Analysis of Pancreatic Elastase-1 Concentrations in Duodenal Aspirates from Healthy Subjects and...
7
Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004), pp. 1405–1411 ( C 2004) Analysis of Pancreatic Elastase-1 Concentrations in Duodenal Aspirates from Healthy Subjects and Patients with Chronic Pancreatitis TYLER STEVENS, MD,* DARWIN CONWELL, MD,* GREGORY ZUCCARO, MD,* FREDERICK VAN LENTE, PhD,† FARAH KHANDWALA, MS,‡ PATRICK HANAWAY, MD,§ JOHN J. VARGO, MD, MPH,* and JOHN A. DUMOT, DO* Fecal pancreatic elastase 1 (PE-1) has been advocated as a noninvasive marker of pancreatic func- tion and allows detection of moderate and severe exocrine insufficiency. Few studies have evaluated the utility of measuring PE-1 in duodenal fluid for the diagnosis of pancreatic insufficiency. Our purpose was (1) to determine the feasibility of measuring PE-1 concentrations in duodenal aspirates obtained through our endoscopic pancreatic function test (ePFT) in healthy subjects and patients with chronic pancreatitis (CP) and (2) to determine correlations between duodenal PE-1 concentrations and bicarbonate and lipase concentrations in duodenal fluid. Healthy subjects (HS) and CP patients underwent an ePFT with CCK or secretin. CP was defined as endoscopic retrograde pancreatography (ERP) Cambridge class III–IV, endoscopic ultrasound (EUS) score >5, or presence of pancreatic calcifications on CT scan. Duodenal fluid PE-1, lipase, and bicarbonate concentrations were mea- sured in each study group. Duodenal lipase and bicarbonate concentrations were measured using an autoanalyzer (Roche Diagnostics, Indianapolis, IN). PE-1 was measured using an ELISA (Genova Diagnostics, Asheville, NC). Ten HS and 10 CP patients were studied. In the CCK test the median peak lipase for HS and CP was 1605 and 113 IU/L, respectively ( P < 0.008). In the secretin test the median peak bicarbonate for HS and CP was 102 and 40 mEq/L, respectively ( p < 0.008). Median PE-1 concentrations for HS and CP were 317 and 63 µg/ml, respectively, after CCK stimulation ( p = 0.046) and 87 and 17 µg/ml, respectively, after secretin stimulation ( p = 0.033). Statistically significant correlations were found between [PE-1] and peak [lipase] (r = 0.83, P < 0.001), as well as [PE-1] and peak [HCO3 − 3 ](r = 0.65, P = 0.037). Conclusions are as follows: (1) PE-1 concen- trations can be measured from duodenal fluid obtained by endoscopic aspiration. (2) Duodenal fluid PE-1 concentrations are decreased in CP compared to HS. (3) Duodenal fluid [PE-1] has an excellent correlation with [lipase] and therefore is a marker of acinar cell function. (4) Secretin-stimulated endoscopic function testing with measurement of bicarbonate and PE-1 may provide a simultaneous assessment of both ductal cell and acinar cell function. KEY WORDS: chronic pancreatitis; pancreatic elastase-1; pancreatic function testing; diagnosis. Pancreatic elastase-1 (PE-1) is one of a family of pro- tease enzymes secreted by pancreatic acinar cells. Unlike Manuscript received March 31, 2004; accepted June 16, 2004. From *The Pancreas Clinic, Section of Endoscopy, Department of Gastroenterology and Hepatology, †Department of Clinical and Labora- tory Medicine, and ‡Department of Biostatistics, Cleveland Clinic Foun- dation, Cleveland, Ohio, and §Genova Diagnostics, Asheville, North Carolina, USA. other pancreatic enzymes, PE-1 is extremely stable within the gastrointestinal tract and therefore may be measured quantitatively in feces (1). It has been demonstrated that Address for reprint requests: Darwin Conwell, MD, The Pancreas Clinic, Digestive Disease Center, Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, 9500 Euclid Avenue, A30, Cleveland, Ohio 44118, USA; [email protected]. Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004) 1405 0163-2116/04/0900-1405/0 C 2004 Springer Science+Business Media, Inc.
-
Upload
tyler-stevens -
Category
Documents
-
view
216 -
download
4
Transcript of Analysis of Pancreatic Elastase-1 Concentrations in Duodenal Aspirates from Healthy Subjects and...

Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004), pp. 1405–1411 ( C© 2004)
Analysis of Pancreatic Elastase-1 Concentrationsin Duodenal Aspirates from Healthy Subjects
and Patients with Chronic Pancreatitis
TYLER STEVENS, MD,* DARWIN CONWELL, MD,* GREGORY ZUCCARO, MD,*FREDERICK VAN LENTE, PhD,† FARAH KHANDWALA, MS,‡ PATRICK HANAWAY, MD,§
JOHN J. VARGO, MD, MPH,* and JOHN A. DUMOT, DO*
Fecal pancreatic elastase 1 (PE-1) has been advocated as a noninvasive marker of pancreatic func-tion and allows detection of moderate and severe exocrine insufficiency. Few studies have evaluatedthe utility of measuring PE-1 in duodenal fluid for the diagnosis of pancreatic insufficiency. Ourpurpose was (1) to determine the feasibility of measuring PE-1 concentrations in duodenal aspiratesobtained through our endoscopic pancreatic function test (ePFT) in healthy subjects and patients withchronic pancreatitis (CP) and (2) to determine correlations between duodenal PE-1 concentrationsand bicarbonate and lipase concentrations in duodenal fluid. Healthy subjects (HS) and CP patientsunderwent an ePFT with CCK or secretin. CP was defined as endoscopic retrograde pancreatography(ERP) Cambridge class III–IV, endoscopic ultrasound (EUS) score >5, or presence of pancreaticcalcifications on CT scan. Duodenal fluid PE-1, lipase, and bicarbonate concentrations were mea-sured in each study group. Duodenal lipase and bicarbonate concentrations were measured using anautoanalyzer (Roche Diagnostics, Indianapolis, IN). PE-1 was measured using an ELISA (GenovaDiagnostics, Asheville, NC). Ten HS and 10 CP patients were studied. In the CCK test the medianpeak lipase for HS and CP was 1605 and 113 IU/L, respectively (P < 0.008). In the secretin test themedian peak bicarbonate for HS and CP was 102 and 40 mEq/L, respectively (p < 0.008). MedianPE-1 concentrations for HS and CP were 317 and 63 µg/ml, respectively, after CCK stimulation(p = 0.046) and 87 and 17 µg/ml, respectively, after secretin stimulation (p = 0.033). Statisticallysignificant correlations were found between [PE-1] and peak [lipase] (r = 0.83, P < 0.001), as wellas [PE-1] and peak [HCO3−
3 ] (r = 0.65, P = 0.037). Conclusions are as follows: (1) PE-1 concen-trations can be measured from duodenal fluid obtained by endoscopic aspiration. (2) Duodenal fluidPE-1 concentrations are decreased in CP compared to HS. (3) Duodenal fluid [PE-1] has an excellentcorrelation with [lipase] and therefore is a marker of acinar cell function. (4) Secretin-stimulatedendoscopic function testing with measurement of bicarbonate and PE-1 may provide a simultaneousassessment of both ductal cell and acinar cell function.
KEY WORDS: chronic pancreatitis; pancreatic elastase-1; pancreatic function testing; diagnosis.
Pancreatic elastase-1 (PE-1) is one of a family of pro-tease enzymes secreted by pancreatic acinar cells. Unlike
Manuscript received March 31, 2004; accepted June 16, 2004.From *The Pancreas Clinic, Section of Endoscopy, Department of
Gastroenterology and Hepatology, †Department of Clinical and Labora-tory Medicine, and ‡Department of Biostatistics, Cleveland Clinic Foun-dation, Cleveland, Ohio, and §Genova Diagnostics, Asheville, NorthCarolina, USA.
other pancreatic enzymes, PE-1 is extremely stable withinthe gastrointestinal tract and therefore may be measuredquantitatively in feces (1). It has been demonstrated that
Address for reprint requests: Darwin Conwell, MD, The PancreasClinic, Digestive Disease Center, Department of Gastroenterology andHepatology, Cleveland Clinic Foundation, 9500 Euclid Avenue, A30,Cleveland, Ohio 44118, USA; [email protected].
Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004) 14050163-2116/04/0900-1405/0 C© 2004 Springer Science+Business Media, Inc.

STEVENS ET AL.
concentrations of PE-1 in feces are five- to sixfold higherthan in pure pancreatic juice, likely because of the stabilityof the protein within the intestinal tract combined with thevast amount of water absorbed during intestinal transit (2).In recent years, the measurement of fecal PE-1 has beenadvocated as a noninvasive marker of pancreatic function.
Like many other indirect pancreatic function tests, fe-cal PE-1 is more reliable for detecting advanced than mildexocrine insufficiency. The sensitivity of fecal PE-1 formoderate and advanced chronic pancreatitis (CP) is 85 to100%; however, the sensitivity for mild chronic pancre-atitis varies from 0 to 63% (3–7). Several studies havedemonstrated superiority of fecal PE-1 over other indi-rect pancreatic function tests (8,9), whereas others havenot (10). Although abnormal fecal PE-1 reliably corre-lates with advanced CP detected on imaging tests, its useis limited in detecting “minimal-change” CP in patientspresenting with abdominal pain and appropriate risk fac-tors (11). Furthermore, stool collection is cumbersome forpatients and lab technicians.
Although duodenal fluid is cleaner and easier to handlethan stool, few studies have evaluated the measurementof duodenal PE-1 for the diagnosis of pancreatic insuf-ficiency. This may relate in part to the time-consumingand invasive nature of collecting duodenal fluid usingdouble-lumen (gastroduodenal) tubes. We have developeda purely endoscopic test that overcomes these difficulties,allowing the endoscopic collection of timed duodenal as-pirates after cholecystokinin (CCK) or secretin stimula-tion. Our initial investigations have shown that this endo-scopic pancreatic function test (ePFT) reliably reproducesthe pancreatic electrolyte secretory curve seen with tradi-tional gastroduodenal tube collection (12) and success-fully differentiates patients with and without establishedCP (13,14). The endoscopic test is better tolerated and lesscostly, eliminates the need for fluoroscopy, and is easier toperform than the traditional direct pancreatic function test(13). Based on this newer endoscopic method of duodenalfluid collection, it has become markedly easier to obtainpancreatic juice for biochemical analysis.
The primary aim of this study was to determine thefeasibility of measuring PE-1 concentrations in duode-nal aspirates obtained through our ePFT. Secondarily, wesought (1) to compare PE-1 concentrations in healthy sub-jects (HS) and patients with CP and (2) to determine if cor-relations exist between duodenal PE-1 concentrations andbicarbonate and lipase concentrations in duodenal fluid.
MATERIALS AND METHODS
Study DesignHealthy subjects (HP) and patients with CP were enrolled in
an IRB-approved protocol to assess the lipase and bicarbonate
concentrations of endoscopically aspirated duodenal drainagefluid. Fluid samples were frozen and PE-1 concentrations weremeasured at a later date. Cases of established CP were selectedbased on the presence of severe ductal and parenchymal changeson imaging tests prior to the endoscopic PFT.
1. Computed tomography (CT) scan showing ductal orparenchymal calcifications.
2. Endoscopic retrograde pancreatogram (ERP): Cambridgeclass III–IV (15).
3. Endoscopic ultrasound showing extensive ductal andparenchymal changes (EUS score >5) (16,17)
Controls were healthy volunteers recruited into previous researchstudies. All fluid samples were obtained within 5 years of thepresent study and had been frozen at −70◦C. An equal numberof CCK- and secretin-stimulated samples were analyzed fromboth groups.
Endoscopic Collection MethodDuodenal fluid was obtained by our previously described
CCK (13)- or secretin (14)-stimulated pancreatic function tests.Subjects underwent a sedated upper endoscopy examination forboth methods. First, gastric fluid is suctioned through the scopeas completely as possible and discarded, then the scope is ad-vanced into the second portion of the duodenum. At the on-set of endoscopy, either the secretin or the CCK hormone isadministered.
Endoscopic Secretin Test. Following a test dose (0.2 µg), afull dose (2 µg/kg) of synthetic porcine secretin (ChiRhoClin,Inc., Burtonsville, MD) is given intravenously. Duodenal aspi-rates are obtained at baseline (bottle A) and at 15-min intervalsfor 1 hr (bottles B–E). Duodenal fluid samples are immediatelyplaced on ice and transferred to the laboratory for bicarbonateanalysis.
Endoscopic CCK Test. CCK (Sincalide; 40 ng/kg/hr;Bracco Diagnostics, Inc., Princeton, NJ) is infused for a totalof 1 hr through an iv catheter. During the infusion, timed aspira-tions of duodenal fluid are obtained at 0, 15, 30, 45, and 60 min(bottles A–E). Fluid was sent immediately on ice for analysisof lipase concentration. For both of the above tests, separatealiquots were set aside and frozen at −70◦C for future studies.
Fluid Analysis. Lipase and bicarbonate concentrations weremeasured shortly after fluid collection. Bicarbonate concen-trations are determined as total carbon dioxide by a rate pHmeasurement using reagents and an autoanalyzer (CX3 Delta;Beckman-Coulter, Brea, CA) (14). Lipase activity is determinedusing the chromogenic lipase substrate 1,2-o-dilauryl-raclycero-3-glutaric acid (6-methylresorufin) ester with reagents obtainedfrom Roche Diagnostics (Indianapolis, IN) and a Roche Diag-nostics Hitachi 917 automated chemistry analyzer (13).
PE-1 concentrations were measured on frozen samples us-ing an ELISA (Genova Diagnostics, Asheville, NC, and ScheBoTech, Wettenberg, Germany). Aliquots from the 15- or 30-minaspirations were utilized. Duodenal fluid was first diluted to aconcentration of 1:10,000. The PE-1 concentration was calcu-lated photometrically compared to standardized solutions.
Statistical MethodsDescriptive statistics include medians and interquartile
ranges. A one-sided Wilcoxon rank sum test was used to analyze
1406 Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004)

PANCREATIC ELASTASE-1 IN DUODENAL ASPIRATES FROM CHRONIC PANCREATITIS PATIENTS
TABLE 1. CHARACTERISTICS OF CHRONIC PANCREATITIS PATIENTS
Pt. No. Test* Age Sex Etiology Imaging Test†
1 CCK 44 F Alcohol ERP Cambridge IVPancreatic calcifications on CT
2 CCK 67 M Alcohol ERP Cambridge III3 CCK 58 F Alcohol ERP Cambridge IV4 CCK 59 M Idiopathic EUS score >55 CCK 57 F Idiopathic ERP Cambridge IV6 SEC 63 M Idiopathic EUS score >57 SEC 47 F Alcohol EUS score >58 SEC 31 M Alcohol ERP Cambridge IV9 SEC 60 M Alcohol ERP Cambridge IV
Pancreatic calcifications on CT10 SEC 27 F Alcohol ERP Cambridge IV
*SEC, secretin.†Cambridge classification for ERP staging of CP; EUS score for staging
of ductal and parenchymal changes in CP (15, 16).
differences in lipase, bicarbonate, and PE-1 concentration be-tween groups. Correlations were analyzed using Spearman rankorder correlations. A significance level of 0.05 was used for allanalyses.
RESULTS
DemographicsDuodenal drainage fluid from 10 healthy subjects (HS)
and 10 CP patients was studied. Within each group, fivepatients underwent the CCK test and five underwent the se-cretin test. The mean age of the CP group was 51 (5 F/5 M).The mean age of the HS group was 33 years (7 F/3 M).All of the CP patients had advanced CP based on imagingtests. The etiology of CP was alcohol in seven patients andidiopathic in three patients (Table 1).
Fig 1. (A) Peak lipase concentrations measured in CCK-stimulated endoscopic pancreaticfunction test. (B) Peak bicarbonate concentrations measured in secretin-stimulated endoscopicpancreatic function test. Horizontal dashed lines denote previously noted cut-points for diagnosisof CP (peak [lipase], <810,000 IU/L for CCK test; peak [HCO−
3 ], <80 mEq/L for secretin test)(13, 14).
Hormone-Stimulated Pancreatic Function TestsThe results of CCK (peak lipase concentration) or se-
cretin (peak bicarbonate concentration) ePFT were com-pared between the HS and the CP patients. Five HS andfive CP patients underwent the CCK test. The medianpeak lipase concentrations for the HS and CP patientswere 1605 IU/L (IQR, 1211–2611) and 113 IU/L (IQR,36–190), respectively (P < 0.008) (normal: >810,000 IU[13] (Figure 1A). Five HS and five CP patients under-went the secretin test. The median peak bicarbonate con-centrations for HS and CP patients were 102 mEq/L(IQR, 98–104) and 40 mEq/L (IQR, 30–61), respectively(P < 0.008) (normal: >80 mEq/L) (Figure 1B).
Pancreatic Elastase-1 ConcentrationsThe PE-1 values of frozen samples for both the CCK
and the secretin tests are shown in Figure 2. For the CCKtest, median PE-1 concentrations for HS and CP were 317µg/ml (IQR, 142–332) and 63 µg/ml (IQR, 29–68), re-spectively (p = 0.046). For the secretin test, median PE-1concentrations for HS and CP patients were 87 µg/ml(IQR, 55–253) and 17 µg/ml (IQR, 15–22), respectively(P = 0.033). Significant correlations were found between[PE-1] and peak [lipase] (r = 0.83, P < 0.001; Figure 3),as well as [PE-1] and peak [HCO3−
3 ] (r = 0.65, P =0.037).
DISCUSSION
We have shown that duodenal fluid [PE-1] is de-creased in patients with advanced chronic pancreatitis
Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004) 1407
STEVENS ET AL.
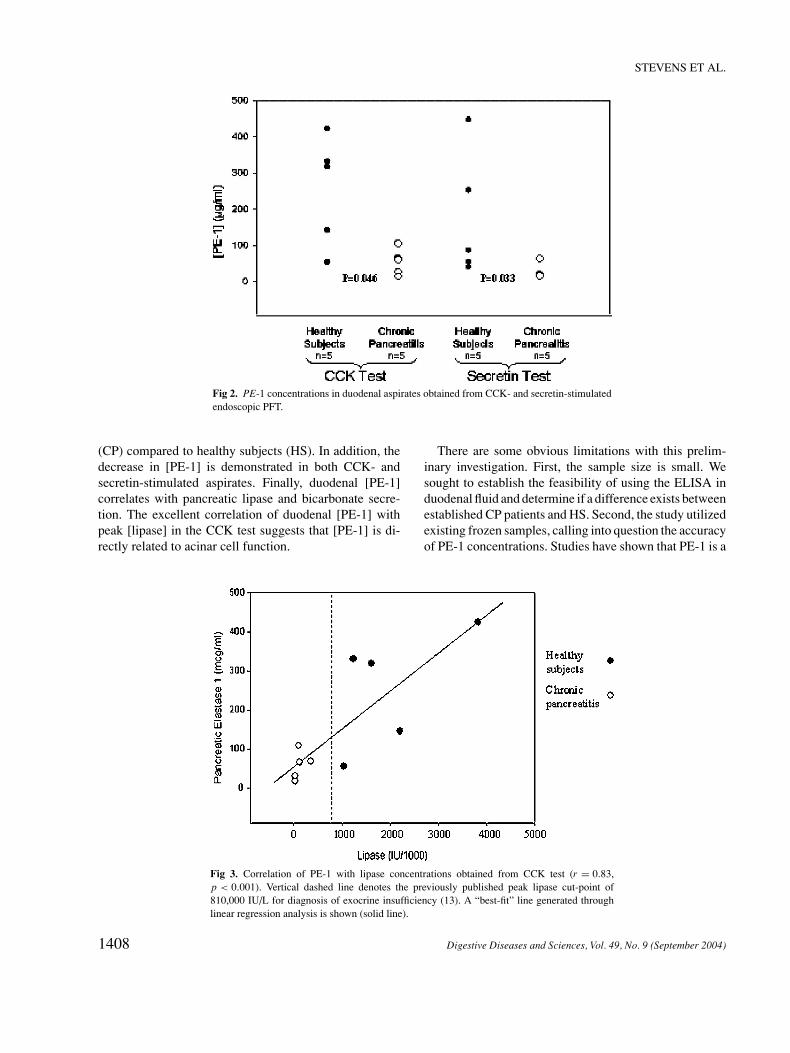
Fig 2. PE-1 concentrations in duodenal aspirates obtained from CCK- and secretin-stimulatedendoscopic PFT.
(CP) compared to healthy subjects (HS). In addition, thedecrease in [PE-1] is demonstrated in both CCK- andsecretin-stimulated aspirates. Finally, duodenal [PE-1]correlates with pancreatic lipase and bicarbonate secre-tion. The excellent correlation of duodenal [PE-1] withpeak [lipase] in the CCK test suggests that [PE-1] is di-rectly related to acinar cell function.
Fig 3. Correlation of PE-1 with lipase concentrations obtained from CCK test (r = 0.83,p < 0.001). Vertical dashed line denotes the previously published peak lipase cut-point of810,000 IU/L for diagnosis of exocrine insufficiency (13). A “best-fit” line generated throughlinear regression analysis is shown (solid line).
There are some obvious limitations with this prelim-inary investigation. First, the sample size is small. Wesought to establish the feasibility of using the ELISA induodenal fluid and determine if a difference exists betweenestablished CP patients and HS. Second, the study utilizedexisting frozen samples, calling into question the accuracyof PE-1 concentrations. Studies have shown that PE-1 is a
1408 Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004)

PANCREATIC ELASTASE-1 IN DUODENAL ASPIRATES FROM CHRONIC PANCREATITIS PATIENTS
very stable protein and resistant to degradation, allowingits measurement in fecal specimens (2, 4). Therefore, sincePE-1 appears to be a highly stable enzyme, and all sam-ples were stored at −70◦C, it is unlikely that significantdegradation occurred.
Pancreatic function testing plays a central role in thediagnosis of exocrine insufficiency and minimal-changeCP. Many experts accept direct hormone-stimulated pan-creatic function tests as the most accurate diagnostic testsand the nonhistologic gold standard for assessing pan-creatic exocrine function (18). Available literature sug-gests that direct PFT provides a sensitivity of 74–90%and specificity of 80–90% (11), however, these studiesare limited in some respects. (1) Most have included pa-tients with established CP characterized by severe ductaland parenchymal changes. There have been relatively fewstudies evaluating the test characteristics of direct PFTin patients with early pancreatitis and minimal imagingchanges. (2) Most studies have suggested discordance offunction tests with imaging tests (ERP), particularly inearly CP (19–22); therefore, a simultaneous assessmentof structure and function may be the ideal diagnosticapproach to early CP. (3) Finally, few studies (23, 24)have compared direct PFT to histology, the only true goldstandard.
In addition to the limitations of the available literature,the practical difficulty of passing gastroduodenal tubeshas restricted the availability of direct pancreatic functiontesting to only a few academic centers. This has led to nu-merous studies investigating less invasive and more time-efficient “tubeless” tests (25). In general, the sensitivitiesof these indirect PFTs are acceptable for moderate andadvanced CP, but poor for mild CP. Most recently, fecalelastase-1 has been advocated as a simple and accurate testfor detecting pancreatic exocrine insufficiency. Althoughfecal elastase-1 is noninvasive and has good accuracy inadvanced exocrine insufficiency, numerous studies havedemonstrated poor reliability for detecting mild exocrineinsufficiency, or early CP, characterized by the absence ofimaging changes and frank steatorrhea (11, 26–28). In ad-dition, stool collection and handling are cumbersome forpatients and laboratory technicians. Hormone-stimulateddirect PFT still remains the gold standard for CPdiagnosis.
Although most direct function tests utilize double-lumen tubes for collection of duodenal fluid, therehave been innumerable permutations of the “traditional”test initially described by Lagerloef (29) and Dreilingand Hollander (30). There is substantial methodologicalvariability among the many published tests, especiallypertaining to the hormonal stimulants and pancreatic out-put parameters. The choice and combination of pancre-
atic stimulants have been especially controversial. CCKprimarily stimulates acinar cells; secretin primarily stim-ulates duct cells. Based on this physiology, secretin testshave traditionally measured bicarbonate and fluid volume,providing an assessment of ductular secretory function,and CCK tests have measured enzyme concentrations andoutputs for assessment of acinar cell function. The combi-nation of both hormonal stimulants has been advocated asthe most comprehensive assessment of exocrine function;however, combining hormones adds complexity and ex-pense to an already cumbersome test and may precipitateacute pancreatitis due to overstimulation of the gland.
Although secretin is not the primary acinar cell secre-tagogue, it does potentiate the release of enzymes fromacinar cells. Furthermore, secretin stimulates water se-cretion and increased flow through the duct, effectively“washing out” residual enzymes (31). Because decreasedamounts of residual enzymes may be present within theducts of patients with exocrine insufficiency, duodenalenzyme concentration after secretin stimulation may es-timate acinar cell function. Raimondo et al. studied asecretin-stimulated endoscopic test with measurement ofboth lipase and bicarbonate, however, the results for thisshortened test were not satisfactory (32).
Although some investigators have advocated specificdirect PFT protocols as the “gold standard,” a widely ac-cepted test has not yet become established. Part of thereason for this is the extreme complexity and relative in-accessibility of many of the test designs to busy clini-cians. In recent years, we have designed an endoscopicpancreatic test that simplifies the collection of hormon-ally stimulated duodenal fluid, facilitating the detectionof pancreatic exocrine insufficiency. The measurement ofpeak lipase concentration for the endoscopic CCK test (13)and peak bicarbonate for the endoscopic secretin test (14)has been shown to differentiate those with and withoutestablished CP.
As mentioned above, the sensitivity and specificity ofdirect PFT for early CP and mild exocrine insufficiencyare not known. Previous studies have suggested that aci-nar cell function declines earlier in the course of CP thanductal function (33). Therefore, a combination of secretinand CCK may offer better sensitivity for early CP thaneither of these hormonal stimulants alone. Others havesuggested that measuring a profile of enzymes (e.g., amy-lase + lipase + trypsin) rather than a single enzyme mayoffer increased sensitivity for detecting early pancreaticdisease (34).
The recent availability of a simple ELISA for PE-1 maycomplement other parameters typically measured with di-rect pancreatic function testing, enhancing the diagnosisof CP and providing an indirect measure of pancreatic
Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004) 1409

STEVENS ET AL.
acinar cell function. Relatively few studies have evaluatedthe diagnostic utility of measurement of elastase-1 inpancreatic juice. Sziegoleit et al. measured PE-1 concen-trations in pure pancreatic juice samples from 12 patientsobtained by the intraductal secretin test (2). The median[PE-1] was 0.26 mg/ml for the six patients with a normalsecretin test, compared to 0.017 mg/ml for the six patientswith an abnormal secretin test. Loser et al. analyzed thecorrelation of duodenal [PE-1] with the concentrations ofother pancreatic enzymes (4). Duodenal [PE-1] correlatedwell with amylase, lipase, and trypsin (r = 0.9, 0.8, and0.8, respectively) as well as bicarbonate concentrationsand fluid volumes. The study demonstrated an excellentsensitivity of fecal PE-1 for moderate and advanced ex-ocrine insufficiency and 63% sensitivity for mild exocrineinsufficiency. Though the authors reported a good corre-lation of duodenal with fecal PE-1, the diagnostic sensi-tivities of duodenal [PE-1] for early-, moderate-, and late-stage pancreatic exocrine insufficiency were not reported.Stein et al. confirmed a good correlation of duodenal [PE-1] with other pancreatic enzymes concentrations and withfecal elastase (9).
Our study demonstrated lower median PE-1 levels ob-tained through the secretin test compared to the CCK test.Because secretin principally stimulates ductal cells to pro-duce large volumes of bicarbonate and water, dilutionof acinar cell proteins results in lower PE-1 concentra-tions. Our data also demonstrate that both hormones pro-duce lower PE-1 concentrations in CP patients comparedto HS. Based on these results, an endoscopic secretintest with PE-1 analysis may provide a complete assess-ment of exocrine function, because it could assess duct(bicarbonate) and acinar cell (PE-1) function simultane-ously. Of course, our preliminary data require confirma-tion in a prospective trial of patients with varying stages ofdisease.
In conclusion, duodenal PE-1 concentrations are lowerin CP compared to HS and PE-1 levels correlate well withother measures of pancreatic function. The excellent cor-relation with lipase suggests that PE-1 is a marker of acinarcell function. Secretin, as well as CCK, allows differen-tiation of CP from health based on PE-1 analysis. Ourpreliminary data suggest that a secretin-stimulated ePFTwith measurement of peak bicarbonate and [PE-1] will al-low a simultaneous assessment of both pancreatic ductalcell and acinar cell function.
ACKNOWLEDGMENTS
Support for this research was provided by an unrestricted edu-cational grant from Solvay Pharmaceuticals, Marietta, Georgia.It was presented in poster form at the meeting of the American
Gastroenterological Association, Digestive Disease Week, NewOrleans, Louisiana, May 2004.
REFERENCES
1. Sziegoleit A, Linder D: Studies on the sterol-binding capacity ofhuman pancreatic elastase 1. Gastroenterology 100:768–774, 1991
2. Sziegoleit A, Krause E, Klor HU, Kanacher L, Linder D: Elastase1 and chymotrypsin B in pancreatic juice and feces. Clin Biochem22:85–89, 1989
3. Dominguez-Munoz JE, Hieronymus C, Sauerbruch T, MalfertheinerP: Fecal elastase test: Evaluation of a new non-invasive pancreaticfunction test. Am J Gastroenterol 90:1834–1837, 1995
4. Loser C, Mollgaard A, Folsch UR: Faecal elastase 1: A novel, highlysensitive, and specific tubeless pancreatic function test. Gut 39:580–586, 1996
5. Martinez J, Laveda R, Trigo C, Frasquet J, Palazon JM, Perez-MateoM: Fecal elastase-1 determination in the diagnosis of chronic pan-creatitis. Gastroenterol Hepatol 25:377–382, 2002
6. Gullo L, Ventrucci M, Tomassetti P, Migliori M, Pezzilli R: Fecalelastase 1 determination in chronic pancreatitis. Dig Dis Sci 44:210–214, 1999
7. Dominic R, Franzini C: Fecal elastase-1 as a test for pancreaticfunction: A review. Clin Chem Lab Med 40:325–332, 2002
8. Takeda M, Shiratory K, Hayashi N, Odagiri E, Takasaki K: Fecalelastase-1: Clinical evaluation of a new noninvasive pancreatic func-tion test. Rinsho Byori 50:893–898, 2002
9. Stein J, Jung M, Sziegoleit A, Zeuzem S, Caspary WF, Lembcke B:Immunoreactive elastase I: Clinical evaluation of a new noninvasivetest of pancreatic function. Clin Chem 42:222–226, 1996
10. Leodolter A, Kahl S, Dominguez-Munoz JE, Gerards C, Glasbren-ner B, Malfertheiner P: Comparison of two tubeless function testsin the assessment of mild-to-moderate exocrine pancreatic insuffi-ciency. Eur J Gastroenterol Hepatol 12:1335–1338, 2000
11. Gredal C, Madsen LG, Larsen S: The Lundh test and faecal elas-tase 1 determination in chronic pancreatitis: a comparitive study.Pancreatology 3:389–394, 2003
12. Stevens T, Conwell DL, Zuccaro G, Van Lente F, Khandwala F,Purich E, Vargo JJ, Fein S, Dumot JA, Trolli PA, O’Laughlin C:Sedationless pancreatic function testing in healthy normal patients.Panceas 27:A412–A413, 2003
13. Conwell DL, Zuccaro G, Vargo JJ, Morrow JB, Obuchowski N,Dumot JA, Trolli PA, Burton A, O’Laughlin C, VanLente F: Anendoscopic pancreatic function test with cholecytokinin-octapeptidefor the diagnosis of chronic pancreatitis. Clin Gastroenterol Hepatol1:189–194, 2003
14. Conwell DL, Zuccaro G, Vargo JJ, Trolli PA, VanLente F,Obuchowski N, Dumot JA, O’Laughlin C: An endoscopic pan-creatic function test with synthetic porcine secretin for the evalu-ation of chronic abdominal pain and suspected chronic pancreatitis.Gastrointest Endosc 57:37–40, 2003
15. Sarner M, Cotton PB: Classification of pancreatitis. Report of aninternational symposium at Cambridge. Gut 25:756–759, 1984
16. Sahai AV, Zimmerman M, Aabakken L, Tarnasky PR, CunninghamJT, vanVelse A, Hawes RH, Hoffman BJ: Prospective assessmentof the ability of endoscopic ultrasound to diagnose, exclude, or es-tablish the severity of chronic pancreatitis found by endoscopic ret-rograde cholangiopancreatography. Gastrointest Endosc 48:18–25,1998
17. Wiersema MJ, Hawes RH, Lehman GA, et al.: Prospective eval-uation of endoscopic ultrasonography and endoscopic retrograde
1410 Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004)

PANCREATIC ELASTASE-1 IN DUODENAL ASPIRATES FROM CHRONIC PANCREATITIS PATIENTS
cholangiopancreatography in patients with chronic abdominal painof suspected pancreatic origin. Endoscopy 25:555–564, 1993
18. Lankisch PG: Exocrine pancreatic function tests. Gut 23:777–798,1982
19. Girdwood AH, Hatfield ARW, Bornman PC, Denyer ME, Kottler M,Marks IN: Structure and function in non-calcific pancreatitis. DigDis Sci 29:721–726, 1984
20. Valentini M, Cavallini G, Vantini I, et al.: A comparative evalu-ation of endoscopic retrograde cholangiopancreatography and thesecretin-cholecystokinin test in the diagnosis of chronic pancre-atitis: A multicenter study in 124 patients. Endoscopy 13:64–67,1981
21. Nakano S, Horiguchi Y, Takeda T, Suzuki T, Nakajima S: Compara-tive diagnostic value of endoscopic pancreatography and pancreaticfunction tests. Scand J Gastroenterol 9:383–390, 1974
22. Malfertheiner P, Buchler M, Stanescus A, Ditschuneit H: Exocrinepancreatic function in correlation to ductal and parenchymal mor-phology in chronic pancreatitis. Hepatogastroenterology 33:110–114, 1986
23. Hayakawa T, Kondo T, Shibata T, Noda A, Suzuki T, Nakano S:Relationship between pancreatic exocrine function and histologicalchanges in chronic pancreatitis. Am J Gastroenterol 87:1170–1174,1992
24. Heij HA, Obertop H, Blankenstein M, Kate FW, Westbroek DL:Relationship between functional and histological changes in chronicpancreatitis. Dig Dis Sci 31:1009–1013, 1986
25. Niederau C, Grendell JH: Diagnosis of chronic pancreatitis.Gastroenterology 88:1973–1995, 1985
26. Glasbrenner B, Schon A, Klatt S, Beckh K, Adler G: Clini-cal evaluation of the fecal elastase test in the diagnosis and
staging of chronic pancreatitis. Eur J Gastroenterol Hepatol 8:1117,1996
27. Amann ST, Bishop M, Curington C, Toskes PP: Fecal pancreaticelastase 1 is inaccurate in the diagnosis of chronic pancreatitis.Pancreas 13:226–230, 1996
28. Gunkel U, Bitterlich N, Keim V: Value of combinations of pancreaticfunction tests to predict mild or moderate chronic pancreatitis. ZGastroenterol 39:207–211, 2001
29. Lagerloef HO: Pancraetic function and pancreatic disease:Studied by means of secretin. Acta Med Scand 128:1–289,1942
30. Dreiling DA, Hollander F: Studies in a pancreatic function, prelimi-nary series of clinical studies with the secretin test. Gastroenterology11:714–729, 1948
31. Feurle GE, Singer MV, Baca I: A new round in the discussion on theaction of secretin on pancreatic protein secretion: A further studyon the effect of secretin on pancreatic secretion in dogs. Pancreas2:422–426, 1997.
32. Raimondo M, Imoto M, Dimagno EP: Rapid endoscopic secretinstimulation test and discrimination of chronic pancreatitis and pan-creatic cancer from disease controls. Clin Gastroenterol Hepatol1:397–403, 2003
33. Lankisch PG, Schreiber A, Otto J: Pancreolauryl test. Evaluation ofa tubeless pancreatic function test in comparison with other indirectand direct tests for exocrine pancreatic function. Dig Dis Sci 28:490–493, 1983.
34. Gullo L, Costa PL, Fontana G, Labo G: Investigation of exocrinepancreatic function by continuous infusion of caerulein and secretinin normal subjects and in chronic pancreatitis. Digestion 14:97–107,1976
Digestive Diseases and Sciences, Vol. 49, No. 9 (September 2004) 1411


![Effect of Elastase-induced the' of thedm5migu4zj3pb.cloudfront.net/manuscripts/110000/110709/...creatic elastase in a dose producing hyperinflation (mean total lung capacity [TLC]=](https://static.fdocuments.in/doc/165x107/60aa2d4585131731732f9b22/effect-of-elastase-induced-the-of-creatic-elastase-in-a-dose-producing-hyperinflation.jpg)