
Analysis of reported randomized trials of streptokinase therapy for acute myocardial infarction in...
4
Analysis of Reported Randomized Trials of Streptokinase Therapy for Acute Myocardial Infarction in the 1980s BHARAT PATEL, MD, and ROBERT A. KLONER, MD, PhD Trials of intracoronary (C) and intravenous (IV) streptoklnase (SK) therapy for myocardial infarction have shown variable effects on mortality and left ventricular (LV) function. A pooled analysis of 10 randomized trials invofving a total of 14,355 pa- tients was performed to lad< for overall trends in the change in mortalfty within 6 weeks (group A) and after 6 weeks (group B) of follow-up, and the change in LV function. All 10 trials, 7 with IC and 3 wlth IV SK, were randomized after 1960. There was a significant reduction In mortality risk in patients in group A treated with IV SK (pooled odds ratio = 0.61, 95% co&fence interval = 0.73 to 0.90, p <O.OOl). In contrast, no significant differences in mortality were detected in patients in group B treat- ed wtth IV SK or in patients in either group treated with IC SK. Two IV SK trials that prospectively strat- ified patient population according to duration of symptoms showed a greater reduction in mortality with adminfstratfon of SK therapy within 3 hours of onset of symptoms. Analysis of LV function was performed before, within 96 hours after and 1 to 4 weeks after SK therapy. Only 2 of 7 IC SK trials showed signiticantly greater improvement in global LV ejection fraction in SK group compared with a control group, both showfng improvement in LV function between early and late after treatment. Thus, IV SK therapy signifffantty reduces short-term rff of death after acute myocardial infarction; 2 trf- als show a greater reduction in mortaltty risk with earlier instkution of IV SK therapy. (Am J Cardiol 1967;59:501-504) D espitethe conflicting valuesof left ventricular (LV) function and mortality ratesin recentrandomized tri- als of thrombolytic therapy for acute myocardial in- farctionl-I5 this mode of treatmentis becoming widely accepted in clinical practice. However, useof intracor- onary (IC) thrombolytic therapy is logistically limited by its substantial financial and technologicdemands. Thus, some trials have too few patients to permit a judgment about the beneficial effects of this therapy. We performed a pooled analysisof 10trial&l5 of IC or intravenous(IV) streptokinase (SK) therapy for acute myocardial infarction published after 1980to review trends in survival and LV function. Methods A retrospective review of 10randomizedcontrolled trial.+5 published between January 1981and June 1986 was performed to analyzetrendsin the effectsof From the Department of Internal Medicine and Division of Car- diology, Wayne State University School of Medicine and Harper Hospital, Detroit, Michigan. Manuscript received April 7, 1986; revised manuscript received August 33,1986, accepted August Z&1986. Address for reprints: Robert A. Kloner, MD, PhD, Division of Cardiology, Harper Hospital, 3990 John R Street, Detroit, Michi- gan 48201. 501 IC or IV SK therapy on mortality rate and LV function after acute myocardial infarction. The information about these trials was obtained from Medlars, the computerizedliterature retrival service of the Nation- al Library of Medicine, Bethesda, and Index Medicus, a bibliography of medical references from the U.S. Department of Health and Human Services, National Institutes of Health, Bethesda. Because management of acute myocardial infarction has undergonesignifi- cant changes in recent years, trials published in the 1960s and 1970s were not included in this analysis. To increase comparability among the trials ana- lyzed, the following approach was undertaken. (1) Tri- als with a clearly defined endpoint of mortality were separated into 2groups. Group A included trials with a follow-up of 6 weeks or less; group B included trials with more than 6 weeks follow-up. (21 An early assess- ment of LV function was subgroupedaccording to whether it was measuredbefore or within 96 hours after SK therapy. When the trials assessed mortality resultswithin 6 weeks and after 6 weeks,2~3~5~6~g,10,1z~15 the analysiswas carried out by including thesedata both in groupsA and B. Assessment of mortality was done by calculating pooled oddsratio and 95% confidence interval by the Mantel-HaenszeP and WoolP7 methods, respective-
-
Upload
bharat-patel -
Category
Documents
-
view
213 -
download
0
Transcript of Analysis of reported randomized trials of streptokinase therapy for acute myocardial infarction in...

Analysis of Reported Randomized Trials of Streptokinase Therapy for Acute Myocardial Infarction in the 1980s
BHARAT PATEL, MD, and ROBERT A. KLONER, MD, PhD
Trials of intracoronary (C) and intravenous (IV) streptoklnase (SK) therapy for myocardial infarction have shown variable effects on mortality and left ventricular (LV) function. A pooled analysis of 10 randomized trials invofving a total of 14,355 pa- tients was performed to lad< for overall trends in the change in mortalfty within 6 weeks (group A) and after 6 weeks (group B) of follow-up, and the change in LV function. All 10 trials, 7 with IC and 3 wlth IV SK, were randomized after 1960. There was a significant reduction In mortality risk in patients in group A treated with IV SK (pooled odds ratio = 0.61, 95% co&fence interval = 0.73 to 0.90, p <O.OOl). In contrast, no significant differences in mortality were detected in patients in group B treat- ed wtth IV SK or in patients in either group treated
with IC SK. Two IV SK trials that prospectively strat- ified patient population according to duration of symptoms showed a greater reduction in mortality with adminfstratfon of SK therapy within 3 hours of onset of symptoms. Analysis of LV function was performed before, within 96 hours after and 1 to 4 weeks after SK therapy. Only 2 of 7 IC SK trials showed signiticantly greater improvement in global LV ejection fraction in SK group compared with a control group, both showfng improvement in LV function between early and late after treatment. Thus, IV SK therapy signifffantty reduces short-term rff of death after acute myocardial infarction; 2 trf- als show a greater reduction in mortaltty risk with earlier instkution of IV SK therapy.
(Am J Cardiol 1967;59:501-504)
D espite the conflicting values of left ventricular (LV) function and mortality rates in recent randomized tri- als of thrombolytic therapy for acute myocardial in- farctionl-I5 this mode of treatment is becoming widely accepted in clinical practice. However, use of intracor- onary (IC) thrombolytic therapy is logistically limited by its substantial financial and technologic demands. Thus, some trials have too few patients to permit a judgment about the beneficial effects of this therapy. We performed a pooled analysis of 10 trial&l5 of IC or intravenous (IV) streptokinase (SK) therapy for acute myocardial infarction published after 1980 to review trends in survival and LV function.
Methods A retrospective review of 10 randomized controlled
trial.+5 published between January 1981 and June 1986 was performed to analyze trends in the effects of
From the Department of Internal Medicine and Division of Car- diology, Wayne State University School of Medicine and Harper Hospital, Detroit, Michigan. Manuscript received April 7, 1986; revised manuscript received August 33,1986, accepted August Z&1986.
Address for reprints: Robert A. Kloner, MD, PhD, Division of Cardiology, Harper Hospital, 3990 John R Street, Detroit, Michi- gan 48201.
501
IC or IV SK therapy on mortality rate and LV function after acute myocardial infarction. The information about these trials was obtained from Medlars, the computerized literature retrival service of the Nation- al Library of Medicine, Bethesda, and Index Medicus, a bibliography of medical references from the U.S. Department of Health and Human Services, National Institutes of Health, Bethesda. Because management of acute myocardial infarction has undergone signifi- cant changes in recent years, trials published in the 1960s and 1970s were not included in this analysis.
To increase comparability among the trials ana- lyzed, the following approach was undertaken. (1) Tri- als with a clearly defined endpoint of mortality were separated into 2 groups. Group A included trials with a follow-up of 6 weeks or less; group B included trials with more than 6 weeks follow-up. (21 An early assess- ment of LV function was subgrouped according to whether it was measured before or within 96 hours after SK therapy.
When the trials assessed mortality results within 6 weeks and after 6 weeks,2~3~5~6~g,10,1z~15 the analysis was carried out by including these data both in groups A and B.
Assessment of mortality was done by calculating pooled odds ratio and 95% confidence interval by the Mantel-HaenszeP and WoolP7 methods, respective-

502 STREPTOKINASE THERAPY IN THE ’80s
ly. In these methods, when a pooled odds ratio, i.e., a pooled estimate of the odds ratios [odds of a patient dying in a treatment group/odds of a patient dying in a control group) from various analyzed trials, is less than 1.0, it implies a favorable effect of treatment in terms of reducing risk of death. Generally, when both the pooled odds ratio and 95% confidence interval are less than 1.0, the reduction in risk of death is significant (p <0.05).
LV functional changes are shown in graphs that illustrate mean global LV eiection fraction results be- fore and early akd late (1 to-4 weeks after SK) after SK therapy.
Results All 10 trials, 7 IC1-12 and 3 IV,19-15 started random-
ization after 1980 (confirmed by personal communica- tion) and collectively randomized the 14,335 patients included in this analysis. Mean duration of symptoms before randomization was less than 6 hours in all 10 trials.
Mortality results in intravenous streptolcinase tri- als: Results of analysis of mortality from 3 IV SK tri- al+‘5 revealed a significant reduction in risk of mor- tality in IV SK group A (n = 13,505, pooled odds ratio = 0.81,95% confidence interval = 0.73 to 0.90, p <O.OOl) (Fig. 1). Only 1 IV S,K trial had mortality results avail- able after 6 weeks of follow-up15 (group B, n = 52;
pooled odds ratio = 0.83, 95% confidence interval = 0.22 to 3.12, difference not significant [NS]) (Fig. 1). Mean duration of follow-up was 2 to 3 weeks in group A and 56 weeks in group B.
Left ventricular function results in intravenous streptokinase trials: Two14J5 of the 3 IV SK trials as- sessed LV function in SK and control groups. One trial14 showed a significantly higher global LV ejection fraction in the SK group (56.8 f 0.7, n = 428) than the control group (53.9 f 0.770, n = 420) 3 weeks after SK therapy (p <0.005). In contrast, another trial15 revealed no significant difference in global LV ejection fraction between SK and control groups early or late after ther- apy (SK group: early 44 f 15%) late = 44 f 16%. n = 21; controlgroup: early42 f 1370, late = 43 f 135'0, n = 16).
Mortality results in intracoronary streptokinase trials: Because fewer patients were included in IC SK trials, 95% confidence intervals were wider; however, there was a trend toward (Fig. 1) a lower mortality risk in both IC SK groups A (n = 810, pooled odds ratio = 0.80,95% confidence interval = 0.48 to 1.33) and B (n = 803; pooled odds ratio = 0.77; 95% confidence interval = 0.51 to 1.17) (NS). Duration of follow-up varied from 2 to 6 weeks in group A and 26 to 104 weeks in group B.
Left ventricular function results in intracoronary streptokinase trials: All 7 IC SK trials assessed global LV ejection fraction in SK and control groups. Of these, only 2 trials 2~10 showed a significant improve-
4 REDUCTION-[ -f INCREASE IN MORTALITY t
IC SK56 WEEKS (n = 610 )
KENNEDY’ I ! ANDERSON’ fe i
4 I 5.8
RAIZNER 4 I SlMOONS6
/w+115.4
I I I
KHAJA’ t I /+ 5.7
AENTROP ” I
I I j+ 10.3
OVERALL RESULT
IC SK=-6 WEEKS (n=603)
KENNEDY 6 I 1 3 i
ANDERSON 3 I I 4 RENTROP” C pm<-- 6.4
KHAJA’ LEIEOFF ’ ,)(,L-- 6.6
SIMOONS I6 I I I I
OVERALL RESWT
IV SK 5 6 WEEKS (n=13505)
GISSI l3 H-l SAM l4 1
OLSON I5 I
t It ’ I
OVERALL RESULT w
Iv SK =- 6 MEKS (n=52)
OLSON I5 I I I i
I ’ 1 1 1 I I II I I I1 I I,
0 0.2 0.6 1.0 1.4 1.6 2.2 2.6 3.0 ODDS RATIO AND 95 % CONFIDENCE INTERVALS
j-4.0
KEY
I ODDS RATIO 1 4 - 95 “‘0 CONFIDENCE-
INTERVAL
FIGURE 1. Odds ratio and 95 ‘36 contldence intervals for mortality data In 10 randomized trials. Note the overall reduction In risk of mortallty (p <O.OOl) wlthln 6 weeks of follow-up In Intravenous (IV) streptoklnase (SK) trials. IC = Intracoronary.
March 1, 1987 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 59 503
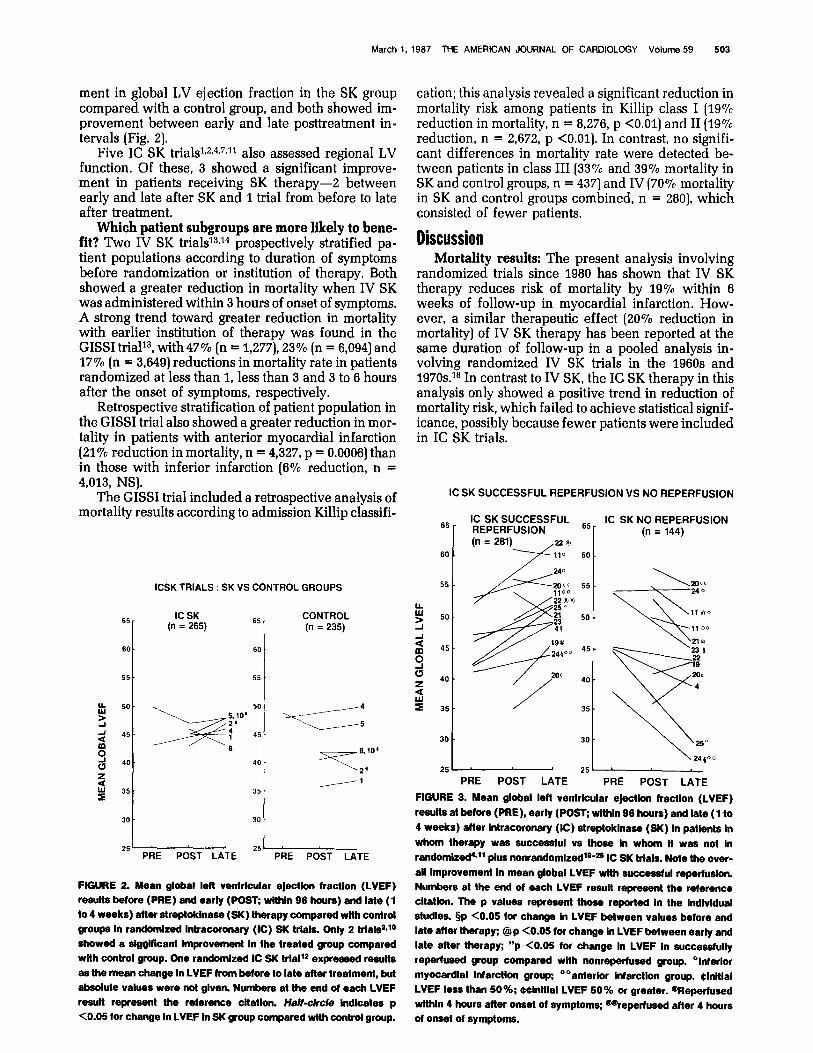
ment in global LV ejection fraction in the SK group compared with a control group, and both showed im- provement between early and late posttreatment in- tervals (Fig. 21.
Five IC SK trials1J,4,7J1 also assessed regional LV function. Of these, 3 showed a significant improve- ment in patients receiving SK therapy-3 between early and late after SK and 1 trial from before to late after treatment.
Which patient subgroups are more likely to hene- fit? Two IV SK tria1s13J4 prospectively stratified pa- tient populations according to duration of symptoms before randomization or institution of therapy. Both showed a greater reduction in mortality when IV SK was administered within 3 hours of onset of symptoms. A strong trend toward greater reduction in mortality with earlier institution of therapy was found in the GISSI trial13, with 47% (n = 1,277), 23% (n = 6,094) and 17% (n = 3,649) reductions in mortality rate in patients randomized at less than 1, less than 3 and 3 to 6 hours after the onset of symptoms, respectively.
Retrospective stratification of patient population in the GISSI trial also showed a greater reduction in mor- tality in patients with anterior myocardial infarction (21% reduction in mortality, n = 4,327, p = 0.0006) than in those with inferior infarction (6% reduction, n = 4,013, NS).
The GISSI trial included a retrospective analysis of mortality results according to admission Killip classifi-
ICSK TRIALS : SK VS CONTROL GROUPS
65 IC SK
I
(n = 265) 65 CONTROL
I
(n = 235)
60 60
25( 25: PRE POST LATE PRE POST LATE
FIGURE 2. Mean global left ventricular ejectlon fraction (LVEF) results before (PRE) and early (WST; wlthln g6 hours) and late (1 to 4 weeks) after streptoklnase (SK) therapy compared with control groups In randomlzed lntracoronary (IC) SK trials. Only 2 trlal#~10 showed a slgglflcant Improvement In the treated group compared with control group. One randomized IC SK trIalI expressed results as the mean change In LVEF from before to late after treatment, but absolute values were not glven. Numbers at the end of each LVEF result represent the reference cltatlon. Ha/f-circle Indicates p <0.05 for change In LVEF In SK group compared wlth control group.
cation; this analysis revealed a significant reduction in mortality risk among patients in Killip class I (1970 reduction in mortality, n = 8,276, p <O.Ol) and II (19% reduction, n = 2,672, p <O.Ol). In contrast, no signifi- cant differences in mortality rate were detected be- tween patients in class III (33% and 39% mortality in SK and control groups, n = 437) and IV (70% mortality in SK and control groups combined, n = 2801, which consisted of fewer patients,
Discussion Mortality results: The present analysis involving
randomized trials since 1980 has shown that IV SK therapy reduces risk of mortality by 19% within 6 weeks of follow-up in myocardial infarction. How- ever, a similar therapeutic effect (20% reduction in mortality) of IV SK therapy has been reported at the same duration of follow-up in a pooled analysis in- volving randomized IV SK trials in the 1960s and 197Os.l* In contrast to IV SK, the IC SK therapy in this analysis only showed a positive trend in reduction of mortality risk, which failed to achieve statistical signif- icance, possibly because fewer patients were included in IC SK trials.
IC SK SUCCESSFUL REPERFUSION VS NO REPERFUSION
65 IC SK SUCCESSFUL 65 IC SK NO REPERFUSION
(n = 144)
60
55
30
25 PRE POST LATE PRE POST LATE
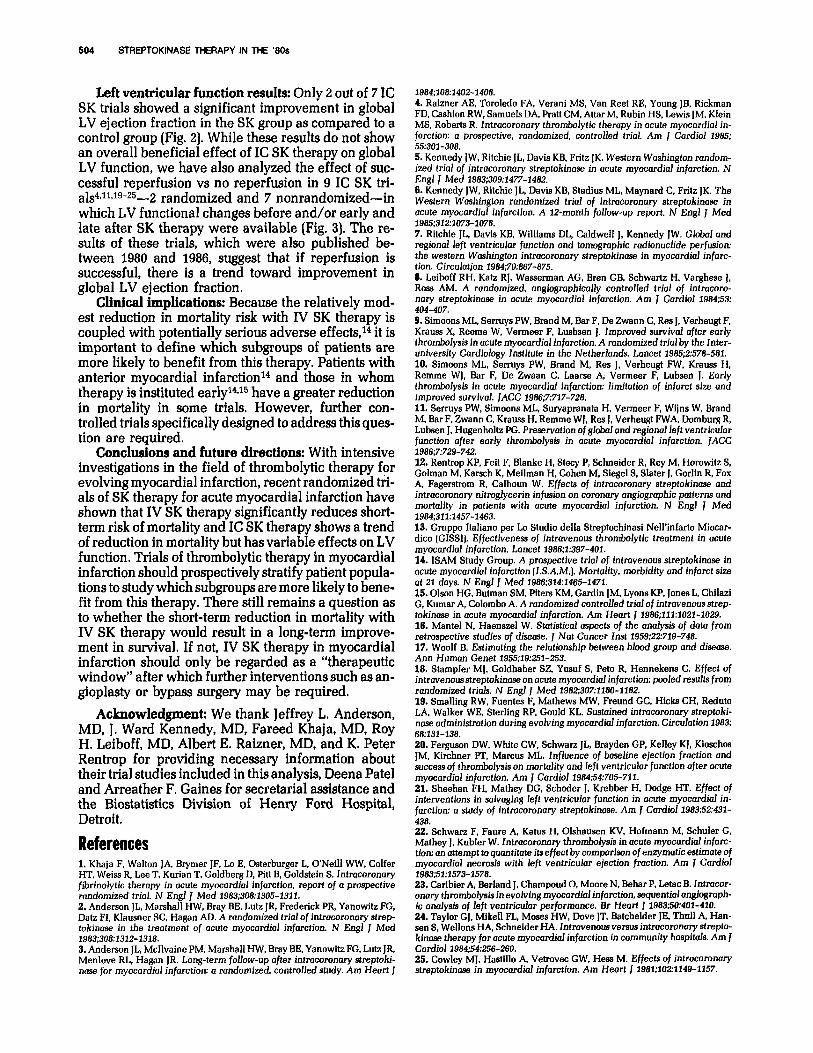
FIGURE 3. Mean global lefl ventricular ejection fraction (LVEF) results at before (PRE), early (POST; within 96 hours) and late (1 to 4 weeks) after lntracoronary (C) streptoklnase (SK) In patlents In whom therapy was successful vs those In whom It was not In randomlred’*ll plus nonrandomlzedle-B IC SK trials. Note the over- all Improvement In mean global LVEF wlth successful reperluslon. Numbers at the end of each LVEF result represent the reference cltatlon. The p values represent those reported In the lndlvldual studies. §p <0.05 for change In LVEF between values before and late after therapy: @p CO.05 for change In LVEF between early and late after therapy; “p <0.05 for change In LVEF In successfully reperfused group compared with nonreperfused group. “lnferlor myocardlal lnfarctlon group; o”anterlor Infarction group. Clnltlal LVEF less than 50%; Wnltlal LVEF 50% or greater. @l?epetfused wlthln 4 hours after onset of symptoms; qeperfused after 4 hours of onset of symptoms.
504 STREPTOKINASE THERAPY IN THE ’80s
Left ventricular function results: Only 2 out of 7 IC SK trials showed a significant improvement in global LV ejection fraction in the SK group as compared to a control group (Fig. 2). While these results do not show an overall beneficial effect of IC SK therapy on global LV function, we have also analyzed the effect of suc- cessful reperfusion vs no reperfusion in 9 IC SK tri- a1s4~11~19-25-.2 randomized and 7 nonrandomized-in which LV functional changes before and/or early and late after SK therapy were available (Fig. 3). The re- sults of these trials, which were also published be- tween 1980 and 1986, suggest that if reperfusion is successful, there is a trend toward improvement in global LV ejection fraction.
Clinical implications: Because the relatively mod- est reduction in mortality risk with IV SK therapy is coupled with potentially serious adverse effects,14 it is important to define which subgroups of patients are more likely to benefit from this therapy. Patients with anterior myocardial infarctionI and those in whom therapy is instituted early14e15 have a greater reduction in mortality in some trials. However, further con- trolled trials specifically designed to address this ques- tion are required.
Conclusions and future directions: With intensive investigations in the field of thrombolytic therapy for evolving myocardial infarction, recent randomized tri- als of SK therapy for acute myocardial infarction have shown that IV SK therapy significantly reduces short- term risk of mortality and IC SK therapy shows a trend of reduction in mortality but has variable effects on LV function. Trials of thrombolytic therapy in myocardial infarction should prospectively stratify patient popula- tions to study which subgroups are more likely to bene- fit from this therapy. There still remains a question as to whether the short-term reduction in mortality with IV SK therapy would result in a long-term improve- ment in survival. If not, IV SK therapy in myocardial infarction should only be regarded as a “therapeutic window” after which further interventions such as an- gioplasty or bypass surgery may be required.
Acknowledgment: We thank Jeffrey L. Anderson, MD, J. Ward Kennedy, MD, Fareed Khaja, MD, Roy H. Leiboff, MD, Albert E. Raizner, MD, and K. Peter Rentrop for providing necessary information about their trial studies included in this analysis, Deena Pate1 and Arreather F. Gaines for secretarial assistance and the Biostatistics Division of Henry Ford Hospital, Detroit.
References 1. KhaJa F, Walton ]A, Brymer JF, Lo E, Osterburger L. O’Nelll WW. Colfer HT. Weiss R, Lee T, Kurlan T, Goldberg D, Pitt B, Goldstein S. Intracoronary fibrinolytic therapy in acute myocardial infarction. report of a prospective randomized trial. N Engl f Med 1983;308:1305-1311. 2. Anderson IL. Marshall HW. Brav BE. Lutz IR. Frederick PR. Yanowitz FG. Datz FI, Kla&er SC, Hagan AD. A randomized trial of introcoronary strep- tokinase in the treatment of acute myocardial infarction. N Engl J Med 1983:308:1312-1318. 3. Anderson IL. McIlvaine PM, Marshall HW. Bray BE. Yanowitz FG, Lutz JR, Menlove RL; Hagan JR. Long-term follow-up after intracomnary streptoki- nase for myocardial infarction: a randomized, controlled study. Am Heart J
1984;108:1402-1408. 4. Raizner AE, Toroledo FA. Verani MS, Van Reet RE. Young JB, Rickman FD. Cashion RW. Samuels DA. Pratt CM. AttarM. Ruhin HS. Lewis IM. Klein MS, Roberts R. Intracoronary thrombolytic therapy in act& myocbrdiai in- farction: a prospective, randomized, controlled trial. Am J Cardiol 1985; 55:301-308. 5. Kennedy JW, Ritchie JL. Davis KB, Fritz JK. Western Washington random- ized trial of intracoronary streptokinase in acute myocardial infarction. N Engl J Med 1983;309:1477-1482. 6. Kennedy JW, Ritchie JL, Davis KB, Stadium ML. Maynard C. Fritz JK. The Western Washington randomized trial of introcoronary streptokinase in acute myocardial infarction. A t2-month follow-up report. N Engl J Med 1985;312:1073-1078. 7. Ritchie JL, Davis KB. Williams DL, Caldwell J, Kennedy JW. Global and regional left ventricular function and tomographic radionuclide perfusion: the western Washington intracoronary streptokinase in myocardial infarc- tion. Circulation 1984;70:887-875. 9. Leiboff RH, Katz RJ, Wasserman AG, Bren GB, Schwartz H. Varghese J, Ross AM. A randomized. angiogmphically controlled trial of intracoro- nary streptokinase in acute myocardial infarction. Am J Cardiol 1984;53: 404-407. 9. Simoons ML, Serruys PW, Brand M. Bar F, De Zwann C. Res J, Verheugt F. Krauss X, Reeme W. Vermeer F, Lusbsen J, Improved survival after early thrombolysis in acute myocardial infarction. A randomized trial by the Inter- university Cardiology Institute in the Netherlands. Lancet 1985;2:578-581. 10. Simoons ML, Serruys PW. Brand M, Res J. Verheugt FW. Krauss H, Remme WJ. Bar F, De Zwaan C. Laarse A. Vermeer F, Lubsen J. Early thmmbolysis in acute myocardial infarction limitation of infarct size and improved survival. JACC 1986;7:717-728. 11. Serruvs PW. Simoons ML. Survanranata H. Vermeer F. Wiins W. Brand M. Bar F.Zwann C. Krauss H.‘Rem”me WJ, Res J, Verheugt FWA: Domburg R, Lubsen J, Hugenholtz PG. Preservation ofglabaland regional left ventricular function after early thrombolysis in acute myocardial infarction. JACC i986;7:72Q-742. 12. Rentroo KP. Feit F. Blanke H. Stecv P. Schneider R. Rev M. Horowitz S. Golman M: Kamch K, Meilman H. Cohen M. Siegel S. Slate; J. Gorlin R. Foi A. Fagerstrom R, Calhoun W. Effects of intracoronary streptokinase and intracaronary nitroglycerin infusion on coronary angiographic patterns and mortality in patients with acute myocardial infarction. N Engl J Med 1984:311:1457-1463. 13. Gruppo Italian0 Per Lo Studio della Streptochlnasi Nell’infarto Miocar- dice (GISSIJ. Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet 1986;1:397-401. 14. ISAM Shtdv Groun. A nrosnective trial of intravenous streptokinase in acute myocardibl infa&ion (1.S:A.M.J. Mortality. morbidity and infarct size at 21 days. N Engl J Med 1986;314:1465-1471. 15. Olson HG, Butman SM. Piters KM, Gardin JM. Lyons KP, Jones L. Chilazi G, Kumar A, Colombo A. A randomized controlled trial of intmvenous strep- tokinase in acute myocardial infarction. Am Heart 1 1986;111:1021-1029. 16. Mantel N. Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Nat Cancer Inst 1959;22:719-748. 17. Woolf B. Estimating the relationship between blood group and disease. Ann Human Genet 1955;19:251-253. 18. Stampfer MJ, Goldhaber SZ, Yusuf S. Peto R. Hennekens C. Effect of intravenous streptokinase on acute myocardial infarction: pooled results from randomized trials. N Engl 1 Med 1982;307:1180-1182. 19. Smalling RW. Fuentes F. Mathews MW. Freund GC, Hicks CH, Reduto LA, Walker WE, Sterling RP. Gould KL. Sustained intracoronary streptaki- nose administration during evolving myocardial infarction. Circulation 1983: 68~131-138. Zb. Ferguson DW, White CW. Schwarz JL. Brayden GP. Kelley KJ, Kioschos IM. Kirchner PT, Marcus ML. Influence of baseline ejection fraction and success of thmmbolysis on mortality and left ventricular Junction after acute myocardial infarction. Am J Cardiol 198454:705-711. 21. Sheehan FH. Mathey DG. Schoder J. Krebber H. Dodge HT. Effect of interventions in salvaging left ventricular function in acute myocardial in- farction: a study of intracomnazy streptokinase. Am J Cardiol 1983;52:431- 438. 22. Schwarz F. Faure A. Katus H. Olshausen KV, Hofmann M, Schuler G, Mathey J, Kubler W. Intmcoronary thrombolysis in acute myocardial infarc- tion: an attempt to quantitate its effect by comparison of enzymatic estimate of myocardial necrosis with left ventricular ejection fmction. Am J Cardiol 1983;51:1573-1578. 23. Carlbier A, Berland J, Champoud 0. Moore N, Behar P. Letac B. Intracor- onary thmmbolysis in evolving myocardial infarction. sequential am&mph- ic analysis of left ventricular performance. Br Heart J 1983;50:481-410. 24. Taylor GJ, Mike11 FL, Moses HW, Dove JT. Batchelder JE. Thull A, Han- sen S. Wellons HA, Schneider HA. Intmvenous versus intmcoronary strepto- kinase therapy for acute myocardial infarction in community hospitals. Am J Cardiol x98454:256-260. 25. Cowley MJ, Hastillo A, Vetrovec GW. Hess M. Effects of introcoronary streptokinase in myocardial infarction. Am Heart / 1981;102:1149-1157.
















