Anatomy of the Callosomarginal Artery Applications to Microsurgery and Endovascular Surgery
9
SURGICAL ANATOMY 602 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com Daniel D. Cavalcanti, MD Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona Felipe C. Albuquerque, MD Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona Benjamin F. Silva, MD Department of Neurosurgery, Bonsucesso General Hospital, Rio de Janeiro, Brazil Robert F. Spetzler, MD Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona Mark C. Preul, MD Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona Reprint requests: Mark C. Preul, MD, c/o Neuroscience Publications, Barrow Neurological Institute, 350 W. Thomas Road, Phoenix, AZ 85013. E-mail: [email protected] Received, March 5, 2009. Accepted, September 25, 2009. Copyright © 2010 by the Congress of Neurological Surgeons T he callosomarginal artery (CMA) is consid- ered the largest branch of the pericallosal artery 1 and is described in 40% to 85% of hemispheres, 1-5 yielding different classifications for this vessel and for the anatomy of the perical- losal artery. Together with the pericallosal artery, the CMA helps supply the anterior two-thirds of the medial and superomedial aspects of both hemi- spheres. There is some confusion in the nomen- clature as to the artery best fitting the definition of “callosomarginal artery.” 5 Moscow et al 6 defined the CMA as the artery that courses in or near the cingulate sulcus and gives rise to 2 or more major cortical branches. Rhoton supports this defini- tion. 1 The confusion exists in that 1 or more large arteries branching from the pericallosal artery often run in the cingulate sulcus and give rise to 2 or more cortical arterial branches. 5 Distal anterior cerebral artery (ACA) aneu- rysms represent 1.5% to 9% of intracranial aneurysms and most often occur at the origin of the CMA. 8-10 That location is also one of the preferred sites for traumatic intracranial aneurysms to develop. 11-14 The CMA can also supply falx meningiomas. Consequently, the artery can be a route for preoperative tumor embolization. 15,16 In 1978, Bogdanović et al 17 described the ori- gin, frequency, and course of the CMA. We per- formed microanatomic dissection of human cadaveric specimens and analyzed digital subtrac- tion angiograms (DSAs) to demonstrate the micro- surgical anatomic features of the CMA and its branches and its relationship with the perical- The Anatomy of the Callosomarginal Artery: Applications to Microsurgery and Endovascular Surgery BACKGROUND: The callosomarginal artery (CMA), the main branch of the pericallosal artery, courses in or near the cingulate sulcus and gives rises to 2 or more major cortical branches. There is confusion about the artery best fitting the definition of “callosomarginal artery.” Distal anterior cerebral artery aneurysms represent 1.5% to 9% of intracranial aneurysms, and most often occur at the origin of the CMA. The microsurgical anatomic features of the CMA, its relationship with the pericallosal artery, and clinical implications are presented. METHODS: The origin, course, branching pattern, and diameter of the CMA and its branches and its relationship with the pericallosal artery were studied in 60 cerebral hemispheres, including cadaveric dissections and angiographic images. RESULTS: The CMA was present in 93.3% of hemispheres studied and arose mainly from A3 (55.2%), a mean of 3.11 ± 1.90 cm from the anterior communicating artery. The mean diam- eter of the CMA at its origin was 1.53 ± 0.36 mm. The CMA ran 1.28 ± 0.89 cm until its first branch, describing an anterior convex curve backward and upward (60.7%). An average of 3 lesser branches originated from the CMA. The most consistent branch was the posterior internal frontal artery (67.9%). The mean diameter of the CMA branches was 0.93 ± 0.33 mm. CONCLUSION: These morphometric measurements can help neurosurgeons access lesions located in distal intracranial vessels. The vessel coursing the longest pathway in or near the cingulate sulcus and otherwise following Moscow's classic definition should be con- sidered the CMA. KEY WORDS: Anatomic study, Anterior cerebral artery, Callosomarginal artery, Endovascular treatment, Microsurgery Neurosurgery 66:602-610, 2010 DOI: 10.1227/01.NEU.0000365003.25338.62 www.neurosurgery-online.com ABBREVIATIONS: ACA, anterior cerebral artery; CMA, callosomarginal artery; DSA, digital subtrac- tion angiogram; ICH, intracerebral hematoma; SD, standard deviation
-
Upload
vovaatanasov -
Category
Documents
-
view
217 -
download
3
Transcript of Anatomy of the Callosomarginal Artery Applications to Microsurgery and Endovascular Surgery

SURGICAL ANATOMY
602 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com
Daniel D. Cavalcanti, MDDivision of Neurological Surgery,Barrow Neurological Institute,St. Joseph’s Hospital andMedical Center,Phoenix, Arizona
Felipe C. Albuquerque, MDDivision of Neurological Surgery,Barrow Neurological Institute,St. Joseph’s Hospital andMedical Center,Phoenix, Arizona
Benjamin F. Silva, MDDepartment of Neurosurgery,Bonsucesso General Hospital,Rio de Janeiro, Brazil
Robert F. Spetzler, MDDivision of Neurological Surgery,Barrow Neurological Institute,St. Joseph’s Hospital andMedical Center,Phoenix, Arizona
Mark C. Preul, MDDivision of Neurological Surgery,Barrow Neurological Institute,St. Joseph’s Hospital andMedical Center,Phoenix, Arizona
Reprint requests:Mark C. Preul, MD,c/o Neuroscience Publications,Barrow Neurological Institute,350 W. Thomas Road,Phoenix, AZ 85013.E-mail: [email protected]
Received, March 5, 2009.
Accepted, September 25, 2009.
Copyright © 2010 by theCongress of Neurological Surgeons
The callosomarginal artery (CMA) is consid-ered the largest branch of the pericallosalartery1 and is described in 40% to 85% of
hemispheres,1-5 yielding different classificationsfor this vessel and for the anatomy of the perical-losal artery. Together with the pericallosal artery,the CMA helps supply the anterior two-thirds ofthe medial and superomedial aspects of both hemi-spheres. There is some confusion in the nomen-clature as to the artery best fitting the definitionof “callosomarginal artery.”5 Moscow et al6 definedthe CMA as the artery that courses in or near thecingulate sulcus and gives rise to 2 or more majorcortical branches. Rhoton supports this defini-
tion.1 The confusion exists in that 1 or more largearteries branching from the pericallosal arteryoften run in the cingulate sulcus and give rise to2 or more cortical arterial branches.5
Distal anterior cerebral artery (ACA) aneu -rysms represent 1.5% to 9% of intracranialaneurysms and most often occur at the origin ofthe CMA.8-10 That location is also one of thepreferred sites for traumatic intracranial aneurysmsto develop.11-14 The CMA can also supply falxmeningiomas. Consequently, the artery can be aroute for preoperative tumor embolization.15,16
In 1978, Bogdanović et al17 described the ori-gin, frequency, and course of the CMA. We per-formed microanatomic dissection of humancadaveric specimens and analyzed digital subtrac-tion angiograms (DSAs) to demonstrate the micro-surgical anatomic features of the CMA and itsbranches and its relationship with the perical-
The Anatomy of the CallosomarginalArtery: Applications to Microsurgeryand Endovascular Surgery
BACKGROUND: The callosomarginal artery (CMA), the main branch of the pericallosal artery,courses in or near the cingulate sulcus and gives rises to 2 or more major cortical branches.There is confusion about the artery best fitting the definition of “callosomarginal artery.”Distal anterior cerebral artery aneurysms represent 1.5% to 9% of intracranial aneurysms,and most often occur at the origin of the CMA. The microsurgical anatomic features of theCMA, its relationship with the pericallosal artery, and clinical implications are presented.METHODS: The origin, course, branching pattern, and diameter of the CMA and its branchesand its relationship with the pericallosal artery were studied in 60 cerebral hemispheres,including cadaveric dissections and angiographic images.RESULTS: The CMA was present in 93.3% of hemispheres studied and arose mainly from A3(55.2%), a mean of 3.11 ± 1.90 cm from the anterior communicating artery. The mean diam-eter of the CMA at its origin was 1.53 ± 0.36 mm. The CMA ran 1.28 ± 0.89 cm until its firstbranch, describing an anterior convex curve backward and upward (60.7%). An average of3 lesser branches originated from the CMA. The most consistent branch was the posteriorinternal frontal artery (67.9%). The mean diameter of the CMA branches was 0.93 ± 0.33 mm.CONCLUSION: These morphometric measurements can help neurosurgeons access lesionslocated in distal intracranial vessels. The vessel coursing the longest pathway in or nearthe cingulate sulcus and otherwise following Moscow's classic definition should be con-sidered the CMA.
KEY WORDS: Anatomic study, Anterior cerebral artery, Callosomarginal artery, Endovascular treatment, Microsurgery
Neurosurgery 66:602-610, 2010 DOI: 10.1227/01.NEU.0000365003.25338.62 www.neurosurgery- online.com
ABBREVIATIONS: ACA, anterior cerebral artery;CMA, callosomarginal artery; DSA, digital subtrac-tion angiogram; ICH, intracerebral hematoma; SD,standard deviation

NE UROSURGERY VOLUME 66 | NUMBER 3 | MARCH 2010 | 603
CALLOSOMARGINAL ARTERY
losal artery. To the best of our knowledge, this study is the firstin the English literature to focus on the microanatomy of theCMA. Clinical cases are presented to demonstrate how knowl-edge of the anatomy can be used to guide endovascular and micro-surgical procedures.
PATIENTS AND METHODSThe anatomy of the CMA was studied in 60 human cerebral hemi-
spheres. The study included the dissection of 15 adult cadaveric brains (30cerebral hemispheres) injected with colored silicone and lightly fixed ina formalin solution, and the analysis of DSAs from 20 patients (30 sides).The mean age of the cadaveric specimens was 72.3 years (range, 47–92years). There were 9 women and 6 men. The DSAs were performedbetween August 2008 and May 2009. The mean age of the patients was57.4 years (range, 35–84 years). There were 7 women and 13 men.
The origin and course of the CMA and its relationship with the peri-callosal artery were identified in the cadaveric specimens. The length of themain trunk of the CMA (between the origin and first branch) and thedistance between the origin of the CMA and the anterior communicatingartery were also measured during dissections. The branching pattern of
the CMA and its branches was evaluated in the specimens and angiograms.The diameter of the vessels in specimens was measured with digital calipers,and the luminal diameter was obtained using the software Web Dominatorfor angiograms (DR Systems, Inc., San Diego, CA).
RESULTSOrigin of the CMA
The CMA was present in 93.3% of the 60 cerebral hemispheresstudied. In 55.2% of the hemispheres dissected, the CMA arosefrom the A3 segment of the ACA with 3 different topographiesrelated to the genu of the corpus callosum: at its lower aspect, at itslevel, and at its upper aspect (Fig. 1; Table 1). The CMA originatedfrom the A4 segment in 24.1% of the hemispheres and from theA2 segment and the anterior communicating artery in 10.3% each.
The mean distance from the origin of the CMA to the anteriorcommunicating artery was 3.11 ± 1.90 cm standard deviation (SD)(range, 0–7.1 cm). The mean diameter of the CMA at its originwas 1.53 mm ± 0.36 SD (range, 0.9–2.6 mm) in the dissections and2.0 mm ± 0.34 SD (range, 1.2–2.5 mm) in the radiologic analy-
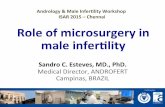
FIGURE 1. Cadaveric photographs showing that the callosomarginal artery(CMA) most often arose from the A3 segment. A, the CMA originated at thelower aspect of the A3 segment and followed an anterior convex curve. Fourmain cortical branches (CBs) arose from the CMA: the anterior internal frontalartery (AIFA), a common trunk of the middle internal frontal artery (MIFA),theposterior internal frontal artery (PIFA), and the paracentral artery (PceA). B,in this specimen, the CMA originated from the A3 segment at the level of thegenu of the corpus callosum. It also followed the characteristic anterior convex curveand was oriented backward and upward. Only 2 branches arose from the CMA:the MIFA and PIFA. The orbitofrontal artery (OfA), frontopolar artery (FpA),AIFA, PceA, superior parietal artery (SParA), and inferior parietal artery (IParA)arose from the pericallosal artery (PrCA). The common trunk created by theOfA and FpA arising from the pericallosal artery matches Moscow’s definition,thereby leading to the identification of 2 CMAs. C, the CMA arose from the A3segment at the upper aspect of the genu of the corpus callosum. It followed an anterior convex curve, while oriented backward and upward, into the cingulate sul-cus. The MIFA, PIFA, and PceA were branches of the CMA. The common trunk of the FpA and AIFA arising from the pericallosal artery also matches Moscow’sdefinition. (Used with permission from Barrow Neurological Institute.)
A B
C

604 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com
CAVALCANTI ET AL
sis. The diameter of the pericallosal artery at the origin of the CMAwas slightly smaller than the CMA itself in the dissections (1.42mm ± 0.32 SD; range, 1.0–2.0 mm) and similar to that of CMAin the angiograms (2.04 mm ± 0.49 SD; range, 1.1–2.9 mm).
Configuration of CMAAfter its origin, the CMA had a characteristic anterior convex curve
in 60.7% of the hemispheres studied (Fig. 1). In 25% of the spec-imens, the CMA ascended with a posteriorly oriented angle withthe pericallosal artery. In 7.1% of specimens, the CMA was ori-ented superiorly and formed aright angle relative to the peri-callosal artery. In 3.6% of thespecimens, the CMA was ori-ented anteriorly and formed aright angle relative to the peri-callosal artery. In another 3.6%of the specimens, the CMA wasoriented upward with an infe-rior convex curve (Fig. 2).
The CMA coursed in the cin-gulate sulcus parallel to the peri-callosal artery in all hemisphereswhere it was present. Together,the 2 vessels were positioned tosupply the superior frontal gyrus,paracentral lobule, cingulate gyrus,corpus callosum, and precuneus.
BranchesThe mean distance from the
origin of the CMA to its firstbranch was 1.28 cm ± 0.89 SD(range, 0.2–4.9 cm). A mean of 3branches ± 1.11 SD (range, 2–6)arose from the CMA (Fig. 3).
Seven main cortical branchescould be identified arising from
the CMA: the orbitofrontal artery, frontopolar artery, anteriorinternal frontal artery, middle internal frontal artery, posteriorinternal frontal artery, paracentral artery, and superior parietalartery. The most consistent branch was the posterior internal frontalartery, which was present in 67.9% of the hemispheres studied(Table 2). The middle internal frontal artery was present in 64.3%of the hemispheres, and the paracentral artery was present in 53.6%.The superior parietal artery and the orbitofrontal artery werebranches of the CMA in only 7.1% and 3.6% of the specimens,respectively. A total of 19 smaller branches (≥0.3 mm) was foundin 14 specimens. Such vessels were classified as cortical branches.
Altogether, the mean diameter of CMA branches was 0.93 mm± 0.33 SD (range, 0.3–1.8 mm) in dissections and 1.31 mm ±0.34 SD (range, 0.7–2.3 mm) in the radiologic analysis. The mid-dle internal frontal artery was usually the most robust branch ofthe CMA, with a mean diameter of 1.14 mm ± 0.23 SD (range,0.8–1.7 mm) in the dissections and of 1.39 mm ± 0.28 SD (range,0.9–2.0 mm) on the DSAs (Table 3). Common trunks arisingfrom the CMA were observed in 14 hemispheres (Figs. 1A and3). The most frequent association in a common trunk was betweenthe middle and posterior internal frontal arteries (42.9%). Otherassociations occurred between the orbitofrontal and frontopolararteries (14.3%); between the anterior and middle internal frontalarteries (14.3%); among the anterior, middle, and posterior inter-nal frontal arteries (7.14%); between the middle and posteriorinternal frontal arteries and the paracentral artery (7.14%); between
TABLE 1. Origin of the Callosomarginal Artery in 30 CadavericHemispheresa
Origin of CMA Percentage of Hemispheres
AComA 10.3%
A2 10.3%
A3
Lower aspect of genu 13.8%
Level of genu 24.1%
Upper aspect of genu 17.2%
A4 24.1%
a CMA; callosomarginal artery; AComA, anterior communicating artery; A2, A3, A4,respective segments of the anterior cerebral artery.
FIGURE 2. Cadaveric photographs showing unusual configurations of the origin of the CMA. A, in this specimen, the CMAarose in an ascendant, posteriorly oriented angle with the pericallosal artery. B, an inferior convex curve, upwardly orientedCMA. C, an anteriorly oriented CMA describing a square angle with the pericallosal artery. D, a superiorly oriented CMAdescribing a square angle with the pericallosal artery. (Used with permission from Barrow Neurological Institute.)
A B
C D

NE UROSURGERY VOLUME 66 | NUMBER 3 | MARCH 2010 | 605
CALLOSOMARGINAL ARTERY
the frontopolar and anterior internal frontal arteries (7.14%); andbetween the posterior internal frontal artery and paracentral artery(7.14%). The branches of the CMA arose from a common trunkwith a frequency of 21.9%.
Clinical Cases (Patients 1–3)Three clinical cases of aneurysms involving the pericallosal-
callosomarginal junction demonstrate how the vascular anatomycan be used to guide endovascular and microsurgical procedures.The first 2 cases underwent endovascular management at the BarrowNeurological Institute (Figs. 4 and 5). The third patient was treatedsurgically at the Bonsucesso General Hospital (Fig. 6).
DISCUSSION
AnatomyEarly studies reported that the CMA occurred in 40% to 56% of
specimens.2,4,18 In recent studies, the CMA was found in as manyas 85% of specimens.1,3,5,17 In the present study, the CMA wasabsent in only 4 hemispheres (6.7%). In these cases, the perical-losal artery alone supplied the anterior two-thirds of the superome-dial surface of the brain (Fig. 7). Instead, the main cortical branchesplus the inferior parietal artery arose from the pericallosal artery.
Moscow et al6 defined the CMA as a vessel coursing in or nearthe cingulate sulcus and giving rise to 2 or more cortical branches.However, as stressed by Ugur et al,5 this definition could lead tothe identification of 2 CMAs. In 5 dissected hemispheres in our
study, 2 vessels fit Moscow’s definition for the CMA (Fig. 1C).In all 5 cases, 1 vessel described a longer course within or near thecingulate sulcus, compared with the other. On the basis of thesefindings, we propose that Moscow’s definition needs an additionalcriterion: when 2 or more vessels match the definition for theCMA, the one with the longer course within or near the cingulatesulcus will be defined as the CMA.
Krayenbühl and Yaşargil19 found that the CMA arose near thegenu of the corpus callosum in 72% of cases. Bogdanović et al17
described the origin of the CMA as being at the level of the genuof the corpus callosum in 81.6% of cases. While studying theanatomic variations of the distal ACA, Ugur et al5 found that theCMA originated from the A3 segment in 64% of hemispheres,from the A2 segment in 18%, from the A4 segment in 12%, andfrom the anterior communicating artery in 6%. These findingsare similar to ours. Rarely, the CMA arises from the A1 segment.20
The variation in the presence and origin of the CMA has yielded2 main definitions for the origin of the pericallosal artery. Snyckersand Drake21 and Stephens and Stilwell22 consider the pericallosalartery as the segment of the ACA distal to the origin of the CMA.Other authors refer to the pericallosal artery as the segment of theACA distal to the anterior communicating artery.1,3,8,23,24
FIGURE 3. Seven main CBs could be identified arising from the CMA: OfA,FpA, AIFA, MIFA, PIFA, PceA, and SParA. This hemisphere illustrates the4 most common main branches of the CMA: the PIFA, PceA, MIFA, andAIFA. The MIFA and PIFA arise from a common trunk. PrCA, pericallosalartery. Used with permission from Barrow Neurological Institute.
TABLE 2. Frequency of Callosomarginal Artery Branches in 56Cerebral Hemispheresa
OfA FpA AIFA MIFA PIFA PceA SParA
3.6% 12.5% 33.9% 64.3% 67.9% 53.6% 7.1%
a OfA, orbitofrontal artery; FpA, frontopolar artery; AIFA, anterior internal frontalartery; MIFA, middle internal frontal artery; PIFA, posterior internal frontal artery;PceA, paracentral artery; SParA, superior parietal artery.
TABLE 3. Mean Diameter of the Callosomarginal Artery in 56Cerebral Hemispheresa
Cadaver Dissections, DSA, CMA Branch Mean (Range) Mean (Range)
(mm) (mm)
Orbitofrontal artery 0.60 0.90
Frontopolar artery 0.93 ± 0.15 (0.8–1.1) 1.0 ± 0.08 (0.9–1.1)
Anterior internal 1.1 ± 0.16 (0.9–1.3) 1.2 ± 0.25 (0.9–1.9)frontal artery
Middle internal 1.14 ± 0.23 (0.8–1.7) 1.39 ± 0.28 (0.9–2.0)frontal artery
Posterior internal 1.04 ± 0.32 (0.3–1.5) 1.31 ± 0.33 (0.7–1.8)frontal artery
Paracentral artery 1.02 ± 0.16 (0.6–1.4) 1.22 ± 0.34 (0.7–1.7)
Superior parietal 1.05 ± 0.21 (0.9–1.2) 1.35 ± 0.26 (1.1–1.6)artery
a CMA, callosomarginal artery. A CMA was found in 29 hemispheres during anatomicdissections and in 27 hemispheres during analysis of 30 angiograms.

606 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com
CAVALCANTI ET AL
The CMA is the widest branch arising from the pericallosal artery.Perlmutter and Rhoton1 found that the mean diameter of the CMAat its origin was 1.8 mm (range, 1.2–1.7 mm). Likewise Ugur et al5found that the mean diameter at its origin was 1.9 mm (range,1.2–3.0 mm). Although both studies reported a slightly larger diam-eter for the CMA than we found in the dissections (1.53 mm),those values are similar to the mean diameter from our radiologicanalysis (2.0 mm). Moreover, the CMA was always the largest branchof the pericallosal artery in all of the hemispheres we dissected.Interestingly, the mean luminal diameter of the CMA and its branchesand of the pericallosal artery measured from the angiograms wasslightly greater than the mean diameter obtained from the speci-mens. The advanced age of the cadaveric specimens could explainthis difference. Indeed, the caliber of vessels elsewhere within thecerebral circulation has been reported to decrease with age.25
Compared with our study, Perlmutter and Rhoton1 also foundthat the origin of the CMA was slightly farther from the anteriorcommunicating artery (mean, 43 mm; range, 12–47 mm). Thecharacteristic deep curve at the beginning of the CMA has alsobeen described in as many as 91.8% of the specimens.17 The pre-dominance of this configuration was less pronounced in our study(60.7%). Instead, we identified a CMA ascending with a posteri-orly oriented angle with the pericallosal artery in one-quarter ofthe hemispheres; this is a configuration more suitable for navi-gating a catheter through the CMA.
Snyckers and Drake21 stated that the typical CMA gives rise tothe anterior, middle, and posterior internal frontal arteries and
terminates as the paracentralart ery. In our study, these last 3branches typically arose fromthe CMA (Table 2). Never -theless, the 7 main branches (theorbitofrontal, frontopolar, ante-rior internal frontal, middleinternal frontal, posterior inter-nal frontal, paracentral, andsuperior parietal arteries1,2,5)usually arise from the CMA orthe pericallosal artery. Perlmutterand Rhoton,1 however, identi-fied these cortical branches asarising more frequently fromthe pericallosal artery than fromthe CMA. They also found that,of the CMAs present, 50% gaverise to 2 major cortical branches,32% gave rise to 3 cortical bran -ches, and 16% gave rise to 4cortical branches. In 1 hemi-sphere, 5 major branches arosefrom the CMA; the middleinternal frontal artery was themost common branch of theCMA. An inferior parietal artery
arising from the CMA was also identified in 1 hemisphere of the50 dissected in that study.1 Ugur et al5 found that the posterior inter-nal frontal and paracentral arteries were the most common branchesof the CMA. They also described an anomalous origin of the arteryof Heubner from the CMA. In another anatomic study, an acces-sory middle cerebral artery originating from the CMA was describedcoursing over the frontal end of the insula. From it originated cor-tical branches to the area supplied by the prefrontal artery.26
PathologyAneurysms arising on the ACA distal to the anterior commu-
nicating artery have a mean incidence of 4.4%.8 More commonly,they occur at the origin of the CMA.8,10,21,27 De Sousa et al8found that 82.4% of 74 distal ACA aneurysms arose from the ori-gin of the CMA. Furthermore, Steven et al10 identified 57% of67 distal ACA aneurysms at this same site.
The reduced dimension of the pericallosal cistern and theapposed medial hemispheric surfaces underlie the tendency ofaneurysms in this region to cause intracerebral hematomas(ICHs).28,29 Snyckers and Drake21 found ICH in 48% of theircases with a distal ACA aneurysm. Sindou et al30 found ICH in47.4% of their series, in which 42.1% of the aneurysms arosefrom the origin of the CMA. Menovsky et al31 found ICH in halfof their series of ruptured pericallosal artery aneurysms.
Others features of aneurysms at this location are their smallsize and their association with multiple aneurysms.8,10,27,29,32,33
Steven et al10 reported that 82% of the distal ACA aneurysms in
FIGURE 4. Patient 1, a 51-year-old woman with a recurrent aneurysm of the pericallosal-callosomarginal junction afterclipping. Angiography showed a large anteroinferiorly oriented aneurysm. The CMA had an anterior convex curve andwas oriented backward and upward. The MIFA, PIFA, and PceA branched from the CMA. Thus, thrombosis and occlu-sion of the parent vessel in this patient could result in ischemic stroke in eloquent areas supplied by these branches. The patientunderwent endovascular treatment of the lesion. Posttreatment angiography confirmed complete obliteration of theaneurysm and patency of the CMA and PrCA. A, digital subtraction angiogram showing a large anteroinferiorly ori-ented aneurysm. B, immediate posttreatment angiogram showing complete occlusion with detachable coils. (Used with per-mission from Barrow Neurological Institute.)
A B

NE UROSURGERY VOLUME 66 | NUMBER 3 | MARCH 2010 | 607
CALLOSOMARGINAL ARTERY
their series were less than 10 mm in diameter. They stressed thata mean of 43% of patients with distal ACA aneurysms harbormultiple aneurysms. In a large series of 470 distal ACA aneurysms,Lehecka et al29 found that 51% of the ruptured aneurysms and 88%of the unruptured aneurysms were smaller than 7 mm. Associatedaneurysms were identified in 52% of the patients, most often onthe middle cerebral artery. On initial computed tomographicscans, they also encountered ICH in 53% of patients, comparedwith 25% of patients with ruptured aneurysms located elsewhere.29
Traumatic intracranial aneurysms are uncommon and representfewer than 1% of all aneurysms.12,13,34,35 They may occur after ablunt or penetrating head injury.7 They are most common in thepediatric population.13,36 The distal ACA is one of the preferred sitesof origin.13,37,38 Nakstad et al39 postulated that shearing forcesbetween the falx, ACAs, and brain during a head injury can leadto the development of aneurysms. Yang et al34 reported 2 CMAaneurysms in a series of 6 traumatic ACA aneurysms that followedblunt craniofacial trauma. In 1 case, the CMA arose from the A4segment. This patient presented with ICH and intraventricularhemorrhage 29 days after the trauma. In the other patient, whowas asymptomatic, the CMA arose from the A3 segment. Baruaet al11 related the development of a traumatic CMA aneurysm aftera penetrating missile head injury. Acute deterioration in the level
of consciousness, seizures, or asustained increase in intra cra -nial pressure after a traumaticbrain injury and a computedtomographic scan demonstratingintracranial hemorrhage shouldjustify angiography to identifytraumatic aneu rysms.13,40
Infectious intracranial aneu -rysms are also uncommon andprimarily affect distal arteries.However, infectious aneurysmsrarely involve the distal ACA.41
In 2 recent studies that togetherincluded 56 infectious aneu -rysms, only 2 aneurysms (3.6%)arose in the distribution of thedistal ACA.42,43
CMA branches can also sup-ply meningiomas at the free edgeof the falx. Consequently, theartery can be used as a route forpreoperative embolization ofintratumoral vessels.16,44 Menin -giomas located elsewhere alongthe course of the CMA can besupplied by this artery,15 andpreoperative devascularizationcan be performed as well. Anarterial feeder arising from theCMA can be catheterized and
occluded most safely if the CMA does not give rise to main corti-cal branches to eloquent areas. Roosen and Lins45 described a pri-mary Ewing sarcoma of the calvaria supplied by the CMA. A rareintracranial mesenchymal chondrosarcoma involving the superiorsagittal sinus and supplied by the CMA has also been reported.46
Occlusion of the CMA can result in a catastrophic condition,depending on the number of branches and which are involved. Acareful analysis of the anatomy and variations on preoperativeangiograms provides evidence about which vessels and corticalareas are at risk. The orbitofrontal artery supplies the olfactorybulb and tract, gyrus rectus, and medial orbitofrontal lobe. Themedial and lateral surfaces of the frontal pole are supplied by thefrontopolar artery.1,47 Disturbance of blood flow in the territory ofthe orbitofrontal and frontopolar arteries from orbitofrontal lobelesions is associated with hand grasping.48 The anterior, middle,and posterior internal frontal arteries supply the superior frontal gyrus.Urinary incontinence can follow injury of the midportion of thesuperior frontal gyrus and anterior cingulate cortex.49 Wheneverthe CMA gives rise to the posterior internal frontal and paracen-tral arteries, its occlusion risks injury to the supplementary motorarea and paracentral lobule.50 Lesions affecting the supplementarymotor area are associated with transient weakness or neglect of thecontralateral side51,52 and the development of speech disorders.48,53
FIGURE 5. Patient 2, a 59-year-old woman with subarach-noid hemorrhage, who was admitted to the emergency room.Angiography showed a superiorly oriented saccular aneurysm
at the pericallosal-callosomarginal junction. The MIFA, PIFA, and PceA branched from the CMA, and the AIFA arosefrom the PrCA. Endovascular treatment with detachable coils occluded the aneurysm completely. A, angiogram showingthe superiorly oriented saccular aneurysm at the pericallosal-callosomarginal junction. B, posttreatment angiogram con-firming complete aneurysmal obliteration and patency of the CMA and PrCA. cCMA, contralateral CMA; cPrCA, con-tralateral PrCA. (Used with permission from Barrow Neurological Institute.)
A B

608 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com
CAVALCANTI ET AL
Mutism and abulia can be associated with injury to this area andto the cingulate gyrus.48,54 Paracentral lobule injuries generateweakness of the contralateral lower extremity.55 Finally, the supe-rior parietal artery helps supply the precuneus gyrus, which, ifdamaged, would place modulation of consciousness at risk.56
Surgical ApproachesAneurysms of the CMA and
distal ACA are typically man-aged through a parasagittal cra -niotomy for an interhemisphericapproach. However, the loca-tion, diameter, and orientationof the aneurysm will determinethe exact position of the cra -niotomy. For aneurysms arisingat the most proximal A2, a mini -supraorbital approach is preferredat our institution.57 At this loca-tion, aneurysms likely arise fromthe origin of the orbito frontal orfrontopolar arteries, given thatthe CMA rarely originates fromA2. De Sousa et al8 suggest abasal frontal para sagit tal cran-iotomy with the head fixed in aneutral position for an interhemi-spheric approach to aneurysmslocated between the anteriorcommunicating artery and thegenu of the corpus callosum.
For A2 aneurysms that arenot amenable to the minisupra-orbital approach and for anyother distal ACA lesions, we
adopt a parasagittal approach and place the craniotomy flap accord-ing to the characteristics and topography of the aneurysm. Thepatient is placed supine on the operating table, the appropriateshoulder is elevated, and the head is placed in the horizontal posi-tion and raised 30 to 45 degrees.58 The interhemispheric fissureis parallel to the ground; therefore, the neurosurgeon’s hands canwork side by side in the same horizontal plane. Moreover, gravityhelps retract the ipsilateral hemisphere. The head is slightly flexedor extended, depending on whether the aneurysm is more distalor proximal, respectively. Because these lesions are primarilyapproached from the right side, the right side is placed down anda quadrangular craniotomy is fashioned with a single burr holeover the superior sagittal sinus. The bone is cut through eitherthe right frontal and/or parietal bone. Our patient 3 was treatedbased on these fundamentals (Fig. 6). Kurtsoy et al59 evaluatedthe applicability of the contralateral interhemispheric approachused with a horizontal head position, as described by Lawtonet al.60 They stressed the benefits of minimizing brain retraction,of obtaining proximal control, and of clipping the neck of theaneurysm without dissecting its dome. When the approach is per-formed through the ipsilateral side, the dome is usually the firstartery-aneurysm structure confronted.59
In a series of 67 patients, Chhabra et al61 reported 28 patientswith distal ACA aneurysms approached through a bifrontal basal ante-rior interhemispheric approach. They concluded that this approach
FIGURE 6. Patient 3, a 46-year-old woman with subarach-noid hemorrhage who had an anterosuperiorly oriented sac-cular aneurysm at the pericallosal-callosomarginal junction.Three main branches arose from the CMA: a common trunkof the AIFA and MIFA, PIFA, and PceA. Inadvertent clip-ping of the parent vessel could have led to a large strokeincluding the superior frontal gyrus, supplementary motorarea, and paracentral lobule. The patient underwent micro-surgical clipping of the aneurysm through an anterior inter-hemispheric approach. Her outcome was uneventful. A,angiogram showing an anterosuperiorly oriented saccularaneurysm at the pericallosal-callosomarginal junction. B,intraoperative photograph, microsurgical view, showing a bilobulated aneurysm in the pericallosal cistern. C, intraoper-ative photograph, microsurgical view, after clipping.
A B
C
FIGURE 7. Cadaveric photograph of a left brain hemisphere illustrating theabsence of the CMA. The PrCA gives rise to the OfA, FpA, AIFA, MIFA,PIFA, PceA, and a common trunk for the SParA and IParA. (Used with per-mission from Barrow Neurological Institute.)

NE UROSURGERY VOLUME 66 | NUMBER 3 | MARCH 2010 | 609
CALLOSOMARGINAL ARTERY
provided the shortest and most direct corridor to such aneurysmswhile facilitating proximal control of the parent A2 segment.
Awareness of the arterial anatomy within the interhemisphericfissure and callosal cistern, together with the angiogram obtainedat the time of the procedure, can help guide the neurosurgeon.Recognizing one major branch of the CMA or pericallosal arteryby its shape, configuration, diameter, and relationship to the othermajor branches will stepwise lead the dissection to the parent ves-sel and aneurysm.
Endovascular SurgeryAlthough endovascular series are small, coiling of distal ACA
aneurysms has evolved. In 1996, Pierot et al62 reported 8 patientswith pericallosal artery aneurysms; endovascular treatment wasattempted in 7 cases. Only in 2 cases were the aneurysms coiledsuccessfully. In 4 cases, the procedure failed. In 3 of these failed cases,the coils protruded into the parent vessel. In 1 case, the aneurysmwas occluded by temporary occlusion of the pericallosal artery.
Six years later Menovsky et al31 reported 12 patients who under-went aneurysm coiling. Initially, complete occlusion was achievedin 11 cases. On 6-month follow-up angiography, only 8 aneurysmsremained completely occluded. Nguyen et al63 reported a recur-rence rate of 52.6% after treating 19 pericallosal aneurysms. Moreover,they stressed that these lesions are associated with a higher rate ofperiprocedural rupture, compared with intracranial aneurysmslocated elsewhere. In 2008, Waldenberger et al64 reported completeocclusion in 93.1% of 29 cases of distal ACA aneurysms. Unlikeprevious reports, they concluded that the endovascular treatment ofthese aneurysms is feasible, safe, and effective. In our patients 1 and2, postoperative angiography confirmed complete occlusion of thepatients’ aneurysms (Figs. 4 and 5).
CONCLUSIONUnderstanding the anatomy of the CMA and its variations is crit-
ical when treating lesions in the interhemispheric region. Manybranches of the pericallosal artery can originate from the CMA.Combined with current technology, the morphometric measure-ments can help endovascular surgeons access lesions located indistal intracranial vessels. We propose an addition to Moscow’sclassic definition of the CMAs. The vessel coursing the longestpathway in or near the cingulate sulcus and otherwise followingthe classic criteria should be considered the CMA. This modifi-cation avoids the dilemma created when 2 or more vessels fit thecriteria established by Moscow et al.6
DisclosureThe authors have no personal financial or institutional interest in any of the
drugs, materials, or devices described in this article.
REFERENCES1. Perlmutter D, Rhoton AL Jr. Microsurgical anatomy of the distal anterior cerebral
artery. J Neurosurg. 1978;49(2):204-228.2. Baptista A. Studies on the arteries of the brain. II. The anterior cerebral artery: some
anatomic features and their clinical implications. Neurology. 1963;13:825-835.
3. Kakou M, Destrieux C, Velut S. Microanatomy of the pericallosal arterial com-plex. J Neurosurg. 2000;93(4):667-675.
4. Ring BA, Waddington MM. Roentgenographic anatomy of the pericallosal arter-ies. Am J Roentgenol Radium Ther Nucl Med. 1968;104(1):109-118.
5. Ugur HC, Kahilogullari G, Esmer AF, et al. A neurosurgical view of anatomicalvariations of the distal anterior cerebral artery: an anatomical study. J Neurosurg.2006;104(2):278-284.
6. Moscow N, Michotey P, Salamon G. Anatomy of the cortical branches of the ante-rior cerebral artery. In: Newton T, Potts D, eds. Radiology of the Skull and Brain:Angiography. Vol 2. St. Louis, MO: CV Mosby; 1974:1411-1420.
7. Parkinson D, West M. Traumatic intracranial aneurysms. J Neurosurg. 1980;52(1):11-20.
8. de Sousa AA, Dantas FL, de Cardoso GT, Costa BS. Distal anterior cerebral arteryaneurysms. Surg Neurol. 1999;52(2):128-135.
9. Mann KS, Yue CP, Wong G. Aneurysms of the pericallosal-callosomarginal junc-tion. Surg Neurol. 1984;21(3):261-266.
10. Steven DA, Lownie SP, Ferguson GG. Aneurysms of the distal anterior cerebral artery:results in 59 consecutively managed patients. Neurosurgery. 2007;60(2):227-234.
11. Barua NU, Ross AH, Sandeman DR. Traumatic callosomarginal aneurysm follow-ing orbital gunshot wound in a 16-year-old girl. Br J Neurosurg. 2007;21(2):237-238.
12. Dubey A, Sung WS, Chen YY, et al. Traumatic intracranial aneurysm: a brief review.J Clin Neurosci 2008;15(6):609-612.
13. Larson PS, Reisner A, Morassutti DJ, Abdulhadi B, Harpring JE. Traumatic intracra-nial aneurysms. Neurosurg Focus. 2000;8(1):e4.
14. Lath R, Vaniprasad A, Kat E, Brophy BP. Traumatic aneurysm of the callosomar-ginal artery. J Clin Neurosci. 2002;9(4):466-468.
15. Lu CS, Chang CN. Hemiparkinsonism in a patient with frontal meningioma. JFormos Med Assoc. 1992;91(12):1216-1218.
16. Urbach H, Solymosi L. Preoperative devascularization of hypervascular tumors.In: Sartor K, ed. Diagnostic and Interventional Neuroradiology: A MultimodalityApproach. Stuttgart, Germany: Thieme; 2003:358-360.
17. Bogdanović D, Marinković S, Teofilovski-Parapid G. The callosomarginal artery.Acta Med Iugosl. 1978;32(3):253-260.
18. Curry R, Culbreth G. The normal cerebral angiogram. Am J Roentgenol RadiumTher. 1951;65(3):345-373.
19. Krayenbühl H, Yaşargil MG. Cerebral Angiography. 2nd ed. New York, NY: ThiemeMedical Publishers; 1968.
20. Krishnamoorthy T, Gupta AK, Bhattacharya RN, Rajesh BJ, Purkayastha S.Anomalous origin of the callosomarginal artery from the A1 segment with an asso-ciated saccular aneurysm. AJNR Am J Neuroradiol. 2006;27(10):2075-2077.
21. Snyckers FD, Drake CG. Aneurysms of the distal anterior cerebral artery. A reporton 24 verified cases. S Afr Med J. 1973;47(39):1787-1791.
22. Stephens R, Stilwell D. Arteries and Veins of the Human Brain. Springfield, IL:Charles C Thomas; 1969.
23. Lin J, Kircheff I. Normal anterior cerebral artery complex. In: Newton T, Potts D,eds. Radiology of the Skull and Brain: Angiography. Vol 2. St. Louis, MO: C.V.Mosby; 1974:1319-1410.
24. Wilson C, Christensen F, Subrahmanian M. Intracranial aneurysms at the perical-losal artery bifurcation. Am Surg. 1965;31:386-393.
25. Padget D. The circle of Willis: its embryology and anatomy. In: Dandy W, ed.Intracranial Arterial Aneurysms. Ithaca, NY: Comstock Publishing Co; 1944.
26. Kahilogullari G, Ugur HC. Accessory middle cerebral artery originating from cal-losomarginal artery. Clin Anat. 2006;19(8):694-695.
27. Hernesniemi JA, Tapaninaho A, Vapalahti MP, Niskanen M, Kari A, LuukkonenM. Saccular aneurysms of the distal anterior cerebral artery and its branches.Neurosurgery. 1992;31(6):994-999.
28. Dandy W. Intracranial Arterial Aneurysms. Ithaca, NY: Comstock Publishing Co;1944.
29. Lehecka M, Lehto H, Niemela M, et al. Distal anterior cerebral artery aneurysms:treatment and outcome analysis of 501 patients. Neurosurgery. 2008;62(3):590-601.
30. Sindou M, Pelissou-Guyotat I, Mertens P, Keravel Y, Athayde AA. Pericallosalaneurysms. Surg Neurol. 1988;30(6):434-440.
31. Menovsky T, van Rooij WJ, Sluzewski M, Wijnalda D. Coiling of ruptured peri-callosal artery aneurysms. Neurosurgery. 2002;50(1):11-15.
32. Ohno K, Monma S, Suzuki R, Masaoka H, Matsushima Y, Hirakawa K. Saccularaneurysms of the distal anterior cerebral artery. Neurosurgery. 1990;27(6):907-913.
33. Yaşargil MG, Carter LP. Saccular aneurysms of the distal anterior cerebral artery.J Neurosurg. 1974;40(2):218-223.

610 | VOLUME 66 | NUMBER 3 | MARCH 2010 www.neurosurgery-online.com
CAVALCANTI ET AL
34. Yang TC, Lo YL, Huang YC, Yang ST. Traumatic anterior cerebral artery aneurysmfollowing blunt craniofacial trauma. Eur Neurol. 2007;58(4):239-245.
35. Yazbak PA, McComb JG, Raffel C. Pediatric traumatic intracranial aneurysms.Pediatr Neurosurg. 1995;22(1):15-19.
36. Buckingham MJ, Crone KR, Ball WS, Tomsick TA, Berger TS, Tew JM Jr. Traumaticintracranial aneurysms in childhood: two cases and a review of the literature.Neurosurgery. 1988;22(2):398-408.
37. Asari S, Nakamura S, Yamada O, Beck H, Sugatani H. Traumatic aneurysm ofperipheral cerebral arteries. Report of two cases. J Neurosurg. 1977;46(6):795-803.
38. Dial D, Maurer GB. Intracranial aneurysms: report of 13 cases. Am J Surg. 1937;35:2-21.
39. Nakstad P, Nornes H, Hauge HN. Traumatic aneurysms of the pericallosal arter-ies. Neuroradiology. 1986;28(4):335-338.
40. Faraji M, Ashrafzadeh F. Penetrating head injuries in children. Neurosurg Q.2005;15:160-163.
41. Holtzman RNN, Brust JC, Hughes JEO, Dickinson PCT. Surgical managementof intracranial aneurysms caused by infection. In: Schmidek H, Sweet W, eds.Schmidek & Sweet Operative Neurosurgical Techniques: Indications, Methods, andResults. Philadelphia, PA: W.B. Saunders; 2000:1302-1327.
42. Chun JY, Smith W, Halbach VV, Higashida RT, Wilson CB, Lawton MT. Currentmultimodality management of infectious intracranial aneurysms. Neurosurgery.2001;48(6):1203-1214.
43. Kannoth S, Iyer R, Thomas SV, et al. Intracranial infectious aneurysm: presenta-tion, management and outcome. J Neurol Sci. 2007;256(1-2):3-9.
44. Yoon YS, Ahn JY, Chang JH, et al. Pre-operative embolisation of internal carotidartery branches and pial vessels in hypervascular brain tumours. Acta Neurochir(Wien). 2008;150(5):447-452.
45. Roosen N, Lins E. Primary Ewing’s sarcoma of the calvarial skull. Neurochirurgia(Stuttg). 1991;34(6):184-187.
46. Cho BK, Chi JG, Wang KC, Chang KH, Choi KS. Intracranial mesenchymalchondrosarcoma: a case report and literature review. Childs Nerv Syst. 1993;9(5):295-299.
47. Kazui S, Sawada T, Naritomi H, Kuriyama Y, Yamaguchi T. Angiographic evalua-tion of brain infarction limited to the anterior cerebral artery territory. Stroke.1993;24(4):549-553.
48. Kumral E, Bayulkem G, Evyapan D, Yunten N. Spectrum of anterior cerebral arteryterritory infarction: clinical and MRI findings. Eur J Neurol. 2002;9(6):615-624.
49. Andrew J, Nathan PW. Lesions on the anterior frontal lobes and disturbances of mic-turition and defaecation. Brain. 1964;87:233-262.
50. Kang SY, Kim JS. Anterior cerebral artery infarction: stroke mechanism and clin-ical-imaging study in 100 patients. Neurology. 2008;70(24 Pt 2):2386-2393.
51. Peraud A, Meschede M, Eisner W, Ilmberger J, Reulen HJ. Surgical resection of gradeII astrocytomas in the superior frontal gyrus. Neurosurgery. 2002;50(5):966-977.
52. Zentner J, Hufnagel A, Pechstein U, Wolf HK, Schramm J. Functional results afterresective procedures involving the supplementary motor area. J Neurosurg.1996;85(4):542-549.
53. Damasio A, Kassel N. Transcortical motor aphasia in relation to lesions of the sup-plementary motor area. Neurology. 1978;28:396-402.
54. Sussman NM, Gur RC, Gur RE, O’Connor MJ. Mutism as a consequence of cal-losotomy. J Neurosurg. 1983;59(3):514-519.
55. Critchley M. The anterior cerebral artery and its syndromes. Brain. 1930;53:120-165.
56. Cavanna AE, Trimble MR. The precuneus: a review of its functional anatomy andbehavioural correlates. Brain. 2006;129(Pt3):564-583.
57. Figueiredo EG, Deshmukh V, Nakaji P, et al. An anatomical evaluation of the mini-supraorbital approach and comparison with standard craniotomies. Neurosurgery.2006;59(4 Suppl 2):ONS212-ONS220.
58. Koos W, Spetzler RF, Lang J. Color Atlas of Microneurosurgery: Microanatomy,Approaches, Techniques, Cerebrovascular Lesions. Stuttgart, Germany: Thieme; 1993.
59. Kurtsoy A, Tucer B, Menku A, Basaslan K, Kemal KR, Akdemir H. Surgical treat-ment of distal anterior cerebral artery aneurysms with horizontal head position.Minim Invasive Neurosurg. 2005;48(5):264-267.
60. Lawton MT, Golfinos JG, Spetzler RF. The contralateral transcallosal approach:experience with 32 patients. Neurosurgery. 1996;39(4):729-735.
61. Chhabra R, Gupta SK, Mohindra S, et al. Distal anterior cerebral artery aneurysms:bifrontal basal anterior interhemispheric approach. Surg Neurol. 2005;64(4):315-320.
62. Pierot L, Boulin A, Castaings L, Rey A, Moret J. Endovascular treatment of peri-callosal artery aneurysms. Neurol Res. 1996;18(1):49-53.
63. Nguyen TN, Raymond J, Roy D, et al. Endovascular treatment of pericallosalaneurysms. J Neurosurg. 2007;107(5):973-976.
64. Waldenberger P, Petersen J, Chemelli A, et al. Endovascular therapy of distal ante-rior cerebral artery aneurysms—an effective treatment option. Surg Neurol.2008;70(4):368-377.
CUSTOMER SERVICE CONTACT INFORMATION
CNS Members: Call Sue Souders at: 301/223-2325.
Non-CNS Members: Call either 301/223-2300 or 1-800/638-3030.
Customer Service fax: 301/223-2400.
Customer Service email: [email protected]