![Renal cell carcinoma presenting with cutaneous metastasis ...onkder.org/pdf/pdf_TOD_873.pdf · Renal cell carcinoma presenting with cutaneous metastasis 165 malignancies.[4] Skin](https://static.fdocuments.in/doc/165x107/5cc8f98788c99324098b8787/renal-cell-carcinoma-presenting-with-cutaneous-metastasis-renal-cell-carcinoma.jpg)
Analysis of nodal metastasis in malignancies of upper aerodigestive tract
3
ANALYSIS OF NODAL METASTASIS IN MALIGNANCIES OF UPPER AERODIGESTIVE TRACT Hemant Chopra, Reader, Som Nath Gupta, Ex. Prof. & Head, Neeraj Sud, Ex. Registrar Department of E.N.T., Dayanand Medical College & Hospital, Ludhiana-141001 A mass appearing in the neck can be a diagnostic challenge. The malignancies of upper aerodigestive tract are mostly squamous cell carcinoma and their metastasis remain largely confined to accessible neck areas permitting useful surgical management. In this study 30 patients were taken up with neck node metastasis. It was found that in supraglottic carcinoma even in no neck incidence of nodal metastasis was high. Even the retropharyngeal lymphnodes not involved in routine radical neck dissection were found to be involved in a few cases, which justifies the search for nodes in retropharyngeal area in routine radical neck dissection. INTRODUCTION Malignant process is described as uncontrolled cellular growth and eventual spread to regional lymph nodes/or distant sites through lymphat- ics or blood stream or both. "Dissemination through the lymphatics is the most common Pathway for the initial spread of carcinoma. Sarcomas may also take this route though, they generally spread via haematogenous route. However local lymph nodes may by-passed "Skip Metastasis" because of venous lymphatic anastomosis or because inflammation or radiation has obliterated the channels. Blady (1948) expressed similar view and added "The metastatic potential of primary lesion depends on the amount of lymphatic drainage, the type of malignancy, and other unknown factors, chemical or physical". Winegar et al (1973) regarded malignant node to be more difficult to diagnose. He stated that "The most significant malignant neck mass is the metastatic variety. The primary suorce is evident after initial examination in majority of the cases if the problem is approached me- thodically." After the fifth decade of life, 90% of the cervical masses have a metastatic cancerous origin Marinello (1961). About 84% of the metastatic lesions are squamous cell carcinoma (Acquarelli et al., 1961). However, there are cases of metastatic neck deposits where inspite of search for primary, none is found. Diehl Jr. (1975) have defined the patient with an unknown primary as one with histologic evidence of malignancy in the cervical lymph nodes, and no apparent site of origin of metastatic tumour is found inspite of using all diagnostic techniques. MATERIAL AND METHODS In this study 30 patients coming to ENT O.P.D., Dayanand Medical College. and Hospital with chief complaints of mass in the neck were selected and admitted to the study. Patients selected fulfilled the following: 1) Primary was symptomatic and detected clinically in mirror examination and conformed on endoscopy and proved on histopathology. The neck was attributable to the primary tumour detected. 2) Patients undergoing excisional surgery for UL) & HNS/VUL 47 NO. 2, APRIL-JUNE 1995 230
-
Upload
hemant-chopra -
Category
Documents
-
view
214 -
download
2
Transcript of Analysis of nodal metastasis in malignancies of upper aerodigestive tract

ANALYSIS OF NODAL METASTASIS IN MALIGNANCIES
OF UPPER AERODIGESTIVE TRACTHemant Chopra, Reader,
Som Nath Gupta, Ex. Prof. & Head,
Neeraj Sud, Ex. Registrar
Department of E.N.T.,
Dayanand Medical College & Hospital, Ludhiana-141001
A mass appearing in the neck can be a diagnostic challenge. The malignancies of upperaerodigestive tract are mostly squamous cell carcinoma and their metastasis remain largelyconfined to accessible neck areas permitting useful surgical management.
In this study 30 patients were taken up with neck node metastasis. It was found thatin supraglottic carcinoma even in no neck incidence of nodal metastasis was high. Eventhe retropharyngeal lymphnodes not involved in routine radical neck dissection were foundto be involved in a few cases, which justifies the search for nodes in retropharyngealarea in routine radical neck dissection.
INTRODUCTION
Malignant process is described as uncontrolledcellular growth and eventual spread to regionallymph nodes/or distant sites through lymphat-ics or blood stream or both.
"Dissemination through the lymphatics is themost common Pathway for the initial spreadof carcinoma. Sarcomas may also take thisroute though, they generally spread viahaematogenous route. However local lymph nodesmay by-passed "Skip Metastasis" because ofvenous lymphatic anastomosis or becauseinflammation or radiation has obliterated thechannels.
Blady (1948) expressed similar view andadded "The metastatic potential of primary lesiondepends on the amount of lymphatic drainage,the type of malignancy, and other unknownfactors, chemical or physical".
Winegar et al (1973) regarded malignantnode to be more difficult to diagnose. He statedthat "The most significant malignant neck massis the metastatic variety. The primary suorceis evident after initial examination in majorityof the cases if the problem is approached me-thodically."
After the fifth decade of life, 90% of thecervical masses have a metastatic cancerousorigin Marinello (1961). About 84% of the metastaticlesions are squamous cell carcinoma (Acquarelliet al., 1961).
However, there are cases of metastatic neckdeposits where inspite of search for primary,none is found. Diehl Jr. (1975) have defined thepatient with an unknown primary as one withhistologic evidence of malignancy in the cervicallymph nodes, and no apparent site of origin ofmetastatic tumour is found inspite of using alldiagnostic techniques.
MATERIAL AND METHODS
In this study 30 patients coming to ENT O.P.D.,Dayanand Medical College. and Hospital withchief complaints of mass in the neck were selectedand admitted to the study.
Patients selected fulfilled the following:
1) Primary was symptomatic and detectedclinically in mirror examination and conformedon endoscopy and proved on histopathology.The neck was attributable to the primary tumourdetected.
2) Patients undergoing excisional surgery for
UL) & HNS/VUL 47 NO. 2, APRIL-JUNE 1995 230
Analysis of Nodal Metastasis in Malignancies of Upper Aerodigestive Tract—Hemant Chopra et. a!.
carcinoma who were at high risk for node metastasiswere subjected to RND who had no neck andhistologically positive nodes were also included.
3) Where Primary was not detected by mirrorexamination the lymph node mass was provedto be metastatic deposits on FNAC.
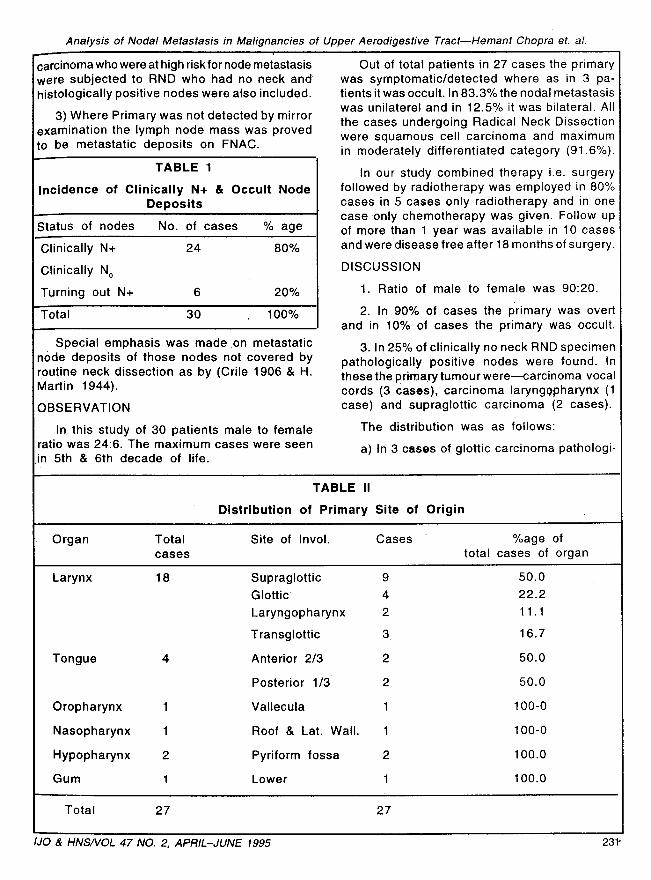
TABLE 1
Incidence of Clinically N+ & Occult NodeDeposits
Status of nodes No. of cases % age
Clinically N+ 24 80%
Clinically N o
Turning out N+ 6 20%
Total 30 100%
Special emphasis was made on metastaticnode deposits of those nodes not covered byroutine neck dissection as by (Crile 1906 & H.Martin 1944).
OBSERVATION
In this study of 30 patients male to femaleratio was 24:6. The maximum cases were seenin 5th & 6th decade of life.
Out of total patients in 27 cases the primarywas symptomatic/detected where as in 3 pa-tients it was occult. In 83.3% the nodal metastasiswas unilaterel and in 12.5% it was bilateral. Allthe cases undergoing Radical Neck Dissectionwere squamous cell carcinoma and maximumin moderately differentiated category (91.6%).
In our study combined therapy i.e. surgeryfollowed by radiotherapy was employed in 80%cases in 5 cases only radiotherapy and in onecase only chemotherapy was given. Follow upof more than 1 year was available in 10 casesand were disease free after 18 months of surgery.
DISCUSSION
1. Ratio of male to female was 90:20.
2. In 90% of cases the primary was overtand in 10% of cases the primary was occult.
3. In 25% of clinically no neck RND specimenpathologically positive nodes were found. Inthese the primary tumour were—carcinoma vocalcords (3 cases), carcinoma larynggpharynx (1case) and supraglottic carcinoma (2 cases).
The distribution was as follows:
a) In 3 cases of glottic carcinoma pathologi-
TABLE II
Distribution of Primary Site of Origin
• Organ Totalcases
Site of Invol. Cases • %age oftotal cases of organ
Larynx 18 Supraglottic 9 50.0
Glottic 4 22.2
Laryngopharynx 2 11.1
Transglottic 3. 16.7
Tongue 4 Anterior 2/3 2 50.0
Posterior 1/3 2 50.0
Oropharynx 1 Vallecula 1 100-0
Nasopharynx 1 Roof & Lat. Wall. 1 100-0
Hypopharynx 2 Pyriform fossa 2 100.0
Gum 1 Lower 1 100.0
Total 27 27
IJO & HNSNOL 47 NO. 2, APRIL–JUNE 1995 231-

Analysis of Nodal Metastasis in Malignancies of Upper Aerodigestice Tract—Hemant Chopra et. a!.
cally positive deposits were found in prelaryngeallymph nodes.
b) In supraglottic carcinoma occult depositswere found in one case retropharyngeal andin one case in prelaryngeal lymph node.
TABLE III
Incidence of Involvement of nodes atDifferent Levels in 24 Cases of N+ Neck
Levels No. of cases % age
Level I 1 4.2Level 11 16 66.6Level 111 1 4.2Level IV 1 4.2Level V 1 4.22 Levels 2 8.33 Levels 2 8.34 Levels - -All Levels - -
I Total 24 100
c) In one case of carcinoma laryngo pharynxmicroscopic deposits were seen in retropharyngeallymph nodes.
Supraglottic carcinoma with clinically no neck
having a retropharyngeal node deposit was asurprise. Retropharyngeal area should be searchedfor nodes in all cases of RND to improve the
regional control of the disease.
4. In all cases the deposits were from squamous
cell carcinoma.
5. The only complication occuring in the series
was pharyngo cutaneous fistula in 2 out of 21
cases (9.5%) of laryngectomies with RND. Thefistula healed spontaneously in both.
6. The 'modality treatment was carried out
(excision of 'the primary and RND followed byradiotherapy) in 24 cases. Only radiotherapy
was given in 5 cases and only CCT in one case.
7. Recurrence occurred in only one case(6.4%) who had undergone excision of primary
with RND left side for supraglottic carcinomawith level II lymph node involvment. Node de-posits develop at level II node contralaterally.
REFERENCES
1. Acquarelli M.J., Matsunaga R.S. & Cruze K. (1961) : Metastatic Carcinoma of the Neck ofUnknown Primary Origin. The Laryngoscope, 962-973.
2. Blady J.V. (1971) : The present status of treatment of cervical metastasis from carcinomaarising in the head and neck region. Am. J. Roentgen. 111 : 56-59.
3. Martin H. & Marfit H.M. (1944) : Cervicaa lymph node metastasis as the first symptom of cancer.Surg. Gyn. Obst., 78:133-159.
4. Martin H. & Romieu C. (1952) : The diagnostic significance of "lump in the neck." Post-gradM., 11: 491-500.
5. Winegar B.K. & Griffin W. (1973) : The occult Primay tumour. Arch. Otolaryngol 98 : 159-163.
1JO & HNSNOL 47 NO. 2, APRIL-JUNE 1995 232


















