Analysis of molecular breakpoint and m-RNA transcripts in a prospective randomized trial of...
9
British ]ournu1 of Haematologg. 1995, 89, 546-554 Analysis of molecular breakpoint and m-RNA transcripts in a prospective randomized trial of interferon in chronic myeloid leukaemia: no correlation with clinical features, cytogenetic response, duration of chronic phase, or survival PATRICIA SHEPHERD, RUTH SUFFOLK, JIM HALSEY* AND NORMAN ALLAN Department of Medicine and MRC Human Genetics Unit, Western General Hospital, Edinburgh, and *CTSU, Radclifle Infirmary, Oxford Received 10 June, 1994; accepted for publication 5 December 1994 Summary. Two hundred and nineteen cases of P h t v e CML and 15 Ph-ve, BCRfve CML cases have been analysed to determine the breakpoint site and its relationship to clinical features, cytogenetic response, duration of chronic phase and survival. 119 cases have had RNA analysis performed to determine the type of BCR/ABL transcript and have also been analysed in a similar way. Presenting features at diagnosis including age, sex, white-cell count and platelet count showed no significant difference for those with 5’ and 3‘ breakpoints and those with either b2a2 or b3a2 BCR/ABL transcripts. However, in a subgroup of patients whose presenting white-cell count was < lOOx 109/1, those with b3a2transcript did have a significantly higher platelet count. Analysis by Sokal risk grouping showed no difference for 5‘ or 3’ breakpoints but a trend for lower stage among those with b2a2 transcripts. No correlation was found either for genomic breakpoint site or BCR/ABL RNA transcript in terms of duration of chronic phase or survival. When stratified by randomized therapy, either interferon-& or standard chemotherapy, no difference was noted in relation to genomic breakpoint site or BCR/ABL transcript. Cyto- genetic response was not related to the molecular findings. Keywords: CML, DNA analysis, RNA analysis, cytogenetic response, prognosis. Chronic myeloid leukaemia (CML) is characterized by the presence of the Philadelphia chromosome which at the molecular level arises because of a breakpoint, usually within the major breakpoint cluster region, in the BCR gene (M-BCR) and translocation of the ABL oncogene from chromosome 9 to lie telomeric to promoter sequences of the BCR gene. A fusion BCR/ABL gene is formed which generates usually either a b2a2 or a b3a2 BCR/ABL RNA transcript depending on whether exon b3 of the M-BCR is expressed. A number of papers have addressed the issue of location of the breakpoint within M-BCR and its effect on prognosis and survival. Those suggesting a link between location of breakpoint and outcome are those by Schaefer- Rego et a1 (1987), Eisenberg et a1 (1988), Shtalrid et a1 (1988), Mills et a1 (1988, 1989), Grossman et aZ(1989) and Tanaka & Kamada (1990). These showed some evidence that those with 5’ breakpoints did better than those with 3’ Correspondence: Dr P. Shepherd, Department of Haematology. Western General Hospital, Edinburgh EH4 2XU. breakpoints. On the other hand, an increasing number of papers have shown no correlation between breakpoint site and outcome (Dyck & Bosco, 1989: Ogawa et al, 1989; Jaubert et aZ, 1990: Morris et al, 1990; Tien et ul, 1990: Tefferi et al, 1990; Opalka et al, 1991; Zaccaria et al, 1992). In a review of these papers (Mills et al, 1991) it was suggested that discrepant results could perhaps be explained best by differences in patient or sample selection. One study has reported BCR/ABL transcripts in CML and found no differencein the type of transcript and survival (Zaccaria et ul, 1993). A further study in a small number of patients did, however, suggest a correlation between the type of BCR/ABL transcript and response to interferon and survival (Inoue et al, 1992). The MRC UK Chronic Myeloid Leukaemia Trial is a multicentre prospective randomized trial of interferon in CML. This provided a unique opportunity to study the location of the breakpoint and the type of BCRIABL m-RNA produced in unselected patients and correlate them with duration of chronic phase and survival, taking into account treatment, clinical features and prognostic factors. 546
-
Upload
patricia-shepherd -
Category
Documents
-
view
212 -
download
0
Transcript of Analysis of molecular breakpoint and m-RNA transcripts in a prospective randomized trial of...

British ]ournu1 of Haematologg. 1995, 89, 546-554
Analysis of molecular breakpoint and m-RNA transcripts in a prospective randomized trial of interferon in chronic myeloid leukaemia: no correlation with clinical features, cytogenetic response, duration of chronic phase, or survival
PATRICIA SHEPHERD, RUTH SUFFOLK, JIM HALSEY* AND NORMAN ALLAN Department of Medicine and MRC Human Genetics Unit, Western General Hospital, Edinburgh, and *CTSU, Radclifle Infirmary, Oxford
Received 10 June, 1994; accepted for publication 5 December 1994
Summary. Two hundred and nineteen cases of Ph tve CML and 15 Ph-ve, BCRfve CML cases have been analysed to determine the breakpoint site and its relationship to clinical features, cytogenetic response, duration of chronic phase and survival. 119 cases have had RNA analysis performed to determine the type of BCR/ABL transcript and have also been analysed in a similar way. Presenting features at diagnosis including age, sex, white-cell count and platelet count showed no significant difference for those with 5’ and 3‘ breakpoints and those with either b2a2 or b3a2 BCR/ABL transcripts. However, in a subgroup of patients whose presenting white-cell count was < lOOx 109/1, those with b3a2 transcript did have a significantly higher platelet count.
Analysis by Sokal risk grouping showed no difference for 5‘ or 3’ breakpoints but a trend for lower stage among those with b2a2 transcripts. No correlation was found either for genomic breakpoint site or BCR/ABL RNA transcript in terms of duration of chronic phase or survival. When stratified by randomized therapy, either interferon-& or standard chemotherapy, no difference was noted in relation to genomic breakpoint site or BCR/ABL transcript. Cyto- genetic response was not related to the molecular findings.
Keywords: CML, DNA analysis, RNA analysis, cytogenetic response, prognosis.
Chronic myeloid leukaemia (CML) is characterized by the presence of the Philadelphia chromosome which at the molecular level arises because of a breakpoint, usually within the major breakpoint cluster region, in the BCR gene (M-BCR) and translocation of the ABL oncogene from chromosome 9 to lie telomeric to promoter sequences of the BCR gene. A fusion BCR/ABL gene is formed which generates usually either a b2a2 or a b3a2 BCR/ABL RNA transcript depending on whether exon b3 of the M-BCR is expressed. A number of papers have addressed the issue of location of the breakpoint within M-BCR and its effect on prognosis and survival. Those suggesting a link between location of breakpoint and outcome are those by Schaefer- Rego et a1 (1987), Eisenberg et a1 (1988), Shtalrid et a1 (1988), Mills et a1 (1988, 1989), Grossman et aZ(1989) and Tanaka & Kamada (1990). These showed some evidence that those with 5’ breakpoints did better than those with 3’
Correspondence: Dr P. Shepherd, Department of Haematology. Western General Hospital, Edinburgh EH4 2XU.
breakpoints. On the other hand, an increasing number of papers have shown no correlation between breakpoint site and outcome (Dyck & Bosco, 1989: Ogawa et al, 1989; Jaubert et aZ, 1990: Morris et al, 1990; Tien et ul, 1990: Tefferi et al, 1990; Opalka et al, 1991; Zaccaria et al, 1992). In a review of these papers (Mills et al, 1991) it was suggested that discrepant results could perhaps be explained best by differences in patient or sample selection. One study has reported BCR/ABL transcripts in CML and found no difference in the type of transcript and survival (Zaccaria et ul, 1993). A further study in a small number of patients did, however, suggest a correlation between the type of BCR/ABL transcript and response to interferon and survival (Inoue et al, 1992). The MRC UK Chronic Myeloid Leukaemia Trial is a multicentre prospective randomized trial of interferon in CML. This provided a unique opportunity to study the location of the breakpoint and the type of BCRIABL m-RNA produced in unselected patients and correlate them with duration of chronic phase and survival, taking into account treatment, clinical features and prognostic factors.
546

DNA and RNA Analysis in CML does not Predict Prognostic Outcome 547 PATIENTS, MATERIALS AND METHODS
The MRC CML I11 Trial is a prospective randomized trial comparing IFN-a (Wellferon) and standard chemotherapy, either busulphan or hydroxyurea, in chronic phase CML. Induction therapy to achieve tumour bulk reduction utilized standard chemotherapy to reduce the white-cell count to < 20 x 109/1 for 4 weeks. At that point, IFN-a was started for those randomized to this arm. The dose of IFN given was 3 MU/d, escalating up to 9-12 MU/d if good control of the WCC was not achieved (< 5 x 109/1) and within patient tolerance. Standard chemotherapy as used for induction therapy was continued in the no IFN-a arm. The trial opened in September 1986. Between December 1988 and February 1991 we tried to collect prospectively samples from all patients randomized into this trial. Samples were requested at diagnosis: if not received a follow-up request was sent. Patients with Ph-ve. BCR-ve disease were excluded from subsequent analysis. During this period we collected 163/ 185 (88%) of possible samples. Of these, 143/185 (77%) were collected within 6 months of randomization and 20/ 185 (11%) more than 6 months from randomization. In addition, we collected samples from 69/152 (54%) patients randomized into the trial prior to December 1988 and 24 patients entered after February 1991 primarily those who were Ph-ve, BCR+ve (six) and 18 who were studied primarily by RNA analysis only. A further two Ph-ve, BCR+ve patients in the trial were analysed elsewhere for location of the breakpoint site by DNA analysis and we also studied two non-trial Ph-ve, BCR+ve patients to determine the breakpoint zone. These four cases are not included in any survival analysis. In total, 219 Ph+ve and 15 Ph-ve, BCR+ve samples were evaluable by DNA analysis, 119 had RNA analysis and 94 had both DNA and RNA analysis.
DNA analysis. High molecular weight DNA was extracted from peripheral blood leucocytes or bone marrow cells using standard proteinase-K digestion and phenol extraction followed by alcohol precipitation. 1Opg of DNA was digested with Bam HI, Hind 111, Bgl I1 restriction enzymes. In some cases, digestion with Eco RI, Xa 11, Sac I and Bcl I1 was carried out. After digestion, samples were run on a 0.8% agarose gel and blotted onto Hybond-N filters. The filters
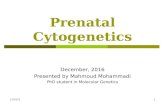
Fig 1. Restriction enzyme map of M-BCR region to show location of zones within M-BCR and categorization as 5’ and 3’ breakpoints taken from Mills et al (1988). The location of the 3’ and 5’ probes used are indicated.
were hybridized with radio-labelled probes. Two probes were used: a 0.6 kb. 3’ Pst 1-Bgl I1 probe (gift of Dr Young) and a 2 kb 5’ probe covering the Bgl-Hind region of the M-BCR (gift of Dr Grosveld) (Fig 1). After hybridization the filters were washed three or four times at 68°C in 0.1% SDS, 0.1% SSC and autoradiographed for 24-72 h. The pattern of rearran- gement with each of the different restriction enzymes was determined, and from this the breakpoint was located in one of four zones: either zone 1 or 2, zone 3, zone 4 or zone 5. Those with a breakpoint 5‘ to the central Hind site, i.e. zones 1 or 2 or zone 3 , had 5’ breakpoints and those 3’ of the Hind site, zones 4 and 5, 3’ breakpoints.
RNA analysis. RNA was isolated from approximately 2 x lo7 frozen white blood cells by resuspension in 4~ guanidinium isothiocyanate and layering on a 5.7 M
caesium chloride solution. The sample was spun at 40K for 3 h at 20°C in a bench-top ultracentrifuge, the supernatant discarded, and the RNA dissolved in 2 0 0 ~ 1 TES, alcohol precipitated, then washed in 700/0 ethanol. The pellet was finally resuspended in 7 pl of DEPC treated sterile water. cDNA was generated using approximately 1 pg of RNA and random hexamers 1 p1 (900.d. units/ml), M-Mol reverse transcriptase (Boehringer Mannheim) 1 u/pl, dNTP’s 1 mM, RNase inhibitor 1 u/p1 in 50 m~ KCI, 10 mM Tris-HCI pH 8.3, MgC12 5 m ~ in a 20p1 reaction. The sample was incubated for 60min at 42°C then denatured at 99°C for 5min and put on ice. PCR reactions were set up in pairs using primers A and B, spanning exons b2, b3 and a2 and using primers B and C spanning the a2 and a3 exons to act as an internal control for the presence of RNA in the sample. The primer sequences were:
A sense b l 5’ GAGCGTGCAGAGTGGAGGGAGAA
B anti-sense a3 5’ TGTGATTATAGCCTAAGACCCGGAG
C sense a2 5’ GGTACCGAATTCAGCGGCCAGTAG
CATCCGG 3’
3’
CATCT 3’
0.5 pg of each primer in a 50 p1 mixture was added to Promega buffer with magnesium chloride (final concentra- tion 2 mu), 10 pl of the cDNA reaction mix and Promega Taq polymerase 2.5 u. Samples were put in a Cetus DNA thermal cycler and denatured at 93°C for 1 min, annealed at 55°C for 1 min and extended at 73°C for 1 min. This was repeated for 35 cycles, the last cycle being held at 73°C for 10min. Samples were run on a 2% TBE gel and stained with ethidium bromide. B3a2 junctions give a 431 bp band and b2a2 junctions a 356bp band. If no band was seen or if samples were being screened for minimal residual disease, a second round of PCR using primers internal to A and B was performed using 5pI of first-round PCR as substrate. The primer sequences were:
D sense 5’ GAAGAAGTGTITCAGAAGCTTCTCC 3’ E anti-sense 5’ GACCCGGAGCTTTTCACCTTTAGTT 3’
Samples from these nested PCRs gave a band of 379 bp representing the b3a2 message and 304 bp representing the b2a2 message.

548 Patricia Shepherd et al
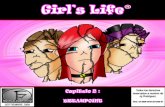
SITE OF BREAKPOINT IN Ph +ve CML Ph -ve BCR +ve CML
n = 219 n = 1 5
’ (55 Yo) \
42 (19%)
Zone 4 Zone 3 84 79
(36 %) 3‘ (42 Yo)
Fig 2. Medical Research Council Chronic Myeloid Leukaemia 111 Trial. DNA analysis to show allocated zones in Ph+ve and Ph-ve. BCRfve CML.
Clinical details. Clinical details of patients were obtained from the database on which registration details and follow- up of patients, including karyotypic information, were recorded at 6-monthly intervals. Clinical staging of patients was done in accordance with the Sokal staging system (Sokal et al, 1984). Cytogenetic response as assessed by 6- monthly marrow examination was defined as ‘minor’ if reduction in number of Ph-positive metaphases to 35-79% occurred, ‘major’ if reduction to 1-34% occurred, and ‘complete’ if there was no Ph chromosome on at least one evaluable cytogenetic sample. Over 20 metaphases were counted in > 80% of patients on IFN-a.
Statistical methods. The log rank method was used to compare the survival of those with 3’ v 5’ breakpoints and those with b2a2 v b3a2 junctions with a follow-up date to 11 March 1994. Patients who had bone marrow transplants during chronic phase were censored at the time of transplant. 63 patients received BMT in this study. Median duration of follow-up for living patients is 53 months (range 20-158 months).
Kaplan-Meier curves for duration of chronic phase and survival were generated. In addition, duration of chronic phase and survival were analysed after stratification for various prognostic factors, particularly age, stage (which includes evaluation of peripheral blood blast and platelet count, spleen size and age) and haemoglobin concentration. Stratification for therapy with interferon against standard chemotherapy was also performed. Standard statistical methods for any difference between the two groups was performed using Student’s t-tests or Wilcoxan rank sum test. Two-tailed P values are quoted throughout.
SPLICE JUNCTIONS IN CML n = 119
Fig 3. Medical Research Council Chronic Myeloid Leukaemia I11 Trial. RNA analysis to show frequency of mRNA transcripts expressed in CML patients.
RESULTS
137/222 evaluable trial samples for DNA analysis and 73/ 1 13 evaluable samples for RNA analysis were studied within

DNA and RNA Analysis in CML does not Predict Prognostic Outcome 549 Table 1. Medical Research Council Chronic Myeloid Leukaemia I11 Trial: breakpoint site and RNA message
Table 111. Medical Research Council CML I11 Trial: relationship between platelet count and breakpoint site.
Zone No. studied b2a2 b,a, b2a2 + b,a2 ~
- 1 or 2 (n = 49) 14 13 1 3 (n = 80) 36 11 24 2 4 (n = 87) 34 2 30 4 5 (n = 8) 4 0 4 - NK (n = 6) 6 2 4 -
the first 6 months of diagnosis. There was no difference in the distribution of breakpoints or type of RNA transcript for the group studied prospectively and those in whom samples were obtained > 6 months from diagnosis or the whole group.
lacation of breakpoints within BCR Of 219 Phfve cases tested, all but six had a breakpoint located to a zone within the M-BCR. Fig 2 shows the percentage of cases in each zone. Overall 55% of cases had 5‘ breakpoint and 42% of cases a 3‘ breakpoint. In six cases the precise breakpoint within the M-BCR could not be deduced from the pattern of rearranged bands seen after Southern blotting and probing with either a 3’ probe or a 5’ probe. However, all showed a rearrangement detected with one of these probes. Analysis of RNA splice patterns in these six cases showed a b2a2 band in two and b3a2 band in three. In the sixth, neither a b2a2 nor a b3a2 nor an ela2 band was detectable. This patient had a rearrangement only with Eco
~ ~~~ ~~
WCC < 100 x 109/1 WCC > 100 io4/i
b2 a2 b3 a2 b2 a2 b3a2 (n = 10) (n = 13) (n = 28) (n = 56)
Platelets ( x 109/1) Mean 381 653 418.1 505.3 Median 351 581 385.5 422.5 Range 162-649 304-1865 142-1390 127-2464
P < 0.01 P = N S
RI on both 3’ and 5’ probes but was negative with Bam HI, Hind 111, Bgl 11, Xba I and Bcl I. Therefore breakpoint appears to be at least 9 kb upstream of the M-BCR.
Fifteen cases of Ph-ve, BCR+ve CML were also mapped. A significantly higher proportion showed breakpoints in zone 2 compared to Ph+ve CML, although the overall numbers of those with 5’ breakpoints compared to 3’ breakpoints was not statistically different. In two cases we were unable to say whether zone 3 or 4 breakpoint was present, because further analysis to determine the exact site within this area was not performed due to lack of DNA.
RNA splice patterns Fig 3 shows the distribution of the particular BCR/ABL hybrid m-RNA produced. In all, 119 patients were studied:
Table 11. Medical Research Council CML I11 Trial: data at diagnosis.
5/ 3/ b2 a2 b3a2 (n = 127) (n = 95) (n = 41) (n = 72)
Mean Hb (g/l) Mean WBC ( x 109/1) Mean platelets ( x 109/1) Mean basophils ( x 109/1) Mean blasts ( x 109/1) Spleen size (cm from costal margin) Liver size (cm from costal margin) Sokal risk group
Low Intermediate High
IFN No IFN Not randomized
Randomized treatment
Mean age f SD
Sex (range)
Male Female
104 108 110 103 220 181 198 207 530 537 395 534
9.9 7.6 7.6 9.4 7.0 4.6 3.7 5.9 9.2 7.3 7.9 8.6 2.1 0.9 1.6 1.4
28 (22%) 28 (30%) 13 (32%)* 11 (16%) 43 (34%) 33 (35%) 17 (41%) 30 (43%) 53 (43%) 33 (35%) 11 (27%) 29 (41%)
62 (49%) 59 (62%) 22 (54%) 40 (56%) 62 (49%) 34 (36%) 19 (46%) 30 (42%) 3 (2%) 2 (2%) 0 (0%) 2 (3%)
49.6 f 12.8 48.6 2z 13.9 48.2 f 13.4 52.7 f 13.2 (13-77) (16-75) (15-74) (20-76)
74 (58%) 55 (58%) 29 (71%) 40 (56%) 53 (42%) 40 (42%) 12 (29%) 32 (44%)
* P value for trend = 0.04. All other values non-significant.

550 Patricia Shepherd et al
> K
50- z w
25-
0 -
CML3 - DNA Breakpoints
3' 9 5 3 6 1.0 5' 1 2 7 5 1 1.0 ( 2 P = 0 . 9 7 )
y .....
3' 9 5 4 2 1.0 5' 1 2 7 5 7 1.0 ( 2 P = 0 . 8 4 ) v~
0 0 1 2 3 4 5
DURATION OF CHRONIC PHASE (YEARS), CENSORED AT BMT
Fig 4. Duration of chronic phase for patients showing either a 5' or 3' breakpoint.
41 (34%) showed a b2a2 junction and 7 2 (61%) a b3a2 junction. In six cases, both b2a2 and b3a2 junctions were detected. 94 of these cases had both DNA analysis and RNA analysis performed. The relationship between the breakpoint zone and the RNA message is shown in Table I. In general, we find that zones 1 or 2 usually have a b2a2 message although one showed a b3a2 message. This must imply that the breakpoint was erroneously ascribed to zone 2, perhaps through co-migration of a rearranged band with the germline. In zone 3 we can see, as expected, that both b2a2 and b3a2 transcripts could be detected although rather more had b3a2 than b2a2. Zone 4 cases showed almost exclusively b3a2 messages, although in two cases a b2a2
message was present which could be due to alternative splicing. All zone 5 cases showed a b3a2 message.
Clinical features at diagnosis Table I1 shows the clinical features at diagnosis according to the breakpoint site and transcript message for evaluable cases. When analysed by DNA breakpoint zone, no statistically significant differences were noted for haemoglo- bin concentration, white-cell count, platelet count, basophil numbers, blast cell numbers, spleen size, liver size or Sokal risk group. Mean ages were similar at 49 years in both groups and male to female ratio was also similar. Similarly, there appeared to be no apparent differences between clinical
CML3 - DNA Breakpoints
N 0 Q / E

DNA and R N A Analysis in CML does not Predict Prognostic Outcome 551
25-
I- z W 0 K W n
3 1 62 22 1.0 5 ‘ 8 0 3 0 1.0 ( 2 P = 0 . 9 6 )
, _ -
CML3 - DNA Breakpoints Only patients diagnosed after 1988
N 0 O / E
characteristics of those with b2a2 and b3a2 breakpoints except for Sokal risk group which was lower among those with b2a2 transcripts ( P for trend = 0.04). In addition, if cases with only a white-cell count < 100 x 109/1 are examined, those with b3a2 breakpoints have a significantly higher platelet count overall than those with b2a2 break- points. This is statistically significant, P < 0.01 (Table 111). There is, however, considerable degree of overlap between the two groups.
Cytogenetic responders Cytogenetic response is rarely seen after the use of hydroxyurea or busulphan but may be seen in patients
75 i 2 z U
50- z w
E j R
treated with IFN-a. In this study we have analysed by DNA analysis 121 F N randomized patients, of whom 107 received IFN-a, and by RNA analysis 62 patients, of whom 60 received IFN-a. On DNA analysis 12/62 (19%) 5’ and 14/59 (24%) 3’ cases showed cytogenetic response ( P = NS). Mean doses of EN-a/week (22 MU, 25 MU) and duration of IFN-a therapy (128 weeks, 124 weeks) respectively were similar. 7/22 (32%) patients with b2a2 junctions and 11/40 (28%) patients with b3a2 junctions showed cytogenetic response (P = NS). Again, mean dose of IFN-&/week and duration of IFN-a therapy were similar (21MU, 24MU; 145 weeks, 147 weeks). Therefore molecular breakpoint location and BCR/ABL transcripts
N 0 O / E b 2 a 2 4 1 17 1.0 b 3 a 2 7 2 3 1 1.0 ( 2 P = 1.04)
0 1 2 3 4 5 DURATION OF CHRONIC PHASE (YEARS), CENSORED AT BMT
Fig 7. Duration of chronic phase for patients expressing b2az and b3a, transcripts.

552 Patricia Shepherd et a1
2 5 -
CML3 - RNA analysis
N 0 O / E b 2 a 2 4 1 1 3 1.0 b 3 a 2 7 2 2 3 1.0 ( 2 P = 1 . 0 5 )
______________. I
show no relationship to the probability of obtaining cytogenetic response.
Prognostic eflect of breakpoint site or type of BCRIABL transcript Analysis of breakpoint site shows no difference between those with 5’ and those with 3’ breakpoints for the duration of chronic phase or survival (Figs 4 and 5 ) censored at the time of BMT if performed. If one looks only at those who were studied prospectively and exclude those who were in the trial prior to December 1988, we can again see that there is no difference between 5’ and 3’ breakpoints for either duration of chronic phase or survival. 5-year survival is 48% and 50% respectively (Fig 6). In addition, there is no difference
100
75
between the individual zones in terms of duration or chronic phase and survival (data not shown). Patients were stratified by type of therapy received, either IFN or standard chemotherapy, and other prognostic parameters, age, stage, and haemoglobin concentration. No significant differences between duration of chronic phase or survival were noted for those with 5’ or 3’ breakpoints stratified by any of these features (data not shown). Likewise, RNA analysis also shows no significant difference in terms of duration of chronic phase or survival for those expressing the b2a2 or the b3a2 transcript (Figs 7 and 8). In those who were studied prospectively, after December 1988, 5-year survival is 52% for b2a2 and 54% for b3a2 (Fig 9).
CMW - RNA analysis ‘---- ........-
Only patients diagnosed after 1988
N 0 O / E b 2 a 2 2 7 6 1.0 b 3 a 2 5 1 16 1.0 ( 2 P = 0.95)
SURVIVAL (YEARS), CENSORED AT BMT IN CHRONIC PHASE Fig 9. Survival of patients diagnosed after 1988 for patients expressing b2a2 or b3az transcripts.

DNA and RNA Analysis in CML does not Predict Prognostic Outcome 5 5 3 Stratification by IFN or chemotherapy and by stage, age, and haemoglobin concentration also showed no significant differences (data not shown).
DISCUSSION
Previous reports on the prognostic significance of molecular breakpoints in CML have given conflicting results in terms of the duration of chronic phase and survival that may have been related in part to patient selection and the inherent heterogeneity in this disease. In this paper we report our results from a prospective multicentre randomized trial of interferon-& in CML. Therefore, theoretically, patient selection should not be important. We have analysed both genomic breakpoints and RNA transcripts seen in patients entered into this trial. Genomic breakpoints were informative in 97% of cases studied. In 3% of cases we were unable to determine the particular site, despite demonstrating rearrangements with a number of enzymes when using both 5‘ and 3’ probes. This may be due to deletion of sequences upstream of the breakpoint. Six cases were found in which the location of the breakpoint could not be pinpointed by restriction enzyme mapping of the M-BCR. RNA analysis showed either b2a2 or b3az transcripts in five of the six cases. The sixth case was unusual in that the breakpoint appeared to be at least 9 kb upstream of the M-BCR. We were unable to identify any RNA transcript in this case, either b2a2, b3az or el a2. This is similar to a report by Negrini et a1 (1992) and has also been reported in small numbers in other series (Saglio et al, 1988, 1990; Bartram et al, 1988; Min et al, 1990; Selleri et al, 1990; Zaccaria et al, 1990). Correlation of RNA transcript with genomic breakpoint sites shows that one-third of zone 3 cases have the b2a2 transcript and two-thirds the b3a2 transcript. One anomalous case was found where an apparent 5’ zone 1 or 2 breakpoint was associated with the b3a2 transcript. Therefore it is probably better to determine the RNA transcript when assessing these patients. Inokuchi et al (1991a, b, 1992) described higher platelet counts in patients with 3’ breakpoints or b3a2 transcripts. A further study by Ardern et a1 (1993) also showed a correlation between 3’ rearrange- ments and higher platelet counts. However, the definition of the breakpoint sites vary between the studies of Inokuchi and those of Ardern, and when the two were compared on the basis of the central Hind I11 site within the M-BCR no correlation was found in Inokuchi’s study. A further series from Opalka et al(1992a, b) showed no correlation with the type of BCR/ARL transcript and platelet counts. Overall in this study we were unable to show a correlation between either genomic or RNA findings and platelet counts (Shepherd et al, 1992). However, when analysed further, we did note significantly higher platelet counts in patients who had a low white-cell count (< 100 x 109/1) at diagnosis for those carrying the b3a2 transcript. Numbers involved at this level are, however, small and therefore prone to statistical error. Overall, we think there may be a subgroup of patients in whom the b3a2 transcript is associated with significant thrombopoiesis. These patients, however, do no worse or better than those in whom the white-cell count is > 100 x 109/1.
Previously published reports on the molecular breakpoint site and prognosis as assessed by duration of chronic phase or survival have largely been on genomic data, but few series have reported RNA data (Zaccaria et al, 1993; Inoue et al, 1992). Our prospectively randomized series has found no prognostic association between genomic breakpoint site or RNA transcript message and duration of chronic phase or survival. There was no difference in outcome for interferon- treated patients or chemotherapy-treated patients according to the defined molecular lesion. Groups studied were similar in prognostic features. This is in contrast to a report by Inoue et a1 (1992) who suggested a correlation between the b3a2 transcripts and clinical response with prolonged survival in a small group of interferon-treated patients. Data from the Italian Study Group suggested a correlation of RNA transcript and cytogenetic response to interferon-& (Zac- caria, 1992). We have been unable to find any such correlation.
In conclusion, we have been unable to identify any significant correlation between molecular lesions as deter- mined at both the genomic and the RNA level for clinical features at diagnosis (except a weak relationship between RNA-determined breakpoint and Sokal stage), karyotypic response to interferon, duration of chronic phase, or survival, taking into account other prognostic and treat- ment-related factors. We hope that this contribution from a large randomized trial will largely settle the issues disclosed.
ACKNOWLEDGMENTS
This work was supported in part by a grant from the Scottish Hospitals Endowment Research Trust (SHERT). We thank all those physicians who entered patients into this trial and provided material for analysis.
REFERENCES
Ardern, J.C., Speak, J., Hyde. K., Hunt, L.P., Lawson, R., Gorst. D.W., Geary, C.G. & Lucas, G.S. (1993) Molecular analysis in chronic granulocytic leukaemia: location of breakpoints within M-BCR and relationship with presentation platelet counts. Clinical and Laboratory Haematology, 15, 2 53-2 58.
Bartram, C., Bross-Bach, U., Schmidt, H. & Waller, H. (1988) Philadelphia-positive chronic myelogenous leukemia with break- point 5’ of the breakpoint cluster region but within the bcr gene. Blut, 55 , 505.
Dyck, J.A. & Bosco, J.J. (1989) Clinical stage of chronic granulocytic leukaemia and bcr breakpoint location in South-East Asian patients. British Journal of Haematology, 72, 64-67.
Eisenberg, A., Silver, R., Soper, L., Arlin, Z., Coleman, M.. Bernhardt, B. & Benn, P. (1988) The location of breakpoints within the breakpoint cluster region (bcr) of chromosome 22 in chronic myeloid leukemia. Leukemia, 2, 642-647.
Grossman. A., Silver, R., Arlin, Z., Coleman, M., Camposano. E., Gascon, P. & Benn, P. (1989) Fine mapping of chromosome 22 breakpoints within the breakpoint cluster region (bcr) implies a role for bcr exon 3 in determining disease duration in chronic myeloid leukemia. American Journal of Human Genetics, 45, 729- 738.

554 Patricia Shepherd et a1 Inokuchi, K., Futaki. M., Yamada, T., Tanabe, Y.. Dan K.,
Shinohara, T., Kuriya, S. & Nomura. T. (1991a). Therelationship between the site of breakpoints within the BCR gene and thrombopoiesis of Philadelphia-positive chronic myelocytic leukaemia. Leukaemia Research, 15, 1067-1073.
Inokuchi, K., Inoue, T., Tojo, A., Futaki. M., Mikake, K., Yamada, T., Tanabe, Y., Ojki, I., Dan, K.. Ozawa. K., Asano, S. & Nomura, T. (1 99 lb) A possible correlation between the type of bcr-abl hybrid messenger RNA and platelet count in Philadelphia-positive chronic myelogenous leukemia. Blood. 78, 3215-3127.
Inokuchi, K. & Nomura, T. (1992) The relationship between the type of bcr-abl hybrid messenger RNA and thrombopoiesis in Philadelphia-positive chronic myelogenous leukemia. kukemia and Lymphoma, 10, 9-15.
Inoue, T., Tojo, A.. Tsuchimoto, D., Okamoto, S., Ogura, H.. Tani, K., Ozawa, K., Shibuya, M. & Asano, S. (1992) Possible correlation between fusion pattern of BCR/ABL mRNA and clinical response to a-interferon in chronic myelogenous leukemia. Leukemia, 6,
Jaubert. J., Martiat, P., Dowding, C., Ifrah. N. & Goldman, J. (1990) The position of the M-BCR breakpoint does not predict the duration of chronic or survival in chronic myeloid leukaemia. British Journal of Huematology. 74, 30-35.
Mills, K.I., Benn. P. & Birnie, G.D. (1991) Does the breakpoint within the major breakpoint cluster region (M-bcr) influence the duration of chronic phase in chronic myeloid leukemia? An analytical comparison of current literature. Blood, 78, 1155-1161.
Mills, K.I., Hynds, S.A., Burnett, A.K., MacKenzie, E.D. & Birnie. G.D. (1989) Further evidence that the site of the breakpoint in the major breakpoint cluster region (M-bcr) may be a prognostic indicator. Leukemia, 3, 837-840.
Mills, K.L. MacKenzie. E. & Birnie, G.D. (1988) The site of the breakpoint within the bcr is a prognostic factor in Philadelphia- positive CML patients. Blood, 72, 1237-1241.
Min, G.L., Martiat, P., Pu, G.I. & Goldman, J. (1990) Use of pulsed field gel electsophoresis to characterize BCR gene involvement in CML patients lacking M-BCR rearrangement. Leukemia, 4,650-656.
Morris. S., Daniel, L., Elias. A. & Leibowitz, D. (1990) Relationship of bcr breakpoint to chronic phase duration, survival, and blast crisis lineage in chronic myelogenous leukemia patients presenting in early chronic phase. Blood, 75, 2035-2041.
Negrini, M.. Tallarico, A.. Pazzi, I., Castagnoli, A.. Cuneo, A. & Castoldi, G.L. (1992) A new chromosomal breakpoint in Ph positive, bcr negative chronic myelogenous leukemia. Cancer Genetics and Cytogenetics, 61, 11-13.
Ogawa. H., Sugiyami. H.. Soma, T., Masaoka, T. & Kishimoto, S. (1 989) No correlation between location of bcr breakpoints and clinical states in Ph-positive CML patients. Leukemia. 3,492-496.
Opalka, B.. Wandl, U.. Beer, U.. Roggenbuck, U., Kloke, 0. & Niederle, N. (1991) Breakpoint localization within the M-bcr and clinical course do not correlate in patients with chronic myelogenous leukemia undergoing alfa interferon therapy. Leukemia, 5 , 452.
Opalka, B., Wandl, U.B.. Kloke, O., Beer, U., Seeber, S. & Niederle, N. (1992a) No correlation between site of breakpoint in the bcr gene and platelet counts in Philadelphia chromosome-positive CML. Leukemia Research, 16, 937-939.
Opalka. B., Wandl, U., Stutenkemper, R., Kloke. 0. & Seeber, S. (1992b) No correlation between the type of bcr-abl hybrid messenger RNA and platelet counts in chronic myelogenous leukemia. Blood, 80, 1854-1855.
948-951.
Saglio, G.. Guerassio, A., Rosso, C., Zaccaria. A., Tassinari. A., Serra, A., Rege-Cambrin, G., Mazza. U. & Gavosto, F. (1990) New type of bcrlabl junction in Philadelphia chromosome-positive chronic myeloid leukemia. Blood. 76, 1819-1824.
Saglio, G., Guerrasio, A.. Tassinari, A., Ponzetto, C.. Zaccaria, A,. Testoni. P.. Celso. B.. Rege, Cambrin. G.. Serra. A,, Pegoraro, L., Avanzi. G., Attadia, V.. Falda. M. & Gavosta, F. (1988) Variability of the molecular defects corresponding to the presence of a Philadelphia chromosome in human malignancies. Blood. 72,
Schaefer-Rego. K.. Dudek, H., Popenoe, D.. Arlin. 2.. Mears. J., Bank, A. & Leibowitz, D. (1987) CML patients in blast crisis have breakpoints localized to a specific region of the BCR. Blood, 70,
Selleri. L., von Lindern. M.. Hermans. A., Meijer, D., Torelli, G . & Grosveld, G. (1990) Chronic myeloid leukemia may be associated with several bcr-abl transcripts including the acute lymphoid leukemia-type 7kb transcript. Blood, 75, 1146-1 153.
Shepherd. P., Bond, C. & Allan, N. (1992) Molecular breakpoints and platelet counts in chronic myeloid leukemia. Blood. 80, 556.
Shtalrid. M., Talpaz, M.. Kurzrock. R., Kantarjian. H., Trujillo, J,, Gutterman, J., Yoffe, G. & Blick, M. (1988) Analysis ofbreakpoints within the bcr gene and their correlation with the clinical course of Philadelphia-positive chronic myeloid leukemia. Blood, 72,
Sokal, J.E.. Cox, E.B., Baccarani. M., Tura, S., Gomez, G.A.. Robertson, J.W., Tso, C.Y., Braun, T.J., Clarkson. B.D., Cer- vantes, F. & Rozman, C.. Italian Cooperative CML Study Group (1984) Prognostic discrimination in ‘good risk’ chronic granulo- cytic leukemia. Blood, 63, 789.
Tanaka, K. & Kamada. N. (1990) Bcr gene rearrangement and expression in chronic myelocytic leukemia. Acta Haematologica.
Tefferi, A., Bren, G.D., Wagner, K.V.. Schaid. D.J., Ash, R.C. & Thibodeau. S.N. (1990) The location of the Philadelphia chromosomal breakpoint site and prognosis in chronic granulo- cytic leukemia. Leukemia, 4, 839-842.
Tien, H.. Wang, C.. Chen, Y.. Shen, M., Wu. H., Lee, F., Chuang, S. & Liu, C. (1990) Chromosome and bcr rearrangement in chronic myelogenous leukaemia and their correlation with clinical states and prognosis of the disease. British Journal of Huematologg, 75,
Zaccaria, A. (1992) DNA rearrangements and type of transcript in a series of CML patients treated with a-IFN: correlation with karyotypic response. (Abstract). 2nd International Conference on CML, Bologna, Italy, p. 225.
Zaccaria, A., Martinelli, G., Buzzi, M., Testoni. N., Farabegoli. P., Zuffa, E., Zamagni, M.D.. Russo, D., Baccarani. M., Ambrosetti. A,, Guerrasio, A., Saglio, G. & Tura, S. (1993) The type of bcriabl junction does not predict the survival of patients with Ph’-positive chronic myeloid leukaemia. British Journal of Haematology, 84,
Zaccaria. A., Martinelli, G., Buzzi, M., Zuffa. E., Zamagni, D.. Testoni. N., Guerrasio, A., Saglio, G. & Tura, S. (1992) M-BCR break-point location does not predict survival in Philadelphia chromosome- positive chronic myeloid leukemia. Hernatologica, 77, 16-20,
Zaccaria, A., Tassinari, A., Testoni, N.. Lauria. F., Tura, S., Algeri. R., Guerrassio. A., Rosso, A. & Saglio, G. (1990) Alternative BCR/ ABL transcripts in chronic myeloid leukemia. Blood, 76, 1663- 1664.
1203-1208.
448-45 5.
485-490.
53, 1559-1568.
469-475.
265-268.