Nurses and Mass Casualty Incident Triage: efficacy and appreciation of nationwide simulation program

R E S E A R C H
Elisabetta PExcellenced’Annunzio”
Daniele AntLecce, Italy.
Antonio CoLecce, Italy.
Giancarlo CFaculty of M
For correspExcellenced’Annunzio”E-mail: e.pa
J Emerg Nu
0099-1767/
Copyright ©All rights re
http://dx.do
■ ■ • ■
ANALYSIS OF EMERGENCY MEDICAL SERVICESTRIAGE AND DISPATCH ERRORS BY
REGISTERED NURSES IN ITALY
Authors: Elisabetta Palma, PhD, MSN, RN, Daniele Antonaci, MSN, RN, Antonio Colì, MSN, RN,and Giancarlo Cicolini, PhD, MSN, RN, Chieti and Lecce, Italy
Introduction: The major elements of an effective emergencymedical services (EMS) system include a single telephoneaccess number, accurate assessment of the urgency of thehealth problem, and timely dispatch of appropriate personneland equipment. In Italy, EMS calls are managed by emergencyoperations centers by registered nurses who have receivedspecialized education in this function. The nurses determine thecriticality of the situations and assign an EMS response prioritylevel identified by a color code, ranging from red (very critical) togreen (not critical). At times, the severity of a situation may beunderestimated, resulting in assignment of a lower EMSresponse priority and the potential for patient death (codeblack). The purpose of this study was to analyze factorsassociated with registered nurse under-triage of EMS callssubsequently found to be associated with deaths, termed“green-black code” cases.
Methods: We carried out a retrospective qualitative analysisof EMS telephone conversations using Fele’s conversationanalysis method. The characteristics of green-black code calls
alma is Lecturer, Department of Nursing Sciences, Center ofon Aging, Clinical Research Center, University of “G.Foundation, Chieti, Italy.
onaci is Chief Nurse, Province of Lecce Emergency Department,
lì is Chief Nurse, Province of Lecce Emergency Department,
icolini is Nurse Director, Second Level Degree Nursing Sciences,edicine, University of Chieti–Pescara, Chieti, Italy.
ondence, write: Elisabetta Palma, PhD, MSN, RN, Center ofon Aging, Clinical Research Center, University of “G.Foundation, Via dei Vestini 31, I-66013 Chieti, Scalo, Italy;
rs ■.
$36.00
2014 Emergency Nurses Association. Published by Elsevier Inc.served.
i.org/10.1016/j.jen.2014.02.009
Master Proof ym
were compared with the characteristics of the population of allEMS calls during the study period.
Results: The study patients were older, with a mean age of 81.6years. The callers were individuals calling on behalf of thepatients, rather than the patients themselves. The callers reportedsymptoms that were not life-threatening. Nurse operators did notalways inquire about the patients’ vital signs as required by theMedical Priority Dispatch System protocol. The phone conversa-tions were shorter than normal (54.26 seconds vs 65 seconds).
Discussion: Although the importance of dispatch systemprotocols is well known, it is also important that nurse triageoperators have proper training to ensure that major parameterssuch as vital signs and symptomatology are obtained and toreduce caller stress level.
Key words: Ambulances/utilization; Emergency medicalservices organization and administration; Health priorities;Quality of health care; Triage
Efforts to improve health care outcomes whilefostering cost containment through appropriateuse of resources have resulted in a proliferation in
the provision of telephone assessment and consultationservices by registered nurses (RNs) in a variety of settings.Handling a telephone call that may involve a request foremergency care requires substantial expertise. The operatoris expected to quickly recognize the severity of the medicalcondition, identify the possible etiology, and determine theresources required while reducing the caller’s anxiety oraggressiveness to obtain the caller’s collaboration.1 Theoperator should use time efficiently, collecting only thenecessary information without prolonging the phone call.Operators require proficiency in effective communicationskills to collect all the relevant data. The subsequentdecision-making process should lead to the best response—the right emergency care mobile resource and the right staffat the right time.
WWW.JENONLINE.ORG 1
en2560.pdf

TABLE 1Correspondence between color and numeric codes
Color code Numeric code Description
White 0 The situation is not an emergency and an ambulance is not needed. The patient is safeor does not have a relevant pathology. The patient’s condition is not life threatening.
Green 1 The situation is not an emergency; the patient has an acute but stable pathology.The patient’s vital signs are normal.
Yellow 2 The situation is a medical emergency. Intervention cannot be delayed; the patient’svital signs are stable at the moment but should be strictly monitored to preventpossible worsening.
Red 3 The situation is an absolute emergency. The patient’s vital signs have deteriorated orindicate an immediate threat to the patient’s life. The vital signs must be stabilizedand supported during the intervention and transportation.
Black 4 The patient is dead.
RESEARCH/Palma et al
In Italy, RNs are responsible for both the triage ofpatients arriving at the emergency department and thetelephone emergencymedical services (EMS) dispatch system.Italian law specifies at least 6 months’ seniority in emergencynursing to perform medical triage. In addition, emergencyoperations center (EOC) RN operators are emergency nurseswith at least 2 years’ seniority in the emergency departmentand expertise in prehospital care.
At the time of the study, Italy did not have a codifiedsystem to standardize the collection and analysis ofprehospital data, although processes were in place forselected conditions, such as trauma and cardiac arrest.2,3 Arecent survey by the Italian Ministry of Health showed thatEOC operators use a dual-mode (color and alphanumeric)code system to classify both the criticality and the severity ofan emergency call4 (Table 1). The code assigned to theprevailing pathology is the second most importantinformation for emergency dispatchers. When a patienthas comorbidities, the operator assigns a code that refers tothe most relevant symptoms (Table 2). Finally, the locationcode indicates where the event took place (Table 2).
Determining Appropriate Response Resources
Emergency dispatching is a dynamic decision-makingprocess,5 as well as the most important activity performedby EOCs. It consists of 4 phases: taking incoming calls,instructing callers, dispatching the appropriate EMS resources,and instructing the ambulance crew. Appropriate conversationtechniques enable the operator to obtain collaboration fromthe caller. In addition, the use of a standardized interview
2 JOURNAL OF EMERGENCY NURSING
Master Proof ym
protocol allows for the collection of all relevant details whileavoiding conflicts with the caller.6,7
Collaboration depends on 3 caller variables: emotionalstatus, knowledge of the situation, and general behaviorwhen reporting an emergency. Theoretically, the emotion-al status of the caller does not really affect collaborationbecause a well-trained operator can guide a scared or angrycaller using specific interrogation techniques, as well as acalm voice. An Italian study confirmed that only 4% ofcallers were annoyed or irritated.8 The caller may be thepatient himself or herself (first-party caller), a person in thepatient’s direct vicinity (second-party caller), or a personwho is not with the patient but is reporting from somedistance (third-party caller). About 55% of EMS phonecalls in Italy are made by first- or second-party callers9
who, if correctly interviewed, may provide all the relevantinformation. That is why the use of a standardizedinterview protocol, together with appropriate training onhow to lead a succinct telephone conversation, is soimportant. When an emergency occurs, the caller has adistorted time perception. For this reason, it is importantthat an emergency medical call be answered by at least thethird ring, although such a response time—about 12seconds—would still prove rather lengthy for an emer-gency call.10 In the case of life-threatening situations,such as cardiac arrest, electrocution, drowning, andsuffocation,11 the telephone conversation should last lessthan 1 minute. The mobilization time (from call end toEMS vehicle dispatch) generally varies from 75 to 90seconds. This time interval is considered part of thestandard ambulance response time set by the law in Italy,
■ ■ • ■
en2560.pdf

TABLE 2Dispatch codes
Prevalent pathology Location
C01: trauma S: street (public or private)C02: cardiocirculatory P: public place
(business location, office)C03: respiratory Y: sport facilityC04: neurologic K: homeC05: psychiatric L: workplaceC06: neoplastic Q: schoolC07: toxicologic Z: other locationC08: metabolicC09: gastroenterologicC10: urologicC11: ophthalmologicC12: otorhinolaryngologicC13: dermatologicC14: obstetric-gynecologicC15: infectiveC19: other pathologyC20: unidentified pathology
Palma et al/RESEARCH
which is 8 minutes for urban areas and for life-threateningemergencies and 20 minutes for rural areas.
Characteristics of Effective Telephone Encounter
What are the main features of satisfactory communicationwhen taking an emergency medical call? Although researchhas increased in recent years, literature concerning thequalitative aspects of telephone dispatching is still ratherpoor. Several studies appear to lack methodologic rigor,12
with the 5-level priority system used in France, Canada, theUnited States, the United Kingdom, and Australia beingmore consensus based than evidence based.13
Several studies have focused on the efficacy of a singletelephone number for all the emergency services, such as 911in the United States or 112, introduced in the Europeancommunity in 2001. With the exception of the province ofVarese (Northern Italy), where a single emergency telephonenumber has been available since 2010, Italy has a differentemergency number for each of the various emergency services(fire, medical, and police emergency).
Data from Italy show that EOC operators are able toscreen about half of all calls, which ensures that emergencyservices (police, fire department, EMS) are activated only
■ ■ • ■
Master Proof ym
when needed.14 One Italian study showed that EOCoperators tend to overestimate the criticality and severitycodes as compared with the assessment performed by theemergency medical team on the scene.15 Several sceneresponder–identified green codes appeared to be over-estimated as yellow, whereas red codes were not alwaysproperly identified.
With regard to telephone conversation contentanalysis, qualitative research is oriented toward definingthe local organizational structure1 whereas sociolinguisticresearch is more oriented toward analyzing telephoneconversations between people serving a formal organiza-tion/institution.16 A study analyzing “special conversa-tions” showed that intervention in emergency situationsconsists of 5 steps: dispatchers take the incoming call andidentify themselves, the caller asks for help, a briefconversation takes place, the caller’s request is respondedto, and the process is completed.17
Review of Literature
A systematic review of the literature concerning telephonetriage performed by EMS system operators identified 326studies.18 The overall quality of these studies was modest,with only a few studies seeming to consistently support theuse of specific criteria to identify medical priorities toimprove patient outcomes. Sometimes calls are notappropriate, for example, patients who do not meet thespecific criteria for an immediate ambulance response. Itappears that the accuracy of emergency response proceduresimproves when operators assign a priority code using theMedical Priority Dispatch System (MPDS) protocol.Statistically, an assessment using the MPDS protocol ismore concordant with the criticality code assigned by theon-scene emergency medical team.18,19 The use of theMPDS protocol also seems to reduce emergency medicaltechnicians’ response time in the most critical cases.20–22
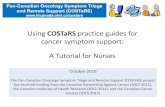
Despite the use of standard protocols, EMS dispatchassessment errors (under-triage) still occur, especially incomplex situations involving patients with multiple orchronic diseases. Underestimating an emergency situationmay be significant, such as when an emergency medicalteam, arriving on the scene of what they were told was agreen code (not particularly critical), finds that the patienthas died in the meantime. Such occurrences, dubbed“green-black code” cases by Italian emergency healthworkers, are considered sentinel events (Figure). Thisstudy aims to detect, through a retrospective qualitativeanalysis of telephone conversations, the factors associatedwith under-triage.
WWW.JENONLINE.ORG 3
en2560.pdf

0
5
10
15
20
25
30
35
2005 2006 2007 2008 2009 2010 2011
green-black codes
IGURE
entinel events (ie, green-black code cases) for the years 2005 through 2011.
RESEARCH/Palma et al
F
S
Methods
The characteristics of 2 different call groups were analyzed.We carried out a retrospective study of a sample of 839EMS calls that occurred during 2011 at the EOC of Lecce,Italy. Permission to access the database was obtained fromthe General Administrative Management of the EOC. Thesample was randomly extracted by use of a table of randomnumbers from a population of 62,392 EMS calls (α b 5%,99% confidence interval [CI]). We compared the charac-teristics of the sample telephone conversations with thecharacteristics of the 15 green-black calls occurring in 2011.The phone calls were analyzed with the aim of collectinginformation on conversational features.
The following variables were considered: details of theevent, telephone conversation, EMS care resources, andpatient data. Specific data were analyzed for each section.
The section on details of the event comprised the timeinterval from call receipt until the appropriate mobile careresourcewas physically en route to the emergency, the dispatcher,the final criticality/priority assessment, and other data.
With regard to the telephone conversation section, thecriticality code assigned while the caller is interrogated is theproduct of a decision-making process that can be based ondispatcher experience or on application of the MPDSprotocol. This code is communicated to the ambulancecrew immediately after the call. Conversations wereanalyzed using the qualitative and phenomenologicaltechniques implemented by Fele23 in his conceptualmodel. Fele is an Italian sociologist who has conductedseveral investigations in the field of the emergency services(police, fire department, EMS). His “conversational analysismethod” is specifically applied to study institution-centeredinteractions, such as those occurring in EOCs.
The section on EMS care resources comprisedinformation regarding the type of resource dispatched, as
4 JOURNAL OF EMERGENCY NURSING
Master Proof ym
well as vehicle response time. In Italy, volunteer-staffedvehicles provide basic life support (BLS) and earlydefibrillation whereas vehicles staffed with a physician andRN provide advanced life support (ALS).
The patient data section permitted analysis of theconcordance between the emergency code initially assignedby the dispatchers and the medical team’s assessment ontheir arrival on scene.
Using Fele’s model, we analyzed the 15 green-blacktelephone conversations, focusing on 4 crucial aspects:incoming call receipt (operators identify the service),problem description (operators collect all relevant datafrom the caller), problem identification (operators assign acriticality code), and call ending (operators reassure thecaller and revise the information collected from the caller).
STATISTICAL ANALYSIS
Data were exported to a Microsoft Access database (version10.00; Microsoft, Redmond, WA) and analyzed by use ofSPSS software for Windows, version 17.0 (SPSS, Chicago,IL). We performed a factorial analysis considering all thevariables of a dispatch. In addition, the qualitative variablesof the green-black code were examined.
Results
The EOC is equipped with an Ericsson MD-110 PBXsystem (Ericsson Enterprise, Stockholm, Sweden) thatroutes emergency calls to operators (there are generally 6dispatchers per shift). During 2011, operators received62,392 emergency calls, from which we randomly extracteda sample of 839 calls. The number of incoming emergencycalls per operator while dispatchers were already handlingphone calls varied from 2 to 47 (mean, 23.41; SD, 11.12).Although the proficiency of operators when creating adispatch depends on several variables, a regression analysisshowed that the variable “operator” was not strictly relatedto the whole green-black code phenomenon. Linearregression analysis (R2 test) showed that the variable“operator” accounted for only 14% of the entire process.
DISPATCH CREATION TIME
The overall time to generate a dispatch was calculated by useof a linear model. The mean time was about 65 seconds(99% CI, 61-69 seconds). The mean duration of telephoneconversations was about the same in both the sample (range,43.8-64.8 seconds) and the green-black code subgroup(range, 61.5-69.4 seconds). The mean time necessary tosend the appropriate mobile care resource and complete the
■ ■ • ■
en2560.pdf

TABLE 3Data comparison between sample and green-black code subgroup
Sample Green-black code subgroup
Patient age (y) 61.8 (99% CI, 57-67) 81.6 (95% CI, 77-86)Dispatch creation time (s) 65.47 (99% CI, 61.4-69.4) 54.26 (95% CI, 44.7-65.7)Ambulance response time (min)Urban areas 11.5 (99% CI, 5.2-17.8) 17.7 (95% CI, 6.2-29.2)Rural areas 19.4 (99% CI, 4.9-33.9) 17.9 (95% CI, 9.6-26.1)
Palma et al/RESEARCH
dispatch was 95 seconds (99% CI, 84-106 seconds). Phonecalls generally lasted less than 120 seconds (82.5%) and, insome cases, less than 60 seconds (43.3%).
COMPLETENESS OF DATA COLLECTION
Operators failed to record all the details required forcomputer-assisted dispatching for 85.7% of the calls. Thismissing information could enable a better post hoc analysis.Some data seemed to be less neglected than others, as in thecase of cardiovascular patients, for whom additionalinformation was almost always present.
EVENT LOCATION
Most phone calls were about medical emergencies occurringat home (76.9%) or in the street (14.1%) (Table 2).
PREVAILING PATHOLOGY
Cardiovascular pathologies were most common (29.9%),followed by trauma-induced musculoskeletal problems(21.9%), and respiratory diseases (13.8%). No prevailingpathology was present in 17% of the cases (Table 2).
CRITICALITY SCORE ASSIGNED BY OPERATOR
In the observed sample, the color codes assigned were asfollows: red in 6.9%, yellow in 56%, green in 36.8%, andwhite (ie, not urgent at all) in 0.3%.
CONCORDANCE IN CRITICALITY SCORE
The EOC operators and scene responders agreed in only31.6% of patients with a green code and in 26.7% ofpatients with a yellow code.
GREEN-BLACK CODE CASES
During 2011, 15 of 62,392 dispatches (1:4,000)classified as nonurgent (green) by the EOC operators
■ ■ • ■
Master Proof ym
were associated with a patient death (black code).The analyses performed in the general populationwere repeated for this particular subgroup; however,the CI was set at 95% because the subgroup wassmaller (Table 3).
In addition, telephone conversations were analyzedto evaluate the quality of communication and theoccurrence of incorrect assessments during calls. Theresponse time in the green-black code subgroup wassignificantly shorter (54.26 seconds; 95% CI, 44-65seconds) when compared with the sample. Most phonecalls lasted less than 60 seconds (66%). In those under-triaged cases (green code), operators had not documentedall the major items of the MPDS protocol (conscious-ness, breathing, circulation) on the dispatch form and aBLS-staffed ambulance (volunteer crew) was sent insteadof an ALS-staffed ambulance.
When volunteers with BLS training assessed thecriticality of the situation, they called the EOC for medicalsupport so that a second ambulance with a nurse and aphysician was sent. The first ambulance arrived within8 minutes (standard time for urban areas) in 25% of cases.Because of the nonurgent emergency code, the meanresponse time of the first ambulance was about 17 minutes(95% CI, 6-29 minutes). The mean response time for ruralareas was 18 minutes (95% CI, 9-26 minutes), indicatingthat the 20-minute standard response time for rural areaswas generally accomplished (86%). When compared withthe mean age of all the patients treated (61.8 years), thepatients in the green-black code subgroup were significantlyolder (mean age, 81.6 years; 95% CI, 77-86 years), asshown in Table 3.
QUALITATIVE ASSESSMENT OF TELEPHONECONVERSATIONS
As proposed by the Fele method, we divided conversationsinto 4 parts: incoming call receipt, problem description,problem identification, and call ending.
WWW.JENONLINE.ORG 5
en2560.pdf

TABLE 4Quality assessment of telephone conversations
Item Points
Opening (service identification)Yes 1No 0
Problem explanationNot accurate 0Quite accurate 1Accurate 2
Problem identification (awareness and breathing)Neither question 0Only 1 question 1Both questions 2
Closure (reassurance)Yes 1No 0
RESEARCH/Palma et al
Incoming Call Receipt
When taking an incoming call, operators should immedi-ately identify the service as well as themselves by saying“Emergency Operations Center 118, I am a nurse.”Operators generally did identify the service (86.7%).
Problem Description
When taking emergency calls, operators ask for detailsaccording to a set of standard questions. They may gothrough the whole list of questions (accurate interrogation),ask only a few questions (inaccurate interrogation), or justlisten (simple listening). The interview was accurate in 4cases (26.7%), the interview was inaccurate in 8 cases(53.3%), and operators simply listened in 3 cases (20%).
Problem Identification
To quickly obtain vital information about patient status andscene conditions, the operator should act according to theMPDS protocol, asking the caller whether the patient isalert and breathing. Operators asked both questions (alertand breathing) in 1 case (6.7%), asked only 1 question (alertor breathing) in 5 cases (33.3%), and did not ask eitherquestion in 9 cases (60%).
Call Ending
At the end of the conversation, operators reassured callers,telling them that an ambulance was on its way, in 13 cases(86.7%). To evaluate the accuracy of telephone conversa-tions, we assigned a score between 0 points (0%) and 6points (100%) to the described variables (Table 4). Themean score of the 15 telephone conversations was 54.4%(95% CI, 43.7%-65.2%).
Discussion
This study focused on the qualitative aspects of EOC RNoperator activity, with the aim of detecting the possiblecauses of underestimation of the severity of healthemergencies subsequently associated with so-called green-black code cases. The 15 calls associated with the green-black code cases were routed to the operators by automaticswitching equipment. This study has several limitations,primarily related to the lack of a common reference modelfor measuring the effectiveness of the dispatch process atEOCs. The few existing studies on this topic referred todifferent organizational settings and were specificallyfocused on indicators such as dispatch accuracy, ambulanceresponse times, and concordance between severity codes
6 JOURNAL OF EMERGENCY NURSING
Master Proof ym
assigned by dispatchers and the actual emergency scenariofound by medical teams on their arrival. Assuming that thegreen-black code cases are sentinel events, we compared the15 deaths with the overall activity of the EOC considered inthis study via a retrospective analysis. The aim was to detectpossible differences in the activity of operators (dispatchappropriateness and effectiveness), the demographic char-acteristics of the patients, or the telephone conversations.Our data refer to a local EOC, which means that the resultscannot be generalized.
The mean length of telephone conversations was 65seconds. The mean dispatch initiation time was 95seconds, with the limit of 120 seconds—a standardaccepted by experts9—generally being respected (82.5%).At times, collecting data from the caller was difficult andtime-consuming, and therefore the delay was not attribut-able to the operators. Although the proficiency level ofoperators when creating a dispatch depends on severalvariables, a regression analysis showed that the variable“operator” was not strictly related to the whole green-blackcode phenomenon.
Because of the small sample size, it is not possible toestablish a relationship between the duration of a dispatchand the criticality code assigned. With regard to thethoroughness of completing the dispatch form, we observedthat items referring to symptoms and events (chest pain,trauma, car accident, sudden illness) were often left blank(85.7%). Symptoms and events more likely to be reportedare “chest pain” (5.6%) and “car accident” (4.7%), perhaps
■ ■ • ■
en2560.pdf

Palma et al/RESEARCH
because such occurrences require implementation of specificprotocols such as acute myocardial infarction and pre-hospital trauma care. Operators generally tend to over-estimate the condition of patients reporting chest pain.20
The vast majority of calls were for medical emergenciesoccurring at home (76.9%), which is consistent withnational statistics. Given their prevalence,21 cardiocircula-tory problems were predominant (29.9%), followed bymusculoskeletal problems (21.9%) and a number of “otherpathologies” (17.4%). The mean duration of telephoneconversations was more or less the same in both the sample(range, 43.8-64.8 seconds) and the green-black codesubgroup (range, 61.5-69.4 seconds). All 15 green-blackcode emergency calls were made by a relative or, in 1 case,by a caregiver. When compared with the sample, the 15patients in the subgroup were older (mean age of 81.6 yearsvs 61.8 years). The presence of chronic conditions and theolder age of the patients may have led callers tounderestimate the severity of the situation. Dispatch wasnot accurate in 11 cases. Operators did not document allelements of the dispatch form when interrogating callers,with vital signs (awareness, breathing) being only partiallyassessed, if not entirely neglected. All of the previously listedfactors could have contributed to under-triage. When weanalyzed the telephone conversations using the Felemethod, it appeared that in all cases callers described avague and generally not alarming situation (dysuria,constipation, leg pain for 3 days). The caller’s descriptionof the problem as nonurgent probably strongly influencedthe operator’s decision on the type of criticality code to beassigned. Our analysis shows that callers had not beeninterrogated accurately enough. Such underestimationsinevitably resulted in dispatch of an ambulance equippedonly with a volunteer-based crew to a “green code” scene(therefore neither emergency lights nor sirens wereactivated). Volunteers, after assessing the emergencyscenario, called the EOC for medical support, so precioustime was wasted waiting for an ALS-staffed ambulance.
Limitations
This article describes the Italian EMS Triage system, whichis performed by nurses. This model could differ from EMSsystems of other Countries.
Implications for Emergency Nurses
Triage is essential for the early recognition and treatment ofseriously ill patients, and it reduces morbidity and mortalityrates. In Italy, telephone triage of EMS calls is performed by
■ ■ • ■
Master Proof ym
experienced nurses with at least 2 years’ seniority in theemergency department. Regular retraining may help theRN operators avoid under-triage by focusing on the MPDSprotocol. It is important that nurses act in accord with theMPDS protocol, asking the caller about the patient’s statusand scene condition, particularly when the caller reportsseemingly non–life-threatening situations, to assign theappropriate EMS response priority level.
Conclusions
Even if green-black code cases are rare (1/4,000interventions), they represent sentinel events indicative ofan EMS system failure. Nurses working at EOCs usuallyassess patients’ conditions and make important decisionswith very limited time (60-120 seconds). The introductionof specific training based on the Fele method could improveboth the quality and effectiveness of telephone triage. Thetraining could involve simulations of EMS calls, as well asthe analysis and discussion of real cases of under-triagedEMS calls.
From a methodologic point of view, the results of thisresearch could be useful in creating a near-miss and adverseevents database. Further research is needed to betterunderstand the green-black code phenomenon and toanalyze the role of communication in the assignation of anunderestimated priority code.
REFERENCES1. Psathas G. Talk and social structure. In: Psathas G, (ed.), Conversation
Analysis: The Study of Talk-in-Interaction. Thousand Oaks, CA: SagePublications; 1995:58-61.
2. Dick WF, Baskett PJ. Recommendations for uniform reporting of datafollowing major trauma—the Utstein style. A report of a working partyof the International Trauma Anesthesia and Critical Care Society(ITACCS). Resuscitation. 1999;42(2):81-100.
3. Cummins RO, Chamberlain DA, Abramson NS. Recommendedguidelines for uniform reporting of data from out-of-hospital cardiacarrest: the Utstein style. A statement for health professionals from a taskforce of the American Heart Association, the European ResuscitationCouncil, the Heart and Stroke Foundation of Canada, and theAustralian Resuscitation Council. Circulation. 1991;20(8):960-75.
4. Ministry of Health. Mattoni-outcome project. Reconnaissance of thelegislation, experiences, trials, relative to emergency and 118 in regionaland national level. NHS Mattone 11-ER-118 System. Avaialble at:http://www.mattoni.salute.gov.it. Published January 21, 2007. AccessedOctober 12, 2013.
5. Leprohon J, Patel VL. Decision-making strategies for telephone triage inemergency medical services. Med Decis Making. 1995;15(3):240-53.
6. DeGroot HA. Patient classification systems and staffing. Part 1,problems and promise. J Nurs Admin. 1994;24(9):43-51.
WWW.JENONLINE.ORG 7
en2560.pdf

RESEARCH/Palma et al
7. Forslund K. Operators experiences of emergency calls. J TelemedTelecare. 2004;10(5):5290-7.
8. Ghiselli G, Calabrò P, Bono D, Enrichens F. I codici giallinell’interpretazioni delle chiamate. Emergency Oggi. 2003;8(9):4-6.
9. Thakore S, McGugan EA, Morrison W. Emergency ambulancedispatch: is there a case for triage? J R Soc Med. 2002;95(3):126-9.
10. Wilde ET. Do emergency medical system response times matter forhealth outcomes? Health Econ. 2013;22(7):790-806.
11. Focarile F. Indicatori di Qualità nell’Assistenza Sanitaria. Turin, Italy:Centro Scientifico Torinese; 1998.
12. Harden RD. Critical appraisal of papers describing 359 triage systems.Acad Emerg Med. 1999;6(11):1166-71.
13. van der Wulp I, van Stel HF. Adjusting weighted kappa for severityof mistriage decreases reported reliability of emergency department triagesystems: a comparative study. J Clin Epidemiol. 2009;62(11):1196-201.
14. Corbetta C. Single emergency number 112: the test of Varese. In: ZoliA, (ed.), I quaderni di AREU. Itacacomunicazione; 2010:21-3.
15. Greggio M, Scapparone P, Costanza R, Leigheb F, Panella M. I codici digravità nell’emergenza sanitaria territoriale: comparazione tra i codiciattribuiti dalla Centrale Operativa 118 dell’ASO di Alessandria e quelliassegnati sul luogo dell’evento. Acts of the XII National Conference ofPublic Health Rome, Italy: Edizioni Iniziative Italiane; 2011:623.Avaialble at: http://www.societaitalianaigiene.org/site/new/image/docs/atticongressi/201110roma.pdf. Accessed April 29, 2013.
8 JOURNAL OF EMERGENCY NURSING
Master Proof ym
16. PeräKylä A, Vehvilainen S. Conversation analysis and the professionalstocks of interactional knowledge. Discourse Soc. 2004;14(6):727-50.
17. Zimmerman H. The interactional organization of calls for emergency. In:Drew P, Heritage J, (eds.), Talk at Work: Interaction in Institutional SettingsCambridge, England: Cambridge University Press; 1992:418-69.
18. Slovis CM, Carruth TB, Seitz WJ, Thomas CM, Elsea WR. A prioritydispatch system for emergency medical services. Ann Emerg Med.2000;14(11):1055-6.
19. Wilson S, Cooke M, Morrell R, Bridge P, Allan TEmergency MedicineResearch Group. A systematic review of the evidence supporting the useof priority dispatch of emergency ambulances. Prehosp Emerg Care.2002;6(1):42-9.
20. Clawson J, Olola CH, Heward A, Scott G, Patterson B. Accuracy ofemergency medical dispatchers’ subjective ability to identify when higherdispatch levels are warranted over a Medical Priority Dispatch Systemautomated protocol’s recommended coding based on paramedicoutcome 385 data. Emerg Med J. 2007;24(8):560-3.
21. Clawson J, Olola C, Heward A, Patterson B, Scott G. The MedicalPriority Dispatch System’s ability to predict cardiac arrest outcomes andhigh acuity pre-hospital alerts in chest pain patients presenting to 9-9-9.Resuscitation. 2008;78(3):298-306.
22. Curka PA, Pepe PE, Ginger VF, Sherrard RC, Ivy MV, Zachariah BS. Apriority dispatch system for emergency medical services. Ann Emerg Serv.1985;22(11):1055-60.
23. FeleG.L’Analisi Della Conversazione.Bologna, Italy: IlMulino; 2007:91-116.
■ ■ • ■
en2560.pdf