Analysis of exhaled breath condensate in respiratory ... · Analysis of exhaled breath condensate...
20
Therapeutic Advances in Respiratory Disease Review Therapeutic Advances in Respiratory Disease (2007) 1(1) 5–23 DOI: 10.1177/ 1753465807082373 ©SAGE Publications 2007 Los Angeles, London, New Delhi and Singapore Analysis of exhaled breath condensate in respiratory medicine: methodological aspects and potential clinical applications Paolo Montuschi Abstract: Analysis of exhaled breath condensate (EBC) is a noninvasive method for studying the composition of airway lining fluid and has the potential for assessing lung inflammation. EBC is mainly formed by water vapor, but also contains aerosol particles in which several biomolecules including leukotrienes, 8-isoprostane, prostaglandins, hydrogen peroxide, nitric oxide-derived products, and hydrogen ions, have been detected in healthy subjects. Inflammatory mediators in EBC are detected in healthy subjects and some of them are elevated in patients with different lung diseases. Analysis of EBC is completely noninvasive, is particularly suitable for longitudinal studies, and is potentially useful for assessing the response to pharmacological therapy. Identification of selective profiles of biomarkers of lung diseases might also have a diagnostic value. However, EBC analysis currently has important limitations. The lack of standardized procedures for EBC analysis and validation of some analytical techniques makes it difficult comparison of results from different laboratories. Analysis of EBC is currently more useful for relative measures than for quantitative assessment of inflammatory mediators. Reference analytical techniques are required to provide definitive evidence for the presence of some inflammatory mediators in EBC and for their accurate quantitative assessment in this biological fluid. Several methodological issues need to be addressed before EBC analysis can be considered for clinical applications. However, further research in this area is warranted due to the relative lack of noninvasive methods for assessing lung inflammation. Keywords: exhaled breath condensate; airway inflammation; non-invasive assessment; therapeutic monitoring; asthma; chronic obstructive pulmonary disease; eicosanoids Introduction Inflammation has an important pathophysio- logical role in respiratory diseases such as asthma and chronic obstructive pulmonary disease (COPD). [Sabroe et al. 2007; Wenzel et al. 2006; Fixman et al. 2007; Barnes 2000; O’Donnell et al. 2006]. The assessment of lung inflammation is relevant for the management of chronic respiratory diseases as it may indi- cate that pharmacological therapy is required before onset of symptoms and decrease in lung function. Moreover, monitoring of airway inflammation might be useful in the follow- up of patients with respiratory diseases, and for guiding pharmacological therapy. Quantifi- cation of inflammation in the lungs is cur- rently based on invasive methods including the analysis of bronchoalveolar lavage (BAL) fluid, bronchoscopy, and bronchial biopsies [Adelroth, Paolo Montuschi Department of Pharmacology, Faculty of Medicine, Catholic University of the Sacred Heart, Rome, Italy. [email protected] 1998], semi-invasive methods such as sputum induction [Berlyne et al. 2000; Hargreave, 2007], and the measurement of inflammatory biomark- ers in plasma and urine which are likely to reflect systemic rather than lung inflammation. Exhaled breath consists of a gaseous phase that contains volatile compounds (e.g. nitric oxide, carbon monoxide, and hydrocarbons) and a liq- uid phase, termed exhaled breath condensate (EBC), that contains aerosol particles in which several nonvolatile compounds have been iden- tified [Montuschi, 2005a; Mutlu et al. 2001; Kharitonov and Barnes, 2001; Hunt, 2002; Kharitonov and Barnes, 2006; Effros et al. 2005; Horvarth et al. 2005; Cepelak et al. 2007; Montuschi, 2002; Montuschi and Barnes, 2002]. Measurement of exhaled nitric oxide (NO) is a http://tar.sagepub.com 5
Transcript of Analysis of exhaled breath condensate in respiratory ... · Analysis of exhaled breath condensate...

Therapeutic Advances in Respiratory Disease Review
Therapeutic Advances inRespiratory Disease
(2007) 1(1) 5–23
DOI: 10.1177/1753465807082373
©SAGE Publications 2007Los Angeles, London,New Delhi and Singapore
Analysis of exhaled breath condensate inrespiratory medicine: methodological aspectsand potential clinical applicationsPaolo Montuschi
Abstract: Analysis of exhaled breath condensate (EBC) is a noninvasive method for studyingthe composition of airway lining fluid and has the potential for assessing lung inflammation.EBC is mainly formed by water vapor, but also contains aerosol particles in which severalbiomolecules including leukotrienes, 8-isoprostane, prostaglandins, hydrogen peroxide,nitric oxide-derived products, and hydrogen ions, have been detected in healthy subjects.Inflammatory mediators in EBC are detected in healthy subjects and some of them areelevated in patients with different lung diseases. Analysis of EBC is completely noninvasive,is particularly suitable for longitudinal studies, and is potentially useful for assessing theresponse to pharmacological therapy. Identification of selective profiles of biomarkers of lungdiseases might also have a diagnostic value. However, EBC analysis currently has importantlimitations. The lack of standardized procedures for EBC analysis and validation of someanalytical techniques makes it difficult comparison of results from different laboratories.Analysis of EBC is currently more useful for relative measures than for quantitativeassessment of inflammatory mediators. Reference analytical techniques are required toprovide definitive evidence for the presence of some inflammatory mediators in EBC andfor their accurate quantitative assessment in this biological fluid. Several methodologicalissues need to be addressed before EBC analysis can be considered for clinical applications.However, further research in this area is warranted due to the relative lack of noninvasivemethods for assessing lung inflammation.
Keywords: exhaled breath condensate; airway inflammation; non-invasive assessment;therapeutic monitoring; asthma; chronic obstructive pulmonary disease; eicosanoids
IntroductionInflammation has an important pathophysio-logical role in respiratory diseases such asasthma and chronic obstructive pulmonarydisease (COPD). [Sabroe et al. 2007; Wenzelet al. 2006; Fixman et al. 2007; Barnes 2000;O’Donnell et al. 2006]. The assessment of lunginflammation is relevant for the managementof chronic respiratory diseases as it may indi-cate that pharmacological therapy is requiredbefore onset of symptoms and decrease inlung function. Moreover, monitoring of airwayinflammation might be useful in the follow-up of patients with respiratory diseases, andfor guiding pharmacological therapy. Quantifi-cation of inflammation in the lungs is cur-rently based on invasive methods including theanalysis of bronchoalveolar lavage (BAL) fluid,
bronchoscopy, and bronchial biopsies [Adelroth, Paolo MontuschiDepartment ofPharmacology, Facultyof Medicine, CatholicUniversity of the SacredHeart, Rome, [email protected]
1998], semi-invasive methods such as sputuminduction [Berlyne et al. 2000; Hargreave, 2007],and the measurement of inflammatory biomark-ers in plasma and urine which are likely toreflect systemic rather than lung inflammation.Exhaled breath consists of a gaseous phase thatcontains volatile compounds (e.g. nitric oxide,carbon monoxide, and hydrocarbons) and a liq-uid phase, termed exhaled breath condensate(EBC), that contains aerosol particles in whichseveral nonvolatile compounds have been iden-tified [Montuschi, 2005a; Mutlu et al. 2001;Kharitonov and Barnes, 2001; Hunt, 2002;Kharitonov and Barnes, 2006; Effros et al. 2005;Horvarth et al. 2005; Cepelak et al. 2007;Montuschi, 2002; Montuschi and Barnes, 2002].Measurement of exhaled nitric oxide (NO) is a
http://tar.sagepub.com 5

Therapeutic Advances in Respiratory Disease
well accepted, standardized, validated and widelyused method for assessing airway inflamma-tion in patients with asthma who are not beingtreated with inhaled glucocorticoids, can be usedto monitor the response to these drugs, andto assess compliance and can predict asthmaexacerbation [Anonymous, 1999; Anonymous,2005]. Moreover, with the use of exhaled NOmeasurements, maintenance doses of inhaled glu-cocorticoids may be significantly reduced withoutcompromising asthma control [Smith et al.2005]. However, the clinical utility of exhaledNO measurement is currently limited to patientswith asthma, as its role in the management ofother respiratory diseases is not yet known.
Recently, attention has focused on EBC asa noninvasive method for studying the compo-sition of airway lining fluid [Montuschi, 2002;Montuschi and Barnes, 2002a; Effros et al.2005b]. Using urea, which is a freely diffusiblemolecule, as a marker, it has been demonstratedthat a measurable fraction (1 in 24 parts) ofthe EBC in healthy subjects is derived fromaerosolized airway lining fluid [Dwyer, 2001].EBC analysis of inflammatory biomarkers is anoninvasive method which has the potential tobe useful for monitoring airway inflammation inpatients with respiratory diseases, including chil-dren [Montuschi, 2002; Montuschi and Barnes,2002a]. As it is completely noninvasive, EBCalso is suitable for longitudinal studies and formonitor the response to pharmacological therapy.Furthermore, different biomarkers might reflectthe different aspects of lung inflammation oroxidative stress, which is an important compo-nent of inflammation. Identification of selectiveprofiles of biomolecules in different inflammatoryairway diseases might be relevant for differentialdiagnosis in respiratory medicine. Collection ofEBC samples is simple, inexpensive, and safe.However, unlike exhaled NO measurement, EBCtechnique does not provide real-time results asEBC samples need to be assayed for differ-ent biomolecules. Several methodological issues,including standardization of EBC technique andvalidation of analytical methods, need to beaddressed before this approach can be consideredfor applications in the clinical setting.
This review describes the methodology ofthe EBC technique, summarizes the currentknowledge on the biomarkers which havebeen identified in EBC, discusses the advan-tages, the limitations, and the potential clinical
applications of EBC analysis, and providessuggestions for further research in this area.
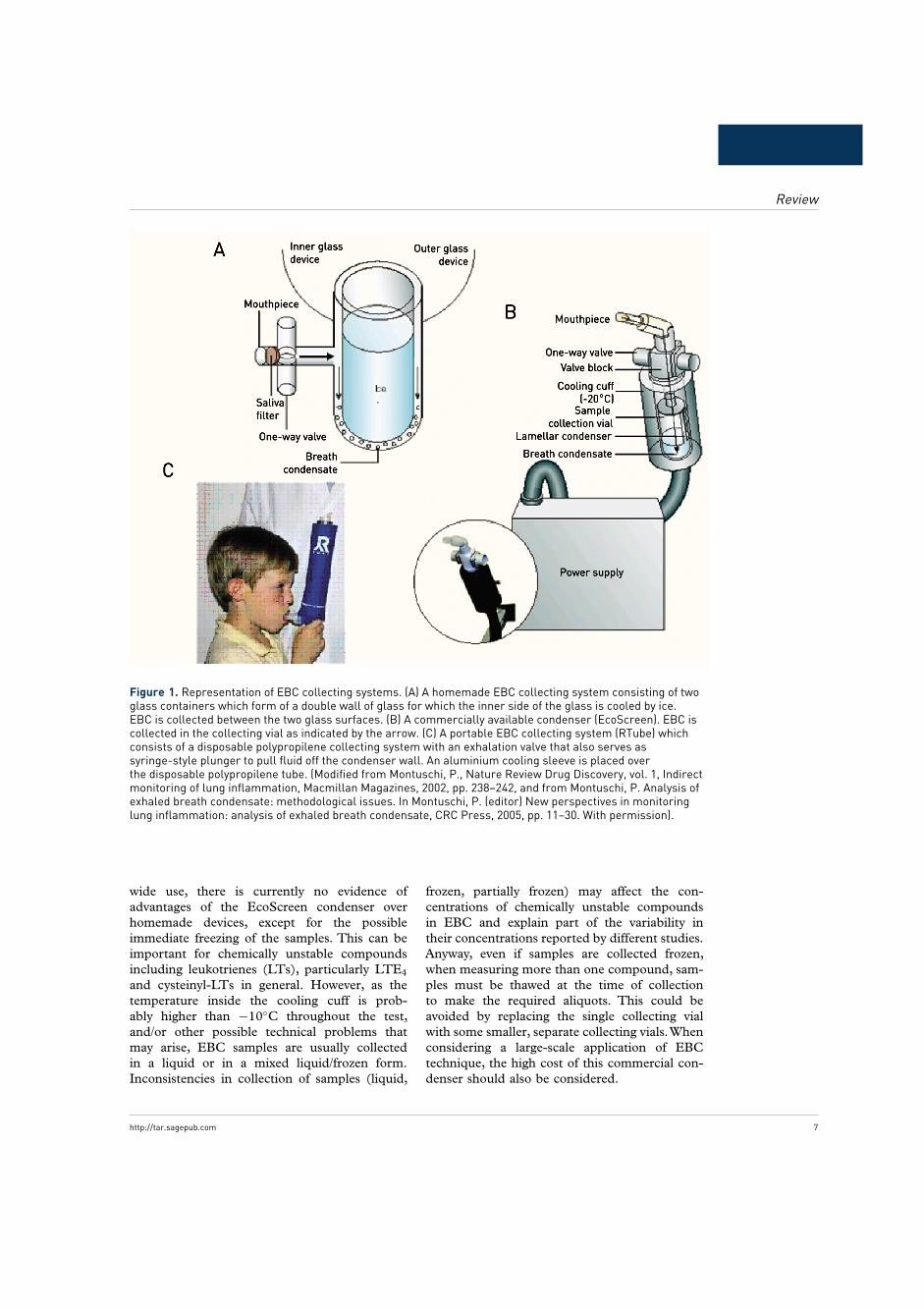
Experimental setupThe collection of EBC sample is simple andeasy to perform. Home-made and commer-cially manufactured condensers are available.Home-made equipment generally consist of amouthpiece with a one-way valve connected toa collecting system which is placed in either iceor liquid nitrogen to cool the breath [Montuschi,2005b]. The collecting system consists of a dou-ble wall of glass, the inner wall of which iscooled by ice (Figure 1A) [Montuschi et al.1999]. Alternatively, jacketed cooling pipes ortubes in buckets have been used [Mutlu et al.2001]. Generally, subjects are asked to breathtidally, with a noseclip on, for 15 min through amouthpiece connected to the condenser. Exhaledair enters and leaves the condensing chamberthrough one-way valves at the inlet and outletwhile the chamber is kept closed. If the col-lecting system consists of two glass containers,EBC is collected between the two glass surfacesat the bottom of the outer glass container in aliquid form [Montuschi et al. 2005b]. Gener-ally, 1.0–2.5 mL of EBC is collected in 15 minbased on respiratory parameters (minute ventila-tion, respiratory rate, tidal volume), material ofcondenser surfaces, temperature, and turbulenceof airflow.
Commercially manufactured condensers are alsoavailable [Montuschi et al. 2000; Montuschi andBarnes, 2002b].The EcoScreen® (JaegerTonnies,Hoechberg, Germany) is an electric refriger-ated system which consists of a mouthpiece witha one-way valve and a collecting system con-nected to a power supply by an extendable arm(Figure 1B). Subjects breath through the mouth-piece that is connected to a valve block in whichinspiratory and expiratory air are separated. Thevalve block is connected to the collecting system,consisting of a lamellar condenser, and a samplecollection vial. The collecting system is insertedinto a cooling cuff maintained at a cold temper-ature by a refrigerator. The actual temperatureinside the cooling cuff and, more importantly,into the cooling system, is not known. Accord-ing to the information provided by the man-ufacturers, the temperature inside the coolingcuff is −10◦C. During expiration, the air flow-ing through the lamellar condenser condenseson the inner surface of the lamellar condenserand drops into the collecting vial. Despite it’s
6 http://tar.sagepub.com
Review
Figure 1. Representation of EBC collecting systems. (A) A homemade EBC collecting system consisting of twoglass containers which form of a double wall of glass for which the inner side of the glass is cooled by ice.EBC is collected between the two glass surfaces. (B) A commercially available condenser (EcoScreen). EBC iscollected in the collecting vial as indicated by the arrow. (C) A portable EBC collecting system (RTube) whichconsists of a disposable polypropilene collecting system with an exhalation valve that also serves assyringe-style plunger to pull fluid off the condenser wall. An aluminium cooling sleeve is placed overthe disposable polypropilene tube. (Modified from Montuschi, P., Nature Review Drug Discovery, vol. 1, Indirectmonitoring of lung inflammation, Macmillan Magazines, 2002, pp. 238–242, and from Montuschi, P. Analysis ofexhaled breath condensate: methodological issues. In Montuschi, P. (editor) New perspectives in monitoringlung inflammation: analysis of exhaled breath condensate, CRC Press, 2005, pp. 11–30. With permission).
wide use, there is currently no evidence ofadvantages of the EcoScreen condenser overhomemade devices, except for the possibleimmediate freezing of the samples. This can beimportant for chemically unstable compoundsincluding leukotrienes (LTs), particularly LTE4
and cysteinyl-LTs in general. However, as thetemperature inside the cooling cuff is prob-ably higher than −10◦C throughout the test,and/or other possible technical problems thatmay arise, EBC samples are usually collectedin a liquid or in a mixed liquid/frozen form.Inconsistencies in collection of samples (liquid,
frozen, partially frozen) may affect the con-centrations of chemically unstable compoundsin EBC and explain part of the variability intheir concentrations reported by different studies.Anyway, even if samples are collected frozen,when measuring more than one compound, sam-ples must be thawed at the time of collectionto make the required aliquots. This could beavoided by replacing the single collecting vialwith some smaller, separate collecting vials.Whenconsidering a large-scale application of EBCtechnique, the high cost of this commercial con-denser should also be considered.
http://tar.sagepub.com 7

Therapeutic Advances in Respiratory Disease
The EcoScreen® II (Jaeger Tonnies, Hoechberg,Germany) has recently been manufactured.This condenser allows to measure respiratoryparameters during the collection of EBC. Alter-natively, the EcoScreen can be connected to apneumotachograph and a computer for onlinerecording of respiratory parameters [Montuschiet al. 2003a]. Another advantage of the Eco-Screen II is that EBC derived from the airwaysor the alveoli can be collected at the same timeinto two separate collecting systems consistingof plastic bags inserted into a refrigerating sys-tem. This device might be useful for studyingthe origin of biomarkers in the lung compart-ments (airways vs alveoli). Compared with thematerial of the collecting system surface (plas-tics vs Teflon-coated metal) might also turnedout to be more appropriate for some compounds(e.g. lipids). However, no published studies areavailable with this condenser.
The RTube® (Respiratory Research, Inc.,Charlottesville, VA) is another commerciallyavailable condenser which has the advantageof being portable [Hunt, 2002]. This deviceconsists of a disposable polypropylene collect-ing system with an exhalation valve that alsoserves as syringe-style plunger to pull fluid offthe condenser wall (Figure 1C) [Hunt, 2002].The refrigerating system consists of an aluminiumcooling sleeve which is placed over the disposablepolypropilene tube (Figure 1C). The tempera-ture of the cooling sleeve can be chosen. Thedevice prevents salivary contamination, and nodetectable amylase concentrations in EBC havebeen reported [Hunt, 2002]. The RTube hasbeen originally manufactured for measuring pHin EBC samples, but it can be used for measuringother compounds [Hunt, 2002]. As measurementof pH in EBC requires deaeration for removal ofcarbon dioxide, a separate device, the pHTube®
(Respiratory Research, Inc., Charlottesville, VA)can be used for this purpose [Hunt, 2002].The RTube is portable, which makes it pos-sible to collect EBC samples at home, whichis particularly suitable for longitudinal studiesor when collection of several samples a day isrequired; the EBC sample in a polypropylenetube can be stored in a freezer at home; a suf-ficient volume of EBC for pH measurement canbe collected in as little as 1 min [Hunt, 2002].However, the RTube has some limitations as EBCsamples need to be brought to the laboratoryfor biochemical assays, and storage conditions infreezer at home (−20◦C) are different from those
required by some chemically unstable mediatorswhich need to be stored immediately at −80◦C.One study reported that compared with RTube,collection of exhaled breath by EcoScreen allowslarger volumes to be collected and detects proteinand lipid mediators with greater sensitivity, whichmight be due to the differences in the collec-tion temperature [Soyer et al. 2006], but furtherstudies to address this issue are required.
Careful sterilization of the EBC equipment isrequired to avoid cross-contamination, althoughstandardized procedures for sterilization of con-densers are not available. It is reasonable to leavethe EBC equipment in an antibacterial solu-tion such as 1% aqueous solution of sodiumhypochlorite for at least 1 h. After sterilization,the EBC collecting system needs to be washedthoroughly with water to remove the antisepticsolution and dried. Some collecting systems suchas the lamellar condenser in the EcoScreen arecoated with Teflon® (E.I. du Pont de Nemours &Company, Inc., Washington, DE) to avoid adhe-sions of biomolecules to the collecting systemsurfaces and the consequent artifactual decreasein their concentrations in EBC. At present, theeffect of different collecting system materials onthe detection of different biomolecules in EBCis largely unknown. The best collecting systemmaterial is likely to be different depending on thephysicochemical properties of the biomoleculeto be detected. A condenser with borosilicateglass coating has been shown to be superior tosilicone, aluminium, polypropylene, and Teflonfor detection of albumin in EBC [Rosias et al.2006]. The effect of antiseptic solutions on theEBC collecting system materials are not currentlyknown. Whether the antiseptic solutions interactand damage the material of the collecting systemsneeds to be clarified. Technical improvementsin the design of new condensers would allowto collect simultaneously several frozen aliquotsmaking it possible to measure different markerswithout thawing the whole sample. The possi-bility of using selective sensors to make on-linemeasurements of hydrogen peroxide [Gajdocsiet al. 2003] and possibly other specific inflam-matory mediators in the breath is currently underinvestigation.
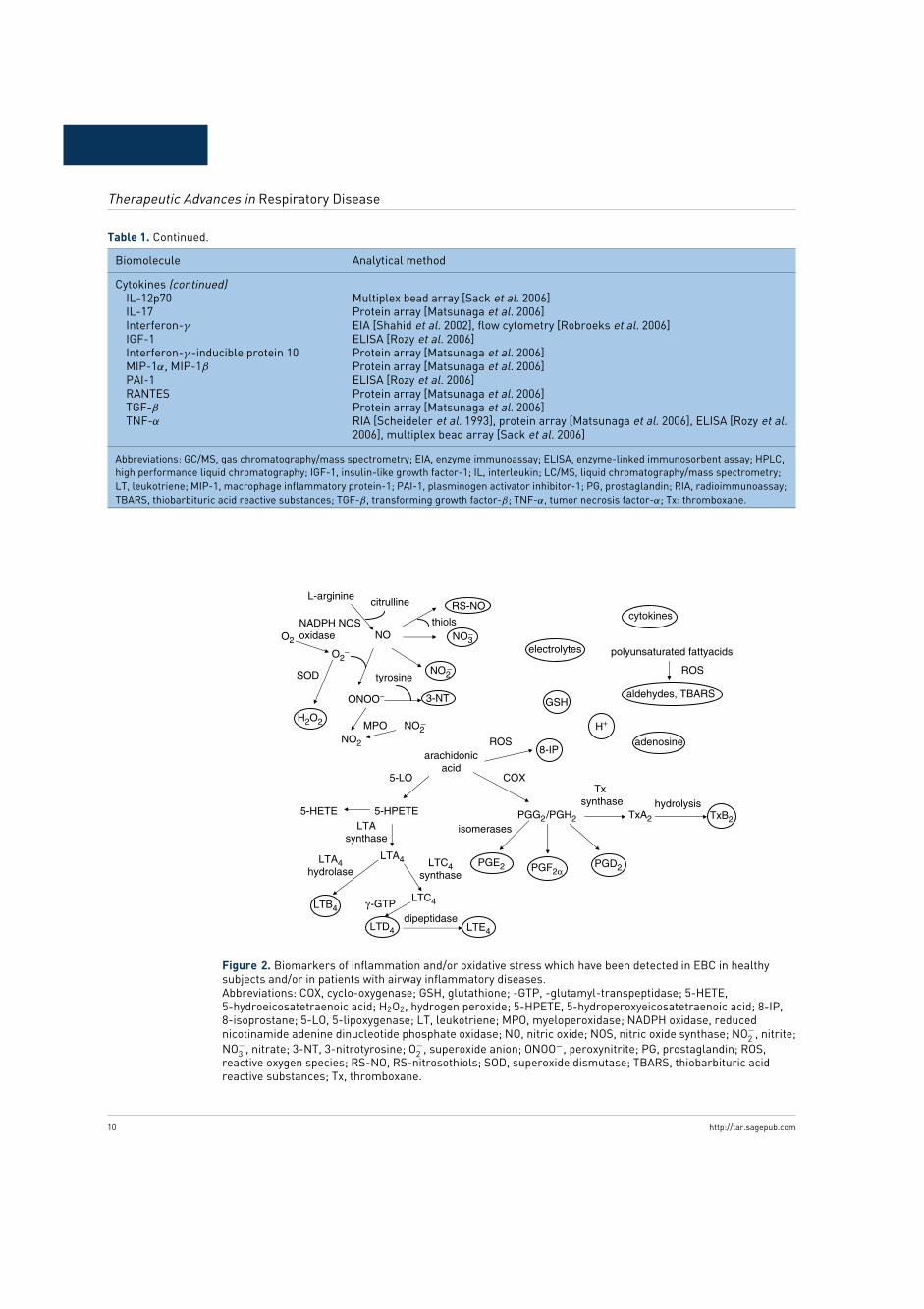
Markers of inflammation in EBCSeveral biomolecules have been detected in EBCof healthy subjects and of patients with differ-ent inflammatory lung diseases (Table 1 andFigure 2). In most studies, markers in EBC were
8 http://tar.sagepub.com

Review
Table 1. Biomolecules in EBC.
Biomolecule Analytical method
Isoprostanes8-Isoprostane (15-F2t-IsoP) GC/MS [Carpenter et al. 1998], RIA [Montuschi et al. 2003a; Montuschi et al. 2003b;
Mondino et al. 2004; Baraldi et al. 2003a; Montuschi et al. 2006; Montuschi et al.2005b], EIA [Montuschi et al. 1999; Montuschi et al. 2000; Montuschi and Barnes,2002b; Antczak et al. 2001; Shahid et al. 2005; Montuschi et al. 2002; Baraldi et al.2003b; Kostikas et al. 2003; Biernacki et al. 2003; Carpagnano et al. 2003a;Zanconato et al. 2004]
LeukotrienesLTB4 LC/MS/MS [Montuschi et al. 2004a; Montuschi et al. 2005a], GC/MS [Cap et al. 2004],
EIA [Montuschi and Barnes, 2002b; Montuschi et al. 2003c; Antczak et al. 2001;Mondino et al. 2004; Biernacki et al. 2003; Montuschi et al. 2005b; Hanazawa et al.2000; Csoma et al. 2002]
LTD4 GC/MS [Cap et al. 2004]LTE4 GC/MS [Cap et al. 2004], EIA [Mondino et al. 2004; Montuschi et al. 2006; Shibata
et al. 2006]Cys-LTs (LTC4/LTD4/LTE4) EIA [Antczak et al. 2001; Baraldi et al. 2003b; Hanazawa et al. 2000; Carraro et al.
2005; Csoma et al. 2002]Prostanoids
PGE2 GC/MS [Carpenter et al. 1998], RIA [Montuschi et al. 2003b; Montuschi et al. 2005b],EIA [Montuschi and Barnes, 2002b]
PGF2α EIA [Montuschi and Barnes, 2002b]PGD2 EIA [Montuschi and Barnes, 2002b]TxB2 RIA [Vass et al. 2003; Mondino et al. 2004; Huszar et al. 2005], EIA [Montuschi and
Barnes, 2002b]Hydrogen ions pH meter or pH microelectrode [Hunt et al. 2000; Vaughan et al. 2003; Kostikas et al.
2002; Larstad et al. 2003; Shimizu et al. 2007; Nicolau et al. 2006; Walsh et al.2006; Dupont et al. 2006; Prieto et al. 2007; Paget-Brown et al. 2005; Kullmannet al. 2006]
Hydrogen peroxide Spectrophotometry [Horvath et al. 1998; Dekhuijzen et al. 1996], fluorometric assay[Schleiss et al. 2000; Jobsis et al. 1997], chemiluminescence [Zappacosta et al.2001]
Nitrogen reactive speciesNitrite Spectrophotometry [Cunningham et al. 2000; Corradi et al. 2001], fluorometric assay
[Balint et al. 2001]Nitrate Fluorometric assay [Balint et al. 2001]S-Nitrosothiols Spectrophotometry [Corradi et al. 2001], fluorometric assay [Kharitonov et al. 2002]3-Nitrotyrosine GC/MS [Larstad et al. 2005; Celio et al. 2006], LC/MS [Goen et al. 2005; Baraldi et al.
2006], HPLC [Celio et al. 2006], EIA [Hanazawa et al. 2000]Adenosine HPLC [Vass et al. 2003]Glutathione HPLC [Corradi et al. 2003b]Aldehydes LC/MS [Corradi et al. 2003a; Corradi et al. 2003b], HPLC [Larstad et al. 2002]TBARS Spectrofluorimetry [Nowak et al. 1999]DNA PCR [Gessner et al. 2004; Carpagnano et al. 2005]Electrolytes (sodium, potassium, calcium,magnesium, chloride)
Ion-selective electrodes [Effros et al. 2002], ion chromatography [Effros et al. 2003]
Keratin Proteomics [Gianazza et al. 2003], ELISA [Jackson et al. 2007]Cytokines
IL-1β EIA [Scheideler et al. 1993], multiplex bead array [Sack et al. 2006]IL-2 Flow cytometry [Robroeks et al. 2006]IL-4 Protein array [Matsunaga et al. 2006], flow cytometry [Robroeks et al. 2006], ELISA
[Shahid et al. 2002]IL-5 ELISA [Profita et al. 2006]IL-6 Multiplex bead array [Sack et al. 2006], EIA [Bucchioni et al. 2003; Carpagnano et al.
2003b], ELISA [Rozy et al. 2006]IL-8 Protein array [Matsunaga et al. 2006], multiplex bead array [Sack et al. 2006], ELISA
[Cunningham et al. 2000]IL-10 Flow cytometry [Robroeks et al. 2006], multiplex bead array [Sack et al. 2006]
(continued)
http://tar.sagepub.com 9
Therapeutic Advances in Respiratory Disease
Table 1. Continued.
Biomolecule Analytical method
Cytokines (continued)IL-12p70 Multiplex bead array [Sack et al. 2006]IL-17 Protein array [Matsunaga et al. 2006]Interferon-γ EIA [Shahid et al. 2002], flow cytometry [Robroeks et al. 2006]IGF-1 ELISA [Rozy et al. 2006]Interferon-γ -inducible protein 10 Protein array [Matsunaga et al. 2006]MIP-1α, MIP-1β Protein array [Matsunaga et al. 2006]PAI-1 ELISA [Rozy et al. 2006]RANTES Protein array [Matsunaga et al. 2006]TGF-β Protein array [Matsunaga et al. 2006]TNF-α RIA [Scheideler et al. 1993], protein array [Matsunaga et al. 2006], ELISA [Rozy et al.
2006], multiplex bead array [Sack et al. 2006]
Abbreviations: GC/MS, gas chromatography/mass spectrometry; EIA, enzyme immunoassay; ELISA, enzyme-linked immunosorbent assay; HPLC,high performance liquid chromatography; IGF-1, insulin-like growth factor-1; IL, interleukin; LC/MS, liquid chromatography/mass spectrometry;LT, leukotriene; MIP-1, macrophage inflammatory protein-1; PAI-1, plasminogen activator inhibitor-1; PG, prostaglandin; RIA, radioimmunoassay;TBARS, thiobarbituric acid reactive substances; TGF-β, transforming growth factor-β; TNF-α, tumor necrosis factor-α; Tx: thromboxane.
arachidonicacid
5-HPETE5-HETE
LTA4
LTC4
LTD4
LTB4
LTE4
PGG2/PGH2 TxA2 TxB2
PGE2 PGF2αPGD2
8-IP
NO
RS-NO
NO3−
ONOO− 3-NT
O2−
O2
H2O2
NO2
NO2−
NO2−
MPO
NADPH NOSoxidase
L-arginine citrulline
tyrosineSOD
thiols
5-LO COX
ROS
LTAsynthase
LTA4hydrolase
LTC4synthase
γ -GTPdipeptidase
isomerases
Txsynthase hydrolysis
polyunsaturated fattyacids
aldehydes, TBARS
ROS
adenosine
GSH
electrolytes
cytokines
H+
Figure 2. Biomarkers of inflammation and/or oxidative stress which have been detected in EBC in healthysubjects and/or in patients with airway inflammatory diseases.Abbreviations: COX, cyclo-oxygenase; GSH, glutathione; -GTP, -glutamyl-transpeptidase; 5-HETE,5-hydroeicosatetraenoic acid; H2O2, hydrogen peroxide; 5-HPETE, 5-hydroperoxyeicosatetraenoic acid; 8-IP,8-isoprostane; 5-LO, 5-lipoxygenase; LT, leukotriene; MPO, myeloperoxidase; NADPH oxidase, reducednicotinamide adenine dinucleotide phosphate oxidase; NO, nitric oxide; NOS, nitric oxide synthase; NO−
2 , nitrite;NO−
3 , nitrate; 3-NT, 3-nitrotyrosine; O−2 , superoxide anion; ONOO−, peroxynitrite; PG, prostaglandin; ROS,
reactive oxygen species; RS-NO, RS-nitrosothiols; SOD, superoxide dismutase; TBARS, thiobarbituric acidreactive substances; Tx, thromboxane.
10 http://tar.sagepub.com

Review
measured with immunoassays, which need to bevalidated with reference analytical methods suchas mass spectrometry or high performance liq-uid chromatography (HPLC). These techniquesalso will accurately quantify the concentrationsof the different markers in EBC. The presenceof LTB4 [Montuschi et al. 2004a; Montuschiet al. 2005a], 8-isoprostane [Carpenter et al.1998] PGE2 [Carpenter et al. 1998], aldehydes[Corradi et al. 2003a] and free 3-nitrotyrosine inEBC has been confirmed by mass spectrometry[Goen et al. 2005; Larstad et al. 2005]. LTB4
[Montuschi et al. 2004a, 2005b] and aldehydes[Corradi et al. 2003] in EBC have been mea-sured by liquid chromatography/mass spectrom-etry (LC/MS), whereas 8-isoprostane and PGE2
in EBC have been measured by gas chromatog-raphy/mass spectrometry (GC/MS) [Carpenteret al. 1998]. Free 3-nitrotyrosine has been mea-sured by both LC/MS [Goen et al. 2005] andGC/MS [Larstad et al. 2005]. Adenosine [Vasset al. 2003], reduced glutathione [Corradi et al.2003], and malondialdehyde (MDA) [Larstadet al. 2002] in EBC have been detectedby HPLC. In patients with asthma exacerba-tions, pH values in EBC are more than twolog orders lower than normal and normal-ize with glucocorticoids [Hunt et al. 2000].Measurement of pH in EBC is very repro-ducible, relatively easy to perform, and pro-vides almost real-time results [Vaughan et al.2003]. This technique could prove to be use-ful for diagnosis and for monitoring therapeu-tic response [Vaughan et al. 2003]. pH valuesin EBC from patients with other lung diseaseshave been reported [Kostikas et al. 2002], butthe biological significance of these data needsto be clarified.
There is a high interindividual variability in thetotal amount of proteins of concentrations inEBC in healthy subjects (from undetectable to1.4 mg) [Scheideler et al. 1993]. At present,the reasons for this variability are unknown.Establishing the protein concentrations in EBCunder standardized conditions is a priority in thisreasearch area. One study has shown that pro-tein concentrations in EBC in 20 healthy subjectsaveraged 2.3 mg/dl [Effros et al. 2002].
Using immunoassays, cytokines have beendetected in EBC in healthy subjects and inpatients with different inflammatory airway dis-eases [Scheideler et al. 1993; Cunninghamet al. 2000; Shahid et al. 2002]. However,
immunoassays for cytokines in EBC still need tobe validated by reference analytical techniques.Moreover, concentrations of cytokines reportedin most studies are close to the detection limitof the assay. At these concentrations, analyticaldata are less reliable. However, due to its bio-logical importance, the issue of the presence ofcytokines in EBC and their accurate quantita-tive measurement in this biological fluid deservesfurther investigation.
Comparisons between absolute concentrationsof EBC markers that have been reported bydifferent studies are currently difficult due todifferences in the EBC collection procedures,condensers, and sample storage and handling;differences in the analytical techniques used;incomplete identification of factors that affectEBC analysis; differences in clinical characteris-tics of study groups (diagnostic criteria, diseaseseverity, pharmacological therapy); interindivid-ual biological variability. The use of referenceindicators in EBC (e.g. electrolytes or conduc-tivity) has been proposed to take into accountchanges in respiratory solute concentrationswhich can result from variations in the dilutionof the respiratory droplets [Effros et al. 2002,2003].
Methodological issuesStandardization of the EBC method and valida-tion of the analytical techniques for measuringeach inflammatory biomarker are required forcomparing data from different laboratories andassessing the clinical utility of EBC analysis.Methodological issues that need to be addressedinclude flow dependence, time dependence, andinfluence of respiratory patterns; origin(s) ofmarkers in EBC; organ specificity of EBC; pos-sible nasal, saliva, and sputum contamination;identification of reference indicators in EBC toascertain to what extent EBC reflects the com-position of airway lining fluid and to adjustfor possible changes in the dilution of respira-tory droplets; influence of temperature, humidity,and collecting-system materials; reproducibilitystudies (between days variability, intrasubjectdiurnal variability); comparisons of collectiondevices; storage issues; possible need for sam-ple pretreatment; for most biomolecules in EBC,the demonstration of their presence in EBC andtheir accurate quantitative measurement by ref-erence analytical techniques (e.g. MS, HPLC);the validation of sensitive, specific, and repro-ducible immunoassays to be used routinely.
http://tar.sagepub.com 11

Therapeutic Advances in Respiratory Disease
Flow dependence and influence ofrespiratory patternsOne study in 15 healthy adults has shownthat hydrogen peroxide concentrations in EBCdepend on expiratory flow rate indicating thatexhaled hydrogen peroxide levels are flow depen-dent [Schleiss et al. 2000]. In six healthy adults,MDA concentrations in EBC collected at threedifferent flow rates were similar [Corradi et al.2003] indicating that MDA concentrations arenot flow dependent. In four healthy children,MDA and glutathione concentrations in EBCsamples collected at different flow rates were sim-ilar [Corradi et al. 2003b]. To study the influenceof ventilation patterns on 8-isoprostane, a markerof lipid peroxidation, and PGE2 concentrationsin EBC, we asked 15 healthy adults to breathat expiratory minute ventilation of 10, 20, and30 L/min for 10, 10, and 5 min, respectively[Montuschi et al. 2003a]. There was no differ-ence in mean 8-isoprostane and PGE2 concen-trations in EBC collected at different expiratoryminute ventilations indicating that the concentra-tions of these eicosanoids in EBC are not influ-enced by this respiratory parameter [Montuschiet al. 2003a]. The lack of correlation between8-isoprostane concentrations in EBC and minuteventilation in mechanically ventilated patientssupports our data [Carpenter et al. 1998]. Like-wise, LTB4 and LTE4 concentrations in EBCwere similar in five healthy subjects who breathedat 14 and 28 breaths/min for 15 min, maintainingthe same tidal volume [Montuschi and Barnes,2003b]. Other authors have demonstrated thatnitrite and protein concentrations in EBC areindependent of respiratory pattern [McCaffertyet al. 2004] and that ethanol concentrationsin EBC samples collected after tidal breathingand deep inspiration and expiration are similar[Rickmann et al. 2001]. These findings indicatethat different markers in EBC behave differ-ently regarding flow dependence and ventilationpatterns. For this reason, each marker should bestudied individually.
For several markers, there is no informationon the influence of airflow and/or ventilationpatterns on their concentrations in EBC andadditional studies are required. Moreover, theinfluence of ventilation patterns on markersin EBC has been mainly studied in healthysubjects and these findings cannot be directlyextrapolated to patients with inflammatory lungdiseases. Assessing the flow dependence ofdifferent biomarkers in EBC is important for
the standardization of this technique as EBCsampling will be performed either at a constantflow rate for a fixed time, or at a constant exhaledvolume for a variable time.
8-Isoprostane concentrations in EBC do notdepend on the duration of EBC collection[Carpenter et al. 1998]. Conflicting results havebeen reported for MDA as in one study MDAconcentrations in samples collected at 10 and20 min were similar [Corradi et al. 2003a],whereas other authors showed that MDA levelsdecreased with prolonged sampling time [Larstadet al. 2003] in analogy to hydrogen peroxideconcentrations in EBC [Svensson et al. 2003]Sampling time is likely to be relevant to EBCconcentrations of unstable compounds such ascysteinyl-LTs or hydrogen peroxide. Additionalstudies are warranted to establish the effect ofsampling time on different biomolecules in EBCand to establish the ideal sampling time for eachof them.
The volume of EBC collected depends on breathtest duration, total exhaled volume, and ventila-tion rate. In healthy subjects, the mean volumesof EBC collected in a 15-min test were almosttwo-fold higher at 28 breaths/min compared withthose at 14 breaths/min [Montuschi et al. 2002b].In healthy subjects, EBC volume is correlatedwith expiratory minute ventilation, although thecondenser efficiency decreases at the higher expi-ratory minute ventilation values [McCaffertyet al. 2004]. The mean volume of EBC collectedduring 10 min of tidal breathing was about 58%of that collected during 20 min of tidal breath-ing [Corradi et al. 2003]. In healthy subjects,the volume of EBC collected is increased whensubjects inhale through their noses and exhalethrough their mouths without wearing a noseclipprobably due to an increase in minute ventilationwhen sample collection is performed without anoseclip [Vass et al. 2003].
Origin(s) of markers in EBCThree aspects related to the origin of mark-ers in EBC need to be considered: their cellu-lar source; the compartment of the respiratorysystem in which they are produced (airways vsalveolar region); the extent to which EBC reflectsthe composition of airway lining fluid and lunginflammation.
EBC technique does not provide direct infor-mation on the inflammatory cells in the
12 http://tar.sagepub.com

Review
respiratory system. Identifying the cellularsource(s) of markers in EBC requires invasivetechniques such as bronchoscopy. A correlationbetween the concentrations of a biomoleculein EBC and a cell type can provide indi-rect information on the cellular source of thatbiomolecule. However, this does not necessar-ily imply that the biomolecule is released bythat cell type as increased biomolecule concen-trations in EBC could also reflect cell activationwithout increased cell counts. Flow dependencemight indicate whether a certain inflammatorymediator is mainly derived from the airways orthe alveoli [Schleiss et al. 2000]. If the concen-trations of a biomolecule in EBC depend onexpiratory flow rate, this could imply that thebiomolecule is mainly derived from the airwaysas flow rate affects the time available for itsaccumulation in the airways, and therefore itsEBC concentrations [Schleiss et al. 2000]. Incontrast, the lack of flow dependence would indi-cate that the biomolecule is mainly derived fromthe alveolar region where flow rate has a minorrole [Schleiss et al. 2000]. As it is flow depen-dent, hydrogen peroxide in EBC should primar-ily be derived from the airways [Schleiss et al.2000], whereas 8-isoprostane [Montuschi et al.2003a; Carpenter et al. 1998], PGE2 [Montuschiet al. 2003a; Montuschi and Barnes, 2002b],glutathione [Corradi et al. 2003a], and aldehy-des [Corradi et al. 2003] should primarily bederived from the alveolar region. These studieswere performed in healthy subjects. In patientswith inflammatory lung disease, the increasednumbers and/or activation of selective inflamma-tory cell types in different compartments of therespiratory system and the high-current velocitywhich can facilitate formation of aerosol particlescontaining nonvolatile inflammatory mediators[Hunt, 2002] might have a different impact onthe concentrations of a specific biomolecule inEBC compared with healthy subjects.
The origin of nonvolatile inflammatory markerswhich are probably contained in aerosol parti-cles (e.g. proteins) in EBC can also be stud-ied by identifying cell-specific markers such askeratin and total phospholipid, which is foundprimarily in surfactant [Jackson et al. 2007].Both airway and alveolar compartments con-tribute to the formation of EBC [Jackson et al.2007]. Using ethanol as a model compound,it has been shown that the ratio between thetwo compartments depends on ventilation, witha shift towards the alveolar region during forced
ventilation [Rickmann et al. 2001]. Studies onthe mechanisms of EBC formation are requiredto established to what extent EBC reflects thecomposition of airway lining fluid.
Whether the concentrations of inflammatorymediators in EBC reflects lung inflammation orsystemic production of these compounds, par-ticularly under conditions of increased perme-ability [Carpenter et al. 1998], is still unknown.Measurement of inflammatory mediators inpatients with systemic inflammatory diseases(e.g. systemic lupus erythematosus) and com-parisons between concentrations of inflamma-tory mediators in EBC and in biological fluids(e.g. plasma and/or urine) reflecting systemicproduction of these compounds might be useful.
Dilution reference indicatorsThe use of dilution reference indicators has beenproposed to 1) estimate the concentrations ofnonvolatile inflammatory mediators in respira-tory fluid; 2) to normalize for interindividualvariations in droplet formation. Although mostEBC is derived from water vapor, the pres-ence of nonvolatile compounds in EBC indi-cates that droplets of the respiratory fluids arecollected [Effros et al. 2002]. Calculation ofairway lining fluid solute concentrations fromEBC requires estimation of the dilution factor.Using electrolyte concentrations in EBC as dilu-tion reference indicator, it has been estimatedthat respiratory fluid represents between 0.01and 2% of EBC volume [Effros et al. 2002].Due to this high variability in the dilution ofrespiratory droplets by water vapor, it has beenargued that increased concentrations of inflam-matory mediators in EBC reported in differentlung diseases could reflect increased droplet for-mation [Effros et al. 2003]. The selective increaseof biomolecules in EBC and the lack of cor-relation between concentrations of structurallyrelated compounds in EBC are not consistentwith this hypothesis [Montuschi and Barnes,2002b]. Measurements of electrolytes, urea, orconductivity have been proposed as dilution ref-erence indicators in EBC [Effros et al. 2003], buttheir role in EBC analysis is debated. Alterna-tively, EBC data can be expressed as a change inratio of one compound to another.
Salivary contaminationEicosanoids and other inflammatory mediatorsare present in saliva [Zakrzewski et al. 1987;McKinney et al. 2000] which could affect EBC
http://tar.sagepub.com 13

Therapeutic Advances in Respiratory Disease
measurements as reported in one study [Gaberet al. 2006]. However, amylase concentrationsin EBC samples are generally undetectable,even with very sensitive assays [Effros et al.2002]. In the small number of EBC samples inwhich amylase concentrations were detectable,they were less than 0.01% of those in salivaindicating trivial salivary contamination [Effroset al. 2002]. Given that leukotriene concentra-tions in saliva are only seven-fold higher thanthose in EBC [Montuschi et al., unpublisheddata] possible salivary contamination is unlikelyto have any relevant effect on measurement ofleukotrienes in EBC. Concentrations of adeno-sine and thromboxane (Tx) B2 in EBC samplesthrough tracheostomy in mechanically ventilatedpatients or through the mouth in healthy sub-jects were similar [Vass et al. 2003]. However,most of the ammonia in the EBC is derivedfrom the mouth, probably as ammonium gas,as indicated by undetectable concentrations ofammonia in EBC samples from patients withtracheostomies [Effros et al. 2002]. These dataindicate that the effect of salivary contaminationon the concentrations of biomolecules in EBClikely depend on their salivary concentrationsand their physicochemical properties (volatile vsnonvolatile compounds). For this reason, theissue of potential salivary contamination of theEBC samples should be considered separately foreach marker.
Validation of analytical methodsPart of the variability of biomarker concen-trations in EBC could be due to analyticalmethods. In most studies published so far, con-centrations of biomolecules in EBC were mea-sured with commercially available immunoassaykits which have not been generally validatedwith reference analytical techniques. Enzymeimmunoassays generally work well in buffer,but their behavior in EBC is not known.Matrix effects due to differences in the com-position of EBC and immunoassy buffer couldbe relevant and might suggest the need forsample pre-treatment. Validation of immunoas-says with reference analytical techniques (e.g.HPLC or MS) is essential for demonstratingthe presence of several biomarkers in EBCand for their accurate quantitative assessment.We have provided evidence for the specificityof 8-isoprostane and PGE2 measurements inEBC by radioimmunoassays (RIAs) developedin our laboratory [Montuschi et al. 2003b] andfor a commercially available assay for LTB4
[Montuschi et al. 2003b]. In these studies, RIAsfor 8-isoprostane and PGE2 and EIA for LTB4
were qualitatively validated by reverse phase-HPLC [Montuschi et al. 2003c; 2003b]. Vali-dation of immunoassays with independent assaymethods is a pre-requisite for large-scale useof immunoassays in EBC analysis. As referenceanalytical techniques are time-consuming, veryexpensive and unsuitable routinely, validation ofimmunoassays might contribute to the develop-ment of EBC analysis in respiratory medicine.
Measurement of markers in EBC for assessingthe response to pharmacological therapyAt present, most of the studies on the effectof anti-inflammatory drugs on markers in EBCare cross-sectional. Few single-center, generallyuncontrolled, interventional studies are available.Large randomized controlled trials using a robustand standardized methodology are required toestablished the effect of drugs on inflamma-tory mediators in EBC in patients with airwayinflammatory diseases.
IsoprostanesF2-Isoprostanes, a group of 64 compounds iso-meric in structure to PGF2α, are currentlyconsidered among the most reliable biomark-ers of oxidative stress and lipid peroxidation[Montuschi et al. 2004b; Montuschi et al. 2007)Concentrations of 8-isoprostane, the most knowncompound belonging to F2-isoprostanes, in EBCare increased in adults with stable asthma, reflect-ing the severity of the disease and the degree ofinflammation [Montuschi et al. 1999]. Despitetreatment with oral or high doses of inhaled glu-cocorticoids, patients with severe asthma havethe highest concentrations of 8-isoprostane inEBC indicating that this eicosanoid is relativelyresistant to inhaled glucocorticoids [Montuschiet al. 1999]. Other authors reported a simi-lar increase in 8-isoprostane in EBC in patientswith stable moderate asthma who were eithersteroid-naive or treated with inhaled glucocorti-coids, although subgroup analysis for the effectsof these drugs was not presented [Kostikas et al.2002]. In contrast to patient with aspirin-tolerantasthma, patients with aspirin-sensitive asthmawho were steroid-naive had higher 8-isoprostaneconcentrations in EBC compared with thosewho were treated with inhaled glucocorticoids[Antczak et al. 2001] indicating that the effectof glucocorticoids on 8-isoprostane might dependon asthma phenotype and/or degree of inflam-mation. In analogy to adults with asthma,
14 http://tar.sagepub.com

Review
8-isoprostane concentrations in EBC were ele-vated in children with asthma who were eithersteroid-naive or treated with inhaled glucocorti-coids compared with those in healthy children[Mondino et al. 2004; Baraldi et al. 2003a;Shahid et al. 2005]. There was no differencein 8-isoprostane levels in EBC between the twostudy groups [Mondino et al. 2004; Baraldi et al.2003a; Shahid et al. 2005]. In healthy subjects,pretreatment with a high dose of inhaled budes-onide (1600 µg/day for 14 days) has no effect onthe increase in 8-isoprostane in EBC induced by2 h exposure to ozone at 400 ppb [Montuschiet al. 2002]. Two open-label studies have shownthat inhaled fluticasone at a dose of 100 µg twicedaily for 4 weeks [Mondino et al. 2004] and oralmontelukast, a LT receptor antagonist, at a doseof 5 mg once a day for 4 weeks have no effecton 8-isoprostane concentrations in EBC in atopicchildren with asthma [Montuschi et al. 2006].
One study reports that oral glucocorticoidsreduce 8-isoprostane concentrations in EBC inpatients with acute asthma [Baraldi et al. 2003b].Compared with healthy children, 8-isoprostaneconcentrations in EBC were elevated in chil-dren with acute asthma [Baraldi et al. 2003b].In these children, oral prednisolone at a dose of1 mg/kg/day for 5 days reduced, but not nor-malized, exhaled 8-isoprostane concentrations[Baraldi et al. 2003b] However, it should benoted that 8-isoprostane concentrations reportedin this study were close to the detection limit ofthe enzyme immunoassay where data are muchless reliable.
Patients with COPD have elevated 8-isoprostaneconcentrations in EBC [Montuschi et al. 2000;Kostikas et al. 2003]. In contrast to healthy sub-jects in whom smoking increases 8-isoprostaneconcentrations in EBC, smoking habit doesnot seem to affect 8-isoprostane levels in EBCin patients with COPD [Montuschi et al.2000]. A 41% reduction of mean 8-isoprostaneconcentrations in EBC has been reportedin patients with COPD exacerbations afterantibiotic treatment [Biernacki et al. 2003].Ibuprofen, a nonselective cyclo-oxygenase (COX)inhibitor, and rofecoxib, a COX-2 selectiveinhibitor, have no effect on 8-isoprostane con-centrations in EBC in patients with COPD[Montuschi et al. 2005b]. The lack of effect ofibuprofen and rofecoxib on exhaled 8-isoprostaneconcentrations indicates that this compound isprimarily formed independently of the COX
pathway [Montuschi et al. 2004b; Montuschiet al. 2007; Morrow et al. 1990].
In patients with obstructive sleep apnea, areduction in exhaled 8-isoprostane concentra-tions after continuous positive airway pressuretherapy has been reported [Carpagnano et al.2003]. However, these data need to be inter-preted cautiously due to the small size effect(−1.9 pg/mL) and the reported 8-isoprostaneconcentrations which were close to detectionlimit of the immunoassay.
LeukotrienesElevated cysteinyl-LT and LTB4 concentrationsin EBC have been reported in both adults andchildren with asthma [Montuschi and Barnes,2002b; Montuschi et al. 2006; Antxzak et al.2001; Mondino et al. 2004; Hanazawa et al.2000; Zanzonato et al. 2004; Carraro et al. 2005;Shibata et al. 2006; Cap et al. 2004; Csomaet al. 2002]. In one study, no difference in cys-LT concentrations in EBC was observed betweensteroid-naive and steroid-treated patients withaspirin-tolerant asthma, whereas steroid treat-ment was associated with lower concentrationsof cysteinyl-LTs in patients with aspirin-sensitiveasthma [Antczak et al. 2001].These findings indi-cate that cysteinyl-LTs concentrations in EBCin patients with aspirin-tolerant asthma are rel-atively resistant to glucocorticoids, although theobservational study design precludes definitiveconclusions. In children with asthma, inhaled flu-ticasone at a dose of 100 µg twice daily for4 weeks has a pronounced effect in reducingexhaled NO concentrations (−53%) over base-line values, but a limited effect on LTE4 con-centrations in EBC (−18%) [Mondino et al.2004]. In contrast, oral montelukast at a doseof 5 mg once daily for 4 weeks seems to havea higher effect on LTE4 concentrations (−33%)in atopic children with asthma than inhaled glu-cocorticoids, but a lower effect on exhaled NOconcentrations (−27%) [Montuschi et al. 2006].Although these studies were open-label, uncon-tolled, and performed in a limited number ofchildren with asthma, they point out the pos-sibility of using the analysis of EBC as a non-invasive tool for assessing the effects of drugsfor asthma. Although several studies reporteddetectable LT concentrations in EBC in patientswith asthma [Montuschi and Barnes, 2002b;Montuschi et al. 2005b, 2006; Antxzak et al.2001; Mondino et al. 2004; Hanazawa et al.2000; Zanzonato et al. 2004; Carraro et al. 2005;
http://tar.sagepub.com 15

Therapeutic Advances in Respiratory Disease
Shibata et al. 2006; Cap et al. 2004; Csoma et al.2002] and other airway inflammatory diseases,some authors were unable to detect cysteinyl-LT concentrations in EBC in adults with asthma[Sandrini et al. 2003]. Due to the lack of a stan-dardized EBC technique, comparisons of resultsfrom different laboratories are currently difficult.In contrast to a limited effect of inhaled glu-cocorticoids on LT concentrations in patientswith stable mild intermittent asthma, a reductionof 60% of median exhaled cysteinyl-LT con-centrations in children with asthma exacerba-tions after oral glucocorticoids has been reported[Baraldi et al. 2003b]. This discrepancy mightbe partly explained by the different route ofadministration (inhaled vs oral) and/or the dif-ferent disease severity (stable vs exacerbatedasthma).
LTB4, but not LTE4, concentrations in EBCare elevated in patients with COPD [Montuschiet al. 2003d; Kostikas et al. 2005]. Steroid-naïve and steroid-treated patients with stableCOPD have similar LTB4 concentrations inEBC [Montuschi et al. 2003d]. In patients withCOPD exacerbations, LTB4 concentrations inEBC were decreased 2 weeks after treatmentwith antibiotics and this effect was maintainedafter 2 months [Biernacki et al. 2003]. LTB4
concentrations in EBC are also increased inpatients with cystic fibrosis exacerbations andare reduced after 2 weeks of antibiotic treatment[Carpagnano et al. 2003b].
ProstanoidsPGE2 concentrations in EBC are elevated insteroid-naive and steroid-treated patients withstable COPD and correlate with LTB4 concen-trations in EBC indicating that the greater thelung inflammation, the higher the production ofPGE2 which may have anti-inflammatory effectsin the airways [Montuschi et al. 2003d]. PGE2
concentrations in EBC in steroid-naive andsteroid-treated patients with COPD were similar[Montuschi et al. 2003d]. Nonselective inhibitionof COX by ibuprofen reduces PGE2 concentra-tions in EBC in patients with COPD, whereasrofecoxib, a selective COX-2 inhibitor, has noeffect [Montuschi et al. 2005b] with potentialimplications for the modulation of airway inflam-mation in COPD. There was no difference inPGE2 concentrations in EBC between patientswith asthma and healthy subjects [Mondino et al.2004; Baraldi et al. 2003] and between patientswith asthma who were either steroid-naïve or
treated with inhaled glucocorticoids [Mondinoet al. 2004; Baraldi et al. 2003a].
TxB2, the stable hydrolysis product of TxA2,a potent bronchoconstrictor, was detected insome patients with asthma who were steroid-naïve [Montuschi and Barnes, 2002b], whereas itwas not detected in either patients with COPD orhealthy subjects [Montuschi et al. 2003d]. Otherauthors reported detectable TxB2 concentrationsin EBC in most of the healthy subjects [Huszaret al. 2005].
PGD2 and PGF2α, which are bronchocon-strictors, were detected in some patients withasthma and healthy subjects [Montuschi andBarnes, 2002b]. In those subjects, in whom theseeicosanoids were detectable there was no dif-ference in their concentrations between the twogroups [Montuschi and Barnes, 2004b].
pHMeasurement of pH is very reproducible andmight prove clinically useful for the diagno-sis and monitoring of pharmacological therapyin inflammatory airway diseases [Hunt, 2002;Vaughan et al. 2003].
pH of deaerated EBC is over two log orderslower in adults with acute asthma than inhealthy subjects and normalizes with glucocor-ticoid therapy [Hunt et al. 2000]. pH values inEBC in children with acute asthma are lowerthan those in children with stable asthma andnormalize with inhaled glucocorticoid therapy[Brunetti et al. 2006]. Treatment with lansopra-zol, a protein pump inhibitor, for two monthsincreases pH values in EBC in patients withmoderate asthma and gastroesophageal refluxdisease, but not in asthmatic patients withoutgastroesophageal reflux disease [Shimizu et al.2007]. Mean pH values are lower in patientswith COPD than in patients with asthma andhealthy subjects [Kostikas et al. 2002]. One studyreported no difference in EBC pH between chil-dren with and without parentally reported symp-toms suggestive of asthma and no consistentassociation between EBC pH and lung function,AHR, and airway inflammation [Nicolau et al.2006]. In patients with COPD, pH values inEBC are negatively correlated with sputum neu-trophils and hydrogen peroxide concentrationsin EBC [Kostikas et al. 2002]. In one study,there were no differences in pH values betweenpatients with COPD who were steroid-naïve and
16 http://tar.sagepub.com

Review
those who were treated with inhaled glucocor-ticoids [Kosikas et al. 2002]. EBC pH can becontinuously monitored in mechanically venti-lated patients and pH values normalize withrecovery [Walsh et al. 2006]. pH values in EBCare lower in patients with allograft rejectionafter lung transplantation compared with thosewithout rejection or healthy subjects [Dupontet al. 2006].
pH values in EBC are unaffected by salivaryor therapeutic artifact, and identical to sam-ples taken directly from the lower airway [Huntet al. 2002]. However, one study has shown thatEBC pH values in samples obtained by RTubeare lower than those in samples obtained byEcoScreen condenser and that the storage for8 weeks had a significant influence on the pHof samples analyzed without deaeration [Prietoet al. 2007]. An extensive normal data revealsmedian EBC pH value is 8.0 with interquar-tile (25–75%) range of 7.8–8.1 [Paget-Brownet al. 2006]. There were no differences basedon age, sex, or race and the distribution wasskewed, with 6.4% of EBC samples having a pHrange <7.4 (Paget-Brown et al.2006). However,some methodological aspects including the effectof ambient CO2, need for sample deaeration,and optimal time for measurement need to beaddressed.
One study has shown that condensate CO2
partial pressure influences pH measurements[Kullmann et al. 2006]. Determination of pH ata standard CO2 level provides the most repro-ducible condensate pH values to date [Kullmannet al. 2006]. Large controlled studies are requiredto establish the effect of inhaled glucocorticoidson pH in EBC in patients with inflammatoryairway diseases including asthma and COPD.
Hydrogen peroxideHydrogen peroxide is detected in EBC but islikely to be less stable than other markers ofoxidant stress such as isoprostanes. Comparedwith healthy nonsmokers, exhaled hydrogen per-oxide is increased in adults and children withasthma [Horvath et al. 1998; Jobsis et al. 1997;Antczak et al. 1997; Emelyanov et al. 2001]and in patients with COPD [Dekhuijzen et al.1996; Nowak et al. 1999; De Benedetto et al.2001], bronchiectasis [Loukides et al. 1998]and ARDS [Kietzmann et al. 1993]. Hydro-gen peroxide concentrations in EBC are furtherelevated in patients with COPD exacerbations
[Dekhuijzen et al. 1996] and in children withacute asthma [Dohlman et al. 1993], but notin adults with unstable asthma [Horvath et al.1998]. Treatment with montelukast at a doseof 10 mg once daily for 2 weeks does notaffect the levels of hydrogen peroxide in EBC inpatients with mild asthma [Sandrini et al. 2003].However, one study reported that nasal trian-cinolone acetonide reduced hydrogen peroxideconcentrations in EBC in patients with allergicrhinitis with and without asthma, supporting theone airway disease hypothesis [Sandrini et al.2003b].
The effect of inhaled glucocorticoids on hydro-gen peroxide concentrations in EBC in patientswith COPD has not been established [Ferreiraet al. 2001; van Beurden et al. 2003a]. Onedouble-blind crossover placebo-controlled studyperformed in 20 stable nonsmoking patients withCOPD showed that beclomethasone at a dose of500 µg twice daily for 2 weeks had no effecton hydrogen peroxide concentrations in EBC[Ferreira et al. 2001]. In contrast, another studyreported that glucocorticoids with more periph-eral deposition (HFA-beclomethasone dipropi-onate at a dose of 400 µg twice daily for 4 weeks)and with more central deposition (fluticasonedipropionate at a dose of 375 µg twice dailyfor 4 weeks) reduced hydrogen peroxide con-centrations in EBC in patients with stable mod-erate COPD [van Beurden et al. 2003a]. In25 patients with COPD who were admitted tohospital because of exacerbations due to lowerrespiratory tract infections, exhaled hydrogenperoxide concentrations were not reduced dur-ing treatment with intravenous dexamethasone,inhaled salbutamol/ipratropium and antibioticsas needed [Kasielski et al. 2001]. In a double-blind, double-dummy, placebo controlled, par-allel group study in 44 patients with stableCOPD, treatment with oral N-acetyl-cysteine,which can have antioxidant effects, at a dose of600 mg a day for 12 months reduced hydro-gen peroxide concentrations in EBC startingfrom 9 months [van Beurden et al. 2003b].Despite this evidence of reduced oxidant stress, amulticenter randomized placebo controlled trialhas shown that N-acetyl-cysteine is ineffectiveat prevention of deterioration in lung func-tion and prevention of exacerbations in patientswith COPD [Decramer et al. 2005]. Moreover,hydrogen peroxide concentrations in EBC inpatients with COPD are transiently increased30 min after nebulization of N-acetyl-cysteine
http://tar.sagepub.com 17

Therapeutic Advances in Respiratory Disease
[Rysz et al. 2007]. In children with cystic fibro-sis exacerbations, antibiotic treatment reduceshydrogen peroxide concentrations in EBC [Ryszet al. 2007].
Elevated levels of hydrogen peroxide in EBC arereduced, but not normalized, after two monthsof antibiotic treatment in patients with activetuberculosis [Kwiatkowska et al. 2007].
The clinical significance of these findings iscurrently unknown. More controlled studies toestablish the effects of pharmacological therapyon exhaled hydrogen peroxide in patients withCOPD are required. As with other biomolecules,a reliable methodology for EBC analysis isrequired for planning and interpreting theresults of interventional studies.
Nitrogen reactive speciesHigh levels of nitrite/nitrate have been found inEBC of adults [Ganas et al. 2001] and chil-dren with asthma [Ratnawati et al. 2006]. Inone study, nitrite/nitrate concentrations in EBCwere lower in adults with asthma who weretreated with inhaled glucocorticoids comparedwith those in steroid-naïve adults with asthma[Ganas et al. 2001]. Increase in nitrite con-centrations in EBC is more pronounced dur-ing asthma exacerbations [Hunt et al. 1995]and severe asthma [Corradi et al. 2001]. In adouble blind, parallel group, placebo controlled,randomised trial, inhaled budesonide at a doseof 100 µg or 400 µg once daily for 3 weekscaused a rapid decrease in nitrite/nitrate concen-trations in EBC which was not dose-dependent[Kharitonov et al. 2002]. Nitrite/nitrate concen-trations returned to baseline values one weekafter treatment withdrawal [Kharitonov et al.2002].
A significant reduction in exhaled S-nitrosothiols,which are derived from interaction of NO orreactive nitrogen species with thiol groups, com-pared with pretreatment levels was only seen atthe end of weeks 1 and 3 of treatment withhigh dose budesonide [Kharitonov et al. 2002].However, whereas reduction in nitrite/nitrateconcentrations in EBC is likely to contribute tothe anti-inflammatory effects of glucocorticoidsin the airways, the reduction in S-nitrosothiolsmight have a different biological significance asS-nitrosothiols have bronchodilator effects andreduced concentrations of these compounds inthe airways has been causally linked to acute
respiratory failure in children [Gaston et al.1998].
Some studies reported elevated levels of3-nitrotyrosine in EBC in both adults [Hanazawaet al. 2000] and children with asthma [Baraldiet al. 2006] and in patients with cystic fibrosis[Balint et al. 2001]. In a single-blind placebo-controlled study, inhaled flunisolide at a dose of800 µg a day for 8 weeks reduced 3-nitrotyrosineconcentrations in EBC in children with mild-to-moderate asthma [Bodini et al. 2006]. However,a study in which 3-nitrotyrosine was measuredwith both GC/MS and HPLC showed that free3-nitrotyrosine in EBC fails as a marker foroxidative stress in children with stable cysticfibrosis and asthma [Celio et al. 2006] althoughlarger study groups are required to draw defini-tive conclusions.
Other markersUsing immunoassay kits, cytokines includinginterleukin (IL)-1β, [Scheideler et al. 1993; Sacket al. 2006] tumor necrosis factor-α (TNF-α)[Scheideler et al. 1993; Sack et al. 2006;Rozy et al. 2006; Matsunaga et al. 2006], IL-4[Shahid et al. 2002; Matsunaga et al. 2006;Robroeks et al. 2006], IL-5 [Profiat et al. 2006],IL-6 [Sandrini et al. 2003; Sack et al. 2006;Rozy et al. 2006], IL-8 [Cunningham et al. 2000;Sack et al. 2006; Matsunage et al. 2006], IL-10[Sack et al. 2006; Robroeks et al. 2006], IL-12p70[Sacks et al. 2006] insulin-like growth factor-1[Rozy et al. 2006], interferon-γ , [Shahid et al.2002; Robroeks et al. 2006] plasminogen activa-tor inhibitor-1 [Rozy et al. 2006] were detectedin EBC in patients with different lung diseases.
However, concentrations of cytokines are gener-ally close to the detection limit of the immuno-assay [Bucchioni et al. 2003; Cunningham et al.2000; Shahid et al. 2002; Carpagnano et al.2003b; Robroeks et al. 2006]. At these concen-trations the analytical variability is high and thereliability of data is questionable. As with otherimmunoassays matrix effects due to differences incomposition between assay buffer and EBC mayplay a role.
Using a chemiluminescence-based membraneprotein array, expression of IL-4, IL-8, IL-17,TNF-α, RANTES, interferon-γ -inducible pro-tein 10, transforming growth factor-β, andmacrophage inflammatory protein 1α and 1β
in EBC were found elevated in steroid-naïve
18 http://tar.sagepub.com

Review
patients with asthma [Matsunage et al. 2006].However, using flow cytometry, IL-2, IL-4,interferon-γ , and IL-10 were detected only in 16,16, 11, and 9%, respectively, of all samples inpatients with asthma and cystic fibrosis at EBCconcentrations which were close to the detectionlimit of the assay [Robroeks et al. 2006]. Using amultiplex fluorescent bead immunoassay (cyto-metric bead array), IL-1β, IL-6, IL-8, IL-10,TNF-α, and IL-12p70 have been found elevatedin EBC patients with acute lung injury com-pared with healthy subjects [Sack et al. 2006].However, cytokines concentrations in EBC werein the order of few pg/ml. Protein array systemsare convenient for analyzing several biomoleculesat the same time, but the development of moresensitive assays and the identification of cytokinesin EBC with reference analytical techniquesstill stand.
Keratin concentrations have been detected inEBC [Jackson et al. 2007; Gianazza et al. 2003]and found elevated in healthy smokers [Gianazzaet al. 2003].
Some authors reported that DNA can bedetected in EBC [Gessner et al. 2004;Carpagnano et al. 2005] whereas other authorsfailed to detect Psedomonas aeruginosa andB. Cepacia by PCR in the EBC of patients withcystic fibrosis [Vogelberg et al. 2003]. Whethergene expression analysis in EBC will have diag-nostic relevance is not known.
ConclusionsMeasurement of biomolecules in EBC mightprovide insights into the pathophysiology of lungdiseases. Selective profiles of inflammatory medi-ators in EBC might have a differential diagnosticvalue in respiratory medicine. As it is com-pletely noninvasive, analysis of EBC is potentiallyuseful for assessing lung inflammation, monitor-ing pharmacological therapy, testing new drugsfor lung diseases, and clarifying the mecha-nism(s) of action of the existing drugs, provid-ing a more rational pharmacological basis fortheir administration. However, EBC analysis iscurrently limited to research purposes, due to thelack of standardization and methodological lim-itations that make it difficult to compate datafrom different laboratories. Future research inthis area should include: the identification ofreference values for the different inflammatorymarkers; large longitudinal studies to ascertain ifsequential EBC analysis in the individual patient
reflects the degree of inflammation and/or dis-ease severity; studies of the relationships betweenEBC markers and symptoms, pulmonary func-tion, and other indices of airway inflammation(e.g. exhaled NO and eosinophil counts in spu-tum); the accurate quantitative assessment ofbiomolecules and the identification of profilesof biomolecules in EBC in different lung dis-eases; large prospective controlled interventionalstudies to establish the usefuleness of EBC anal-ysis for monitoring pharmacological therapy inlung diseases, as the available studies are mainlycross-sectional; studies to establish the useful-ness of EBC analysis for predicting therapeuticresponse and assessment of new drugs; identifi-cation of other biomolecules in EBC; studies toestablish the feasibility and significance of geneexpression analysis in EBC; studies on drug dis-position (e.g. antibiotics); studies on formation ofEBC, its origin in the respiratory system and itsrelationships with airway lining fluid.
Whether and when EBC analysis will be applica-ble in the clinical setting cannot be anticipated.Due to the important pathophysiological role ofinflammation in lung diseases such as asthmaand COPD, the relative lack of noninvasive tech-niques for monitoring airway inflammation andtherapy, and the importance of its potential appli-cations, further research on EBC analysis iswarranted.
AcknowledgmentsSupported by Catholic University of the SacredHeart, Fondi di Ateneo 2005–2007.
Conflict of interest statementThe authors declare that there is no conflict ofinterest.
ReferencesAdelroth, E. (1998) How to measure airwayinflammation: bronchoalveolar lavage and airwaybiopsies. Can Respir J 5: 18A–21A.
Anonymous (1999) Recommendations forstandardised procedures for the on-line andoff-line measurement of exhaled lower respiratorynitric oxide and nasal nitric oxide in adults andchildren – 1999. Official statement of the AmericanThoracic Society 1999. Am J Respir Crit Care Med160: 2104–2117.
Anonymous (2005). ATS/ERS recommendations forstandardized procedures for the online and offlinemeasurement of exhaled lower respiratory nitric oxideand nasal nitric oxide. Am J Respir Crit Care Med171: 912–930.
http://tar.sagepub.com 19

Therapeutic Advances in Respiratory Disease
Antczak, A. et al. (1997) Increased hydrogen peroxideand thiobarbituric acid-reactive products in expiredbreath condensate of asthmatic patients. Eur Respir J10: 1235–1241.
Antczak, A. et al. (2001) Increased exhaledcysteinyl-leukotrienes and 8-isoprostane inaspirin-induced asthma. Am J Respir Crit CareMed 166: 301–306.
Balint, B. et al. (2001) Increased nitrotyrosinein exhaled breath condensate in cystic fibrosis.Eur Respir J 17: 1201–1207.
Baraldi, E. et al. (2003a) Cysteinyl leukotrienesand 8-isoprostane in exhaled breath condensate ofchildren with asthma exacerbations. Thorax 58:505–509.
Baraldi, E. et al. (2003b) Increased exhaled8-isoprostane in childhood asthma. Chest 124:25–31.
Baraldi, E. et al. (2006) 3-Nitrotyrosine, a marker ofnitrosative stress, is increased in breath condensate ofallergic asthmatic children. Allergy 61: 90–96.
Barnes, P.J. (2000) Chronic obstructive pulmonarydisease. N Engl J Med 343: 269–280.
Berlyne, G.S. et al.(2000) A comparison of exhalednitric oxide and induced sputum as markers ofairway inflammation. J Allergy Clin Immunol 106:638–644.
Biernacki, W.A. et al. (2003) Increased leukotriene B4and 8-isoprostane in exhaled breath condensateof patients with exacerbations of COPD. Thorax 58:294–298.
Bodini, A. et al. (2006) Flunisolide decreases exhalednitric oxide and nitrotyrosine levels in asthmaticchildren. Mediators Inflamm 4: 31919.
Brunetti, L. et al. (2006) Exhaled breath condensatepH measurement in children with asthma, allergicrhinitis and atopic dermatitis. Pediatr Allergy Immunol17: 422–427.
Cap, P. et al. (2004) Gas-chromatography massspectrometry analysis of exhaled leukotrienes inasthmatic patients. Thorax 59: 465–470.
Carpagnano, G.E. et al. (2003a) 8-Isoprostane,a marker of oxidative stress, is increased in exhaledbreath condensate of patients with obstructive sleepapnea after night and is reduced by continuouspositive airway pressure therapy. Chest 124:1386–1392.
Carpagnano, G.E. et al. (2003b) Increasedleukotriene B4 and interleukin-6 in exhaled breathcondensate in cystic fibrosis. Am J Respir Crit CareMed 167: 1109–1112.
Carpagnano, G.E. et al. (2005) 3p microsatellitealterations in exhaled breath condensate from patientswith non-small cell lung cancer. Am J Respir Crit CareMed 172: 738–744.
Carpenter, C.T. et al. (1998) Exhaled breathcondensate isoprostanes are elevated in patients withacute lung injury and ARDS. Chest 114: 1653–1659.
Carraro, S. et al. (2005) Exhaled breath condensatecysteinyl leukotrienes are increased in children withexercise-induced bronchoconstriction. J Allergy ClinImmunol 115: 764–770.
Celio, S. et al. (2006) Free 3-nitrotyrosine in exhaledbreath condensates of children fails as a marker foroxidative stress in stable cystic fibrosis and asthma.Nitric Oxide 15: 226–232.
Cepelak, I. et al. (2007) Exhaled breath condensate:a new method for lung disease diagnosis. Clin ChemLab Med (in press).
Corradi, M. et al. (2001) Increased nitrosothiols inexhaled breath condensate in inflammatory airwaydiseases. Am J Respir Crit Care Med 163: 854–858.
Corradi, M. et al. (2003a) Aldehydes and glutathionein exhaled breath condensate of children with asthmaexacerbations. Am J Respir Crit Care Med 167:395–399.
Corradi, M. et al. (2003b) Aldehydes in exhaledbreath condensate of patients with chronicobstructive pulmonary disease. Am J RespirCrit Care Med 167: 1380–1386.
Csoma, Z. et al. (2002) Increased leukotrienes inexhaled breath condensate in childhood asthma.Am J Respir Crit Care Med 166: 1345–1349.
Cunningham, S. et al. (2000) Measurement ofinflammatory markers in the breath condensate ofchildren with asthma. Eur Respir J 15: 955–957.
De Benedetto, F. et al. (2001) Validation of a newtechnique to assess exhaled hydrogen peroxide:results from normals and COPD patients. MonaldiArch Chest Dis 55: 185–188.
Decramer, M. et al. (2005) Effects ofN-acetylcysteine on outcomes in chronic obstructivepulmonary disease (Bronchitis Randomized on NACCost-Utility Study, BRONCUS): a randomisedplacebo-controlled trial. Lancet 365: 1552–1560.
Dekhuijzen, R.P.N. et al. (1996) Increased exhalationof hydrogen peroxide in patients with stable andunstable chronic obstructive pulmonary disease.Am J Respir Crit Care Med 154: 813–816.
Dohlman, A.W. et al. (1993) Expired breath hydrogenperoxide is a marker of acute airway inflammation inpediatric patients with asthma. Am Rev Resp Dis 148:955–960.
Dupont, L.J. et al. (2006) The pH of exhaled breathcondensate of patients with allograft rejection afterlung transplantation. Am J Transplant 6: 1486–1492.
Dwyer, T.M. (2001) Expired breath condensate(EBC) and the ultimate disposition of airway surfaceliquid (ASL). Am J Respir Crit Care Med 163: A406.
Effros, R.M. et al. (2002) Dilution of respiratorysolutes in exhaled condensates. Am J Respir Crit CareMed 165: 663–669.
Effros, R.M. et al. (2003) A simple method forestimating respiratory solute dilution in exhaledbreath condensates. Am J Respir Crit Care Med 168:1500–1505.
20 http://tar.sagepub.com

Review
Effros, R.M. et al. (2005a) Utility of exhaled breathcondensates in chronic obstructive pulmonary disease:a critical review. Curr Opin Pulm Med 11: 135–139.
Effros, R.M. et al. (2005b) Exhaled breathcondensate: formation and physicochemicalproperties. In Montuschi P (ed), New perspectivesin monitoring lung inflammation: analysis of exhaledbreath condensate. CRC Press: Boca Raton, Florida,pp. 31–52.
Emelyanov, A. et al. (2001) Elevated concentrationsof exhaled hydrogen peroxide in asthmatic patients.Chest 120: 1136–1139.
Ferreira, I.M. et al. (2001) Exhaled nitric oxideand hydrogen peroxide in patients with chronicobstructive pulmonary disease: effects of inhaledbeclomethasone. Am J Respir Crit Care Med 164:1012–1015.
Fixman, E.D. et al. (2007) Basic mechanisms ofdevelopment of airway structural changes in asthma.Eur Respir J 29: 379–389.
Gaber, F. et al. (2006) Saliva is one likely source ofleukotriene B4 in exhaled breath condensate. EurRespir J 28: 1229–1235.
Gajdocsi, R. et al. (2003) The reproducibility andaccuracy of the on-line hydrogen peroxide bioassayand the decreasing effect of storage on H2O2concentration. Eur Respir J 22, Suppl. 45: 279s.
Ganas, K. et al. (2001) Total nitrite/nitrate in expiredbreath condensate of patients with asthma. RespirMed 95: 649–654.
Gaston, B. et al. (1998) Bronchodilator S-nitrosothioldeficiency in asthmatic respiratory failure. Lancet351: 1317–1319.
Gessner, C. et al. (2004) Detection of p53 genemutations in exhaled breath condensate ofnon-small cell lung cancer patients. Lung Cancer43: 215–222.
Gianazza, E. et al. (2003) Increased keratin contentdetected by proteomic analysis of exhaled breathcondensate from healthy persons who smoke.Am J Med 117: 51–54.
Goen, T. et al. (2005) Sensitive and accurate analysesof free 3-nitrotyrosine in exhaled breath condensateby LC-MS/MS. Chromatogr B Analyt Technol BiomedLife Sci 826: 261–266.
Hanazawa, T. et al. (2000) Increased nitrotyrosine inexhaled breath condensate of patients with asthma.Am J Respir Crit Care Med 162: 1273–1276.
Horvath, I. et al. (1998) Combined use of exhaledhydrogen peroxide and nitric oxide in monitoringasthma. Am J Respir Crit Care Med 158: 1042–1046.
Horvath, I. et al. (2005) Exhaled breath condensate:methodological recommendations and unresolvedquestions. Eur Respir J 26: 523–548.
Hunt, J. (2002) Exhaled breath condensate: anevolving tool for non-invasive evaluation of lungdisease. J Allergy Clin Immunol 110: 28–34.
Hunt, J. et al. (1995) Condensed expirate nitriteas a home marker for acute asthma. Lancet 346:1235–1236.
Hunt, J.F. et al. (2000) Endogenous airwayacidification. Implications for asthmapathophysiology. Am J Respir Crit Care Med161: 694–699.
Huszar, E. et al. (2005) Comparative measurementof thromboxane A2 metabolites in exhaled breathcondensate by different immunoassays. Inflamm Res54: 350–355.
Jackson, A.S. et al. (2007) Comparison of biomarkersin exhaled breath condensate and bronchoalveolarlavage. Am J Respir Crit Care Med 175: 222–227.
Jobsis, Q. et al. (2000) Hydrogen peroxide and nitricoxide in exhaled air of children with cystic fibrosisduring antibiotic treatment. Eur Respir J 16: 95–100.
Jobsis, Q. et al. (1997) Hydrogen peroxide in exhaledair is increased in stable asthmatic children. EurRespir J 10: 519–521.
Kasielski, M. and Nowak, D. (2001) Long-termadministration of N-acetylcysteine decreaseshydrogen peroxide exhalation in subjects with chronicobstructive pulmonary disease. Respir Med 95:448–456.
Kharitonov, S.A. and Barnes, P.J. (2006) Exhaledbiomarkers. Chest 130: 1541–1546.
Kharitonov, S.A. and Barnes, P.J. (2001) Exhaledmarkers of pulmonary disease. Am J Respir CritCare Med 163: 1693–1722.
Kharitonov, S.A. et al. (2002) Dose-dependent onsetand cessation of action of inhaled budesonide onexhaled nitric oxide and symptoms in mild asthma.Thorax 57: 889–896.
Kietzmann, D. et al. (1993) Hydrogen peroxide inexpired breath condensate of patients with acuterespiratory failure and with ARDS. Intensive CareMed 19: 78–81.
Kostikas, K. et al. (2002) pH in expired breathcondensate of patients with inflammatory airwaydiseases. Am J Respir Crit Care Med 165: 1364–1370.
Kostikas, K. et al. (2003) Oxidative stress in expiredbreath condensate of patients with COPD. Chest 124:1373–1380.
Kostikas, K. et al. (2005) Leukotriene B4 in exhaledbreath condensate and sputum supernatant inpatients with COPD and asthma. Chest 127:1553–1559.
Kullmann, T. et al. (2006) Exhaled breath condensatepH standardised for CO2 partial pressure. Eur RespirJ 29: 496–501.
Kwiatkowska, S. et al. (2007) Elevated exhalation ofhydrogen peroxide and circulating IL-18 in patientswith pulmonary tuberculosis. Respir Med 101:574–580.
Larstad, M. et al. (2002) Determination ofmalondialdehyde in breath condensate by
http://tar.sagepub.com 21

Therapeutic Advances in Respiratory Disease
high-performance liquid chromatography withfluorescence detection. J Chromatogr B AnalytTechnol Biomed Life Sci 766: 107–114.
Larstad, M. et al. (2003) Influence of sampling timeon malondialdehyde levels and pH in exhaled breathcondensate. Eur Respir J, Suppl 45: 38s.
Larstad, M. et al. (2005) Selective quantification offree 3-nitrotyrosine in exhaled breath condensate inasthma using gas chromatography/tandem massspectrometry. Nitric Oxide 13: 134–144.
Loukides, S. et al. (1998) Elevated levels of expiredbreath hydrogen peroxide in bronchiectasis. Am JRespir Crit Care Med 158: 991–994.
Matsunaga, K. et al. (2006) Airway cytokineexpression measured by means of protein array inexhaled breath condensate: correlation withphysiologic properties in asthmatic patients.J Allergy Clin Immunol 118: 84–90.
McCafferty, J.B. et al. (2004) Effects of breathingpattern and inspired air conditions on breathcondensate volume, pH, nitrite, and proteinconcentrations. Thorax 59: 694–698.
McKinney, E.T. et al. (2000) Plasma, urinary,and salivary 8-epi-prostaglandin F2α levels innormotensive and preeclamptic pregnancies.Am J Obstet Gynecol 183: 874–877.
Mondino, C. et al. (2004) Effects of inhaledcorticosteroids on exhaled leukotrienes andprostanoids in asthmatic children. J Allergy ClinImmunol 114: 761–767.
Montuschi, P. (2002) Indirect monitoring of lunginflammation. Nat Rev Drug Discov 1: 238–242.
Montuschi, P. (editor) (2005a) New perspectives inmonitoring lung inflammation: analysis of exhaledbreath condensate. CRC Press: Boca Raton,Florida.
Montuschi, P. et al. (2005b) Analysis of exhaledbreath condensate: methodological issues. InMontuschi P (ed), New perspectives in monitoringlung inflammation: analysis of exhaled breathcondensate. CRC Press: Boca Raton, Florida,pp. 11–30.
Montuschi, P. and Barnes, P.J. (2002a) Analysis ofexhaled breath condensate for monitoring airwayinflammation. Trends Pharmacol Sci 23: 232–237.
Montuschi, P. and Barnes, P.J. (2002b) Exhaledleukotrienes and prostaglandins in asthma. J AllergyClin Immunol 109: 615–620.
Montuschi, P. et al. (1999) Increased 8-isoprostane,a biomarker of oxidative stress, in exhaled condensateof asthma patients. Am J Respir Crit Care Med 160:216–220.
Montuschi, P. et al. (2000) Exhaled 8-isoprostane asan in vivo biomarker of oxidative stress in patientswith COPD and healthy smokers. Am J Respir CritCare Med 162: 1175–1177.
Montuschi, P. et al. (2002) Ozone-induced increasein exhaled 8-isoprostane in healthy subjects is
resistant to inhaled budesonide. Free Radic Biol Med33: 1403–1408.
Montuschi, P. et al. (2003a) Methodological aspectsof exhaled prostanoid measurements. Eur Respir J,Suppl. 45: 18s.
Montuschi, P. et al. (2003b) Validation of8-isoprostane and prostaglandin E2 measurements inexhaled breath condensate. Inflamm Res 52: 502–507.
Montuschi, P. et al. (2003c) Validation of leukotrieneB4 measurements in exhaled breath condensate.Inflamm Res 52: 69–73.
Montuschi, P. et al. (2003d) Exhaled leukotrienes andprostaglandins in COPD. Thorax 58: 585–588. Chest127: 1553–1559.
Montuschi, P. et al. (2004a) Ion trap liquidchromatography/tandem mass spectrometry analysisof leukotriene B4 in exhaled breath condensate. RapidCommun Mass Spectrom 18: 2723–2729.
Montuschi, P. et al. (2004b) Isoprostanes: markersand mediators of oxidative stress. FASEB J 18:1791–1800.
Montuschi, P. et al. (2005a) Liquidchromatography/mass spectrometry analysis ofexhaled leukotriene B4 in asthmatic children.Respir Res 19: 6 :119.
Montuschi, P. et al. (2005b) Effects ofcyclo-oxygenase inhibition on exhaled eicosanoidsin patients with COPD. Thorax 60: 827–833.
Montuschi, P. et al. (2006) Effects of a leukotrienereceptor antagonist on exhaled leukotriene E4 andprostanoids in children with asthma. J Allergy ClinImmunol 118: 347–353.
Montuschi, P. et al. (2007) Insights into oxidativestress: the isoprostanes. Curr Med Chem 14: 703–717.
Morrow, J.D. et al. (1990) A series of prostaglandinF2-like compounds are produced in vivo in humansby a non-cyclooxygenase, free radical-catalyzedmechanism. Proc Natl Acad Sci USA 87:9383–9387.
Mutlu, G.M. et al. (2001) Collection and analysis ofexhaled breath condensate in humans. Am J RespirCrit Care Med 164: 731–737.
Nicolau, N.C. et al. (2006) Exhaled breathcondensate pH and childhood asthma: unselectedbirth cohort study. Am J Respir Crit Care Med 174:254–259.
Nowak, D. et al. (1999) Increased content ofthiobarbituric acid-reactive substances and hydrogenperoxide in the expired breath condensate of patientswith stable chronic obstructive pulmonary disease:no significant effect of cigarette smoking. Respir Med93: 389–396.
O’Donnell, R. et al. (2006) Inflammatory cells in theairways in COPD. Thorax 61: 448–454.
Paget-Brown, A.O. et al. (2006) Normative data forpH of exhaled breath condensate. Chest 129:426–430.
22 http://tar.sagepub.com

Review
Prieto, L. et al. (2007) Differences in exhaled breathcondensate pH measurements between samplesobtained with two commercial devices. Respir Med(in press).
Profita, M. et al. (2006) Noninvasive methods for thedetection of upper and lower airway inflammationin atopic children. J Allergy Clin Immunol 118:1068–1074.
Ratnawati, R. et al. (2006) Exhaled breath condensatenitrite/nitrate and pH in relation to pediatric asthmacontrol and exhaled nitric oxide. Pediatr Pulmonol 41:929–936.
Rickmann, J. et al. (2001) Breath condensate reflectsdifferent compartments of respiratory tract dependingon ventilation pattern. Am J Respir Crit Care Med163: A407.
Robroeks, C.M. et al. (2006) Cytokines in exhaledbreath condensate of children with asthma and cysticfibrosis. Ann Allergy Asthma Immunol 96: 349–355.
Rosias, P.P.R. et al. (2006) Breath condenser coatingsaffect measurement of biomarkers in exhaled breathcondensate. Eur Respir J 28: 1036–1041.
Rozy, A. et al. (2006) Inflammatory markers inthe exhaled breath condensate of patients withpulmonary sarcoidosis. J Physiol Pharmacol57 (Suppl 4): 335–340.
Rysz, J. et al. (2007) Increased hydrogen peroxideconcentration in the exhaled breath condensateof stable COPD patients after nebulizedN-acetylcysteine. Pulm Pharmacol Ther 20:281–289.
Sabroe, I. et al. (2007) Targeting the networks thatunderpin contiguous immunity in asthma andchronic obstructive pulmonary disease. Am J RespirCrit Care Med 175: 306–311.
Sack, U. et al. (2006) Multiplex analysis of cytokinesin exhaled breath condensate. Cytometry A 69:169–172.
Sandrini, A. et al. (2003a) Effect of montelukast onexhaled nitric oxide and nonvolatile markers ofinflammation in mild asthma. Chest 124:1334–1340.
Sandrini, A. et al. (2003b) Effect of nasaltriamcinolone acetonide on lower airwayinflammatory markers in patients with allergicrhinitis. J Allergy Clin Immunol 111: 313–320.
Scheideler, L. et al. (1993) Detection of nonvolatilemacromolecules in breath: a possible diagnostic tool?Am Rev Respir Dis 148: 778–784.
Schleiss, M.B. et al. (2000) The concentration ofhydrogen peroxidein exhaled air depends onexpiratory floe rate. Eur Respir J 16: 1115–1118.
Shahid, S.K. et al. (2002) Increased interleukin-4 anddecreased interferon-gamma in exhaled breath
condensate of children with asthma. Am J Respir Crit
Visit SAGE journals onlinehttp://online.sagepub.com
Care Med 165: 1290–1293.
Shahid, S.K. et al. (2005) Exhaled 8-isoprostane inchildhood asthma. Respir Res 6: 79.
Shibata, A. et al. (2006) Increased leukotriene E4 inthe exhaled breath condensate of children with mildasthma. Chest 130: 1718–1722.
Shimizu,Y. et al. (2007) Proton pump inhibitorimproves breath marker in moderate asthma withgastroesophageal reflux disease. Respiration (in press).
Smith, A.D. et al. (2005) Use of exhaled nitric oxidemeasurements to guide treatment in chronic asthma.N Engl J Med 352: 2163–2173.
Soyer, O.U. et al. (2006) Comparison of two methodsfor exhaled breath condensate collection. Allergy 61:1016–1018.
Svensson, S. et al. (2003) Sampling time is importantfor the collection of hydrogen peroxide in exhaledbreath condensate (EBC). Eur Respir J, Suppl 45: 78s.
van Beurden, W.J. et al.(2003a) Effects of inhaledcorticosteroids with different lung deposition onexhaled hydrogen peroxide in stable COPD patients.Respiration 70: 242–248.
van Beurden, W.J. et al. (2003b) Markers ofinflammation and oxidative stress during lowerrespiratory tract infections in COPD patients.Monaldi Arch Chest Dis 59: 273–280.
Vass, G. et al. (2003) Comparison of nasal andoral inhalation during exhaled breath condensatecollection. Am J Respir Crit Care Med 167: 850–855.
Vaughan, J. et al. (2003) Exhaled breath condensatepH is a robust and reproducible assay of airwayacidity. Eur Respir J 22: 889–894.
Vogelberg, C. et al. (2003) Pseudomonas aeruginosaand Burkholderia cepacia cannot be detected by PCRin the breath condensate of patients with cysticfibrosis. Pediatr Pulmonol 36: 348–352.
Walsh, B.K. et al. (2006) Exhaled-breath condensatepH can be safely and continuously monitored inmechanically ventilated patients. Respir Care 51:1125–1131.
Wenzel, S.E. (2006) Asthma: defining of thepersistent adult phenotypes. Lancet 368: 804–813.
Zakrzewski, J.T. et al. (1987) Lipid mediators incystic fibrosis and chronic obstructive pulmonarydisease. Am Rev Respir Dis 136: 779–782.
Zanconato, S. et al. (2004) Leukotrienes and8-isoprostane in exhaled breath condensate ofchildren with stable and unstable asthma. J AllergyClin Immunol 113: 257–263.
Zappacosta, B. et al. (2001) A fast chemiluminescentmethod for H(2)O(2) measurement in exhaled breathcondensate. Clin Chim Acta 310: 187–191.
http://tar.sagepub.com 23