ANCILLARY PROCEDURES
50
ANCILLARY PROCEDURES
-
Upload
ashely-mullins -
Category
Documents
-
view
33 -
download
2
description
ANCILLARY PROCEDURES. Done in the patient. CBC Na, K Creatinine SGOT, SGPT 12-L ECG. CBC. Complete Blood Count. broad screening test to check for such disorders as anemia, infection, and many other diseases Red blood cell (RBC) count - PowerPoint PPT Presentation
Transcript of ANCILLARY PROCEDURES

ANCILLARY PROCEDURES

Done in the patient
• CBC• Na, K• Creatinine• SGOT, SGPT• 12-L ECG

CBC

Complete Blood Count– broad screening test to check for such disorders as anemia,
infection, and many other diseases
• Red blood cell (RBC) count• count of the actual number of red blood cells per volume
of blood
• Hemoglobin • measures the amount of oxygen-carrying protein in the
blood
• Hematocrit • measures the percentage of red blood cells in a given
volume of whole blood

Complete Blood Count
• Mean corpuscular volume (MCV)– measurement of the average size of RBCs
• Elevated: macrocytic – ex.: vitamin B12 deficiency
• Decreased: microcytic – ex.: iron deficiency anemia or thalassemias
• Mean corpuscular hemoglobin (MCH)– average amount of O2-carrying hemoglobin inside a
red blood cell• Macrocytic RBCs have a higher MCH, while microcytic red
cells have a lower value

Complete Blood Count
• Mean corpuscular hemoglobin concentration (MCHC) – calculation of the average concentration of
hemoglobin inside a red cell• Decreased: hemoglobin is abnormally diluted inside the
red cells– ex.: iron deficiency anemia and thalassemia.
• Increased: (hyperchromia); hemoglobin is abnormally concentrated inside the red cells– ex.: burn patients and hereditary spherocytosis

Complete Blood Count
• Red cell distribution width (RDW) – calculation of the variation in the size of your RBCs
• Platelet count – number of platelets in a given volume of blood

Complete Blood Count11/23/09 11/28/09 Unit NV
Hgb 96 118 g/L 120-170
RBC 2.93 3.73 X10^12/L 4.0-6.0
Hct 0.28 0.35 0.37-0.54
MCV 94.3 94.60 U^3 87 + -5
MCH 32.6 31.50 pg 29 + -2
MCHC 34.6 33.30 g/dL 34 + -2
RDW 13.40 14.10 11.6 – 14.6
Platelet 481 830 X10^9/L 150-450

Anemia
• Low RBC, Hgb, Hct• Due to insufficient production of EPO by the
diseased kidneys (CKD stage 3)

Thrombocytosis
• Occurs as an acute phase response to infection

Complete Blood Count
• White blood cell (WBC) count – count of the actual number of white blood cells
per volume of blood
• White blood cell differential– looks at the types of white blood cells present– five different types of white blood cells:
neutrophils, lymphocytes, monocytes, eosinophils, and basophils

Complete Blood Count
11/23/09 11/28/09 Unit NVWBC 17.70 15.39 X10^9/L 4.5-10.0Diff ctNeutrophils 0.75 0.75 0.50-0.70 Segmenters 0.74 0.72 0.50-0.70 Bands 0.01 0.01 0-0.05Metamyelocytes 0.01Lymphocytes 0.24 0.23 0.20-0.40Monocytes 0.00-0.07Eosinophils 0.01 0.02 0.00-0.05BasophilsMyelocytes

Leukocytosis
• With predominance of neutrophils connotes active bacterial infection

BLOOD CHEMISTRY
Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• AST / ALT– Test associated with the cellular integrity of the
Liver, indicates hepatocellular injury and necrosis
Enzyme AKA Increase in:
Aspartate transaminase (AST)
Serum Glutamic Oxaloacetic Transaminase (SGOT) or aspartate aminotransferase (ASAT)
•acute liver damage •cardiac damage•skeletal damage•*not specific for liver damage
Alanine transaminase (ALT)
Serum Glutamic Pyruvate Transaminase (SGPT) or Alanine aminotransferase (ALAT)
•acute liver damage•viral hepatitis or •paracetamol(acetaminophen) overdose

Biochemical Blood Tests
• AST / ALT
– Active liver insult probably drug induced (aspirin).
11/23/09 11/28/09 Unit N.V.
SGPT-ALT 37.8 U/L 0-31
SGOT-AST 55.3 U/L 0-38

Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• Creatinine– used to measure GFR; indicator of renal functionIncrease in• Acute tubular necrosis, Dehydration, Diabetic
nephropathy, Eclampsia, Glomerulonephritis, Kidney failure, Muscular dystrophy, Preeclampsia, Pyelonephritis, reduced kidney blood flow (shock, congestive heart failure), Rhabdomyolysis, Urinary tract obstruction
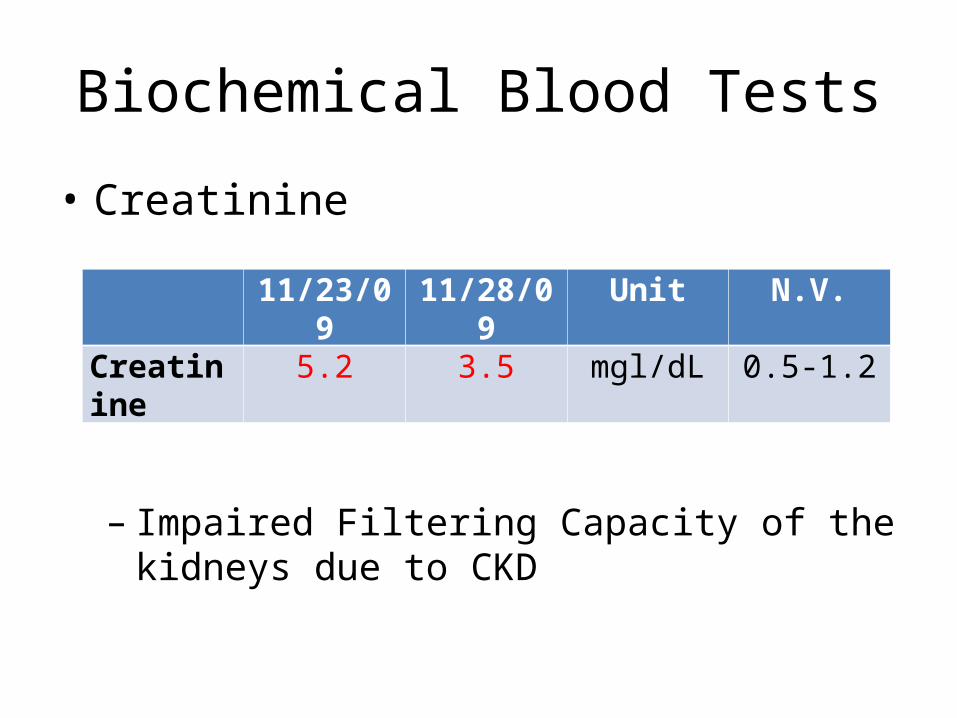
Biochemical Blood Tests
• Creatinine
– Impaired Filtering Capacity of the kidneys due to CKD
11/23/09 11/28/09 Unit N.V.
Creatinine 5.2 3.5 mgl/dL 0.5-1.2

Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• Sodium– major extracellular cation– maintains the proper acid-base equilibrium for the
proper osmotic balance– osmotic regulation of extra-cellular fluid balance
and acid balance, as well as renal, cardiac and adrenal functions

Biochemical Blood Tests• SodiumIncreased in:
– Water deficit– Water deficit exceeding
sodium deficit – Excessive intake of sodium – Adrenal Cortex Hyper-
function– Diabetes– Pyloric Obstruction – Congestive Heart Failure
– Insufficient Anti-Diuretic Hormone production by the hypothalamic-pituitary complex
– Alcohol intake reduces the sodium lost in the urine

Biochemical Blood Tests
• SodiumDecreased in:
– Pyloric Spasm– Hyperglycemia and Diabetes
mellitus lo– Excess Perspiration leads to
loss in the sweat– Adrenal Cortex Hypo-function– Diarrhea and metabolic
alkalosis
– Excess progesterone blocks the action of aldosterone but insufficient progesterone results in greater loss of sodium in the urine
– Renal Dysfunction– Syndrome of Inappropriate
Anti-Diuretic Hormone

Hyponatremia
• Sodium
• Most probably due to impaired kidney function
11/23/09 Unit N.V.Sodium 130 mmol/L 137-147
Biochemical Blood Tests
• Liver Function test– AST/ ALT
• Kidney Profile test– Creatinine– Electrolytes
• ( Na, K, Ca, PO)
– BUN– Uric Acid
• Lipid Profile test– TG– Total Cholesterol– LDL, HDL, VLDL

Biochemical Blood Tests
• Potassium– major intracellular cation– essential to heart and kidney
function as well as to the maintenance of blood and urine pH
– increased in:• Renal Dysfunction• Adrenal Cortex under function • Catabolic/Dysaerobic State• Metabolic Acidosis• Respiratory Dysfunction • Bradycardia• Massive Tissue Destruction• Diabetes without adequate
insulin

Biochemical Blood Tests
• PotassiumDecreased in:
• Diarrhea and/or vomiting• Adrenal Cortex over
function• Several Types of Anemia• Metabolic Alkalosis• Diuretic Use• Familial Periodic Paralysis
• Diets High in Refined Foods due to lack of potassium in the diet
• Hypertension• Insulin use• Anabolic/Anaerobic
States

Hyperkalemia
• Potassium
• Most probably due to impaired kidney function
11/23/09 Unit N.V.
Potassium 5.4 mmol/L 3.8 - 5

OTHER ANCILLARY PROCEDURE

ECG
• Sinus rhythm• Left ventricular hypertrophy– pathological reaction to cardiovascular disease, or high
blood pressure– increase afterload that the heart has to contract against– causes of increased afterload that can cause LVH include
aortic stenosis, aortic insufficiency, and hypertension
• Peak T-waves– Due to hyperkalemia

Requested but not done• iCA• iPO4• BUN• Uric acid• Lipid profile• ABG• Ultrasound of KUBP• Sputum GS, proceed to C/S if PMN >25/lpf and epithelial
cells <10/lpf• Sputum AFB
Biochemical Blood Tests
• Ionized Calcium– is calcium that is freely flowing in blood and not bound to
proteins – free calcium– test to monitor patients having kidney and parathyroid
problem

Biochemical Blood Tests
Increased in:• Hyperparathyroidism, • immobilization, • idiopathic hypocalciuria, • metastatic bone tumor, • milk-alkali syndrome, • multiple myeloma, • paget's disease, • sarcoidosis, • too much vitamin D, • use of thiazide diuretics
Decreased in:• Hypoparathyroidism, • malabsorption, • osteomalacia, • pancreatitis, • renal failure • rickets, • vitamin D deficiency

Biochemical Blood Tests
• Ionized Phosphate– charged particle (ion) that contains the mineral
phosphorus– Helps to build and repair bones and teeth, help nerves
function, and make muscles contract– amount of phosphate in the blood affects the level of
calcium in the blood– Used to monitor kidney and bone disease

Biochemical Blood Tests
Increased in:• Kidney disease • Hypoparathyroidism• acromegaly• Too much vitamin D in the body• decrease in magnesium levels. • Pregnancy
Decreased in: • Hyperparathyroidism• Osteomalacia• Lack and malbsorption of vitamin D• severe burns • kidney or liver diseases. • Severe malnutrition or starvation. • Alcohol dependence • High calcium levels

Relationship of Blood Ca and PO
Biochemical Blood Tests
• BUN – measure of the amount of nitrogen in the blood in the
form of urea, and a measurement of renal function– Urea is a substance secreted by the liver, and removed
from the blood by the kidneys
– Normal value: 10–20 mg/dL or 3.6–7.1 mmol/L

Biochemical Blood Tests
• BUN– Increased in:
• kidney injury or disease• Congestive heart failure • Excessive protein levels in
the gastrointestinal tract • Gastrointestinal bleeding • Hypovolemia• Heart attack • Shock • Urinary tract obstruction
– Decreased in:– Liver failure– Low protein diet– Malnutrition – Over-hydration

Biochemical Blood Tests
• BUA– Most of the uric acid is filtered out by the kidneys and
passes out of the body in urine. – if too much uric acid is being produced or if the kidneys
are not able to remove it from the blood normally, the level of uric acid in the blood increases
– Normal value: 3.4-7.0 mg/dL (men)

Biochemical Blood Tests
• BUA– Increased in:
• Kidney disease or kidney damage• leukemia, lymphoma, and multiple myeloma or cancer
treatments, hemolytic anemia, sickle cell anemia, or heart failure• liver disease (cirrhosis), obesity• Starvation, malnutrition • Medicines: diuretics, vitamin C, lower doses of aspirin (75 to 100
mg daily), niacin, warfarin, cyclosporine, levodopa, tacrolimus, and some medicines used to treat leukemia, lymphoma, or tuberculosis
• Foods that are very high in purines: organ meats

Biochemical Blood Tests
• BUA– Decreased in:
• Severe liver disease, Wilson's disease, or some types of cancer• Syndrome of inappropriate antidiuretic hormone (SIADH), a
condition that causes large amounts of fluid to build up in the body
• Not eating enough protein • Sulfinpyrazone, large amounts of aspirin (1,500 mg or more daily),
probenecid and allopurinol

Lipid Profile
• Assess risk of heart disease• Includes:– Total cholesterol: <200 mg/dL– Triglycerides: <150 mg/dL– LDL: <100 mg/dL– HDL: >60 mg/dL

Arterial Blood Gas
• used to determine the pH of the blood, the partial pressure of carbon dioxide and oxygen, and the bicarbonate level

Arterial Blood Gas
• Expected result:– Metabolic acidosis
Normal Value Expected results
pH 7.35 – 7.45
pCO2 35 – 45 mmHg
HCO3 22-26 meq/L

Ultrasound of KUBP
• used to assess the size, location, and shape of the kidneys and related structures, such as the ureters bladder, and prostate
• can detect cysts, tumors, abscesses, obstructions, fluid collection, and infection within or around the kidneys.
• can also detect calculi (stones) of the kidneys and ureters

Gram's Stain and Culture of Sputum
• Help to identify certain pathogens by their characteristic appearance
• To be adequate for culture, a sputum sample must have: – >25 neutrophils and <10 squamous epithelial cells
per low-power field
• Sensitivity and specificity of the sputum Gram's stain and culture are highly variable

Sputum AFB
• used to determine an active Mycobacterium tuberculosis infection or an infection due to another member of the Mycobacterium family, or TB-like symptoms due to another cause
• Done in patients having history and symptoms that suggest pulmonary TB such as: – Positive exposure– chronic cough (at least 2weeks), significant weight loss,
low grade fever
• Positive result: presence of ACID FAST BACILLI