ANATOMY, PHISIOLOGY and ILLNESSES of the NOSE and PARANASAL SINUSES
47
ANATOMY, PHISIOLOGY and ILLNESSES of the NOSE and PARANASAL SINUSES Head of otolaryngology department Prof. Alexander I. Yashan
description
ANATOMY, PHISIOLOGY and ILLNESSES of the NOSE and PARANASAL SINUSES. Head of otolaryngology department Prof. Alexander I. Yashan. Anatomy of the nose. Line drawing of the key arterial vessels of the nose. - PowerPoint PPT Presentation
Transcript of ANATOMY, PHISIOLOGY and ILLNESSES of the NOSE and PARANASAL SINUSES

ANATOMY, PHISIOLOGY and ILLNESSES of the NOSE and
PARANASAL SINUSES
Head of otolaryngology department
Prof. Alexander I. Yashan

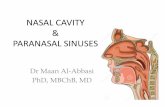
Anatomy of the nose






Line drawing of the key arterialvessels of the nose.

Computerized axial tomography (CAT) radiograph of the nose.Coronal section view of the osteomeatal unit.Note
bilateral concha bullosa.

Line drawing of the sagittal view of the lateral nasal wall indicating the approximate location of the major sensory nerves.

NASAL SEPTUM ANATOMY

NASAL SEPTUM DEFORMITY (DEVIATION)

NASAL SEPTUM DEFORMITY (DEVIATION)
• This pathology meets in many people and practically it’s impossible to meet a person with not deviated partition of nose. Deformation of nasal septum long time can remain not noticed and cause not complaints. Only at violation of the nasal breathing or appearance of other symptoms its deformity is diagnosed.
• Attend factors• Traumas of the nose (75 % of cases). • Inconsistency between growth of nasal septum and nasal
cavity. Nasal septum growths quicker then nasal cavity.• Congenital deformity (rachitis).• Compensate deformity (pressure on septum by
hypertrophied nasal turbinates, or by tumor of the nose).

Clinic of Nasal septum DEFORMITY
• One side or both sides nasal airway obstruction (heavy breathing through the nose).
• Nasal drainage.
• Hyposmia.
• Deformation of external nose.
• Nose-bleeds.

Diagnostics•Anamnesis (trauma). General examination of the faceAnterior and posterior rhinoscopia – it is possible to see the deformity of nasal septum either in cartilaginous or in bone parts or in both septum parts: S-like, arched, angled-like deformity; ridge or spur of the septum.•The anemization of a nasal mucous lining (by a cotton tip applicator moistened with lidocain+adrenalin 1:10 solution) for best visualization of deeper departments of the nasal cavity;•Probing of the nose after anemization by the cotton tip applicator.•X-ray.

Complications – appears due to nasal congestion or due to
pathological reflexes:• Acute and chronic rhinitis (hypertrophy), vasomotor rhinitis;• Acute and chronic sinusitis (due to deterioration of sinuses
aeration and drainage);• Acute and chronic otitis media (due to dysfunction of
eustachian tube);• Acute and chronic pharyngitis (due to breathing through
the mouth);• Acute and chronic laryngitis;• Conjunctivitis (due to dysfunction of nasolacrimal canal);• Reflex disorders of internal organs (bronchial asthma,
asthmatic bronchitis, enuresis, and headache).

Treatment• Nasal septum deformity is treated by a surgical
method only. Indications for septoplasty are the nasal congestion and full airway obstruction, or presence of other complications.
• There are several variants and methods of operation. The most accepted surgical methods are:
• Radical submucous nasal septum resection (Killian approach).
• The sparing operations (Voyachec approach): • a/ mobilization; • b/ redresation; • c/ circular resection; • d/ partial resection



FURUNCLE OF the NOSE- inflammation of fat glands or hair follicles, located in entrance of the nose or on its external surface.Pathogenic organisms: most common are staphylococci and streptococci.Attend factors1. Micro trauma of nasal skin (during self cleaning).2. Irritation of nasal skins by dischar-ges due to acute rhinitis or sinusitis.3. General furunclousis.4. Diabetes or other metabolic disorders.

Clinic• Spontaneous pain in the nose especially in the site of furuncle.• Fever.• Edema of nasal skin and surrounding tissues.• General inspection and anterior rhinoscopia• Cone-shaped infiltrates on one of nostril’s walls or on the
external surface of the nose.• Painfulness and edema of the external nose and surrounding
tissue: cheek, bridge of the nose, upper lip, eyelids.• Redness of nasal skin, it is tense and very sensible.• On a 3-5 day, and sometimes later, in the center of furuncle
appears purulent cavity, with opening on apex. At the beginning pus is liquid dripping out, forming scab on the furuncle surface and masking real infiltrate. After removing of scab, thin hole can be revealed. Then contents of furuncle become jelly-like, forming shank (grey necrotic masses). It can be removed itself, either by doctor, or by the patient himself.
• It is categorically banned to squeeze out pus from the furuncle of nose, as it can result in intracranial complications (thrombosis of cavernous sinus).

Complications• Lymphadenitis of cervical lymphatic nodes.
• Thrombosis of facial veins.
• Thrombosis of cavernous sinus of brain is the most serious complication of the furuncle. It appears due to spreading of inflammatory thrombosis from facial veins to the cerebral sinuses (through anastomosis between angular vein - the branch of facial vein and ophthalmic vein – from cavernous sinus).

Treatment• 1. Greasing of a skin by antiseptics ointments, or ointments with
antibiotics and corticosteroids.• 2. Surgical incision of furuncle (after appearance of purulent apex) with
draining by rubber band.• 3. Anti-inflammatory drugs.• 4. Antibacterial therapy (antibiotics - better passing through blood brain
barrier).• 5. Physical therapy procedures (fonoforesis with ointments) at the end of
disease.• Patients with the furuncle of nose must be treated in hospital.• Care of patient• Progressing edema of patient’s face soft tissue has to disturbance
medical personal, as well as changes of consciousness and septic sings: fever with chills and sweating all over, strengthening of headache, appearance of meningeal signs, dizziness, and vomits. Appearance of such pathological sings indicates on development of intracranial complications.
• Prophylaxis• 1. Tempering of organism.• 2. Medical treatment of acute rhinitis.• 3. Medical treatment of endocrine diseases (diabetes).

RHINITIS (COLD) - is inflammation of nasal mucus lining
Acute and Chronic rhinitis
• ACUTE RHINITIS (COMMON COLD) • is the most frequent human disease. An average adult suffers a
common "cold" two to three times per year, more often in childhood and less often the older he gets as he develops more immunity. The common "cold" is caused by any number of different viruses, some of which are transmitted through the air, but most are transmitted from hand-to-nose contact. Once the virus gets established in the nose, it causes release of the body chemical histamine, which dramatically increases the blood flow to the nose, causing swelling and congestion of nasal tissues, and stimulating the nasal mucosa to produce excessive amounts of mucus.

• Acute rhinosinusitis: sudden in onset, lasting up to 4 weeks. Symptoms resolve after treatment.
• Subacute rhinosinusitis: acute rhinosinusitis that progresses 4 to 12 weeks. Symptoms eventually may be less severe than in the acute phase and still resolve after treatment.
• Recurrent acute rhinosinusitis: symptoms and physical findings of acute rhinosinusitis, lasting 1 to 4 weeks. More than four episodes per year, with intervening symptom-free interludes.

Pathogenic organisms: • viruses (adenoviruses, rhinoviruses) - at the beginning of the
disease (1-3 days);• staphylococci and streptococci;• bacteria.• Acute rhinitis is very contagious disease. The spreading way is
mainly air-drop, but contact transmission (through hands, crockery, objects) is possible too. The incubation period is 1-3 days. The bacterial super infection often joins to the viral infection (mainly gram positive cocci flora). The immunity to viruses lasts out only short time after convalescence so it’s possible to have reinfection of same virus.
Attend factors• Cooling of the organism;• Breathing with heated or dry air;• Other defects in the nose and throat (allergy, septum deformity)• Low general resistance of organism;• Stresses.

Diagnosis of Acute Rhinosinusitis, Major and
Minor Factors Major Factors Minor Factors
Facial pain/pressure Headache
Facial congestion/fullness Fatigue
Nasal obstruction/blockage Halitosis
Nasal discharge/ purulence/ discolored postnasal drainage
Dental pain
Hyposmia/anosmia Cough
Purulence in nasal cavity on examination
Earpain/ pressure/ fullness
Fever

Cliniccan be divided in three stages:
• 1. „Dry stage” lasts from few hours to few days. At the beginning of disease there is easy indisposition. Dryness and tickling in the nose, sneeze, easy pain in the throat and feeling of head compression can be marked. Progressing nasal congestion begins in the first stage and continues in second and third stages. The mucous lining of the nasal cavity gets a purple-red color and acutely infiltrates.
• 2. Stage of serosous excretions is characterized by abundant watery excretions from the nose. The patient also suffers from full nasal obstruction, headache, sub febrile temperature, and hyposmia. The nasal discharge is thin and plentiful, it irritates the skin around the nose. Then discharges become more tick. Second stage lasts 2-4 days.
• 3. Stage of mucous-purulent excretions. In this stage the quantity of excretions diminishes, they become mucus and purulent (adding of bacterial infection) . This stage lasts 2-4 days.
• In next 6-12 days (eventual phase) the symptoms of “lowering” infection can appear – causing the inflammation of throat and larynx, that shows up pain in a throat, hoarse of voice, cough and others like that.
• If in an inflammatory process spreads to paranasal sinuses, pain in the area of their projection appears (brow, bridge of the nose, cheeks). If inflammation spreads to the Eustachian tube, fullness in the ear and hearing loss appear.

Complications
• • Acute sinusitis.• • Acute otitis media.• • Acute pharyngitis.• • Acute laryngitis.• • Acute tonsillitis• • Pneumonias and others like that.• • Furuncle of the external nose.• • Possible transition in chronic rhinitis.

Medical Treatment
• At the beginning of disease his development can be stopped by means sudorific medication (hot mustard baths on feet, for children - paraffin “socks”). Decongestants drops in the nose (0,1 % solutions of naphthyzin, galazolin, sanorin, rhinozolin). These medications improve the nasal breathing, save permeability of opening between paranasal sinuses and nasal cavity, and reduce mucous lining edema of the Eustachian tube.
• The term of decongestants drops administration must not exceed a 1 week. More prolonged use of these medications can develop the medicinal rhinitis.
• Antihistamines and decongestants help relieve the symptoms of a "cold," but time alone cures it. In persons with headache analgesics are prescribed (paracetamol, analgil, ascofen and others like that). Medications in the aerosol packing are used: ingalipt, cameton; and also inhalation of hot air and irrigation of nasal cavity by antiseptic solutions (decoctions of medical flowers and leafs - 10 g on 200 the ml boiled water). Physical therapy procedures are also applied.

Rhinitis in newborns• is always heavy disease, as their protective mechanism is not
enough developed. Babies carry difficulty of the nasal breathing heavier, than senior children, as, except for violation of breathing, a cold hinders still and pectoral feeding.
• This disease presents a special danger to babies. The nasal meatuses in infants are very narrow, and nasal obstruction is very likely to follow even a minor swelling of the mucosa.
• Apart from disorders due to the absence of nasal respi ration, such as excitability, broken sleep, etc., nasal ob struction may often lead to emaciation of the baby, which is unable to suck at the breast normally
• Clinic • The temperature of body is often high. There can be meningeal
symptoms, quite often the violated function of the digestion system is observed (vomits, diarrhea). At the heavy cases the inflammation of pharyngeal tonsil can occurred (adenoiditis). Other complications are the inflammations of ear, throat, lungs and others like that.

Medical Treatment Rhinitis in newborns
• Decongestant drops in the nose (0,01-0,05 % solution of adrenalin, nazivin, rhinozolin) to maintain the nasal cavity passability during breast-feeding. Before feeding the secretion from the nasal cavity is sucked by a bulb.
• Prophylaxis • Out contact of child with virus infect
patient.

CHRONIC RHINITIS (CHRONIC COLD) is chronic unspecific inflammation of nasal mucus lining.
• Reasons • Repeated attacks of acute rhinitis.• The prolonged action of external harmful factors
(dust, gases, overheated air and others like that).• Infection lesion located near to the nose
(adenoids, sinusitis, tonsillitis, carious teeth).• Nasal septum deformity.• Disease of internal organs (hearts, stomach,
kidneys and others like that).• Deep damages of mucous lining due to acute
infectious diseases (scarlet fever, diphtheria and others like that).
• Constitutional inclination.

Chronic catarrhal rhinitis. • Its symptoms are basically the same, though not so marked
as those of acute rhinitis. Patients complain of nasal obstructions and nasal discharge. The obstruction is not constant and is worse on lying down. When the patient turns in bed, the upper nostril opens up and the lower nostril closes. The discharge may be abundant or poor; sometime it may be mucus, sometime – purulent; may be postnasal discharge. Although there can be dryness, hyposmia, headache, disorders of sleep.
• Rhinoscopia reveals the diffuse edema of nasal mucous lining and its diffuse redness. In some cases the inferior turbinate may be so congested and swollen that is impossible to see deeper parts of the nose. To make visible inner parts of nasal cavity it’s necessary to do anemization of mucous lining by application of 0,1 % adrenalin solution .

Chronic hypertrophy rhinitis • is more common in males. The principle deference of this
disease from catarrhal rhinitis is the development of fibrous tissues in the submucosal layer of the nose, particularly over the inferior turbinate. The disease is characterized by diffuse or limited hyperplasia of mucous lining. This fibrous tissue contracts in different places (mostly on inferior turbinate) so mucus surface becomes irregular. Patients suffer from the abundant nasal secretion and obstruction, headache and hyposmia. Excretion from the nose is mainly mucus, and it becomes purulent when pathogenic organisms change.
• On rhinoscopia in common cases the nasal cavity is filled by abundant, thick, viscid, yellowish discharges. After cleaning (by blowing patient's nose) the mucosal lining looks congested, swollen and deep in colour. The turbinates are enlarged and hypertrophied particulary the inferior one, so it hampers to inspect the inner parts of nasal cavity. Surface of mucous lining is irregular, pitted and looks mulberry-shaped or mulberry-shaped

diagnostic• The anemization probe is used. The nasal lining is
smeared by vasoconstrictor solutions (adrenalin, naphthyzin and others like that). In patients with catarrhal rhinitis the nasal lining become thinner and nasal breathing becomes better; in patients with hypertrophy rhinitis the hypertrophy places do not change and breathing either not becomes better, or get better only in insignificant measure.
• Chronic hypertrophy rhinitis can complicate by appearance of polypes, especially when allergy present, so chronic polipous rhinosinusitis can develop. In rare cases malignant growth can occur, so a morphological examination is needed.

Chronic atrophy rhinitis • is more common in females. Atrophy of nasal mucous lining is main
characteristic of this disease. Mucous membrane loses some of its mucous glands also it sheds (теряет) ciliated epithelium and in many places it undergoes metaplasia turning into squamous stratified epithelium. The dis ease is often accompanied by diminished mucous secre tion which tends to dry into crusts, but has no bad smell (in contrast to ozaena). The olfactory nerves become atrophic.
• Symptoms. A young female patient suffers of constant dry ness in the nose and nasopharynx. Another common com plaint is a feeling of foreign body in the nose or dull pressure at the nasal root. Paradoxical to the wide nasal meatuses, nasal obstruction appears due to the crusts accumulation on the surface of turbinates and nasal septum. After self removing of this crusts the little bleeding can occur. The headache, hyposmia or anosmia (full or partial loss of smell) can present. In may cases the atrophic process spreads to the pharynx and larynx, so dryness of the throat can occur.
• On rhinoscopia the reduction or absence of secretion and formation of crust in the nose can be observed. The nasal cavity fills with yellowish or green crusts or scabs. After removal of the crusts, the nasal passages are seen to be very wide and in anterior rhinoscopy offer a clear view of the posterior wall of the nasopharynx. The nasal mucous membrane appears dry, very thin, and pale (not red).

Medical Treatment • This may be local or general. Above all, the underlying
cause of disease should be found out and should be eradicated, if possible. Liquidation of inflammation focus, that can be located near to the nose or alongside should be done (medical treatment of carious teeth, chronic tonsillitis, adenoids, chronic sinusitis and others like that). The presence of any nasal deformity should be eradicated. Physician should advise patients to avoid the harmful factors of external environment (even to change the unhealthy job), to eliminate smoking of tobacco, drinking and to keep to a diet. If necessary, medical treatment of internal diseases is administrated (hearts, stomach, kidney, and others like that). If allergy present, the expose of allergen is needed to avoid the contact with it. Antiallergic medical treatment is prescribed. Antihistamines and decongestants help relieve the symptoms of a "cold". In cases with fever, antibiotics may have to be used after culture and sensitivity test of the nasal discharge have been done.

Chronic catarrhal rhinitis. • Local treatment consists of prescribing astringent and vasoconstrictor drops.
Decongestants drops or sprays in the nose (0,1 % solutions of naphthyzin, galazolin, sanorin, rhinozolin, and so on) and anti-inflammatory prescription nasal sprays (argyrols, polydexa, izofra) is prescribed, with duration no more than 1 week. These medications improve the nasal breathing, save permeability of opening between paranasal sinuses and nasal cavity, and reduce mucous lining edema of the Eustachian tube.
• For thinning secretions, especially for older persons, more fluids drinking (eliminating caffeine, and avoiding diuretics - fluid pills) may be recomended. Mucous-thinning agents such as guaifenesin (Humibid, Robitussin) may also thin secretions.
• Irrigating of the nasal cavity by sodium chloride solution (a 1 tea-spoon on a 1 glass of water), can be advised. The patient breathes in the nose the heated solution from the tea-pot spout, or from the built palm. Nasal irrigations may alleviate thickened secretions. These can be performed two to four times a day either with a nasal douche device or a Water Pik with a nasal irrigation nozzle.
• In patients with diffuse swelling of the nasal mucous membrane the injections of glucocorticoid solutions (dexamethazone, hydrocortisone est.) in the inferior turbinate (once in 2-3 days) are effective.
• Also the physiotherapeutic procedures should be prescribed (endonazal electrophorus of calcium chloride or zinc sulfate, ultrasonic therapy, UShF, appliques of dirt).

Chronic hypertrophy rhinitis. • Conservative treatment, as a rule, has only temporal effect in
such patients. The injections of glucocorticoid solutions in the inferior turbinate are useful. If they are not effective after 3-4 times, more vigorous surgical procedures are performed. Places of hyperplasia of mucous lining are removed by means of:
• Chemicals (chemiocaustics) – solutions of silver nitrate, chromic or trichlor acetic acids (10 %) are applied to pathological tissue.
• Galvanocautery – cauterization with a special instrument - pointed electrocauter.
• Criodestruction (by liquid nitrogen). • Resection of part of the inferior turbinate by surgical
instruments (nasal scissors, conсhotom, nasal snare (петля)).

Chronic atrophy rhinitis. • The treatment of those patients may only be symptomatic, it aims to irritate nasal mucous
membrane to increase production of mucus. It relieves dryness and crusting in the nose by alkaline douches with subsequent application of iodine glycerol solution, oint ments or menthol oil. The nose may also be cleansed of crusts by warm alkaline spray. Below are the formulae of the alkaline solution and some of the drops and ointments commonly used:
• Rp. Jodi puri 0.05-0.1 ""• Kalii jodati 0.2• Glycerini • Aq. destill. aa 5.0• 01. Menthae pip. gtt. 1• DS. Five drops in each nostril twice a day• #• Rp. Mentholi crystallisati 0.1 • 01. Provincialis 20.0 • DS. Five drops in each nostril twice a day• #• Rp. Natrii bicarbonici 60.0• Natrii biborici 30.0• Natrii chlorati 10.0
01. Menthae pip. gtt. VM. f. pulv.
• DS. One teaspoonful in a glass of water for a nasal douche• enzymes (0,001 g tripsin on 50 ml isotonic solution) or mineral waters (“Glade of cvasova”,
“Borgom” and others like that. ). After cleaning conduct instilyatsii vegetable butters with tocoferolom and retinolom; useful butters of sea-buckthorn and wild rose. Appoint electroforez nicotine acid or potassium of iodide on the area of neck or nose and navcolonosovih bosoms. Enough effective there is in the conditions of warm moist climate.

Neurovegetative form of vasomotor rhinitis
• describes a nonallergic "hyperirritable nose" that feels congested, blocked, or wet.
• The mucosa of the nose have an abundant supply of arteries, veins, and capillaries, which have a great capacity for both expansion and constriction. Normally these blood vessels are in a half-constricted, half-open state. But when a person exercises vigorously, his/her hormones of stimulation (i.e., adrenaline) increase. The adrenaline causes constriction or squeezing of the nasal mucosa so that the air passages open up and the person breathes more freely.

Attend factors
• Frequent acute inflammatory processes of upper airways;
• Violation of the vegetative nervous system;
• Nasal septum deformity;
• The prolonged foreign body in nasal cavity;
• The protracted supercooling of organism;
• Digestive apparatus disorders.

VASOMOTOR RHINITIS
• „Rhinitis" means inflammation of the nose and nasal mucosa. "Vasomotor" means blood vessel forces. Two forms are distinguished:
• Neurovegetative;
• Allergic.

Clinic. • Vasomotor rhinitis is characterized by intermittent at tacks with
very brief and sometimes long periods of relief. The attacks, very violent at times, are accompanied by prolonged paroxysms of sneezing, nasal obstruction and pro fuse, mostly watery, discharge from the nose or postnasal drip. Many patients have additional symptoms of lacrimation, itching of the eyes, nasal interior and hard palate, and headache.
• Rhinoscopia. • Turbinates may be enlarged.• Edema of nasal mucous lining.• Mucus-watery or foamy excretions in nasal meatuses a
generous amount.• Bluish or cyanotic color of nasal mucous lining with white or
gray spots on it (Voyachec spots). • In the intervals between the attacks, all morbid symptoms may
utterly disappear, so there may be no rhinoscopic sign at all. But in pro tracted cases, the swelling of the nasal mucosa may become stable or turn into hyperplasia, as in chronic rhinitis.

Sinusitis