Anatomy of a Reading Response. paper format heading title page # 1” margin double spaced.

Purdue UniversityWeldon School of Biomedical Engineering
BME 256/295: Human Physiology and Physiological Modeling in Health and Disease
Spring 2011
Instructors:Charles F. Babbs, MD, PhD; W. A. Tacker, MD, PhDG-170A; G-170C, Lynn Hall496-2661; [email protected], [email protected] Office Hours: by arrangement, please E-mail us
Teaching assistant: Alan Truong. Email: [email protected] office hours: by appointment, please email.
Secretary: Cindy Ferguson, [email protected] meeting time: Mondays, Wednesdays, Fridays 2:30 p.m. – 3:20 p.m.
Meeting Place: BMED 1001
Objectives: (1) To introduce students to the physiology and medicine underlying practical problems in biomedical engineering, especially with respect to medical device development(2) To introduce students to the process of mathematical modeling of human anatomy and physiology, including technical description of objectives, methods, results, and conclusions from modeling exercises(3) To put more biology and medicine into biomedical engineering.
Focus: heart, lungs, blood vessels, and kidneys, and common afflictions thereof. (Other organ systems, especially neuro-musculo-skeletal systems are dealt with elsewhere in the BME curriculum, including BME 204, Biomechanics of Hard and Soft Tissues, BME 301, Bioelectricity and the Mammalian Nervous System, BME 528 Measurement and Stimulation of the Nervous System, and BME 540 Biomechanics.)
Prerequisites: Second semester sophomore standing, pre-calculus, calculus, elementary computer programming, introductory college biology
Background of instructors: Charles F. Babbs, MD, PhD and Willis A. ("Tack") Tacker, MD, PhD, combined > 60 years of teaching, research and publications experience in medicine, pharmacology, applied physiology and biomedical engineering.
1

Course climate: "Show up on time. Do your best." – Gene Keady(If you prefer to sleep or read newspapers, do not come to class.)
Respectful feedback is welcomed.
Course requirements and assignments: Lectures and whole class discussion Reading and Web study Problem sets (due 1 week prior to exams, grade penalty for lateness or sloppiness) Exams (3 unit examinations plus one final)
Textbooks: Boron WF and Boulpaep EL, Medical Physiology, Elsevier Sanders, 2005.National Library of Medicine medical encyclopedia and dictionary online:www.nlm.nih.gov/medlineplus/encyclopediawww.nlm.nih.gov/medlineplus/mplusdictionary
Reading assignments: Please see separate sheet organized by lecture topics.
Problem set work groups: Modified random assignment of group members (see handouts) Practice "teaming" Solutions, not answers required (see style guide) All group members must sign off on solutions Single group grade for all members on problem sets Group studying for exams is encouraged
Group dynamics: try hard to contribute equally and to resolve differences. Talk with staff if major problems arise. Encourage more quiet or shy members to contribute.
Happiness is keeping up and not procrastinating or cramming.
Grade composition (subject to change with notice): 3 closed-book exams, 50% Problem sets, 30% Comprehensive final closed-book exam 20%
2

Grading scale:90-100% A80-90% B70-80% C60-70% D0--60% F
Make-up exams:Given at the discretion of the instructor; format may be different from regular exams. Advance notice, when possible, is highly recommended. Students must adhere to Purdue policy as outlined: http://www.purdue.edu/usp/acad_policies/attendance.shtml
Policy on academic honesty:The commitment of the acts of cheating, lying, stealing, and deceit in any of their diverse forms (such as the use of ghostwritten papers, the use of substitutes for taking examinations, the use of illegal cribs, plagiarism, and copying during examinations) is dishonest and must not be tolerated. Moreover, knowingly to aid and abet, directly or indirectly, other parties in committing dishonest acts is in itself dishonest.
In this course, problem sets = group work, but exams = individual work. Students are encouraged to share freely and extensively with each other EXCEPT FOR the written exams. A single event of cheating on an exam in this course will result in a grade of zero for that exam. A second event of cheating will result in disciplinary action by the School and the University. This action may range from academic probation to expulsion from Purdue with encumbered records (meaning that your credit at Purdue is not transferable to any other institution, ever).
Emergency statement:In the event of a major campus emergency, course requirements, deadlines and grading percentages are subject to changes that may be necessitated by a revised semester calendar or other circumstances.
Adaptive programs statement:Students with disabilities must be registered with Adaptive Programs in the Office of the Dean of Students before classroom accommodations can be provided. If you are eligible for academic accommodations because you have a documented disability that will impact your work in this class, please schedule an appointment with the instructor as soon as possible to discuss your needs.
3

Tentative calendar for BME 256/295, Spring 2011
Date Instructor TopicMon Jan 10 Babbs &
Staff Course introduction and overview of body systems
Wed Jan 12 Tacker Vascular anatomy and compositionFri Jan 14 Tacker Vascular anatomy and compositionMon Jan 17 MLKWed Jan 19 Babbs AtherosclerosisFri Jan 21 Babbs Atherosclerosis and stentsMon Jan 24 Babbs Hemostasis and anticoagulantsWed Jan 26 Babbs Hemostasis and anticoagulantsFri Jan 28 Babbs Renovascular disease and stents Mon Jan 31 Babbs Renovascular disease
(problem set #1 due: An AIBPCWed Feb 2 Babbs Restenosis after angioplastyFri Feb 4 Babbs Restenosis after angioplastyMon Feb 7 Staff Exam 1Wed Feb 9 Tacker Aneurysms Fri Feb 11 Tacker Aneurysms and endovascular devicesMon Feb 14 Babbs The heart as a pumpWed Feb 16 Babbs The heart as a pumpFri Feb 18 Babbs Congestive heart failureMon Feb 21 Tacker Myocardial ischemia and infarction
Wed Feb 23 Tacker Myocardial ischemia and infarctionFri Feb 25 Tacker Peripheral vascular disease Mon Feb 28 Tacker Peripheral vascular disease and devices
(problem set #2 due: Neonatal CPR)Wed Mar 2 Babbs Adult onset diabetes pathophysiologyFri Mar 4 Babbs Adult onset diabetes treatment optionsMon Mar 7 Staff Exam 2Wed Mar 9 Babbs Stroke IFri Mar 11 Babbs Stroke interventions Mon Mar 14 Spring breakWed Mar 16 Spring breakFri Mar 18 Spring breakMon Mar 21 Babbs Carotid artery disease and distal protection devicesWed Mar 23 Tacker Aortic dissectionsFri Mar 25 Tacker Skin, burns, barriers, and graftsMon Mar 28 Hiles Tissue engineering
4

Wed Mar 30 Tacker Dental and GIFri Apr 1 Tacker Benign prostatic hyperplasia: diagnosis and imagingMon Apr 4 Tacker Benign prostatic hyperplasia: therapeutic systems
(problem set #3 due: Exercise responsive pacemaker)Wed Apr 6 Babbs Pulmonary physiology Part IFri April 8 Babbs Pulmonary physiology Part II Mon April 11 Babbs Exam 3Wed Apr 13 Babbs Kidney and urinary tract Part IFri Apr 15 Babbs Kidney and urinary tract Part IIMon Apr 18 Babbs Kidney and urinary tract pathology Part IIIWed Apr 20 Babbs Renal failure and dialysis Fri Apr 22 Babbs Shock IMon Apr 25 Babbs Shock IIWed Apr 27 Babbs Ventricular assist devicesFri Apr 29 Babbs Ventricular assist devices
(problem set #4 due: Deep brain stimulation)TBA Staff Final exam 1:00 – 3:00 p.m. MJIS 1001
5

BME 256/295 reading and Web study assignments
Course introduction and overview of body systemsSyllabusBoron Chapter 1, "Foundations of Physiology"Boron Chapter 22, "Regulation of Arterial Pressure and Cardiac Output", pp 534-545 (2nd Edition, Chapter 23, pp 554-576)
Vascular anatomy and compositionBoron Chapter 17, "Organization of the Cardiovascular system", pp. 423-446(2nd Edition, Chapter 18, pp 429-447)Boron Chapter 18, Arteries and Veins"(2nd Edition, Chapter 19)
Atherosclerosishttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click atherosclerosishttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click coronary heart disease
Hemostasis and anticoagulantshttp://themedicalbiochemistrypage.org/blood-coagulation.html
Peripheral arterial diseasehttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click atherosclerosis of the extremities
Restenosishttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click angioplasty
Aneurysmshttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click aortic aneurysms
The heart as a pumpBoron Chapter 20, "Cardiac Electrophysiology and the ECG", pp. 483-507(2nd Edition, Chapter 21, pp 504-528)Boron Chapter 21, "The Heart as a Pump", pp. 508-526(2nd Edition, Chapter 22, pp 529-544)
Congestive heart failureBoron Chapter 21, "The Heart as a Pump", pp. 527-533(2nd Edition, Chapter 22, pp 544-553)Boron Chapter 30, "Ventilation and Perfusion of the Lungs", pp. 700-711 (Section on matching ventilation and perfusion)(2nd Edition, Chapter 31, pp 714-724)
http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click left-sided heart failure, right-sided heart failure
6

Myocardial infarctionshttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click heart attack
Adult onset diabeteshttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click diabetes, diabetic neuropathy, atherosclerosis
Renovascular diseaseBoron Chapter 39, pp. 866-867, and Chapter 49, pp. 1059-1061 (sections on rennin-angiotensin, aldosterone system) (2nd Edition, Chapter 40, pp 870-874)http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click renal artery stenosis
Strokehttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click stroke
Carotid artery diseasehttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click carotid artery surgeryhttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click carotid duplex
Aortic dissectionshttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click aortic dissection
ShockBoron Chapter 28, "Transport of Oxygen and Carbon Dioxide in the Blood"(2nd Edition, Chapter 29)http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click hypovolemic shock, cardiogenic shock, septic shock
Ventricular assist deviceshttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click aortic cardiogenic shockhttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click ventricular assist device
Respiratory systemBoron Chapter 25, "Organization of the Respiratory System" (2nd Edition, Chapter 26)Boron Chapter 26, "Mechanics of Respiration" (2nd Edition, Chapter 27)
Kidney and urinary tractBoron Chapter 32, "Organization of the Urinary System" (2nd Edition, Chapter 33)
Physiology of chronic renal failureBoron, Chapter 33, "Glomerular Filtration and Renal Blood Flow" (2nd Ed., Chapter 34)http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click chronic renal failure
Benign prostatic hyperplasiahttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click prostate diseases
7

http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click aortic enlarged prostate
Prostate cancer http://www.nlm.nih.gov/medlineplus/encyclopedia.html, click prostate cancerhttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click PSA
Renal stone diseasehttp://www.nlm.nih.gov/medlineplus/encyclopedia.html, click kidney stones
8

Instructions for BME 256/295 Problem setsan introduction to mathematical modeling
and analysis of biological systems
Group process
Perhaps more than in any other engineering discipline, biomedical engineering is done in teams. You are not condemned to live your life in a cubicle. We want you to practice "teaming". We strongly encourage the group to work together in solving the problems in a "colloquial learning" style, which works like this. The group meets in a small group room, preferably with a dry erase board or chalkboard and an Internet connection. One or two group members serve as official note takers. Students take turns at the board working the steps or sub-parts of the problems. Respectful suggestions, arguments and discussions from other group members should be part of the process, as each step of the problem is solved. Everyone learns in the process, and it is more fun than solo studying. Some items, such as the numerical value of a constant, can be deferred to avoid bogging down. Work in algebra most of the time, defer use of exact numerical values until the problem is solved algebraically and it is time to do a specific example. Write a Matlab script to evaluate the solution for an interesting family of specific cases, including frequently a sensitivity analysis.
Once the whole group has solved the problems, members can take turns preparing a formal written report. When the entire problem set is completed and agreed on, it can be given to the TA.
Goal of problem set reports
Your objective is to write a detailed statement and solution of each problem in the style of a mathematics textbook or research paper, combining English prose and mathematical notation in complete sentences. Consider each problem write-up to be a mini-technical report on a topic of interest, such as that produced by a working biomedical engineer for a medical device company. A detailed style guide is attached, showing the recommended organization and level of detail for problem set write-ups.
For each problem include the problem statement or objective, a sketch of the relevant model or anatomy, definitions of all variables, the logical and algebraic steps for solving the problem, general algebraic solution, a specific test solution, optional Matlab code for numerical solution of multiple cases, graphs or tables including exact numerical values for selected cases, and a discussion of the significance of the results, especially whether they meet reasonable expectations for biologically reasonable values, and appendices when needed (e.g. Matlab code). What matters is the validity of the assumptions, the approach, the logic, model geometries, variable definitions, inputs, and the numerical methods upon which the results depend. The "answer" alone, right or wrong, is not
9

sufficient. Numerical results must be in correct units. You have permission to paraphrase the problem statements and copy the drawings therein.
Getting help on problem sets
Groups are allowed to get advice and input on problem sets from the Web, faculty, other students, provided they acknowledge the sources in their reports. Acknowledgements may be textual (e.g. "According to Professor Otto, …" or "According to www.DiabetesResearch.com, …) or they can be footnoted citations of journal articles or books (e.g. DiFiore, M.S.H., Atlas of Human Histology, 5th Edition, Lea and Febiger, Philadelphia, 1981.) If groups take bad advice without checking it, they will not get credit.
Problem set grades
Student groups of 4 are responsible to turn in a joint report for problem sets. A cover sheet should include a title, date, names and signatures of all group members. Signatures indicate important and substantial participation by and agreement with the content and the accuracy of the results. Group members share credit equally. Honest, respectful discussion can help ensure that all contribute about equally to the final results. With multiple minds at work, the probability of obtaining a valid solution and full credit should approach 100 percent.
Problem set workload
Problems are designed to require about one hour of group discussion to solve and about three hours of individual effort to write up professionally. With a maximum of 4 problems per set this translates to 4 hours of group discussion and 4 hours of individual writing and one hour of individual miscellaneous work. For a group of 4 students, assuming each student writes up one problem, this translates to 9 hours total work per problem set. Problem sets come out every 3 weeks. On average problem sets should take 3 hours per week to prepare. A good plan that helps with personal growth toward professionalism is to meet weekly to work on problem sets and to avoid procrastination.
10

Problem set tips
1. Note on unit conversion (adapted from The Math Forum at Drexel):
Converting units of measurement is a simple as multiplying by one. For example, to convert 50 minutes to hours, do the following:
50 minutes 1 hour----------- x ---------- = 0.83 hrs. 1 60 minutes
Since one hour and 60 minutes are physically the same, the result is multiplication by unity, which does not change the value, only the units.
Here is a more complex example. If a particular numerical result is 44 miles per hour, and you wish to find the answer in kilometers per hour using common knowledge, proceed as follows:
44 miles 5280 feet 12 inches 2.54 cm 1 meter 1 km------- x ------------ x ---------- x ------- x -------- x ----- hour 1 miles 1 foot 1 inch 100 cm 1000 m
= 70.81 kph. Note that all of the units will cancel except km / hr.
To find equivalent units for all kinds of measurement go to the table in http://en.wikipedia.org/wiki/Conversion_of_units
2. Hints for accurate calculations
a. Make sure the units are physically reasonable. If you came up with square meters for length, there must be an error.
b. In numerical examples, carry units through each step of the calculation. Note there will be a grade deduction for answers with no units or incorrect units.
c. Check the order of magnitude of the result against common sense. Here are some humorous examples from actual students at another institution:heart rate of 70 beats/second, urine production rate of 4 liters/minute, body temperature of 101°C; a blood pressure of 100 mV (millivolts)
d. Develop a feel for quantities. For example, if you compute a total blood volume of 5 mL (a teaspoon of fluid) for an adult human, something is wrong. For those of you who still think in British units, consider the following: 1 meter is about a yard in length; 1 cm is about half an inch; 1 liter (equal to 1000 cm3) is about a quart; 1 liter of water weighs 1 Kg (about 2 pounds), hence for water, 1 mL = 1 cm3 = 1 gram; body fluids are dilute aqueous solutions and their volumes weigh about the same as pure water.
11

e. Use no more than three significant figures in numerical results. If you do not understand why a cardiac output of 5.046981 Liters/min is ridiculous, or if you have not heard of the terms "significant figures" or "significant digits", please ask.
3. Avoiding known failure modes
a. Reading someone else’s solution to a problem is not educationally equivalent to generating your own solution.
b. We encourage students to work together in groups to understand the concepts in the problems, rather than dividing the problems amongst members of the groups to work alone.
c. Although it is tempting to postpone working on homework until the night before it is due, this is a poor plan because it limits the group's ability to learn by discussion with fellow students and the teaching staff.
12

Style guide for problem set solutions
Charles F. Babbs, MD, PhD, Instructor
E-mail: [email protected]
Submitted December 7, 2010 __________________________________
13
Title
Author(s) andcontact information
Date Signature(s)(can be electronic)

Objective
To explore quantitatively the relative effect of increasing pulmonary edema on the rate of diffusion of oxygen in an alveolus.
Theory
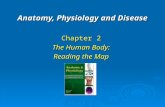
Figure 1. Anatomic sketch of a partially flooded pulmonary alveolus.
Figure 1 shows shrinkage of the alveolar gas volume with accumulation of pulmonary edema fluid along the inside wall of an alveolus. The heavy solid black line represents diminished surface area of the air-water interface. The shaded region indicates increased thickness of fluid, across which respiratory gases must diffuse. Pulmonary capillaries filled with passing blood are embedded in the alveolar wall.
14
Abnormal fluid layerNormal
fluid layer
Pulmonary capillary with red blood cells
Theory-sketch of model-variable definitions-assumptions
Objective
Text paraphrased from assignment

Consider a spherical model of the alveolar gas bubble for which the internal radius is r . As edema fluid accumulates, r shrinks by amount r, as illustrated in Figure 2. The normal thickness of fluid lining the moist alveolar wall is denoted h.
Figure 2. Mathematical model of a partially flooded, spherical alveolus. Smooth dark shading represents the alveolar wall. Dotted light shading represents pulmonary edema fluid.
Assume a simplified diffusion equation for gas exchange across the alveolar wall, in which the
Rate of gas diffusion = = ,
where A is the surface area of the alveolar gas bubble, t is the thickness of the water layer between the surface of the alveolar gas bubble and the pulmonary capillary, c is the difference in oxygen concentration in alveolar gas compared to pulmonary capillary blood, and D is a constant related to the solubility of oxygen in water and the number of capillaries surrounding the alveolus. Critically in this problem we assume that the rate of oxygen diffusion is directly proportional to the surface area of the alveolar gas bubble and inversely proportional to the diffusion distance or thickness.
15
r
r r
h
alveolar wall
edema fluid
Punctuation of math and text in a sentence

Owing to the action of pulmonary surfactant to reduce surface tension, the normal diffusion distance, t = h, is small. This fluid layer is normally too thin to be seen under the light microscope1.
Expressing the diffusion equations in terms of the variables of the model and combining the concentration difference and diffusion constants into a single constant, D', we can obtain an algebraic expression for the rate of gas diffusion across the combined fluid layers in Figure 2 in terms of the surface area of the gas bubble and the total diffusion distance, which is
Rate of diffusion = .
To compare diffusion for alveoli with pulmonary edema vs. normal alveoli, we can take the ratio of the diffusion rates for r > 0 to that for r = 0 to obtain the diffusion ratio
.
Results
Suppose that r = r/2, so that the diameter of the alveolar gas bubble is decreased by one half, and suppose that normal fluid thickness h = r/10. How does the accumulation of edema fluid influence oxygen diffusion?
The rate of diffusion in a normal alveolus would be 40 D' r2. However, the rate of diffusion in a half flooded alveolus is only
Thus half flooded alveoli are only about 1.7/40 or 4 percent as effective in gas exchange as normal alveoli.
To show how quickly the diffusion capacity of an alveolus diminishes with flooding of the lungs, we plot the rate of diffusion as a function of r/r in a numeric program such as Matlab.
1 DiFiore, M.S.H., Atlas of Human Histology, 5th Edition, Lea and Febiger, Philadelphia, 1981.
16
Reference
A specific numerical result
Additional assumptions stated.

Figure 3. Predicted falloff in gas diffusion with increasing thickness of pulmonary edema lining the walls of an alveolus. Fluid thickness is expressed as a fraction of normal alveolar radius. Diffusion is expressed as a fraction of normal. The parameter, h, is the normal thickness of water lining the alveolar wall, expressed as a fraction of alveolar radius.
As the thickness of the abnormal fluid layer increases, diffusion effectiveness falls sharply. For h = 0.1 the assumed normal fluid thickness is 5% of alveolar diameter. For h = 0.02 normal fluid thickness is just 1% of the alveolar diameter. The relative effect of extra fluid on diffusion is greater if the normal baseline fluid layer is thinner. Doubling the normal fluid thickness essentially halves diffusion, as expected from the diffusion equation.
17
Nicely drawn plot
Legend
Graphical results described. They never actually "speak for themselves".

Discussion
The results are geometrically valid for small values of r only. The assumed diffusion equation is that for a rectangular slab. However, the unfolded spherical shell is would be a truncated cone with inside area < outside area, as shown in Figure 4.
Figure 4. A spherical shell of alveolar fluid, unfolded onto a flat surface showing differences in inside area (top) and outside area (bottom). In vivo oxygen would diffuse from top to bottom. Carbon dioxide would diffuse from bottom to top.
For larger values of r the effective diffusion area is somewhat greater than that modeled. An improved model based on calculus would give more accurate results in such cases. However, the major effects of fluid on gas diffusion happen with small values of r < 0.2. So the general conclusions of the analysis remain valid.
Conclusions
The accumulation of a thin layer of pulmonary edema fluid dramatically reduces respiratory gas diffusion in flooded alveoli. Rapid treatment of even mild to moderate pulmonary edema is important to prevent systemic hypoxemia.
18
2r
2(rr)
Limitations of the model
Biological or medical significance
Limitations discounted

Further Instructions for BME 256/295 Problem Sets
The complete problem set should include ONE title page, ONE references section, and ONE appendix.
1. Title page –You can type your names in the signature section, that is an acceptable electronic signature.
2. Objective – restate the objective from the problem set, or write your own.3. Theory – this includes diagrams of models, derivations of equations, and the
equations in algebraic, simplified form, i.e.:
You should define each variable in the equations.Theory does not include numerical results or figures used to compute numerical results. This section should be in the same order as the problem set questions (i.e. if questions 1, 2, 5, and 8 required you to derive equations, the equations should be presented in that order).
4. Results – This section should also follow the order of the problem set. For each numerical result you should
a. Restate the equation in its simplified form (do not immediately start substituting values)
b. State the value of each variable and its units AND the reason you chose that value (you were given it in the question, you solved for it in question 3, you derived it from this image or this source). If you derived the value from an outside source, reference the source and describe how you derived it – i.e. it was given in Table 2 of [ref] or it was calculated from this figure and copy the figure into the text and make sure it is clear how you derived the number from the figure. You are responsible if you get bad information from your source.
c. Rewrite the equation with the numerical variables with the CORRECT units and clear conversion of units, and write your answer – with TWO significant figures unless you have a good reason to use more. For example:
2.7 x 106 m
d. Briefly discuss your result and/or answer the problem set questions related to the results
e. Figures should be in the text and each figure should be referenced in the text (i.e. (Figure 1) or (see Figure 1) and discussed when you reference it. The caption of the figure should give a figure # and a description of what is displayed in the figure.
f. If you used Matlab to find your result, reference the code in the appendix.
19

5. Discussion – answer the Discussion questions here. You should be able to support your assumptions – i.e, for whether or not the amount of blood held in the capillaries is reasonable, you could try to look up the answer or you could talk to an expert (i.e. Drs. Babbs and Tacker). If you look up numbers/information to support your discussion, reference your source (again, you’re responsible for the quality of the source). Make sure and answer every part of each discussion question.
6. Conclusion – give a brief conclusion that shows you get the point of the problem. Did you achieve your objective? What is the medical relevance of this problem?
7. References – We’re going to now use AMA citation style, which is very well explained here: http://healthlinks.washington.edu/hsl/styleguides/ama.html. When you cite a reference in the text, use [1] or (1). Use this1 for footnotes only.
8. Appendix – include Matlab code here (if necessary), please do not send a different file with the code.
General rules:
EDIT your work for spelling, grammar, and formatting issues. Each equation should be placed properly in the text in a readable format (i.e. not too small and fuzzy).
Due to formatting issues with converting from Microsoft Vista .docx to .doc, we require that you hand in a HARD COPY as well as email the TA an ELECTRONIC copy. The hard copy should:
1. Be double-sided (we’re trying to save paper here)2. Be in color if NECESSARY to understand the figures.3. Be free of formatting issues (you are responsible for making sure your problem
set prints correctly!)
The ELECTONIC copy is due at 2:29 p.m. on the due date. The HARD COPY is due in class on the due date.
Your electronic file should be called: Group#_ProblemSet#.doc
For example, if you are group 20 and this is problem set 3, your file would be called:Group20_ProblemSet3.doc
20

BME 256/295 Spring 2011 Problem Set Work Groups
Group # Name 1 Name 2 Name 3 Name 41 Au, Anthony S. Richett, Brittany K. Sanghani, Aditya D. Schaller, Ryan J.
2 Kochert, Megan N. Olashuk, Justin E. Rauchenstein, John Wallis, Stacey M.
3 Chow, Andrew C. Okleshen, Dane A. Peckenpaugh, Eric J. Waite, Jennifer M.
4 Bong, Terri L. Gossett, Paull C. Iliff, Benjamin P. Joseph, Micheal I.
5 Cahyadi, Bernard E. Duffy, Daniel R. Louis, Kevin T. Mah, Krysten R.
6 Morris, Matthew E. Ng, Kyle Y. Shen, Luhou Zanath, Erica N.
7 Leow, Yijun E. Truesdell, Stephen M. VanCamp, Michael J. Zhang, Johnny
8 Druyos, Timothy P. Rasmussen, Matthew T. Shah, Michelle Yu, Calvin K.
9 Blatchley, Michael R. Kohrs, Hannah B. McCormick, Cassandra L. McCuen, Emily C.
10 Schmitt, Dakota L. Throne, Kristina L. Weinberg, Charles A. Wilson, Robert L.
11 Chelminski, Alexander Z. Kuhn, Allison E. Mercer, Elizabeth Wei, Duanyi
12 Costalunga, Kevin M. Crofton, Kirsty E. Pepper, Nathan D. Wu, Chieh-En
13 Findley, Kelly M. McNamara, Thomas J. Reidy, John D. Thomas, Richard M.
14 Hunnicutt, Jarrod S. Kingsley, Jeffrey A. Kvindlog, Anna C. Naik, Manshi K.
15 Ayarza, German E. Blum, Kevin M. Clifford, Timothy P. Grimes, Amanda M.
16 Chandramouli, Aaditya G. Jaitpal, Siddhant V. Plag, Nathan J.
17 Cavanaugh, Caitlin M. Guerra, Alexandra N. Manring, Jonathan E.
21