Anaesthesia and Intensive Care A-Z | ElsevierAsia
10
A severity characterisation of trauma (ASCOT). Trauma scale derived from the Glasgow coma scale, sys- tolic BP, revised trauma score, abbreviated injury scale and age. A logistic regression equation is used to provide a probability of mortality. Excludes patients with a very poor or very good prognosis. Has been claimed to be superior to the trauma revised injury severity score system although more complex. Champion HR, Copes WS, Sacco WJ, et al (1996). J Trauma; 40: 42–8 A–adO 2 , see Alveolar–arterial oxygen difference ABA, see American Board of Anesthesiology Abbott, Edward Gilbert, see Morton, William Abbreviated injury scale (AIS). Trauma scale first described in 1971 and updated many times since. Comprises a classification of injuries with each given a 6-digit code (the last indicating severity, with 1 ¼ minor and 6 ¼ fatal). The codes are linked to International Classification of Diseases codes, thus aiding standardisation of records. The anatomical profile is a refinement in which the locations of injuries are divided into four categories; the AIS scores are added and the square root taken to minimise the contribution of less severe injuries. Copes WS, Lawnick M, Champion HR, Sacco WJ (1988). J Trauma; 28: 78–86 Abciximab. Monoclonal antibody preparation used as an antiplatelet drug and adjunct to aspirin and heparin in high risk patients undergoing percutaneous transluminal coronary angioplasty. Consists of Fab fragments of immunoglobulin directed against the glycoprotein IIb/IIIa receptor on the platelet surface. Inhibits platelet aggregation and thrombus formation; effects last 24–48 h after infusion. Careful consideration of risks and benefits should precede use since risk of bleeding is increased. Licensed for single use only. l Dosage: 250 mg/min iv 10–60 min (up to 24 h in unstable angina) before angioplasty with 125 mg/kg/min (up to 10 mg/min for 12 h afterwards). l Side effects: bleeding, hypotension, nausea, bradycardia. Thrombocytopenia occurs rarely. Abdominal compartment syndrome. Combination of increased intra-abdominal pressure and organ dysfunction, e.g. following abdominal trauma or extensive surgery, resulting from haemorrhage, leakage of oedema fluid and/or massive intestinal oedema. May also follow liver transplant- ation and acute pancreatitis. Intra-abdominal pressures above 20–25 cmH 2 O may be associated with reduced venous return and cardiac output, impaired ventilation, reduced renal blood flow and oliguria. Increased CVP may lead to raised ICP. Diagnosed clinically and by measuring intra-abdominal pressure via a bladder catheter or nasogastric tube, using a water column manometer. Management includes laparotomy and leaving the abdomen open and/or using silastic material to cover the abdominal contents. Paracentesis may be effective if raised intra-abdom- inal pressure is due to accumulation of fluid, e.g. ascites. Full resuscitation must be performed before decompression as rapid release of pressure may result in sudden washout of inflamma- tory mediators from ischaemic tissues, causing acidosis and hypotension. Malbrain ML, Cheatham ML, Kirkpatrick A, et al (2006). Intensive Care Med; 32: 1722–1732, and Cheatham ML, Malbrain ML, Kirkpatrick A (2007). Intensive Care Med; 33: 951–62 See also, Compartment syndromes Abdominal decompression. Technique in obstetric anal- gesia whereby negative pressure is applied to the abdomen in order to reduce labour pain and possibly shorten labour. Thought to act by making the uterus more spherical during contractions, thus contracting with less force. Now rarely used. See also, Obstetric analgesia and anaesthesia Abdominal field block. Technique using 100–200 ml local anaesthetic agent, involving infiltration of the skin, subcuta- neous tissues, abdominal muscles and fascia. Provides anal- gesia of the abdominal wall and anterior peritoneum, but not of the viscera. Now rarely used. Rectus sheath block, trans- versus abdominis plane block, iliac crest block and inguinal hernia field block are more specific blocks. Abdominal sepsis, see Intra-abdominal sepsis Abdominal trauma. May be blunt (e.g. road traffic acci- dents) or penetrating (e.g. stabbing, bullet wounds). Often carries a high morbidity and mortality because injuries may go undetected. May lead to massive intra-abdominal blood loss or abdominal compartment syndrome. The abdomen can be divided into three areas: w intrathoracic: protected by the bony thoracic cage. Con- tains the spleen, liver, stomach and diaphragm. Injury may be associated with rib fractures. The diaphragm may also be injured by blows to the lower abdomen (which impart pressure waves to the diaphragm) or by penetrating injuries of the chest. w true abdomen: contains the small and large bowel, bladder and, in the female, uterus, fallopian tubes and ovaries. w retroperitoneal: contains the kidneys, ureters, pancreas and duodenum. May result in massive blood loss from retroperitoneal venous injury. l Management: w basic resuscitation as for trauma generally. w initial assessment: examination of the anterior abdom- inal wall, both flanks, back, buttocks, perineum (and in A I
-
Upload
elsevier-health-solutions-apac -
Category
Health & Medicine
-
view
1.377 -
download
0
description
This updated encyclopaedia of anaesthesia and intensive care medicine covers aspects relating to Anesthesia & critical care medicine. With extensive line diagrams & topic descriptions, this is a reference title that every post graduate should own. If you would like to purchase this title, please visit Elsevier Asia Bookshop.
Transcript of Anaesthesia and Intensive Care A-Z | ElsevierAsia

A severity characterisation of trauma (ASCOT).Trauma scale derived from the Glasgow coma scale, sys-tolic BP, revised trauma score, abbreviated injury scaleand age. A logistic regression equation is used to provide aprobability of mortality. Excludes patients with a very poor orvery good prognosis. Has been claimed to be superior to thetrauma revised injury severity score system although morecomplex.Champion HR, Copes WS, SaccoWJ, et al (1996). J Trauma;40: 42–8
A–adO2, see Alveolar–arterial oxygen difference
ABA, see American Board of Anesthesiology
Abbott, Edward Gilbert, see Morton, William
Abbreviated injury scale (AIS). Trauma scale firstdescribed in 1971 and updated many times since. Comprisesa classification of injuries with each given a 6-digit code (thelast indicating severity, with 1 ¼ minor and 6 ¼ fatal). Thecodes are linked to International Classification of Diseasescodes, thus aiding standardisation of records. The anatomicalprofile is a refinement in which the locations of injuries aredivided into four categories; the AIS scores are added and thesquare root taken to minimise the contribution of less severeinjuries.Copes WS, Lawnick M, Champion HR, Sacco WJ (1988).J Trauma; 28: 78–86
Abciximab. Monoclonal antibody preparation used as anantiplatelet drug and adjunct to aspirin and heparin inhigh risk patients undergoing percutaneous transluminalcoronary angioplasty. Consists of Fab fragments ofimmunoglobulin directed against the glycoprotein IIb/IIIareceptor on the platelet surface. Inhibits platelet aggregationand thrombus formation; effects last 24–48 h after infusion.Careful consideration of risks and benefits should precede usesince risk of bleeding is increased. Licensed for single useonly.l Dosage: 250 mg/min iv 10–60 min (up to 24 h in unstable
angina) before angioplasty with 125 mg/kg/min (up to10 mg/min for 12 h afterwards).
l Side effects: bleeding, hypotension, nausea, bradycardia.Thrombocytopenia occurs rarely.
Abdominal compartment syndrome. Combination ofincreased intra-abdominal pressure and organ dysfunction,e.g. following abdominal trauma or extensive surgery,resulting from haemorrhage, leakage of oedema fluid and/ormassive intestinal oedema.May also follow liver transplant-ation and acute pancreatitis. Intra-abdominal pressuresabove 20–25 cmH2O may be associated with reduced venousreturn and cardiac output, impaired ventilation, reduced renalblood flow and oliguria. Increased CVP may lead to raisedICP. Diagnosed clinically and by measuring intra-abdominal
pressure via a bladder catheter or nasogastric tube, using awater column manometer.
Management includes laparotomy and leaving the abdomenopen and/or using silastic material to cover the abdominalcontents. Paracentesismay be effective if raised intra-abdom-inal pressure is due to accumulation of fluid, e.g. ascites. Fullresuscitationmust be performed before decompression as rapidrelease of pressure may result in sudden washout of inflamma-tory mediators from ischaemic tissues, causing acidosis andhypotension.Malbrain ML, Cheatham ML, Kirkpatrick A, et al (2006).Intensive Care Med; 32: 1722–1732, and Cheatham ML,Malbrain ML, Kirkpatrick A (2007). Intensive Care Med;33: 951–62See also, Compartment syndromes
Abdominal decompression. Technique in obstetric anal-gesia whereby negative pressure is applied to the abdomen inorder to reduce labour pain and possibly shorten labour.Thought to act by making the uterus more spherical duringcontractions, thus contracting with less force. Now rarelyused.See also, Obstetric analgesia and anaesthesia
Abdominal field block. Technique using 100–200 ml localanaesthetic agent, involving infiltration of the skin, subcuta-neous tissues, abdominal muscles and fascia. Provides anal-gesia of the abdominal wall and anterior peritoneum, but notof the viscera. Now rarely used. Rectus sheath block, trans-versus abdominis plane block, iliac crest block andinguinal hernia field block are more specific blocks.
Abdominal sepsis, see Intra-abdominal sepsis
Abdominal trauma. May be blunt (e.g. road traffic acci-dents) or penetrating (e.g. stabbing, bullet wounds). Oftencarries a high morbidity and mortality because injuries maygo undetected. May lead to massive intra-abdominal bloodloss or abdominal compartment syndrome. The abdomencan be divided into three areas:
w intrathoracic: protected by the bony thoracic cage. Con-tains the spleen, liver, stomach and diaphragm. Injurymay be associated with rib fractures. The diaphragmmay also be injured by blows to the lower abdomen(which impart pressure waves to the diaphragm) or bypenetrating injuries of the chest.
w true abdomen: contains the small and large bowel,bladder and, in the female, uterus, fallopian tubes andovaries.
w retroperitoneal: contains the kidneys, ureters, pancreasand duodenum. May result in massive blood loss fromretroperitoneal venous injury.
l Management:w basic resuscitation as for trauma generally.w initial assessment: examination of the anterior abdom-inal wall, both flanks, back, buttocks, perineum (and in
A
I

men, the urethral meatus) for bruises, lacerations, entryand exit wounds. Signs may be masked by unconscious-ness, spinal cord injury or the effects of alcohol ordrugs. Abdominal swelling usually indicates intra-abdominal haemorrhage; abdominal guarding or rigidityusually indicates visceral injury. Absence of bowelsounds may indicate intra-peritoneal haemorrhage orperitoneal soiling with bowel contents. Colonic or rectalinjuries may cause blood pr. A high index of suspicion isrequired for retroperitoneal injuries since examination isdifficult.
w imaging: abdominal X-ray may reveal free gas under thediaphragm (erect or semi-erect; may also be visible onchest X-ray) or laterally (lateral decubitus X-ray); otherinvestigations include pelvic X-ray and urological radi-ology if indicated (e.g. iv urogram, etc.), CT and MRIscanning and ultrasound.
w peritoneal lavage is indicated in blunt abdominal traumaassociated with:- altered pain response (head injury, spinal cord injury,drugs, etc.).
- unexplained hypovolaemia following multiple trauma.- equivocal diagnostic findings.
w insertion of a nasogastric tube and urinary catheter (pro-vided no urethral injury; a suprapubic catheter may benecessary).
w indications for laparotomy include penetrating injuries,obvious intra-abdominal haemorrhage, signs of bowelperforation or a positive peritoneal lavage.
See also, Pelvic trauma
ABO blood groups. Discovered in 1900 by Landsteiner inVienna. Antigens may be present on red blood cells, withantibodies in the plasma (Table 1). The antibodies, mostlytype-M immunoglobulins, develop within the first fewmonths of life, presumably in response to naturally occurringantigens of similar structure to the blood antigens. Infusion ofblood containing an ABO antigen into a patient who alreadyhas the corresponding antibody may lead to an adverse reac-tion; hence the description of groupO individuals as universaldonors, and of group AB individuals as universal recipients.[Karl Landsteiner (1868–1943), Austrian-born US patholo-gist]See also, Blood cross-matching; Blood groups; Blood trans-fusion
ABPI, see Ankle Brachial Pressure Index
Abruption, see Antepartum haemorrhage
Absolute risk reduction. Indicator of treatment effect inclinical trials. For a reduction in incidence of events from a%to b%, it equals (a–b)%. Does not give an indication of themagnitude of a or b.See also, Meta-analysis; Number needed to treat; Odds ratio;Relative risk reduction
Abuse of anaesthetic agents. May occur because of easyaccess to potent drugs by operating theatre or ICU staff.Opioid analgesic drugs are the most commonly abusedagents, but others include benzodiazepines and inhalationalanaesthetic agents. Abuse may be suggested by behaviouralor mood changes, or excessive and inappropriate requests foropioids. Main considerations include the safety of patients,counselling and psychiatric therapy for the abuser, and legalaspects of drug abuse. May be associated with alcoholism.Berry CB, Crome IB, Plant M, Plant M (2000). Anaesthesia;55: 946–52See also, Misuse of Drugs Act; Sick doctor scheme; Substanceabuse
Acarbose. Inhibitor of intestinal alpha glucosidases andpancreatic amylase; used in the treatment of diabetes melli-tus, usually in combination with a biguanide or sulfony-lurea. Delays digestion and absorption of starch andsucrose. Has a small blood glucose lowering effect.l Dosage: 50 mg orally once daily, increasing up to 200 mg
8 hourly.l Side effects include flatulence and diarrhoea, and rarely
hepatic dysfunction. Contraindicated in pregnancy andinflammatory bowel disease.
See also, Meglitinides; Thiazolidinediones
Accessory nerve block. Performed for spasm of trapeziusand sternomastoid muscles (there is no sensory component tothe nerve). 5–10 ml local anaesthetic agent is injected 2 cmbelow the mastoid process into the sternomastoid muscle,through which the nerve runs.
Accident, major, see Incident, major
ACD, Acid–citrate–dextrose solution, see Blood storage
ACD-CPR, Active compression decompression CPR,see Cardiac massage; Cardiopulmonary resuscitation
ACE, Angiotensin converting enzyme, see Renin/angioten-sin system
ACEanaestheticmixture. Mixture of alcohol, chloroformand diethyl ether, in a ratio of 1:2:3 parts, suggested in 1860 asan alternative to chloroform alone. Popular into the 1900s as ameans of reducing total dose and side effects of any one of thethree drugs.
ACE inhibitors, see Angiotensin converting enzymeinhibitors
Acetaminophen, see Paracetamol
Acetazolamide. Carbonic anhydrase inhibitor, whichreduces bicarbonate formation and hydrogen ion excretion,thereby creating a metabolic acidosis. Also a weak diuretic,but rarely used as such. Used to treat glaucoma, metabolicalkalosis, altitude sickness and childhood epilepsy. Useful inthe treatment of severe hyperphosphataemia because itleads to urinary excretion of phosphate. May be used tolower ICP by reducing CSF production. Has been used toalkalinise the urine in tumour lysis syndrome or to enhanceexcretion in drug intoxications, e.g. with salicylates.l Dosage: 0.25–0.5 g orally/iv, once/twice daily.
Acetylcholine (ACh). Neurotransmitter, the acetyl esterof the base choline (Fig. 1). Synthesised from acetylcoenzyme
Table 1 Antigens and antibodies in ABO blood groups
Group Incidence in UK (%) Red cell antigen Plasma antibody
A 42 A Anti-B
B 8 B Anti-A
AB 3 A and B None
O 47 None Anti-A and anti-B
2 ABO blood groups

A and choline in nerve ending cytoplasm; the reaction iscatalysed by choline acetyltransferase. Choline is activelytransported into the nerve and acetylcoenzyme A is formed inmitochondria. ACh is stored in vesicles.l ACh is the transmitter at:
w autonomic ganglia.w parasympathetic postganglionic nerve endings.w sympathetic postganglionic nerve endings at sweatglands and some muscle blood vessels.
w the neuromuscular junction.w many parts of the CNS where it has a prominent role inlearning.
Has either muscarinic or nicotinic actions, depending on theacetylcholine receptors involved. ACh is hydrolysed to cho-line and acetate by acetylcholinesterase on the postsynapticmembrane. Other esterases also exist, e.g. plasma cholines-terase.See also, Muscarine and muscarinic receptors; Neuromuscu-lar transmission; Nicotine and nicotinic receptors; Parasym-pathetic nervous system; Sympathetic nervous system;Synaptic transmission
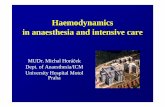
Acetylcholine receptors. Transmembrane proteins acti-vated by acetylcholine (ACh). ACh receptors may be mus-carinic or nicotinic (Fig. 2a). Injected ACh first stimulatesmuscarinic receptors. As the dose is increased, nicotinicreceptors are stimulated; i.e. parasympathetic stimulationand sweating precedes effects at ganglia and the neuromus-cular junction (NMJ).
The structure of the postsynaptic (nicotinic) receptors atthe NMJ has been identified largely through work on theelectric eel. Each receptor consists of five glycosylated pro-tein subunits which project into the synaptic cleft. The sub-units have been designated a (mw 40 000), b (mw 49 000),g (mw 60 000) and d (mw 67 000). The g subunit is thought tobe replaced by an e subunit in mammals. The subunits spanthe postsynaptic membrane and form a cylinder around acentral ion channel (Fig. 2b). The two a subunits of eachreceptor carry the binding sites for ACh. Occupation ofthese sites causes a configurational change of the subunits,thus opening the ion channel; cations (mainly sodium, potas-sium and calcium) flow through the channel according to theirconcentration gradients and thus generate an action potential.Non-depolarising neuromuscular blocking drugs at normaldoses reduce the number of receptors available to ACh. Athigher doses they may also block the ion channel. Muscarinicreceptors are G protein-coupled receptors.
Neuronal forms of ACh receptors are more heterogenouswith a large number of subunit configurations.See also, Muscarine and muscarinic receptors; Neuromuscu-lar transmission; Nicotine and nicotinic receptors; Parasym-pathetic nervous system; Sympathetic nervous system;Synaptic transmission
Acetylcholinesterase. Enzyme present in the basementpostsynaptic membranes of cholinergic synapses andneuromuscular junctions. Also found in red blood cellsand the placenta. Converts acetylcholine (ACh) into acetate
CH3 CH3CH2 CH2
CH3
CH3
N+ O C
O
Fig. 1 Structure of acetylcholine
Somatic muscle
Nicotinic MuscarinicParasympathetic
Sympathetic
Nicotinic
AdrenergicNicotinicMost nerves
MuscarinicNicotinicTo sweat glands
NicotinicTo adrenalmedulla
Lipids
Cytoskeleton
βα
εα
δ
10 nm
(a)
(b)
Fig. 2 (a) Types of acetylcholine receptors. (b) Structure of nicotinic
acetylcholine receptor
Acetylcholine
Anionic site
Choline Acetylatedenzyme
Acetate
Esteratic site
(CH3)3 N CH2 CH2 CH3O
O
C
(CH3)3 N CH2 CH2 OH CH3
O
C
O
HO
HO
CH3
O
C
O
+
+
Fig. 3 Action of acetylcholinesterase
Acetylcholinesterase 3

and choline, thus terminating its action. The N(CH3)3þ part
of ACh binds to the anionic site of the enzyme, and theacetate end of ACh forms an intermediate bond at the esteraticsite. Choline is liberated, and the intermediate substrate/en-zyme complex is then hydrolysed to release acetate (Fig. 3).See also, Acetylcholinesterase inhibitors; Neuromusculartransmission; Synaptic transmission
Acetylcholinesterase inhibitors. Substances whichincrease acetylcholine (ACh) concentrations by inhibitingacetylcholinesterase. Used clinically for their action at theneuromuscular junction in myasthenia gravis and in thereversal of non-depolarising neuromuscular blockade.Concurrent administration of an antimuscarinic agent, e.g.atropine or glycopyrronium, reduces unwanted effects ofincreased ACh concentrations at muscarinic receptors. Ef-fects at ganglia are minimal at normal doses. Central effectsmay occur if the drug readily crosses the blood–brain bar-rier, e.g. physostigmine (used to treat the central anticholi-nergic syndrome).Have also been used to treat tachyarrhythmias.l Classification:
w prosthetic: competitive inhibition at the anionic site ofthe enzyme prevents binding of ACh, e.g. edropho-nium, tetrahydroaminocrine.
w oxydiaphoretic: acts as a substrate for the enzyme; thereaction proceeds as far as the intermediate substrate/enzyme complex. Hydrolysis of the complex and thusreactivation of the enzyme is slow.
Examples:- neostigmine, physostigmine (few hours).- pyridostigmine (several hours).- distigmine (up to a day).
Organophosphorus compounds act as oxydiaphoreticinhibitors, but the substrate/enzyme complex is minimallyhydrolysed; inhibition lasts for weeks until new enzyme issynthesised.
Acetylcholinesterase inhibitors augment depolarisingneuromuscular blockade andmay cause depolarising block-ade in overdose. They may also cause bradycardia, hypoten-sion, agitation, miosis, increased GIT activity, sweating andsalivation.
Centrally acting acetylcholinesterase inhibitors (e.g. done-pezil, rivastigmine, galantamine) are used for symptomatictreatment of Alzheimer’s dementia. Of potential anaestheticrelevance because of their side effects (including nausea,vomiting, fatigue, muscle cramps, increased creatine kinase,convulsions, bradycardia, confusion) and enhancement of theactions of suxamethonium.[Alois Alzheimer (1864–1915), German neurologist andpathologist]See also, Neuromuscular transmission; Organophosphoruspoisoning
N-Acetylcysteine. Derivative of the naturally occurringamino acid, l-cysteine. A free radical scavenger, it acts asan antidote in paracetamol poisoning, probably by restoringdepleted hepatic stores of glutathione or by acting as analternative substrate for a toxic metabolite of paracetamol.Also used as an ocular lubricant.
Has been investigated for a possible role in protectionagainst myocardial reperfusion injury, treatment of ful-minant hepatic failure, and treatment of MODS, acutelung injury and neuropsychiatric complications of carbonmonoxide poisoning. Has also been used as a mucolyticbecause of its ability to split disulphide bonds in mucusglycoprotein.
l Dosage:w paracetamol poisoning: 150 mg/kg (to a maximum of12 g) in 200 ml 5% dextrose iv over 15 min, followed by50 mg/kg in 500 ml dextrose over 4 h, then 100 mg/kgin 1 litre dextrose over 16 h.
w to reduce viscosity of airway secretions: 200 mg8 hourly, orally. Has been delivered by nebuliser.
l Side effects: rashes, anaphylaxis. Has been associatedwithbronchospasm in asthmatics.
Achalasia. Disorder of oesophageal motility caused by idio-pathic degeneration of nerve cells in the myenteric plexus orvagal nuclei. Results in dysphagia and oesophageal dilatation.A similar condition may result from American trypanosomalinfection (Chagas’ disease). Aspiration pneumonitis orrepeated chest infections may occur. Achalasia is treated bymechanical distension of the lower oesophagus or by surgery.Heller’s cardiomyotomy (longitudinal myotomy leaving themucosa intact) may be undertaken via abdominal or thoracicapproaches. Preoperative respiratory assessment is essential.Patients are at high risk of aspirating oesophageal contents,and rapid sequence induction must be performed.[Carlos Chagas (1879–1934), Brazilian physician; Ernst Hel-ler (1877–1964), German surgeon]See also, Aspiration of gastric contents; Induction, rapidsequence
Achondroplasia. Skeletal disorder, inherited as an autoso-mal dominant gene, althoughmost cases arise by spontaneousmutation. Results in dwarfism, with normally sized trunk andshortened limbs. Flat face, bulging skull vault and spinaldeformity may make tracheal intubation difficult, and thelarynxmay be smaller than normal. Obstructive sleep apnoeamay occur. Foramen magnum and spinal canal stenoses maybe present. The former may result in cord compression onneck extension; the latter maymake central regional blockadedifficult and reduce volume requirements for epiduralanaesthesia.
Aciclovir. Antiviral drug; an analogue of nucleoside2’-deoxyguanosine. Inhibits viral DNA polymerase; activeagainst herpes viruses and used in the treatment of encephal-itis, varicella zoster (chickenpox/shingles) and postherpeticneuralgia, and for prophylaxis and treatment of herpes infec-tions in immunocompromised patients. Treatment shouldstart at onset of infection; the drug does not eradicate thevirus but may markedly attenuate the clinical infection.l Dosage:
w as topical cream, 5 times daily.w 200–800 mg orally, 2–5 times daily in adults.w 5–10 mg/kg 8 hourly iv, infused over 1 h.
l Side effects: rashes, GIT disturbances, hepatic and renalimpairment, blood dyscrasias, headache, dizziness, severelocal inflammation after iv use, confusion, convulsions,coma.
Acid. Substance which yields hydrogen ions in solution.
Acidaemia. Arterial pH < 7.35 or hydrogen ion concen-tration > 45 nmol/l.See also, Acid–base balance; Acidosis
Acid–base balance. Maintenance of stablepH in body fluidsis necessary for normal enzyme activity, ion distribution andprotein structure. Normally, blood pH is maintained at 7.35–7.45 (hydrogen ion (Hþ) concentration 35–45 nmol/l); intra-cellular pH changes with extracellular pH. During normal
4 Acetylcholinesterase inhibitors

metabolism of neutral substances, organic acids are producedwhich generate hydrogen ions.l Maintenance of pH depends on:
w buffers in tissues and blood, which minimise the in-crease of Hþ concentration.
w regulation by kidneys and lungs; the kidneys excreteabout 60–80 mmol and the lungs about 15–20000mmol Hþ per day.
Because of the relationship between CO2, carbonic acid,bicarbonate (HCO3
�) and Hþ, and the ability to excreteCO2 rapidly from the lungs, respiratory function is importantin acid–base balance:
H2Oþ CO2 Ð H2CO3 Ð HCO�3 þ Hþ
Thus hyper- and hypoventilation cause alkalosis and acidosisrespectively. Similarly, hyper- or hypoventilation may com-pensate for non-respiratory acidosis or alkalosis respectively,by returning pH towards normal.
Sources of Hþ excreted via the kidneys include lactic acidfrom blood cells, muscle and brain, sulphuric acid from me-tabolism of sulphur-containing proteins, and acetoacetic acidfrom fatty acid metabolism.l The kidney can compensate for acid–base disturbances in
three ways:w by regulating the amount of HCO3
� reabsorbed. 80–90% of filtered HCO3
� is reabsorbed in the proximaltubule:- filtered sodium ion is exchanged for Hþ across thetubule cell membrane.
- filtered HCO3� and excreted Hþ form carbonic acid.
- carbonic acid is converted to CO2 and water by car-bonic anhydrase on the cell membrane.
- CO2 and water reform carbonic acid (catalysed againby carbonic anhydrase) within the cell.
- carbonic acid releases HCO3� and Hþ.
- HCO3� passes into the blood; Hþ is exchanged for
sodium ion, etc.w by forming dihydrogen phosphate from monohydrogenphosphate in the distal tubule (HPO4
2�þHþ!H2PO4�).
The Hþ is supplied from carbonic acid, leaving HCO3�
which passes into the blood.w by combination of ammonia, passing out of the cells,with Hþ, supplied as above. The resultant ammoniumions cannot pass back into the cells.
In acid–base disorders, the primary change determineswhether a disturbance is respiratory or metabolic. The direc-tion of change in Hþ concentration determines acidosis oralkalosis. Renal or respiratory compensation attempts torestore normal pH, not reverse the primary change. Forexample, in the Henderson–Hasselbalch equation:
pH ¼ pKa þ log[HCO�
3 ]
[CO2]
adjustment of the HCO3�/CO2 concentration ratio restores
pH towards its normal value, e.g.:w primary change: increased CO2; leads to decreased pH(respiratory acidosis).
w compensation: HCO3� retention by kidneys; increased
ammonium secretion, etc.An ‘alternative approach’ suggestedbyStewart in 1983 focuseson the strong ion difference to explain the underlying pro-cesses rather than the above ‘traditional approach’ which con-centratesmore on interpretation ofmeasurements. It is based onthe degree of dissociation of ions in solution, in particular theeffects of strong ions and weak acids, and the role of bicarbon-ate as a marker of acid–base imbalance rather than a cause.[Peter Stewart (1921–1993), Canadian physiologist]
See also, Acid; Base; Blood gas tensions; Breathing, controlof; Davenport diagram; Siggaard-Andersen nomogram
Acid–citrate–dextrose solution, see Blood storage
Acidosis. A process in which arterial pH < 7.35 (or hydro-gen ion > 45 mmol/l), or would be < 7.35 if there were nocompensatory mechanisms of acid–base balance.See also, Acidosis, metabolic; Acidosis, respiratory
Acidosis, metabolic. Acidosis due to metabolic causes,resulting in an inappropriately low pH for the measuredarterial Pco2.l Caused by:
w increased acid production:- ketone bodies, e.g. in diabetes mellitus.- lactate, e.g. in shock, exercise.
w acid ingestion: e.g. salicylate poisoning.w failure to excrete hydrogen ion (Hþ):- renal failure.- distal renal tubular acidosis.- carbonic anhydrase inhibitors.
w loss of bicarbonate:- diarrhoea.- gastrointestinal fistulae.- proximal renal tubular acidosis.- ureteroenterostomy.
l May be differentiated by the presence or absence of ananion gap:w anion gap metabolic acidosis occurs in renal failure,lactic acidosis, ketoacidosis, rhabdomyolysis and fol-lowing ingestion of certain toxins (e.g. salicylates,methanol, ethylene glycol).
w non-anion gap (hyperchloraemic) metabolic acidosis iscaused by the administration of chloride-containingsolutions (e.g. saline) in large volumes, amino acidsolutions, diarrhoea, pancreatic fistulae, ileal loop pro-cedures, after rapid correction of a chronically compen-sated respiratory alkalosis or renal tubular acidosis.
l Primary change: increased Hþ/decreased bicarbonate.l Compensation:
w hyperventilation: plasma bicarbonate falls by about1.3 mmol/l for every 1 kPa acute decrease in arterialPco2, which usually does not fall below 1.3–1.9 kPa(10–15 mmHg).
w increased renal Hþ secretion.l Effects:
w hyperventilation (Kussmaul breathing).w confusion, weakness, coma.w cardiac depression.w hyperkalaemia.
l Treatment:w of underlying cause.w bicarbonate therapy is reserved for treatment of severeacidaemia (e.g. pH under 7.1) because of problemsassociated with its use.If bicarbonate is required, a formula for iv infusion is:
base excess� body weight (kg)
3mmol
Half this amount is given initially.w other agents under investigation include sodiumdichloroacetate, Carbicarb (sodium bicarbonate andcarbonate in equimolar concentrations) and THAM(2-amino-2-hydroxymethyl-1,3-propanediol).
Morris CG, Low J (2008). Anaesthesia; 63: 294–301 and396–411See also, Acidaemia; Acid–base balance
Acidosis, metabolic 5

Acidosis, respiratory. Acidosis due to increased arterialPco2. Caused by alveolar hypoventilation.l Primary change: increased arterial Pco2.l Compensation:
w initial rise in plasma bicarbonate due to increased car-bonic acid formation and dissociation.
w increased acid secretion/bicarbonate retention by thekidneys. In acute hypercapnia, bicarbonate concentra-tion increases by about 0.7 mmol/l per 1 kPa rise inarterial Pco2. In chronic hypercapnia it increases by2.6 mmol/l per 1 kPa.
l Effects: those of hypercapnia.l Treatment: of underlying cause.See also, Acidaemia; Acid–base balance
ACLS, see Advanced Cardiac Life Support
Acquired immune deficiency syndrome (AIDS), seeHuman immunodeficiency viral infection
Acromegaly. Disease caused by excessive growth hor-mone secretion after puberty; usually caused by a pituitaryadenoma but ectopic secretion may also occur. Incidence is6–8 per million population.l Features:
w enlarged jaw, tongue and larynx; widespread increase insoft tissue mass; enlarged feet and hands. Nerve entrap-ment may occur, e.g. carpal tunnel syndrome.
w respiratory obstruction, including sleep apnoea.w tendency towards diabetes mellitus, hypertension andcardiac failure (may be due to cardiomyopathy).Thyroid and adrenal impairment may occur.
Apart from the above diseases, acromegaly may presentdifficulties with tracheal intubation and maintenance ofthe airway.
Treatment is primarily pituitary surgery with or without sub-sequent radiotherapy. Some patients respond to bromocrip-tine or somatostatin analogues.Smith M, Hirsch NP (2000). Br J Anaesth; 85: 3–14
ACT, Activated clotting time, see Coagulation studies
Acta Anaesthesiologica Scandinavica. Official journal ofthe Scandinavian Society of Anaesthesiology and IntensiveCare Medicine, first published in 1957.
ACTH, see Adrenocorticotrophic hormone
Actin. One of the protein components of muscle (mw43 000). In muscle, arranged into a double strand of thinfilaments (F-actin) with globular ‘beads’ (G-actin), to whichmyosin binds, along their length. Present in all cells as micro-filaments.See also, Muscle contraction
Action potential. Sequential changes in transmembranepotential that result in the propagation of electrical impulsesin excitable cells (Fig. 4a).l Stages involved are summarised as follows:
w A: depolarisation of the membrane by 15 mV (thresholdlevel).
w B: rapid depolarisation to þ40 mV.w C: repolarisation, rapid at first then slow.w D: hyperpolarisation.w E: return to the resting membrane potential.
Depolarisation causes opening of sodium channels andentry of sodium ions into the cell, which causes further de-
polarisation. Sodium permeability then falls. Potassiumpermeability increases slowly and helps bring about repolar-isation. Normal ion distribution is restored due to action of thesodium/potassium pump. The action potential is followedby a refractory period.
Action potentials in nerve and other cells involve similarchanges; in cardiac muscle, however, a plateau followsdepolarisation, brought about by calcium entry. The refractoryperiod is thus lengthened (Fig. 4b).l There are five phases of the cardiac action potential:
w phase 0: fast depolarisation and sodium entry.w phase 1: onset of repolarisation due to sodium channelclosure.
w phase 2: plateau due to calcium entry.w phase 3: repolarisation.w phase 4: resting membrane potential. In pacemakercells, there is slow spontaneous depolarisation, due todecreased potassium permeability, leading to initiationof impulses.
See also, Nerve conduction
Activated charcoal, see Charcoal, activated
Activated clotting time, see Coagulation studies
Activated protein C, see Drotrecogin alfa; Protein C
Activation energy. Energy required to initiate a chemicalreaction. For ignition of explosive mixtures of anaesthetic
–55–70
+40
0 21 3
mV
Time (ms)
A
BC
DE
0
(a)
–90
+20
0 100 200
mV
Time (ms)
0
12
3
4
0
(b)
Fig. 4 (a) Nerve action potential (solid) showing changes in sodium
(dotted) and potassium (dashed) conductance. (b) Cardiac action
potential (see text)
6 Acidosis, respiratory

agents the energy may be provided by sparks, e.g. from build-up of static electricity or electrical equipment. Combustion ofcyclopropane requires less activation energy than thatof diethyl ether. Activation energy is less for mixtures withO2 than with air, and least for stoichiometric mixtures ofreactants.See also, Explosions and fires
Active compression/decompression cardiopulmon-ary resuscitation, see Cardiac massage; Cardiopulmonaryresuscitation
Active transport. Energy-requiring transport of particlesacross cell membranes. Protein ‘pumps’ within the mem-branes utilise energy which is usually supplied by ATPmetabolism, in order to move ions and molecules, oftenagainst concentration gradients. A typical example is thesodium/potassium pump.
Acupuncture. Use of fine needles (usually 30–33 G) toproduce healing and pain relief. Originated in China thou-sands of years ago, and closely linkedwith the philosophy andpractice of traditional Chinese medicine. Thus abnormalitiesin the flow of Qi (Chi: the life energy that circulates aroundthe body along meridians, nourishing the internal organs)result in imbalance between Yin and Yang, the two polaropposites present in all aspects of the universe. Internalabnormalities may be diagnosed by pulse diagnosis (palpationof the radial arteries at different positions and depths).The appropriate organ is then treated by acupuncture atspecific points on the skin, often along the meridian namedafter, and related to, that organ. Yin and Yang, and flow of Qi,are thus restored.
Modern Western acupuncture involves needle insertion atsites chosen for more ‘scientific’ reasons; e.g. around anaffected area, at trigger points found nearby, or more prox-imally but within the appropriate dermatome. These may becombined with distant or local traditional points, althoughconclusive evidence for the existence of acupuncture pointsand meridians has never been shown. The needles may be leftinserted and stimulated manually, electrically or thermally toincrease intensity of stimulation. Pressure at acupuncturepoints (acupressure) may produce similar but less intensestimulation.l Possible mechanisms:
w local reflex pathways at spinal level.w closure of the ‘gate’ in the gate control theory of pain.w central release of endorphins/enkephalins, and pos-sibly involvement of other neurotransmitters.
w modulation of the ‘memory’ of pain.Still used widely in China. Increasingly used in the West forchronic pain, musculoskeletal disorders, headache and mi-graine, and other disorders in which modern Western medi-cine has had little success. Claims that acupuncture may beemployed alone to provide analgesia for surgery are nowviewed with scepticism, although it has been used to provideanalgesia and reduce PONV (e.g. 5 minutes’ stimulation atthe point P6 (Pericardium 6: 1–2 inches (2.5–5 cm) proximalto the distal wrist crease, between flexor carpi radialis andpalmaris longus tendons).Wang SM, Kain ZN, White P (2008). Anesth Analg; 106:602–10 and 611–21
Acute cortical necrosis, see Renal failure
Acute crisis resource management, see Crisis resourcemanagement
Acute demyelinating encephalomyelopathy, see De-myelinating diseases
Acute life-threatening events – recognition and treat-ment (ALERT). Multiprofessional course developed in aneffort to reduce the incidence of potentially avoidable car-diac arrests, admissions to ICU and in-hospital deaths.Aimed especially at pre-registration house officers, wardnurses and physiotherapists, but suitable for other clinicalgroups. Based on principles of many life-support trainingprogrammes (e.g. ALS, ATLS, APLS, CCrISP), its devel-opment embraces both clinical governance and multiprofes-sional education. Uses a structured and prioritised system ofpatient assessment and management to assist ward staff torecognise patients at risk of deterioration and those who arealready seriously ill. Using a system of assessment similar tothat of CCrISP, participants are taught to manage life-threat-ening events and to organise subsequent care.Smith GB, Osgood VM, Crane S (2002). Resuscitation; 52:281–6See also, Early warning scores; Medical emergency team;Outreach team
Acute lung injury (ALI). Syndrome of inflammation andincreased permeability of lung tissue associated with a varietyof clinical, radiological and physiological abnormalities thatcannot be explained by, but may coexist with, left atrial orpulmonary capillary hypertension. Associated with sepsis,multiple trauma, aspiration pneumonitis, multiple bloodtransfusion, pancreatitis, cardiopulmonary bypass and fatembolism. Onset is usually within 2–3 days of the precipitat-ing illness or injury, although direct lung insults usually havea shorter insult-to-onset time. Acute respiratory distresssyndrome (ARDS) is now regarded to be the most severeform of ALI. Both ARDS and ALI have similar diagnosticfeatures which include:
w acute onset.w bilateral diffuse infiltrates seen on the chest X-ray.w pulmonary wedge pressure £ 18 mmHg or absence ofclinical evidence of left atrial hypertension.
w arterial hypoxaemia resistant to oxygen therapy alone(Pao2/FIo2 < 39.9 kPa [300 mmHg] for definition ofALI; < 26.6 kPa [200 mmHg] for definition ofARDS), regardless of the level of PEEP.
The definitions of ALI and ARDS are increasingly beingchallenged.Other features:
w reduced respiratory compliance, lung volumes andincreased work of breathing.
w V·/Q·mismatch and increased shunt.
w pulmonary vascular resistance may be raised.w an air bronchogram may be seen on the chest X-ray.w in uncomplicated ALI, plasma oncotic pressure isnormal.
w MODS may occur and is a common cause of death.l Pathophysiology: ALI results from damage to either the
lung epithelium or endothelium. Two pathways of injuryexist:w direct effects of an insult on lung cells, e.g. aspiration,smoke inhalation.
w indirect result of an acute systemic inflammatoryresponse involving both humoral (activation of comple-ment, coagulation and kinin systems; release ofmediators including cytokines, oxidants, nitric oxide,etc.) and cellular (neutrophils, macrophages andlymphocytes) components. Pulmonary infiltration byneutrophils leads to interstitial fibrosis, possibly as a
Acute lung injury 7

result of damage caused by free radicals. Examplesinclude sepsis, pancreatitis, fat embolism, etc.
Histopathological findings can be divided into threephases: exudative (oedema and haemorrhage), prolifera-tive (organisation and repair) and fibrotic.
l Treatment is largely supportive:w general support: nutrition, DVT prophylaxis, preven-tion of infection, etc.
w O2 therapy (trying where possible to keep FIo2 below0.6). CPAP is often helpful as it improves FRC.
w ventilatory support: IPPV may be necessary if CPAPis ineffective. PEEP is often required, but airwaypressure is often already high because of reducedcompliance, increasing the risk of barotrauma andimpaired cardiac output. CO2 elimination may demandincreasing minute volumes but this too risks ventila-tor-associated lung injury. This has led to the devel-opment of lung protection strategies includinglow-frequency minute volume ventilation with extra-corporeal CO2 removal, permissive hypercapniaand the use of smaller than normal tidal volumes.Other ventilatory strategies used to minimise ventila-tor-associated lung injury in ALI include inverse ratioventilation (at I:E ratios of up to 4:1), airway pres-sure release ventilation and high frequency ventila-tion. Extracorporeal membrane oxygenation hasbeen used with varying success.
w posture of the patient: prone ventilation may improveoxygenation in some patients.
w fluid restriction is usually instituted to reduce lungwater, although avoidance of initial fluid overload isthought to be more important. Diuretics have beenused, with careful monitoring of renal function.
w vasodilator drugs have been used to decrease pul-monary vascular resistance, e.g. prostacyclin. Nitricoxide has also been used to produce pulmonary vaso-dilatation, but there is, as yet, little evidence of long-term benefit.
w fears over leakage of colloids into pulmonary interstitialspaces, with subsequent exacerbation of oedema, arebalanced by possible advantages of colloids in maintain-ing oncotic pressure.
w corticosteroid therapy is controversial. There appearsto be no benefit to their prophylactic administration, norin high-dose, short-term therapy at the onset of ALI/ARDS. However, corticosteroids may have a role innon-resolving ARDS.
w free radical scavengers, antiprostaglandins and antipro-teases have been investigated.
Wheeler AP, Bernard GR (2007). Lancet; 369: 1553–64
Acute phase response. A reaction of the haemopoietic andhepatic systems to inflammation or tissue injury, assumed tobe of benefit to the host. There is a rise in the number/activityof certain cells (neutrophils, platelets) and plasma proteins(e.g. fibrinogen, complement,C-reactive protein, plasmino-gen, haptoglobin) involved in host defence, whilst there is areduction in proteins which have transport and binding func-tions (e.g. albumin, haemoglobin, transferrin). Initiated byactions of cytokine mediators such as interleukins (IL-1a,IL-1b, IL-6 and IL-11), tumour necrosis factors (a and b) andleukaemia inhibitory factor.
Serum levels of acute phase proteins (e.g. C-reactive pro-tein) can be helpful in diagnosis, monitoring and prognosis ofcertain diseases. The rise in fibrinogen levels causes an ele-vation inESR. The fall in albumin is due to redistribution anddecreased hepatic synthesis.
Acute physiology, age, chronic health evaluation, seeAPACHE III scoring system
Acute physiology and chronic health evaluation, seeAPACHE/APACHE II scoring systems
Acute physiology score (APS). Physiological componentof severity of illness scoring systems, such asAPACHE II/IIIand Simplified APS.Weighted values (e.g. 0 to 4 in APACHEII) are assigned to each of a range of physiological variables(e.g. temperature, mean arterial blood pressure, serum creati-nine) on the basis of its derangement from an established‘normal’ range, as measured either upon ICU admission orwithin 24 h of entry. The sum of all assigned weighted valuesfor the physiological variables that comprise a given scoringsystem constitutes the acute physiological score. The higherthe acute physiology score, the sicker the patient.See also, Mortality/survival prediction on intensive care unit;Simplified acute physiology score
Acute respiratory distress syndrome (ARDS). Previ-ously termed adult respiratory distress syndrome, despite theprocess also occurring in children. First described in 1967 asnon-cardiogenic pulmonary oedema secondary to condi-tions not primarily affecting the lungs (e.g. shock, sepsis,pancreatitis, massive blood transfusion, fat embolism).Now regarded as the most severe form of acute lung injury(ALI). Distinguished from ALI purely on the Pao2/FIo2 ratiowhich is < 26.6 kPa (200 mmHg) for ARDS.
Pathophysiology, treatment, etc. is as for ALI. Histo-logical appearances are similar to respiratory distress syn-drome of the newborn, hence its name. Overall mortality ofARDS is approximately 50–60% but depends on the under-lying cause; it is highest following aspiration pneumonitisor sepsis. Early deaths are rare, and patients dying late in thecourse of the illness usually die with hypoxaemia not becauseof it. For survivors, residual pulmonary impairment is pos-sible but rarely severe.Wheeler AP, Bernard GR (2007). Lancet; 369: 1553–64
Acute tubular necrosis, see Renal failure
Acyclovir, see Aciclovir
Addiction, see Alcoholism; Substance abuse
Addison’s disease, see Adrenocortical insufficiency
ADEM, Acute demyelinating encephalomyelopathy, seeDemyelinating diseases
Adenosine. Nucleoside, of importance in energy homeo-stasis at the cellular level. Reduces O2 consumption, increasescoronary blood flow, causes vasodilatation and slows atrio-ventricular conduction (possibly via increased potassiumconductance and reduced calcium conductance). Also aninhibitory CNS neurotransmitter.
Has become the drug of choice for treatment of SVT(including that associated with Wolff–Parkinson–Whitesyndrome) and diagnosis of other tachyarrhythmias by slow-ing atrioventricular conduction. Its short half-life (8–10 s)and lack of negative inotropism make it an attractive alterna-tive to verapamil. Unclassified as an antiarrhythmic drug.
Has also been used as a directly acting vasodilator drug inhypotensive anaesthesia. Increases cardiac output, withstable heart rate. Its effects are rapidly reversible on stoppingthe infusion.
8 Acute phase response

l Dosage:w SVT: 3 mg by rapid iv injection; if unsuccessful after 1–2 min this is followed by 6 mg and then 12 mg.
w hypotensive anaesthesia: 50–300 mg/kg/min. ATP hasalso been used.
l Side effects are usually mild and include flushing, dys-pnoea and nausea. Bronchoconstriction may occur in asth-matics. Bradycardia is resistant to atropine. Adenosine’saction is prolonged in dipyridamole therapy (becauseuptake of adenosine is inhibited) and reduced by theo-phylline and other xanthines (because of competitiveantagonism). Transplanted hearts are particularly sensitiveto adenosine’s effects.
Adenosine monophosphate, cyclic (cAMP). Cyclicadenosine 3’,5’-monophosphate, formed from ATP by theenzyme adenylate cyclase. Activation of surface receptorsmay cause a guanine nucleotide regulatory protein (G pro-tein) to interact with adenylate cyclase with resultantincreases in intracellular cAMP levels (Fig. 5). Many sub-stances act on surface receptors in this way, including cat-echolamines (b effects), vasopressin, ACTH, histamine,glucagon, parathyroid hormone and calcitonin.
Some substances inhibit adenylate cyclase via an inhibitoryregulatoryprotein, e.g.noradrenalineata2-adrenergic receptors.
cAMP causes phosphorylation of proteins, particularlyenzymes, by activating protein kinases. Phosphorylationchanges enzyme activity and therefore cell metabolism; thusthe intracellular concentration of cAMP determines cellactivity, and cAMP acts as a ‘second messenger’.
cAMP is inactivated by phosphodiesterase to 5’-AMP.Phosphodiesterase inhibitors, e.g. aminophylline andenoximone, increase cAMP levels.
Adenosine triphosphate and diphosphate (ATP andADP). ATP is the most important high-energy phosphatecompound. When hydrolysed to form ADP, it releases largeamounts of energy which may be utilised in many cellularprocesses, e.g. active transport,muscle contraction, etc. Itsphosphate bonds are formed using energy from catabolism;aerobic glycolysis generates 38 moles of ATP per mole ofglucose, and anaerobic glycolysis yields 2 moles of ATP.
Other high-energy phosphate compounds include phos-phorylcreatine (in muscle), ADP itself, and other nucleotides.See also, Cytochrome oxidase system; Metabolism; Tricar-boxylic acid cycle
Adenylate cyclase, see Adenosine monophosphate, cyclic
ADH, Antidiuretic hormone, see Vasopressin
Adhesion molecules. Molecules normally sited on cellsurfaces, involved in embryogenesis, cell growth and differ-entiation, and wound repair. Also mediate endothelial cell/leucocyte adhesion, transendothelial migration and cytotoxicT cell-induced lysis. Four major families exist: integrins,cadherins, selectins (named after the tissues in which theywere discovered: L-selectin (leucocytes), E-selectin (endo-thelial cells), P-selectin (platelets)) and members of theimmunoglobulin superfamily.
In general, contact between an adhesion receptor and theextracellular milieu results in the transmission of informationallowing the cell to interact with its environment. Defectiveinteractions involving adhesion molecules are implicated indisease (e.g. certain skin diseases, metastasis of cancer cells).Many pathogens use adhesion receptors to penetrate tissuecells. Overexpression of intravascular adhesion molecules orreceptors has been implicated in rheumatoid arthritis andrejection of transplanted organs. Control of vascular integrityand defence against invasive pathogens requires regulation ofadhesive interactions among blood cells and between bloodcells and the vessel walls. Circulating leucocytes bind to theselectins of activated endothelial cells, become activated bychemoattractants andmigrate through intracellular gaps to thesite of inflammation. Thus adhesion molecules play a part inthe inflammatory response in sepsis.
Adiabatic change. Volume change of a gas in which there isno transfer of heat to or from the system. Sudden compressionof a gas without removal of resultant heat causes a rise intemperature. This may occur in the gas already present in thevalves and pipes of an anaesthetic machine when a cylinderis turned on (hence the danger of explosion if oil or grease ispresent). Sudden adiabatic expansion of a gas results in cool-ing, as in the cryoprobe.See also, Isothermal change
Adjustable pressure-limiting valves. Valves which opento allow passage of expired and surplus fresh gas from abreathing system, but close to prevent indrawing of air.Ideally the opening pressure should be as low as possible toreduce resistance to expiration, but not so low as to allow thereservoir bag to empty through it. Most contain a thin discheld against its seating by a spring, as in the original Heid-brink valve. Adjusting the tension in the spring, usually byscrewing the valve top, alters the pressure at which the valveopens. The valve must be vertical in order to functioncorrectly.
Modern valves, even when screwed fully down, will openat high pressures (60 cmH2O). Most are now encased in ahood for scavenging of waste gases.[Jay A Heidbrink (1875–1957), US anaesthetist]See also, Anaesthetic breathing systems; Non-rebreathingvalves
ADP, see Adenosine triphosphate and diphosphate
Adrenal gland. Situated on the upper pole of the kidney,each gland is composed of an outer cortex and an innermedulla. The cortex consists of the outer zona glomerulosa(secreting aldosterone), the middle zona fasciculata (secret-ing glucocorticoids) and inner zona reticularis (secreting sexhormones). Hypersecretion may result in hyperaldosteron-ism, Cushing’s syndrome and virilisation/feminisation
Cell membrane
ββ-Receptor αα2-Receptor
ATP cAMP 5'-AMP
Phosphodiesterase
Protein kinase
Gs, stimulatory guanine nucleotide regulatory proteinGi, inhibitory guanine nucleotide regulatory protein
Phosphorylation of enzymes + other proteins
Adenylatecyclase
Gs Gi
Fig. 5 cAMP involvement in transmembrane signalling
Adrenal gland 9

respectively. Hyposecretion causes adrenocortical insuffi-ciency.
The adrenal medulla is thought to be derived from a sym-pathetic ganglion in which the postganglionic neurones havelost their axons, and secrete catecholamines into the blood-stream. Hypersecretion results in phaeochromocytoma.See also, Sympathetic nervous system
Adrenaline (Epinephrine). Catecholamine, acting as a hor-mone and neurotransmitter in the sympathetic nervoussystem and brainstem pathways. Synthesised and releasedfrom the adrenal glandmedulla and central adrenergic neur-ones ( for structure, synthesis and metabolism, see Catechol-amines). Called epinephrine in the USA because the nameadrenaline, used in other countries, was too similar tothe US-registered trade name Adrenalin that referred to aspecific product (both adrenaline (Latin) and epinephrine(Greek) referring to the location of the adrenal gland ‘on thekidney’).
Stimulates both a- and b-adrenergic receptors; displayspredominantly b-effects at low doses, a- at higher doses. Lowdose infusion may lower BP by causing vasodilatation inmuscle via b2-receptors, despite increased cardiac output viab1-receptors. Higher doses cause a-mediated vasoconstric-tion and increased systolic BP, although diastolic pressuremay still decrease.l Clinical uses:
w with local anaesthetic agents, as a vasoconstrictor.w in anaphylactic reaction, cardiac arrest, bronchos-pasm.
w as an inotropic drug.w in glaucoma (reduces aqueous humour production).w in croup.
Adrenaline may cause cardiac arrhythmias, especially in thepresence of hypercapnia, hypoxia and certain drugs, e.g.halothane, cyclopropane and cocaine. During halothaneanaesthesia, suggested maximal dosage of adrenaline is10 ml 1:100000 solution (100 mg) in 10 min, or 30 ml(300 mg) in 1 h. More dilute solutions should be used ifpossible. Adrenaline should not be used for ring blocks ofdigits or for penile nerve blocks, because of possible ischae-mia to distal tissues.l Dosage:
w anaphylaxis: 0.1 mg iv (1 ml 1:10000 solution),repeated as required. The recommended initial route ingeneral medical guidelines is usually im (0.5–1.0 ml1:1000 solution), reflecting the risks of iv administrationwithout appropriate monitoring.
w cardiac arrest: 1 mg (10 ml 1:10 000) iv.w by infusion: 0.01–0.15 mg/kg/min initially, increasingas required.
w croup: 0.4 ml/kg nebulised up to 5 ml maximum,repeated after 30 min if required.
Subcutaneous injection in shocked patients results in un-reliable absorption. Adrenaline may be administered via atracheal tube in 2–3 times the iv dose.
See also, Tracheal administration of drugs
a-Adrenergic receptor agonists. Naturally occurringagonists include adrenaline and noradrenaline whichstimulate both a1- and a2-adrenergic receptors.
Methoxamine andphenylephrine are synthetica1-receptoragonists, used to cause vasoconstriction, e.g. to correcthypotension in spinal anaesthesia.
Clonidine acts on central a2-receptors. Clonidine andother a2-receptor agonists (e.g. dexmedetomidine) havebeen shown to reduce pain sensation and reduce requirements
for general anaesthetics and have also been used for sedationin ICU. Other a2-receptor agonists (e.g. xylazine, detomidineand medetomidine) have been used in veterinary practice asanaesthetic agents for many years.
b-Adrenergic receptor agonists. Agonists includeadrenaline and isoprenaline which stimulate both b1- andb2-adrenergic receptors. Dopamine and dobutamine actmainly at b1-receptors.
Salbutamol and terbutaline predominantly affectb2-receptors, and are used clinically to cause bronchodilatationin asthma, and as tocolytic drugs in premature labour. For-oterol and salmeterol are longer acting agents given by inhal-ation for chronic asthma. Ritodrine is also used as a tocolyticdrug. Some b1-receptor effects are seen at high doses, e.g.tachycardia. They have been used in the treatment of cardiacfailure and cardiogenic shock; stimulation of vascularb2-receptors causes vasodilatation and reduces afterload.
a-Adrenergic receptor antagonists (a-Blockers). Usu-ally refer to antagonistswhich act exclusively ata-adrenergicreceptors.l Drugs may be:
w selective:- a1-receptors, e.g. prazosin, doxazosin, terazosin, indora-min, phenoxybenzamine. Tamsulosin acts specifically ata1A-receptors and is used in benign prostatic hypertrophy.
- a2-receptors: yohimbine.w non-selective, e.g. phentolamine.
Labetalol and carvedilol (a drug with similar effects) areantagonists at both a- and b-receptors. Other drugs may alsoact at a-receptors as part of a range of effects, e.g. chlorpro-mazine, droperidol.
Antagonism may be competitive, e.g. phentolamine, ornon-competitive and therefore longer-lasting, e.g. phenoxy-benzamine.
Used to lower BP and reduce afterload by causing vaso-dilatation. Compensatory tachycardia may occur.l Side effects: postural hypotension, dizziness, tachycardia
(less so with the selective a1-antagonists, possibly becausethe negative feedback of noradrenaline at a2-receptors isunaffected). Tachyphylaxis may occur.
b-Adrenergic receptor antagonists (b-Blockers). Com-petitive antagonists at b-adrenergic receptors.l Actions:
w reduce heart rate, force of contraction and myocardialO2 consumption.
w increase coronary blood flow by increasing diastolicfilling time.
w antiarrhythmic action results from b-receptor antagonismand possibly a membrane-stabilising effect at high doses.
w antihypertensive action (not fully understood but mayinvolve reductions in cardiac output, central sympa-thetic activity, and renin levels).
w some have partial agonist activity (intrinsic sympatho-mimetic activity), e.g. pindolol, acebutolol, celiprololand oxprenolol.
w practolol, atenolol, metoprolol, betaxolol, bisoprolol,nebivolol and acebutolol are relatively cardioselective,but all will block b2-receptors at high doses. Celiprololhas b1-receptor antagonist and b2-receptor agonist prop-erties, thus causing peripheral vasodilatation in additionto cardiac effects.
w labetalol and carvedilol have a- and b-receptor blockingproperties. The former is available for iv administrationand is widely used for acute reduction in BP.
10 Adrenaline