Anatomical Landmarks
32
INTRODUCTION Radiographic recognition of disease requires knowledge of radiographic appearance of normal structures.
-
Upload
drhariomrd -
Category
Documents
-
view
21 -
download
1
description
ppt
Transcript of Anatomical Landmarks

INTRODUCTION
Radiographic recognition of disease requires knowledge of radiographic appearance of normal structures.

RADIOLUCENT LANDMARKS OF MAXILLA
Tooth- Pulp
Periodontal structures Periodontal ligament spaceBone marrow spaces
Incisive foramen
Intermaxillary suture
Nasal fossa
Nasopalatine canals
Lateral fossa
Naso lacrimal canal
Maxillary sinus

RADIOPAQUE LANDMARKS OF MAXILLA
Tooth- Enamel, Dentin
Periodontal structures Cementum, lamina dura ,Trabecular pattern
Anterior nasal spine
Naso labial fold
Zygomatic process of maxilla
Zygomatic arch
Pterygoid plates
Hamulus
Maxillary tuberosity
Nasal septum
Coronoid process
Tooth Anatomy
Teeth are composed primarily of dentin, with an enamel cap over the coronal portion and a thin layer of cementum over the root surface.
Radiographic Appearance of Enamel
ENAMEL appears more radio-opaque than other tissues.
It is 90% mineral causes greator attenuation of X-ray photons.
RADIOGRAPHIC APPEARANCE OF DENTIN
75% mineral content less radiopaque than enamel. Radiopacity similar to bone.
ENAMELODENTINAL JUNCTION appears as a distinct interface separating these two structures.

Radiographic appearance of CEMENTUM 50%mineral content and it appears as a very thin layer on
the root surface. It is usually not so apparent radiographically.
.
Radiographic Appearance of the Pulp
It is composed of soft tissues so it appears radiolucent.
Pulp chambers and root canals extend from the interiors of the chamber till the root apices.
It is seen radiographically also as apical foramen.

ENAMEL
PULP
DENTIN

CERVICAL BURNOUT
Radiographs sometimes show diffuse radiolucent areas with ill defined borders present on the mesial or distal aspects of the teeth in the cervical region.
These regions appear between the edge of the enamel cap and the crest of the alveolar ridge
Perception of these areas is due to contrast with the adjacent ,relatively radiopaque enamel and alveolar –bone.
It should not be confused with root caries which has similar appearance.
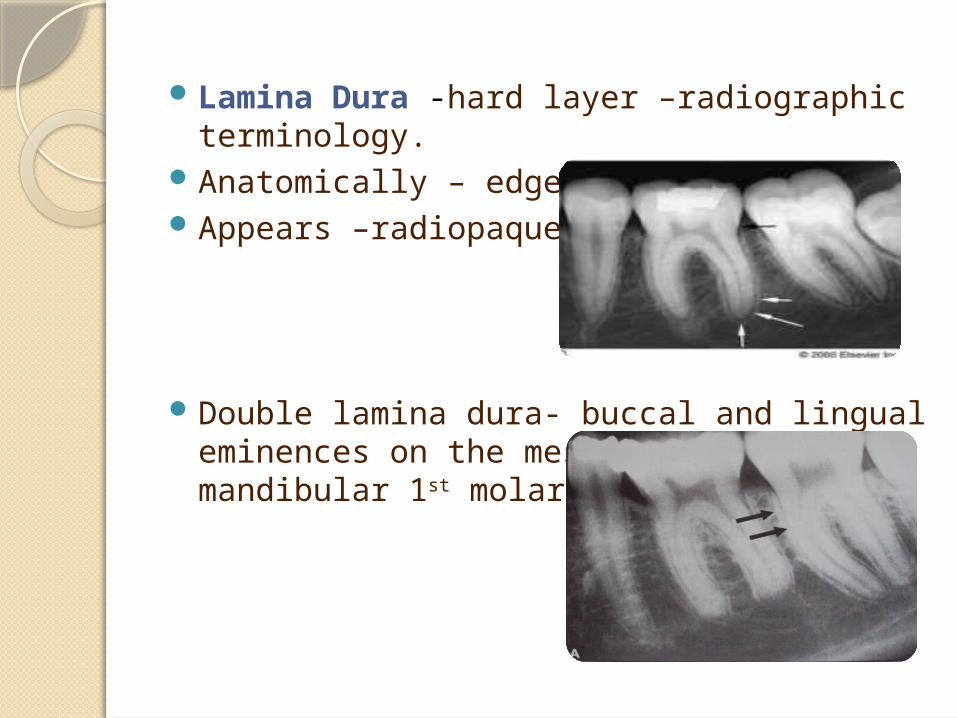
Lamina Dura -hard layer –radiographic terminology.Anatomically – edge of cortical bone.Appears –radiopaque.
Double lamina dura- buccal and lingual eminences on the mesial surface of mandibular 1st molar roots.
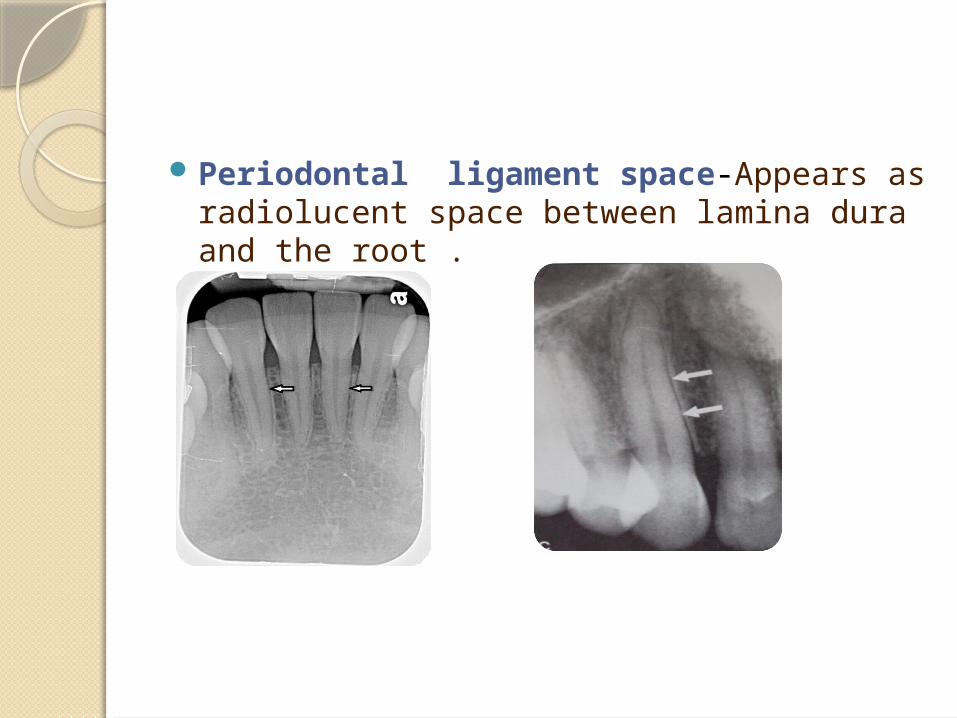
Periodontal ligament space-Appears as radiolucent space between lamina dura and the root .

Alveolar crest- Appears as radiopaque . Normal level-1.5 mm from CEJ . It is the radiopaque gingival margin of the alveolar
process which surrounds the teeth.
Flat proximal tooth surface- Convex tooth surface-
narrow alveolar crest flat alveolar crest

Cancellous bone or Trabecular bone or Spongiosa
Appears as thin radiopaque plates (trabeculae ) surrounding small radiolucent marrow spaces.
Anterior maxilla-mesh or network pattern
Thin ,numerous,fine ,granular ,dense .With smaller marrow spaces and numerous
Posterior maxilla-mesh or network pattern
Similar to anterior maxilla with marrow spaces slightly larger

Anterior mandible- (Trajectory pattern)(Stepladder pattern-central incisors)
Thicker ,coarser .oriented more horizontally .fewer with large marrow spaces
Posterior mandible-Trajectory pattern or linear pattern)(Stepladder pattern-1st molar)
Comparable to anterior mandible ,with larger marrow spaces ,sparse trabeculation inferiorly.

RADIOLUCENT LANDMARKS OF MAXILLA Intermaxillary suture/Median maxillary suture/Mid
pallatine sutureAppears between two portions of premaxilla May terminate as V shape widening at alveolar crest

Incisive foramen or Nasopalatine or Anterior palatine foramen –
Location-behind maxillary central incisorsSize –varies- 2mm – 1cm or more
Average-3*3 mm
Normal limits- <6 mm Shape-varies-slit like, round ,oval ,heart shape ,diamond
shape
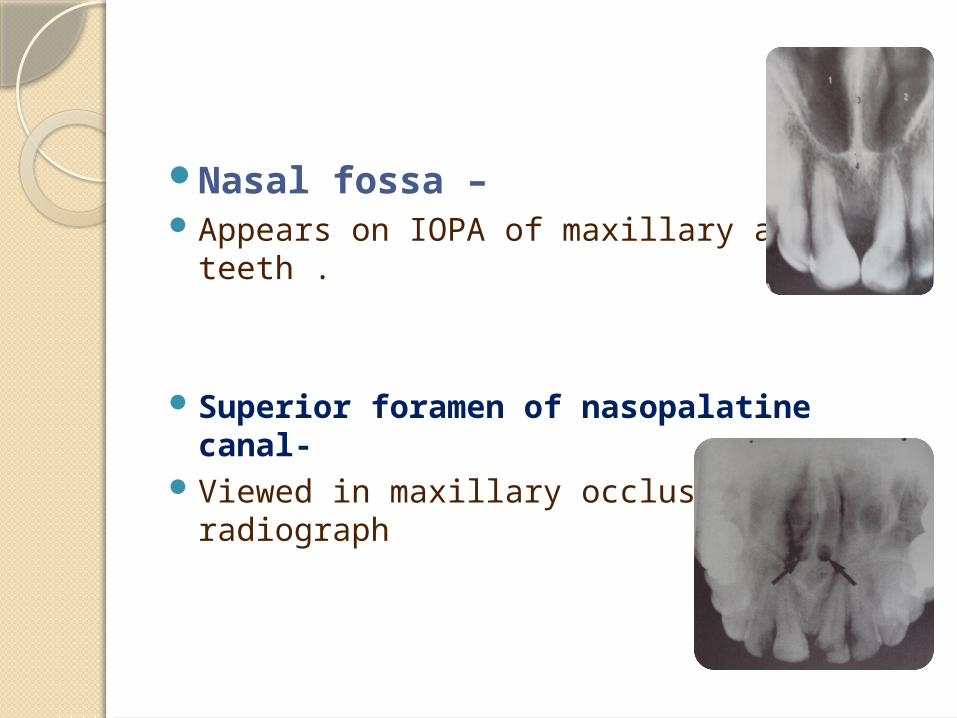
Nasal fossa –Appears on IOPA of maxillary anterior teeth .
Superior foramen of nasopalatine canal-Viewed in maxillary occlusal radiograph
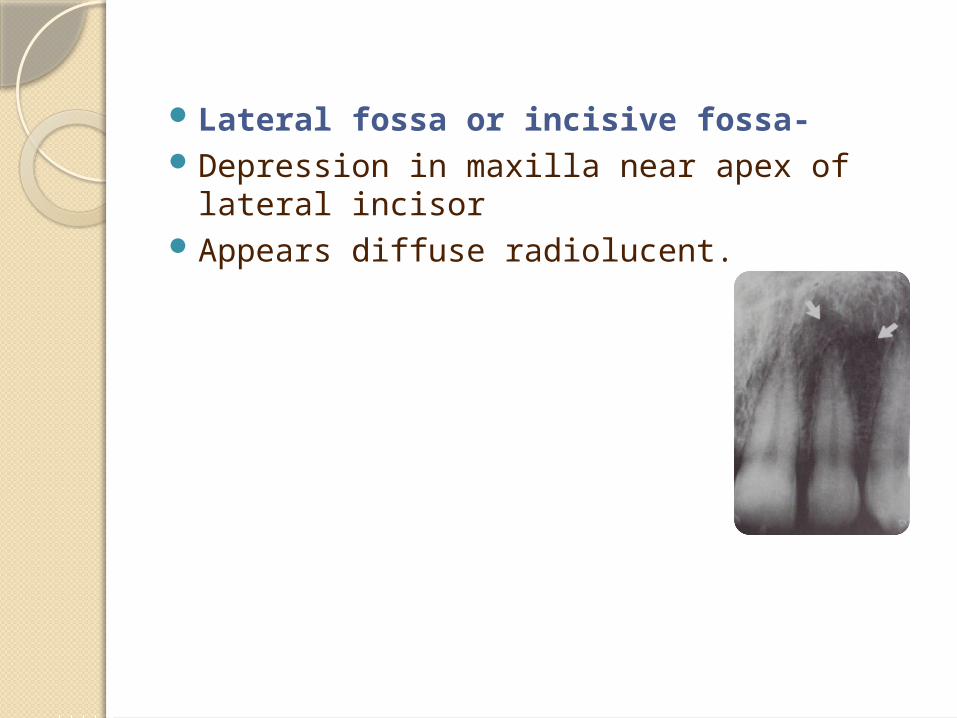
Lateral fossa or incisive fossa- Depression in maxilla near apex of lateral incisor Appears diffuse radiolucent.

Nasolacrimal canal –
Commonly seen in occlusal films.Oval shaped in the region of molars.
Occlusal radiograph
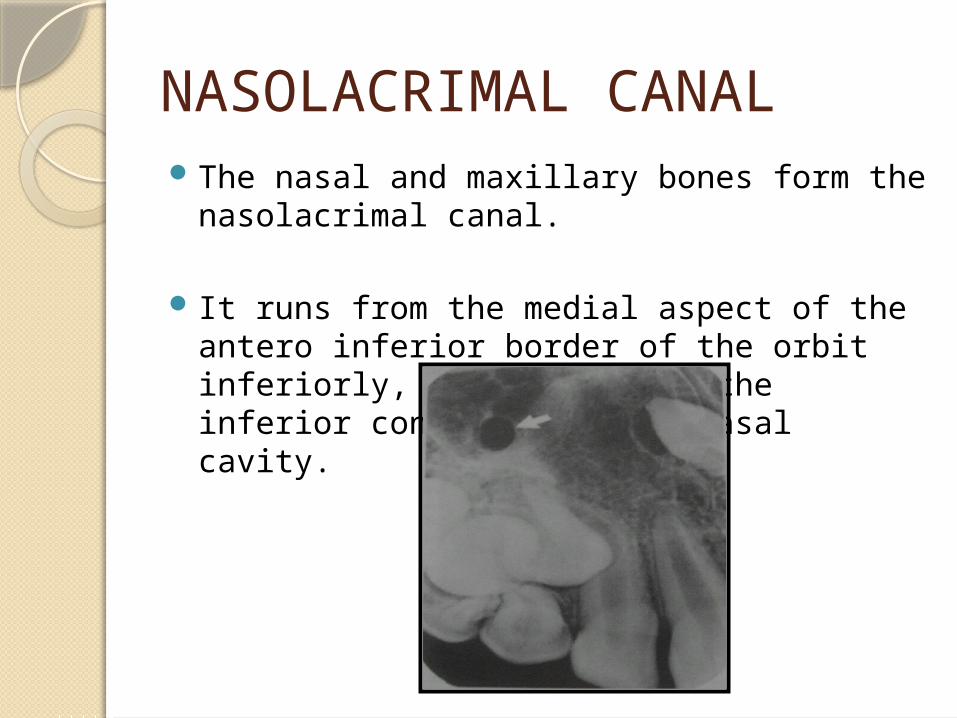
NASOLACRIMAL CANALThe nasal and maxillary bones form the
nasolacrimal canal.
It runs from the medial aspect of the antero inferior border of the orbit inferiorly, to drain under the inferior conchae into the nasal cavity.

RADIOGRAPHIC FEATURES OF MAXILLARY SINUSMAXILLARY SINUS is an air containing cavity
lined by mucous membrane.Appears as the three sided pyramid .
Base -formed by mesial wall adjacent to nasal cavity.
Apex –extending laterally into the zygomatic process of maxilla.

Maxillary sinus /Antrum
Floor of maxillary sinus Small maxillary sinus does not appear on radiograph
Maxillary sinus extending into alveolar bone Large maxillary sinus extending int maxillary
tuberosity area

Inverted Y
Formed by bony structures between Formed by anterior wall of maxillary
maxillary sinus and nasal cavity sinus and floor of nasal fossa
RADIOPAQUE LANDMARKS OF MAXILLA
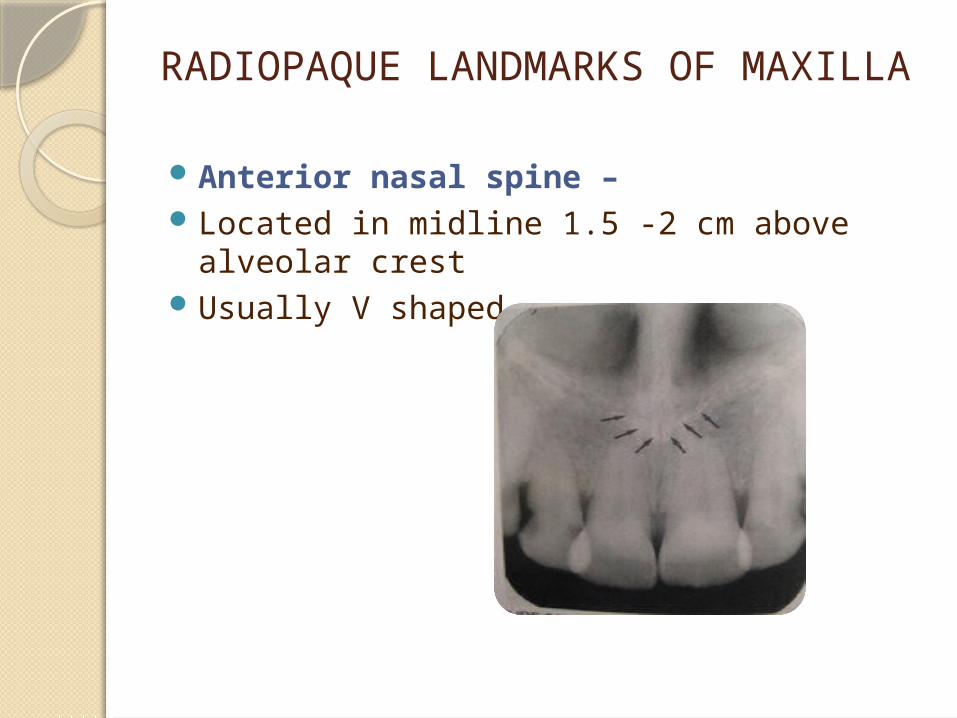
Anterior nasal spine –Located in midline 1.5 -2 cm above alveolar crestUsually V shaped .
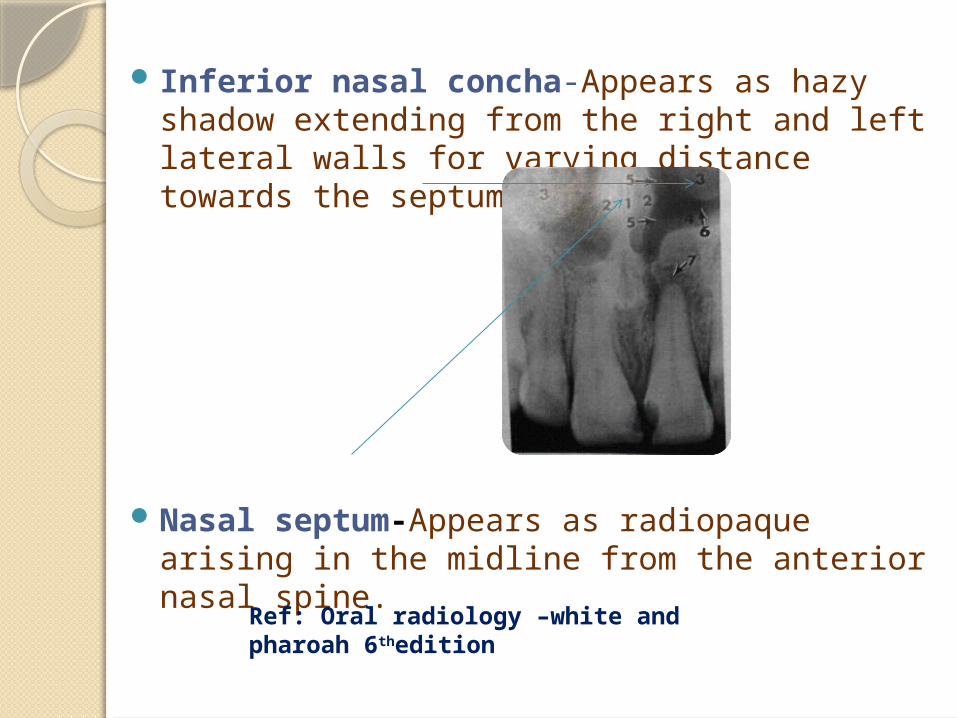
Inferior nasal concha-Appears as hazy shadow extending from the right and left lateral walls for varying distance towards the septum
Nasal septum-Appears as radiopaque arising in the midline from the anterior nasal spine.
Ref: Oral radiology –white and pharoah 6thedition
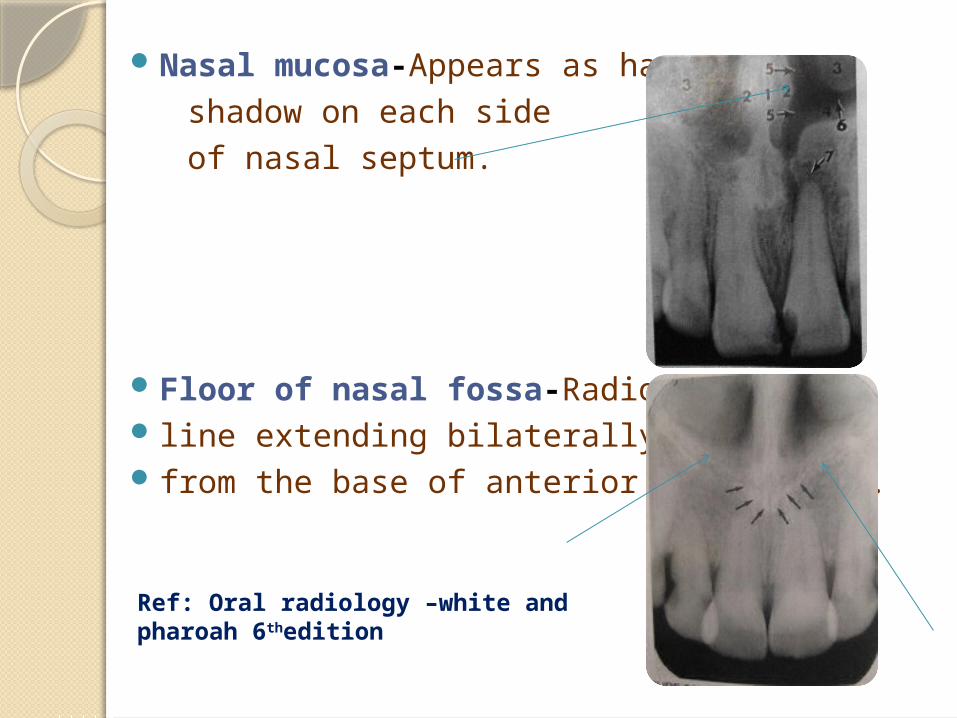
Nasal mucosa-Appears as hazy
shadow on each side
of nasal septum.
Floor of nasal fossa-Radiopaque line extending bilaterally away from the base of anterior nasal spine.
Ref: Oral radiology –white and pharoah 6thedition

Nasolabial fold –Appears in canine –premolar region
Shadow of tip of noseAppears over roots of central incisors
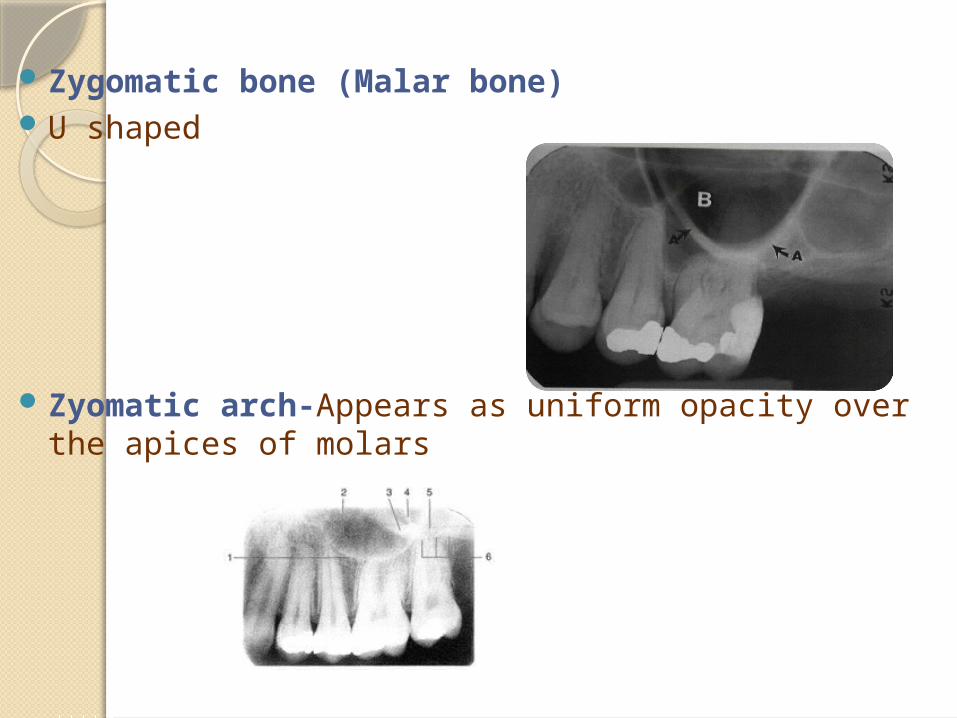
Zygomatic bone (Malar bone)U shaped
Zyomatic arch-Appears as uniform opacity over the apices of molars
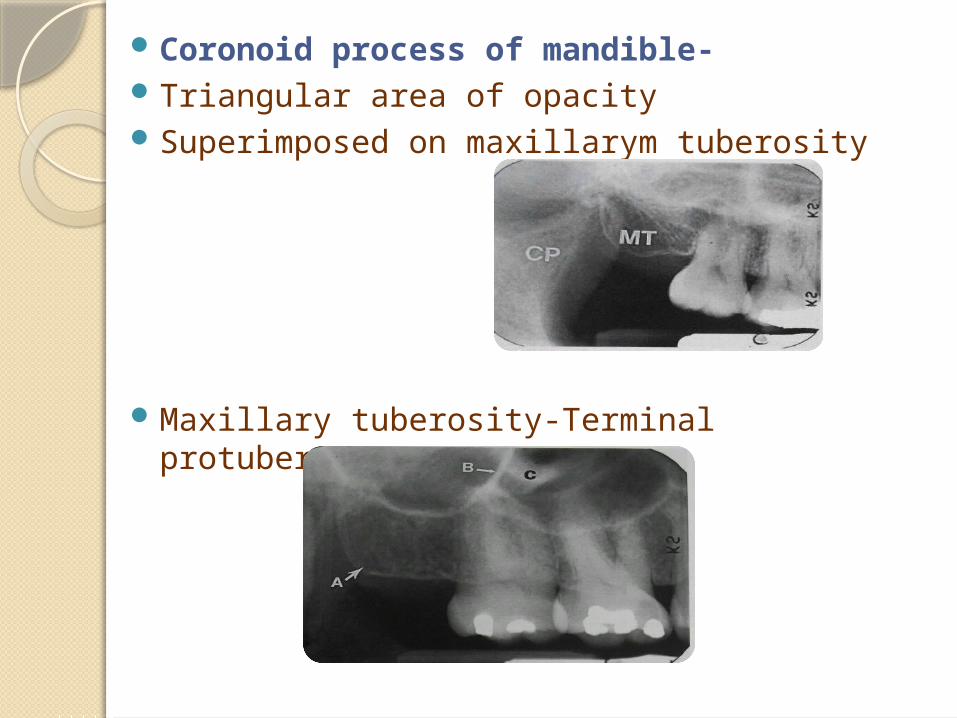
Coronoid process of mandible-Triangular area of opacity Superimposed on maxillarym tuberosity
Maxillary tuberosity-Terminal protuberance

Pterygoid plates-Lies immediately posterior to tuberosity of maxilla Hamular process-extends inferiorly from medial
pterygoid plate.
CONCLUSIONA good diagnosis mandateed appreciation of a wide
range of variation in the appearance of normal structures
Most patients demonstrates many of the normal radiological landmarks , but it is a rare patient who shows them all .
Hence absence of one or several landmarks in any individual should not be necessarily considered abnormal.
REFERENCESText book of dental and maxillofacial radiology-
karjodhkar 2nd editionOral radiology –white and pharoah 6th editionEssentials of dental radiography and radiology-Eric
Whites 4th edition








![Ultrasound guidance versus anatomical landmarks for ...€¦ · [Intervention Review] Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization Patrick](https://static.fdocuments.in/doc/165x107/5f9beef95154c7333f47d212/ultrasound-guidance-versus-anatomical-landmarks-for-intervention-review-ultrasound.jpg)