AND · WThLLIAM GOLDRING TABLE 1-Concluded Urine Poen Redcells Whiteand Number pH Specificgravity...
13
STUDIES OF THE KIDNEY IN ACUTE INFECTION III. OBSERVATIONS WITH THE URINE SEDIMENT COUNT (ADDIS) AND THE UREA CLEARANCE TEST IN LOBAR PNEUMONIA1 By WILLIAM GOLDRING (From the Department of Medicine of New York University and the Third (New York University) Medical Division, Bellevue Hospital, New York) (Received for publication November 29, 1930) McIntosh and Reimann (1) reviewed some previous studies on kidney function in pneumonia. They found that of six investigators, three reported impairment of renal function (2, 3, 4), two reported the absence of impairment (5, 6), and one (7) emphasized the occurrence of renal hyperfunction during the course of lobar pneumonia. It seemed to them that a further series of observations was necessary to throw some light, if possible, on the cause for such discordant results. The tests employed were the phenolsulphonphthalein test and the ure aconcentration index (8). Thirteen patients were studied. They reported renal hyperfunction, by one or the other of the tests em- ployed, in nine patients and moderate depression of renal function in four. In no instance was there encountered serious impairment of renal function. In a previous study (9), we showed by means of the urine sediment count, that during the course of acute rheumatic infection, there is an abnormal increase in the excretion of formed elements in the urine, persisting for some weeks after recovery, with a final return to normal. In another study (10) we showed by means of the urea clearance test, that during the acute phase of rheumatic infection there occurred a period of renal hyperfunction, followed, in the convalescent phase by a period of renal hypofunction. The latter functional state persisted for a varying number of days and in every instance where the patient was observed over a sufficient period of time, it was followed by com- 1 Funds for this study were obtained from the Rheumatic Fever Fund of the Committee for Encouragement of Medical Research. 355
Transcript of AND · WThLLIAM GOLDRING TABLE 1-Concluded Urine Poen Redcells Whiteand Number pH Specificgravity...

STUDIES OFTHEKIDNEY IN ACUTEINFECTION
III. OBSERVATIONSWITH THE URINE SEDIMENTCOUNT(ADDIS) ANDTHE UREA CLEARANCETEST IN LOBAR PNEUMONIA1
By WILLIAM GOLDRING
(From the Department of Medicine of New York University and the Third (New YorkUniversity) Medical Division, Bellevue Hospital, New York)
(Received for publication November 29, 1930)
McIntosh and Reimann (1) reviewed some previous studies onkidney function in pneumonia. They found that of six investigators,three reported impairment of renal function (2, 3, 4), two reported theabsence of impairment (5, 6), and one (7) emphasized the occurrenceof renal hyperfunction during the course of lobar pneumonia. Itseemed to them that a further series of observations was necessary tothrow some light, if possible, on the cause for such discordant results.The tests employed were the phenolsulphonphthalein test and theure aconcentration index (8). Thirteen patients were studied. Theyreported renal hyperfunction, by one or the other of the tests em-ployed, in nine patients and moderate depression of renal function infour. In no instance was there encountered serious impairment ofrenal function.
In a previous study (9), we showed by means of the urine sedimentcount, that during the course of acute rheumatic infection, there is anabnormal increase in the excretion of formed elements in the urine,persisting for some weeks after recovery, with a final return to normal.In another study (10) we showed by means of the urea clearance test,that during the acute phase of rheumatic infection there occurred aperiod of renal hyperfunction, followed, in the convalescent phase bya period of renal hypofunction. The latter functional state persistedfor a varying number of days and in every instance where the patientwas observed over a sufficient period of time, it was followed by com-
1 Funds for this study were obtained from the Rheumatic Fever Fund of theCommittee for Encouragement of Medical Research.
355

KIDNEY STUDIES IN PNEUMONIA
TABLE IUrine sediment count in normal persons
Number
1
23456789
10111213
14
151617181920212223
24
252627282930313233343536
pHSpecific
pHgravity
5.05.05.05.55.05.05.55.05.85.56.75.65.05.85.75.55.05.55.05.05.55.55.06.55.55.05.55.85.75.06.55.05.35.05.55.55.05.5
1.0301.0401.0311.0231.0441.0201.0101.0271.0271.0271.0321.0281.0361.0301.0281.0281.0401.0181.0351.0281.0321.0261.0381.0271.0221.0271.0361.0291.0201.0321.0241.0341.0341.0341.0371.0301.0361.042
Urinevolume per
12 hours
cc.
36925947335520861677622840826918633714725923428515814517080
335343274360344186226239363287387137220120187237414210
* Centrifuge method (see reference 15).t All were of the hyalin variety.
Protein per12 hours*
mgm.
5.318.010.212.88.9
22.18.4
32.857.723.126.824.8
18.616.842.0
5.610.418.35.8
21.717.260.225.949.526.626.229.352.215.413.92.9
7.826.934.217.99.0
Red cells White andper 12 epithelialhours cells per12 hours
millions
0
0
0
0
0
0
0
0
0
0
0
0
0.0090.0100.2600.0100.0130.0200.0200.0220.0270.0280.0340.0400.0500.0900.0600.0700.0700.0710.0720.0760.0880.1270.1300.1400.1450.157
nmjilions
0.2200.0640.1180.1170.0620.0770.5800.3000.7300.6700.6000.4000.0820.7901.1000.8100.1150.2900.3600.5201.3600.0560.1800.4700.2700.7200.1900.3700.7000.2620.0970.3400.6383.4000.2800.6300.0280.131
356
Casts per12 hourst
thousands
9.20000003.802.24.10007.83.202.200
002.01.81.0002.000000.52.12.600
I I~~~~~~~~~~~~~~

WThLLIAM GOLDRING
TABLE 1-Concluded
Urine Poen Red cells White andNumber pH Specific volume per rothon per per 12 epithelial Casts pergravity 12hours 1hors* hours cells per 12 hourst12 hours
cc. mgm. millions milions thousands
37 6.5 1.026 385 22.1 0.159 0.192 038 5.5 1.027 205 10.2 0.205 039 f 6.0 1.031 312 33.7 0.160 0.810 0
t 5.0 1.030 348 30.1 0.200 0.870 3.840 5.8 1.031 256 28.7 0.210 0.320 041 5.5 1.033 384 46.0 0.300 0.830 6.442 5.5 1.028 302 6.5 0.390 1.040 043 5.0 1.030 293 42.2 0.560 2.430 044 5.0 1.033 218 22.3 0.650 1.270 4 8
45 1 5.5 1.038 355 15.3 0.931 0.047 3.9{ 5.0 1.043 280 10.0 1.530 0.024 0
Average .............................. 21.8 0.146 0.540 1.3
plete restitution of normal renal function. Since there was no reasonto believe that such findings should be peculiar to acute rheumaticinfection alone, we decided to repeat the same observations in a groupof patients with lobar pneumonia.
Adult patients were selected from a series under investigation by thepneumonia service. No patients were selected who presented signsor gave a previous history of congestive heart failure, nephritis, orhypertension. Patients who developed reaction from pneumococcusserum were likewise excluded. The urine sediment counts were per-formed according to the technique described by Addis (11). The ureaclearance test was performed according to the technique described byM6ller, McIntosh and Van Slyke (12), and McKay (13). Blood andurine urea nitrogen determinations were made by the gasometricmethod of Van Slyke (14). Both urine sediment counts and bloodurea clearances were made at intervals during the acute stage of thedisease and during convalescence.
Table 1 indicates the results of 49 urine sediment counts performedon 45 medical students in whom there was no reason to suspect ab-normality in the kidneys. The urinary protein was determined by themethod described by Shevky and Stafford (15). We felt it wasreasonable to accept as the upper limit of normal excretion for a
357

L oo 0 " w 4 ~o 0 w 0 (- " w No 4 0 0 0~o NO 0 0 0fiB. . . . . . . . . . . . . . . . .
m Cr4 CrE oO -e Os 4eq (2 ;5_ 4of eqOZ 00> CO (7% 0 0 (V O0
sm~~~~~~~t 0 C1 O- 0 C) m 0 0 qd Xbbu Ili C og8o
(R m LO I- LO0eO e )rmo eoo 0 0X
X 52 ~~40 LO C SW0s C4 C4 - ON00 0 OU0s Ufin \0 t-
OO O o O;
e OOOOO+OOOO0b~\0 0 U) 800.=NUM . . . . . . . . . . . . . . . . . . . .o~~~~~~~ C! C! LO Ocr0!0 0
N~~~~~~~~~~~~~O0NON.u
P. ~~~~~~~~~ON v0 0 eOo 0eNN+O ONo oo ssow _ o N o N N N N e cs esON 0
xI O O O O O O O ~~~m In \1 t-O 00eO O 000
358 KEIDNEY STIJDICES IN PNEUM[ONIA
aEco
R0.V-4
t-zl
Ca
-844
0m01%V-4
t-.,C11414u3.4Cd
.2
It
*t0S
as .0 tj PO c d 0 OQ.e m mmmm u VV V
d .0p p
0I
ta0~~~0 ON e
on Cdnv4

WILLIAM GOLDRING
0O-OoX O O O O N o X O N o N o 0O o n
.... . . . . . . . . . . . . . . . .(:.~~~~~~O m 0 4 eNf ) C h0S0%SO #O)
En
__ _4 H _ _~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~1s - 0% U f) o e e o 0s
V00 V-000 0 Cc00e d00V cIV 0 e4V0 00~
r\%_ 0 0 0°0\~~~~~~~~~~~~~C d ce 4
O0 Cd cQoO e WWNNNOOr_+osroooX o
Cd Od %0 0.. 0000(0D%00
0o 0 0 o 0 0 0% 0 c oV00000 C \0 0\ 0 \0 000o 0000 0o f)0%.0.0. -0 0 00 00 0\ 00 -40i'N )0
8 a oo0 8 0 oC oo oo 0 o o 0\ 8\ Mc 8C \
0
f)
14 0a,-4
o)00%m
) f) 0%4
iE)
000 n%00
. .
cs~~~~~~0 9 : Mt Ch 8 eo 0 \ u0\ 0 to O 0s_C000 0 -- 0 On
_--4 en I 00% V~~~~~~C%
o,-4if)0~0 _9C~ 00% ooo_eO4uo o __00\0C14in0 tt
in_4 00 to l4t "_1_4 N NX 4 _NN_ _tQQO- I- C14 - -
O O O OI ) i i ) -4
Of f - SOO O O-; '-4 0" ~4 0 -0 00' CN' eiVC4 00 0e c- 00 ~ 00%'4C6 ~
0Vm)"o to oMto%0%0o o o U O O OO-48005ZI 0o o OVm f) 0 0 if)ef) ,- )\0 0C)to en u) 0-- 00%u) m 0
00 0 0 0,c ;O'O 'c0 000~ c;00 ;
C1400 000 0% O00MNCf8!)88Q% ! Il
C o %0 v) \ 0% - - \0 00 00 t- 0 0-4 .00
V0%'r fee ) 000 * ee ") ~o of) r- N' + cV0
V00V L(DtoC 1 0"0o " \ - \ U00 0
i n o- ° --t o V- V- o W- V- -4 -- c" Co t oo In
~~-4'-~~~0 0 0
v-
000000-1
0C4v4000000 00000'W-
n00 t00
- --- - -- - - - -- - -- --- -( --
0 C) 00 0 0 00 f 00000 I 0z ) 0 0 i 0e 0 f)
if if i ) in to to to if i to totoD in in In In In if ito fo in If) If f) Ii ni) If t
MtC14 t 4t -40 0 t- 0 V0 if) t- eq en 00 t-' 000 C4 00 V-4t- 0 t- U) 0%ooo0 f C'1I \O e14 v-4 t-.V o 00 "0N00 0 0\4 \00 0%Kq -t0'In C%V0
0- 0n0U)
-0 00%V-0%0 -40 ~ U)00%--v
-
en
e eq -40 - eqnenNV-4v-4 d4 -1 C14 C '4 '4 '4 C4 C- '4
RV t 00 _ m rto No-00 N 0 _ en to %)
V NV c- eq eq eqeqC4 4CM4 e e
4 ,0 O co i0u2 c c .
rZ4u 0 0 W4mwwwwI.I; l; O Ecn
359

KIDNEY STU'DIES IN PNEUMONIA
44
0
0
44
ONc)~
C'NI
cd
O\
CN N
C'
C.) 0)(C.)~
ON
00'ce
ONO
c' C\
~-4
10 0
01) C.);Z. ;L
C4 C-4 ,-4C , \ C, ~a,c
0)Q: ON Cm'-+ E0 048d r
000" C0 0 ON 0 0 0 0 0N4V O C)uScn O O m m O 00 Ln m CO C O OC1 CO O
J>tf0 LOt~ C\ t1-1)\OOC
U 00 a m n X
C\ t-00 Q 004 c) O00I'
Ca in to 1- 08 'IO rN o t- oO 00 inO tC) r ,O s ,cq 0 r_C _ o \N
*,=|0 -S '-4-ClON c - C-
t-o m CQ t- QIt 1o in to 'I C mto°0 -0 0COoo0
'nczcs *.
'
C0000000000 00)5 000o OINt4sv]
LOO inoo cq oi o) oor r
os- 0 O Om C1 \ ~O 0 n m C\ cq 00 C1
Cl)~~~~~~~~~~~1
C0\ 00 00\0 000o c OOl__ c1- cq Q1 cq (1 C1 cq 14 q cqO
5O CD O O O O O O O OO0 O 0 O
bO~~~O
ooi UeO 0 OO OLO O O Oi O
0'ouOS09 00 -. 00 LO O o) O en 00 m t-
40 00
'-C-
OON O oC C\ C\ C
O 4. 4%-i -4 -4ONc,_qM C\ CD ON ON C\ C~ - .. - -en
C- 0 O N N -
Cd 06 s e t-4 .. -.
U-0) cd cd cOf) c - Z
360
I'd
C..
-1¢
d d

WILLIAM GOLDRING
period of 12 hours, 500,000 red blood cells, 1,000,000 white blood cells,and epithelial cells, 5,000 casts, and 30 mgm. of protein (16).
Table 1 in the preceeding paper, indicates the results of 34 bloodurea clearance determinations in 17 patients and medical students inwhom there was no past or present evidence of renal disease. Thenormal range varies from 75 per cent to 125 per cent of normal renalfunction.2
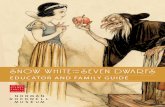
Table 2 shows the results of the urine sediment counts in 44 patientswith lobar pneumonia. By comparison with table 1, it is evident thatat some period during the precritical stage of lobar pneumonia, 38 of 44patients showed an abnormal excretion of protein and one or more ofthe formed elements. There were 40 sediment counts made when thetemperature was 101°F. or higher. Of these, protein was excreted ingreater amount than 30 mgm. per 12 hours 34 times. Casts wereexcreted in greater number than 5,000 per 12 hours 26 times. Whiteblood cells and epithelial cells were excreted in greater number than1,000,000 per 12 hours 29 times. However red blood cells were ex-creted above the normal rate of 500,000 per 12 hours only 16 times.The occurrence of microscopic hematuria in the course of lobarpneumonia appears to be of greater significance than the occurrence ofabnormal excretion in the urine of the other formed elements orprotein (16). The extent of the microscopic hematuria appears tocarry no significance as far as its interpretation goes. Of moreimportance is the time of occurrence of hematuria and its subsequentbehavior. This fact is demonstrated by two of our patients. Patient1 had a fairly normal urine sediment before and immediately after thecrisis. However, microscopic hematuria made its first appearance 12days after the crisis and on repeated tests this progressed to frankbloody urine. The almost concomitant occurrence of hypertensionand generalized edema with progressive renal functional failure in-dicated the development of acute diffuse glomerulonephritis. Partof the clinical course in this patient is shown in chart 1. The samecomplication was observed in patient 31 with the exception that thehematuria was entirely microscopic, practically negligible in degree,and deared up more rapidly. The clinical course in this patient is
2 For further details of the blood urea clearance test see reference (12).
361

KIDNEY STUDIES IN PNEUMONIA
shown in chart 2. Whether the pneumococcus or a secondarilyinvading streptococcus was responsible for the nephritis in these twopatients is not possible to say with certainty.
Of entirely different significance is the hematuria which occurred inpatients 2, 20, 30, 42, and 43. In these patients microscopic hematuriaoccurred before or about the time of the crisis, disappearing com-pletely, promptly after the crisis. With the onset of microscopic
MARCH APRI1 MAY JulePATE Is a a I na2 a I 5 7 9 t1 a 5sS a a 0 I
305 Loom F CowUCkmT DWrwI&osmtuL s104 t t CRtl$3 3/26
TEMPt. I o's 4M-II ATUtIA +4/loFr 101to PEP.RTUSWON4/lit
too rnPZA 4/i*9
WUo0o~ooo~Ooo |t I9 t tBy
"EIWT WqPOQoOOCOUNT 240 ° r
EDEMA 3t2+
IBLOOD tooPREM5URE OPKSSURL ~~S140l00
70oMAXIMUM 1.0LW
CONC. 3.03PowtR I.010
1.007
40(Zh*/ ) 20I
CHART 1. Patient A, Number 1. White, male, aged 39. Hematuria wasfirst noted 14 days after the crisis. Then followed a rise in blood pressure, gen-eralized edema including the face and impairment of renal function. Hematuriaand impaired renal function were present at a subsequent examination, 2 monthsafter discharge.
hematuria during the acute phase of the disease, its prompt disappear-ance and the absence of systemic manifestation, hypertension, andedema, these cases must be interpreted as instances of focal glomeruli-tis and are of no prognostic significance. In patient 44 the occurrenceof hematuria, for the first time, in convalescence is highly suggestiveof the onset of diffuse glomerulonephritis, but the absence of hyper-tension or edema and the lack of renal function study, makes it
362

WILLIAM GOLDRING 363
impossible to be certain of any more than a focal glomerular lesion.The appearance or disappearance of microscopic hematuria apparentlybears no relationship to the excretion rate of the other formed elementsor protein. These appear to be of different pathogenesis as well as ofdifferent significance as far as our observations go. Apparently amore severe renal lesion is necessary to permit the excretion of red
APRIL MAYDATE 3457$90 12 4 K o D2 a 1234567890It 14 16X X a 2
101I 04 I|tLobAlt P14NOMIATEMP. 103 COMPLICATR* t | "u|X ommmA-mDwra
99 2t . *. ..
BLOOD 130
9070 7 ~
WEMATIA I,000.000
COUNT 04.o
UEMA 3+2+
0WIAMIMUM 1.035
GhONG. LOZOPOWER 1.015
1.0103.005
P.S.P. T0
so30
CHART 2. Patient Me, Number 31. While male, aged 31. Generalizededema involving the face was first noted 13 days after the crisis. Distinct hema-tuna was not present one week after the onset. The blood pressure did not rise,but renal function was temporarily impaired. Patient left the hospital apparentlywell.
blood cells. This fact had been previously observed in studying theurine sediment in congestive heart failure (16).
In table 3 are shown the results of the blood urea clearance testduring the acute and convalescent stages of lobar pneumonia. Ourresults confirm the findings of McIntosh and Reimann (1). Of 13patients studied, 9 showed a period of renal hyperfunction (increasedurea excreting activity) during the acute stage, 2 showed a period ofrenal hypofunction (decreased urea excreting activity) during theacute stage, and 2 showed no change from normal function. Of the 9

KIDNEY STUDIES IN PNEUMONIA
0ONf4-4-~~C
t-Cl4
4r.)u:
(n*En
CN
.4_
04-)0-e::
C)-ela .c *;b ¢nW. p :
_N 4'
'-4 44
cd >
. -e44)
Cd C'45 re en e 4 C'4 f Q\ OC\ 00 00 0; * n 0A.E.o.t.s .s.s .X.s . .
C) 0sCOlO\O1 0 00 0 0 0 0 C\ ONON CO O\ 00Cd t- 00 -d4 en - - t- O - in C- 0- - - i- \ -4
4 u S ON 00X 4 \OX )ONOOO
> lt~~~~~~~~~~~~~C o O O _) C) _4 C) _ _ __
-f) C)
\oO r_ t- \f) -) o t) o
ON \ - C'4 e) - 4 en nO t O
\O4 OOO - O\-
4-4\~ -,4 -4 c4 - ~-4 -q L-4 U--4
44r in) if in 4- 00 in\'fnU) f) 14 in
O '. ONi L 0 iC\ 4 -1 0 - -1\ '-C4 '- O - '-4\ -4It C\ l-dd C O O OONmmmOOOOO ON
Q , .
0 10
.. -- - o q U-) _q oq U- r) ce in m en ot o 0s in en cr U- ono
; O*bh000rNeOd'C) 0000qe 000 0 Cs-0rn o c) __) en en _) D0 C
2 \S\ C\ c C ONNCO\ ONN\ C\_-4 '
nOm4O °
O- o4 e \6 _{' Jr;_1 ~(:N-t__ 4 - _1 -{
E ' ~ ~ ~ ~~~~~t4 if)~~~~~~e -.O in 0
0 c
z N ^ _ ^ _ _ X ms N o ~ N n * _^ m^~i_ o
4) u c
u p
364
.44
,-00z
Cd
.11
0Inv
P4

WILLIAM GOLDRING
0~~~~~~0
00 0 0 \0V C1 co0V0 \ 00 0 144in 0 \ V 00V 0 00 00 0\
0 O~ 0 01 C
:-4 - 4) - -
+-+~~~~~~~~~~~~~~~~~N
u) oo oo ~~o \0 w t o oo eqoo ino
00 0)O \U' 0000 00 C4'40f006 ~0V
-----v- -0r W)\ C- tJ4 0m 00 000
000- 40e4000000
00 C m0%0% 04! m(4) \040%
C4~~~~~~~C4if14 004) 0\ o U')2 4 \ m \
Ca
oo00%CS 1")i t'to) ~f0\00 t- inf Wf) e.0\ )
0%14>
000o 'o o o ooo o Co r o eO O o d
Ce0%s oe r 4)
C14 V- V-4 W-U) oo oreu ).
'eC)
01 C, obo - ooo
C) e 0 0s 0 U) 0s U) + 00w 00 m SC'
CdC
* 4
> ~~W
365

36KIDNEY STUDIES IN PNEUMONIA
patients who showed hyperfunction, 3 showed a depression of renalfunction following the crisis. With 4 exceptions in the entire group,all remained normal or returned to normal after a period of depressedrenal function. Of these four exceptions, in only one (patient 1)did we have sufficient correlated data to establish the diagnosis ofdiffuse glomerulonephritis. This same likelihood is quite possible inthe other three instances (patients 3, 11, 12). Return of normalfunction occurred in from 3 to 7 days. Patient 13 is of interest sinceduring the acute stage of the disease he developed a blood urea clear-ance of 8.35 per cent of normal renal function and a blood urea nitro-gen of 80.5 mgm. per 100 cc. of blood. Seven days later, the resultsof both tests were normal and he made an uneventful recovery.
CONCLUSIONS
1. Observations with the urine sediment count, have been made in44 adults with lobar pneumonia. Deviations from normal sedimentfindings have been presented and discussed. The occurrence of micro-scopic hematuria appeared to be of greater prognostic significance thanthe appearance of the other formed elements or protein in the urine.
2. Observations with the blood urea clearance test were made in 13patients with lobar pneumonia. Renal hyperfunction (increased ureaexcreting activity) was the rule during the acute stage of the disease.Slight to marked depression of renal function (decreased urea excret-ing activity) occurred during both the acute and convalescent stages.
3. In two patients of this series there was sufficient correlated clini-cal data, to be certain of a complicating acute diffuse glomerulo-nephritis.
BIBLIOGRAPHY
1. McIntosh, J. F., and Reimann, H. A., J. Clin. Invest., 1926, iii, 123. KidneyFunction in Pneumonia.
2. Tileston, W., and Comfort, C. W. Jr., Arch. Int. Med., 1914, xiv, 620. TheTotal Nonprotein Nitrogen and the Urea of the Blood in Health and inDisease as Estimated-by Folin's Methods.
3. Schwartz, H., and McGill, C., Arch. Int. Med., 1916, xvii, 42. Blood UreaDeterminations in 211 Cases.
4. Bookman, A., Arch. Int. Med., 1917, xx, 112. A Study of Renal Function inPatients Convalescing from Acute Fevers.
366

WILLIA GOLDRING
5. Rackemann, F., Longscope, W. T., and Peters, J. P., Arch. Int. Med., 1916,xviii, 496. The Excretion of Chlorides and Water and the Renal Functionin Serum Disease.
6. Frothingham, C., Arch. Int. Med., 1918, xxii, 74. Studies on Renal FunctionDuring and Immediately Following Someof the Acute Infectious Diseases.
7. Lewis, D. S., Arch. Int. Med., 1917, xix, 1. The Clinical Value of Ambard'sCoefficient of Urea Excretion.
8. Van Slyke, D. D., Linder, G. C., Hiller, A., Leiter, L., and McIntosh, J. F.,Jour. Clin. Invest., 1926, ii, 255. The Excretion of Ammonia and TitratableAcid in Nephritis.
9. Goldring, W.,;and Wyckoff, J., J. Clin. Invest., 1930, viii, 569. Studies of theKidney in Acute Infection. I. Observations with the Urine SedimentCount (Addis) in Acute Rheumatic Infection.
10. Goldring, W., J. Clin. Invest., 1931, x, 345. Studies of the Kidney in AcuteInfection. II. Observations with the Urea Clearance Test in AcuteRheumatic Infection.
111.Addis, T., J. Am. Med. Assoc., 1925, lxxxv, 163. A Clinical Classification ofBright's Disease.
12. Moller, E., McIntosh, J. F., and Van Slyke, D. D., J. Clin. Invest., 1928,vi, 427. Studies of Urea Excretion. II. Relationship between UrineVolume and the Rate of Urea Excretion by Normal Adults.
13. McKay, E. M., J. Clin. Invest., 1929, vi, 505. Studies of Urea Excretion.V. The Diurnal Variation of Urea Excretion in Normal Individuals andPatients with Bright's Disease.
14. Van Slyke, D. D., J. Biol. Chem., 1927, lxxiii, 695. Determination of Urea byGasometric Measurement of the Carbon Dioxide Formed by the Action ofUrease.
15. Shevky, M. C., and Stafford, D. D., Arch. Int. Med., 1923, xxxii, 222. AClinical Method for the Estimation of Protein in Urine and other BodyFluids.
16. Goldring, W., In press. Observations on the Clinical Application of the UrineSediment Count (Addis).
367

![Metabolism of benzo[a]pyrene humanmammary epithelialcells ... · broblastswereexposedto4.0FMBaPin thestudies ofDNAad-duct formation. Separation by high-pressure liquid chromatog-raphyofadductsbetween(±)-7,8-dihydroxy-9,10-epoxy-7,8,9,10-tetrahydrobenzo[a]pyrene](https://static.fdocuments.in/doc/165x107/5c7ac3f109d3f2f93e8c83f3/metabolism-of-benzoapyrene-humanmammary-epithelialcells-broblastswereexposedto40fmbapin.jpg)