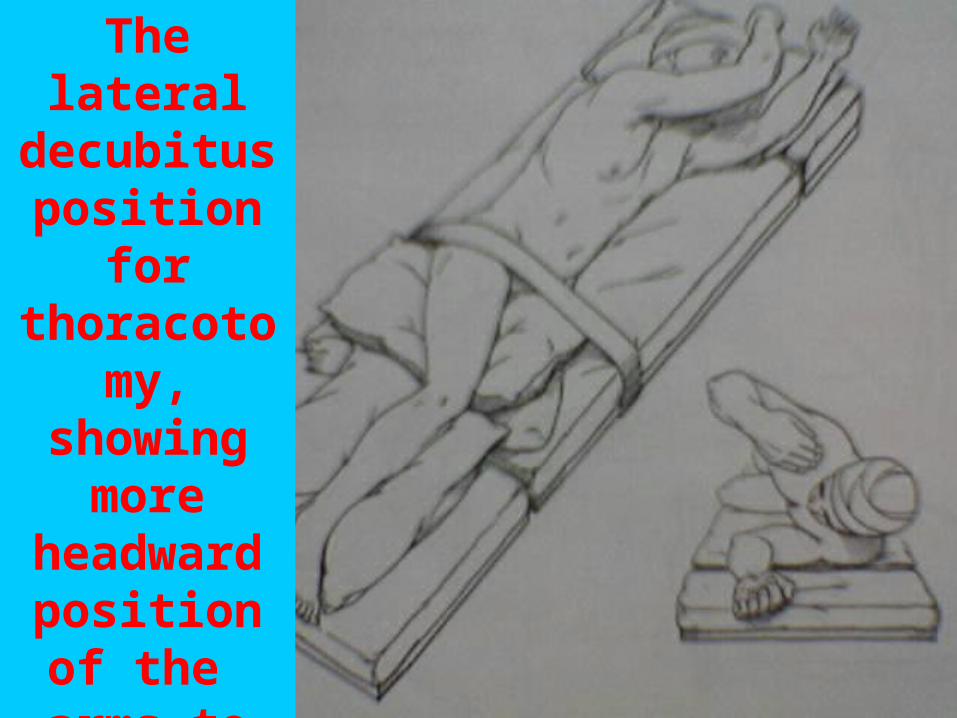
The lateral decubitus
position for thoracotomy,
showing more
headward position of
the arms to facilitate surgical exposure
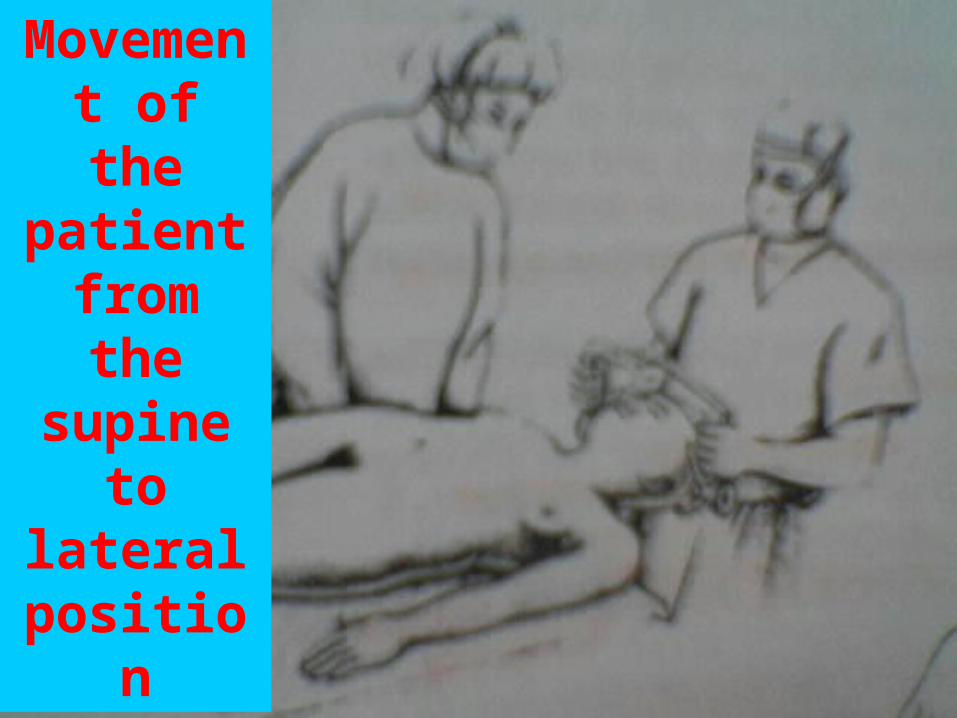
Movement of the
patient from the supine to
lateral position
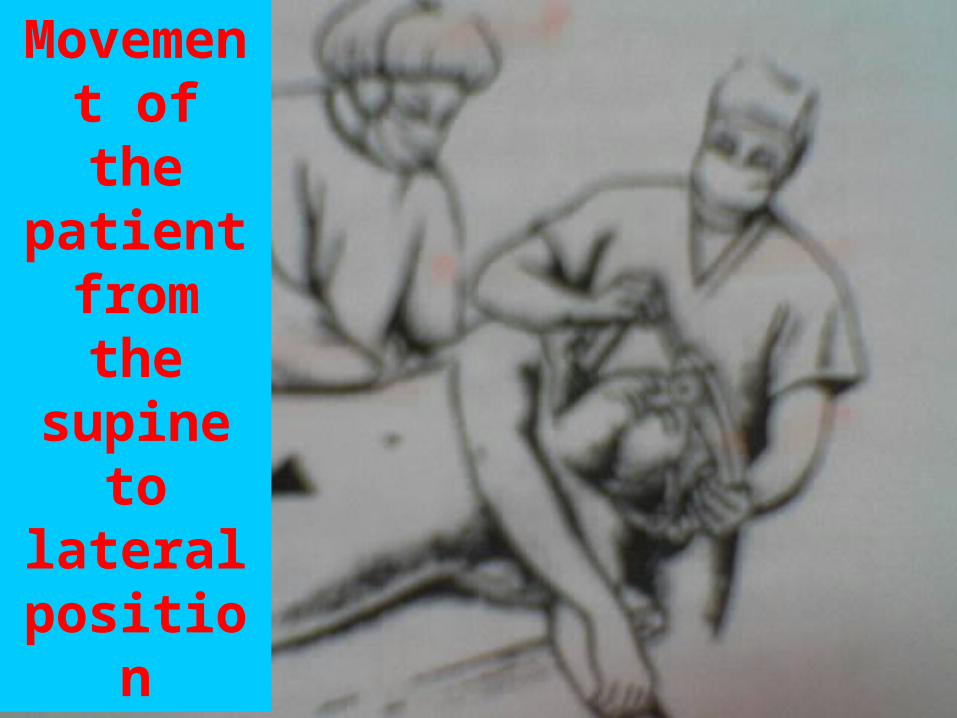
Movement of the
patient from the supine to
lateral position

Movement of the
patient from the supine to
lateral position

Movement of the
patient from the supine to
lateral position

The lateral oblique position ( three-quarters prone). The axillary roll is
placed under the chest, and the lower shoulder is brought forward to the edge of the bed or just slightly over the edge
Femoral neck fracture can be managed in the
supine position on the fracture table

For midfemoral fracture, the patient is placed on the fracture table in the lateral position, with the legs spaced and positioned to allow
xray at an angle in several planes

Lateral view of upright shoulder position. The
endotracheal tube and head are secured to prevent movement
and accidental extubation

Arrangement for surgery in the sitting position. The scrub nurse is to the right of the surgeon to place the instruments into the surgeon’s right
hand. The entire left side of the patient is available for the anesthesiologist’s care

The patient is in semisitting position with the knees flexed slightly. The headrest support is fastened to the upper part of the table so that the head can be lowered without changing the relationship of the pinion head holder to the torso. Arms must be supported and buttocks
padded.

The head can slip while in the horseshoe headrest, and pressure may develop in the eye owing to the weight of the head

GOOD DAY !!!