Anaconda Experiment in Endovascular Stent Therapy … · Central Annals of Vascular Medicine &...
5
Central Annals of Vascular Medicine & Research Cite this article: Erdogan MB, Zor H, Ozcaliskan O, Erdogmus O (2015) Anaconda Experiment in Endovascular Stent Therapy of Abdominal Aortic Aneurysms: Early Results of a Single Center. Ann Vasc Med Res 2(2): 1016. *Corresponding author Ozerdem Ozcaliskan, Medical Park Gaziantep Hospital, Department of Cardiovascular Surgery, Gaziantep, Turkey, Tel: 90 533 7658138; Email: Submitted: 03 March 2015 Accepted: 22 April 2015 Published: 24 April 2015 Copyright © 2015 Ozcaliskan et al. OPEN ACCESS Keywords • Abdominal aortic aneurysm • Endovascular stent treatment • Anaconda Research Article Anaconda Experiment in Endovascular Stent Therapy of Abdominal Aortic Aneurysms: Early Results of a Single Center Mustafa Bilge Erdogan 1 , Hakan Zor 2 , Ozerdem Ozcaliskan 1 , Onur Erdogmus 3 1 Department of Cardiovascular Surgery, Medical Park Gaziantep Hospital Cardiovascular Surgery Clinic, Turkey 2 Department of Cardiovascular Surgery, Gazi University Cardiovascular Surgery Clinic, Turkey 3 Department of Cardiovascular Surgery, Medical Park Gaziantep Hospital Cardiology Clinic, Turkey Abstract Background: We investigated the efficacy, preoperative, postoperative and early stage outcomes of Anaconda type endovascular stent-grafts in patients who had intervention in our clinic with the diagnosis of abdominal aortic aneurysm. Material – Methods: During the years of 2010 and 2013, 23 patients (19 male, 4 female) had endovascular stent-graft procedure with the diagnosis of infrarenal abdominal aortic aneurysm. The mean age was 76.1 (67-82). All patients had Anaconda endovascular stent graft procedure. Results: The intervention was performed to all patients in angiology laboratory under the sterilization and technical conditions of a surgery room. Aortoiliac stenting was done for all patients. The mean procedural time was 70.5 (55-97) minutes. No patient required open surgery. Graft placement was successful in all patients. None of the patients died during the procedure. One patient died in early stage due to congestive heart failure and pulmonary edema. None of the patients had graft infection or aneurysmal rupture. Conclusions: In selected patients with abdominal aortic aneurysm, early stage mortality and morbidity of stent graft procedure are low. Procedure is technically easy to apply with high success rates. Good preoperative preparation, technically well equipped catheter laboratory and an experienced surgical team are sufficient for that. BACKGROUND Standard treatment in abdominal aortic aneurysms is still surgical treatment [1]. However, endovascular stent graft application in selected cases has being used more common. Since the procedure is particularly performed with an easy technique and being less invasive; at first, it was used in selective atherosclerotic, infectious and inflammatory cases; it has also being used in traumatic or atherosclerotic aortic dissections, traumatic or iatrogenic pseudo aneurysms. Lower mortality and morbidity rates and short hospital stay durations are among the most important reasons to be preferred [2]. The short and mid- term outcomes so far, have showed that this method, especially when it’s preferred in patients with high surgical risk, has low mortality and morbidity [3]. It was reported that the most important problem in different series and various stent materials is endoleak (%11-44) [4,5]. However, long term outcomes are still not known. In our study, we aimed to investigate the operative and postoperative early stage outcomes of aortoiliac endovascular grafts applied in our clinic in the years of 2010 and 2013. MATERIAL – METHODS During the years of 2010 and 2013, 23 patients (19 male, 4 female) had endovascular stent-graft procedure (Figure 1) with the diagnosis of infrarenal abdominal aortic aneurysm. The mean age was 76.1 (67-82). All patients were evaluated with 3 mm
Transcript of Anaconda Experiment in Endovascular Stent Therapy … · Central Annals of Vascular Medicine &...

Central Annals of Vascular Medicine & Research
Cite this article: Erdogan MB, Zor H, Ozcaliskan O, Erdogmus O (2015) Anaconda Experiment in Endovascular Stent Therapy of Abdominal Aortic Aneurysms: Early Results of a Single Center. Ann Vasc Med Res 2(2): 1016.
*Corresponding authorOzerdem Ozcaliskan, Medical Park Gaziantep Hospital, Department of Cardiovascular Surgery, Gaziantep, Turkey, Tel: 90 533 7658138; Email:
Submitted: 03 March 2015
Accepted: 22 April 2015
Published: 24 April 2015
Copyright© 2015 Ozcaliskan et al.
OPEN ACCESS
Keywords•Abdominal aortic aneurysm•Endovascular stent treatment•Anaconda
Research Article
Anaconda Experiment in Endovascular Stent Therapy of Abdominal Aortic Aneurysms: Early Results of a Single CenterMustafa Bilge Erdogan1, Hakan Zor2, Ozerdem Ozcaliskan1, Onur Erdogmus3
1Department of Cardiovascular Surgery, Medical Park Gaziantep Hospital Cardiovascular Surgery Clinic, Turkey2Department of Cardiovascular Surgery, Gazi University Cardiovascular Surgery Clinic, Turkey3Department of Cardiovascular Surgery, Medical Park Gaziantep Hospital Cardiology Clinic, Turkey
Abstract
Background: We investigated the efficacy, preoperative, postoperative and early stage outcomes of Anaconda type endovascular stent-grafts in patients who had intervention in our clinic with the diagnosis of abdominal aortic aneurysm.
Material – Methods: During the years of 2010 and 2013, 23 patients (19 male, 4 female) had endovascular stent-graft procedure with the diagnosis of infrarenal abdominal aortic aneurysm. The mean age was 76.1 (67-82). All patients had Anaconda endovascular stent graft procedure.
Results: The intervention was performed to all patients in angiology laboratory under the sterilization and technical conditions of a surgery room. Aortoiliac stenting was done for all patients. The mean procedural time was 70.5 (55-97) minutes. No patient required open surgery. Graft placement was successful in all patients. None of the patients died during the procedure. One patient died in early stage due to congestive heart failure and pulmonary edema. None of the patients had graft infection or aneurysmal rupture.
Conclusions: In selected patients with abdominal aortic aneurysm, early stage mortality and morbidity of stent graft procedure are low. Procedure is technically easy to apply with high success rates. Good preoperative preparation, technically well equipped catheter laboratory and an experienced surgical team are sufficient for that.
BACKGROUNDStandard treatment in abdominal aortic aneurysms is still
surgical treatment [1]. However, endovascular stent graft application in selected cases has being used more common. Since the procedure is particularly performed with an easy technique and being less invasive; at first, it was used in selective atherosclerotic, infectious and inflammatory cases; it has also being used in traumatic or atherosclerotic aortic dissections, traumatic or iatrogenic pseudo aneurysms. Lower mortality and morbidity rates and short hospital stay durations are among the most important reasons to be preferred [2]. The short and mid-term outcomes so far, have showed that this method, especially when it’s preferred in patients with high surgical risk, has low
mortality and morbidity [3]. It was reported that the most important problem in different series and various stent materials is endoleak (%11-44) [4,5]. However, long term outcomes are still not known. In our study, we aimed to investigate the operative and postoperative early stage outcomes of aortoiliac endovascular grafts applied in our clinic in the years of 2010 and 2013.
MATERIAL – METHODSDuring the years of 2010 and 2013, 23 patients (19 male, 4
female) had endovascular stent-graft procedure (Figure 1) with the diagnosis of infrarenal abdominal aortic aneurysm. The mean age was 76.1 (67-82). All patients were evaluated with 3 mm
Central
Ozcaliskan et al. (2015)Email:
Ann Vasc Med Res 2(2): 1016 (2015) 2/5
section contrast computed tomography in preoperative term.
The largest diameter of infrarenal aorta, aortic bifurcation, iliac arteries and diameters were measured for all patients. The mean aneurysmal diameter was 58 mm (±3.5) and infrarenal non aneurysmatic region aeurysmal neck was 1.97 cm (±0.37). Besides, it was evaluated whether there were aortic wall calcifications, thrombus in vessel lumen and occlusion in distal vessels. Both common iliac mean diameters were 8.71 (±0.82). Moreover, the angle between aneurysmal sac and normal aorta in vertical plane was 48 (±12) degrees. During the procedures, all sizes of endovascular stent grafts were present. Following the measurements, grafts which were 20% larger than the proximal and distal intact vessel wall diameters were chosen. In case of need of switching to open surgery, all patients were prepared preoperatively. In case of open surgery, 6 units of total blood and fresh frozen plasma were kept ready for each patient.
The interventions were performed to all patients in angiology laboratory by cardiovascular surgeon, invasive cardiologist and anesthesiologist under the sterilization conditions of a surgery room. All patients had lumbar epidural catheter in preoperative stage by anesthesiology. During the procedure, isobaric marcain was used as anesthetic. Epidural catheter was not removed for 24 hours for postoperative pain management.
RESULTSDemographics and risk factors of patients are seen in Table 1.
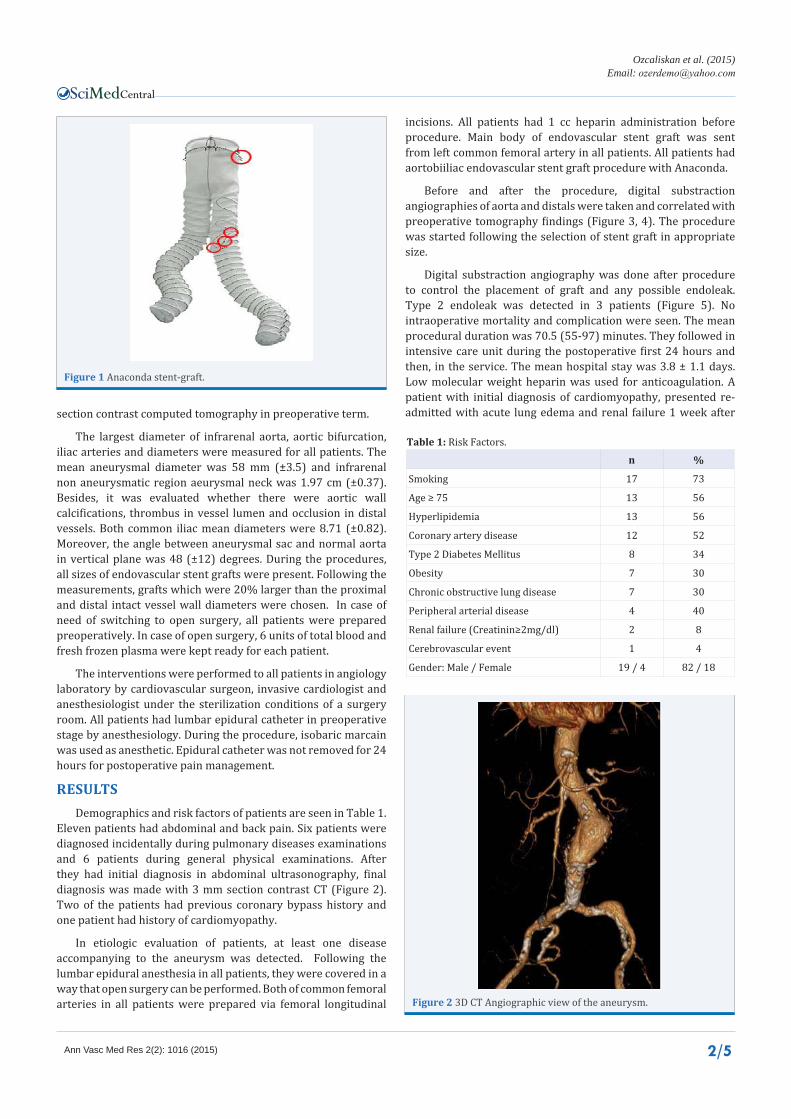
Eleven patients had abdominal and back pain. Six patients were diagnosed incidentally during pulmonary diseases examinations and 6 patients during general physical examinations. After they had initial diagnosis in abdominal ultrasonography, final diagnosis was made with 3 mm section contrast CT (Figure 2). Two of the patients had previous coronary bypass history and one patient had history of cardiomyopathy.
In etiologic evaluation of patients, at least one disease accompanying to the aneurysm was detected. Following the lumbar epidural anesthesia in all patients, they were covered in a way that open surgery can be performed. Both of common femoral arteries in all patients were prepared via femoral longitudinal
incisions. All patients had 1 cc heparin administration before procedure. Main body of endovascular stent graft was sent from left common femoral artery in all patients. All patients had aortobiiliac endovascular stent graft procedure with Anaconda.
Before and after the procedure, digital substraction angiographies of aorta and distals were taken and correlated with preoperative tomography findings (Figure 3, 4). The procedure was started following the selection of stent graft in appropriate size.
Digital substraction angiography was done after procedure to control the placement of graft and any possible endoleak. Type 2 endoleak was detected in 3 patients (Figure 5). No intraoperative mortality and complication were seen. The mean procedural duration was 70.5 (55-97) minutes. They followed in intensive care unit during the postoperative first 24 hours and then, in the service. The mean hospital stay was 3.8 ± 1.1 days. Low molecular weight heparin was used for anticoagulation. A patient with initial diagnosis of cardiomyopathy, presented re-admitted with acute lung edema and renal failure 1 week after
Figure 1 Anaconda stent-graft.
Figure 2 3D CT Angiographic view of the aneurysm.
n %
Smoking 17 73
Age ≥ 75 13 56
Hyperlipidemia 13 56
Coronary artery disease 12 52
Type 2 Diabetes Mellitus 8 34
Obesity 7 30
Chronic obstructive lung disease 7 30
Peripheral arterial disease 4 40
Renal failure (Creatinin≥2mg/dl) 2 8
Cerebrovascular event 1 4
Gender: Male / Female 19 / 4 82 / 18
Table 1: Risk Factors.

Central
Ozcaliskan et al. (2015)Email:
Ann Vasc Med Res 2(2): 1016 (2015) 3/5
annually in the world due to abdominal aortic aneurysm [7].
Although the treatment indications of abdominal aortic aneurysms are variable, those 5.5 cm in diameter, 0.5 cm enlargement of aneurysm in 6 month- follow up and being symptomatic (abdominal and back pain) point out the need of intervention to aneurysm [8].
The gold standard for abdominal aortic aneurysms is still CT angiography. While aneurysmal diameter and level are measured clearly, it is also the most sensitive method for the presence of thrombus in aneurysm and measurement of real lumen. Three digit- images can be obtained with CT angiography. Besides, magnetic resonance angiography can also be used especially in preoperative stage [9]. For selection of the cases suitable for endovascular intervention; the diameter of aneurysm, the presence of sufficient non aneurysmatic normal aortic tissue in proximal infrarenal, the angle of aneurysm in vertical plane, iliac and femoral arteries diameter, the presence of accessory renal artery should be considered. Intervention is recommended for the cases in which aneurysmal diameter is 5.5 cm, and smaller aneurysms requires follow-up and consideration of presence of symptoms [10]. Infrarenal non aneurysmal aortic tissue should be at least 15 mm in length for graft proximal implantation [11]. The
Figure 3 Angiography of aorta and distals before the procedure.
Figure 4 Angiography of aorta and distals after the procedure.
Figure 5 Angiographic view of Type 2 Endoleak.
Figure 6 Postoperative CT angiography on control visit.
the discharge. Control tomography showed no issues related to graft. However, he died due to low cardiac output and coexisting multi organ failure. Remaining patients had first, third and sixth month controls. All patients were evaluated with abdominal CT (Figure 6). No graft migration or endo leak was detected.
DISCUSSIONTo define aortic aneurysms, it is sufficient to measure over
50% of normal aortic diameter to diagnose aneurysm [6]. Treatment of abdominal aortic aneurysms can be classified as medical, surgical and endovascular methods. Although 40-80% of abdominal aortic aneurysms are treated via endovascular stent, surgical treatment is still the gold standard. Endovascular treatment is still performed in approximately 50000 people

Central
Ozcaliskan et al. (2015)Email:
Ann Vasc Med Res 2(2): 1016 (2015) 4/5
graft implantation is hard when the angle between aneurysmal sac and aorta in vertical plane is over 60 degrees [11,12]. In the cases which aneurysms approach to iliac arteries, occlusion with internal iliac artery embolization is recommended to prevent endoleak. Femoral artery diameters require being minimally 8 mm to perform the procedure in good conditions [13]. Moreover, the existence of accessory renal artery should be determined. Accessory renal artery can be seen 30% in community. In this situation, post procedural partial renal infarct may be seen [12]. In cases that inferior mesenteric artery is in aneurysmal sac; there is no harm in occlusion of artery with graft. However, in the presence of superior mesenteric artery narrowness, endo graft implantation is contraindicated [11].
Preoperative mortality of open surgery in abdominal aortic aneurysms changes between 5-20% in different series [7]. Mortality rates increase with risk factors, aneurysmal rupture, renal and liver failure, cardiopulmonary disease. Endovascular stent treatment is preferred especially in high risk group. Open surgical treatment is still preferred especially in young patients [8]. The reason for endovascular stent treatment not being preferred in young patients is that the long term outcomes are not known yet. In our patient group, they were selected from the patients with older age group as an additional risk factor as seen in Table 1. In studies with risk groups, there was significant dominance of endovascular treatment compared to open surgery [9,10]. Based on DREAM and EVAR 1 studies, it was mentioned that the endovascular treatment is less invasive [11,12]. In both studies, the surgery duration, transfusion need, intensive care unit stay duration was les compared to the patients who had open surgery [13]. Mid- term findings of these two studies were shown no difference than open surgery.
Patient follow-ups are performed with ultrasonography and CT angiography. After postoperative 1, 6, and 12 month- follow-ups, annual controls are recommended [13]. We followed this protocol for our patients. Especially for the follow-up of endoleak or device migration, the most appropriate method is CT angiography. Angiography is only recommended in specific cases. In suspicion of endoleak, angiography should be done for documentation and detection of endoleak location. CT angiography was sufficient in our all follow-ups.
Despite of its all advantages, endovascular graft implantation has its own complications. Due to surgical procedure; interventional failure, distal embolization, aortic dissection, aneurysmal rupture, iliac or femoral artery damage, pseudoaneurysm, hematoma in the area and infection may be seen. Besides, postprocedural endoleak, aneurysmal enlargement, stent graft infection, graft leg obstruction and internal iliac artery closure may also be seen [14]. The most common complication of endovascular treatment is endoleak,
it is seen 10-50 % in different series [15]. Type 1 and 3 leaks are serious which cause the direct perfusion of aneurysmal sac and certainly require intervention. In general, type 1 leaks are seen 10%, in distal or proximal communication area when there is a size incompatibility between aneurysmal neck and graft. The most common method in treatment is additional stent graft use [16]. Type 2 which is the most common leak, are seen 25%. They generally occur due to back- flow. Most of them are thrombosed spontaneously without the need of intervention. Limited number of cases is shown with aneurysmal development in literature. Type 3 leaks are mostly related to the manufacturing errors in graft. They certainly should be intervened. Type 4 also includes the leaks from graft pores related to manufacturing, they generally close spontaneously. In our patient group, we saw type 2 endoleak in 3 patients. One spontaneously closed at 3rd month and the others in 6th month.
Post implantation syndrome is an acute inflammatory picture immediately after stent placement [17,18]. It is mostly seen within first 10 days following implantation. Fever, leukocytosis, increase in C-reactive protein, endotoxin and interleukin 6 are seen [19,20]. Etiology does not involve the infection. No patient in our series presented with this picture.
There are still long series studies such as EVAR, DREAM and OVER TRIAL about the significant dominance of endovascular stent treatment over open surgery [21-23]. Endovascular stent grafts are applied to increasing number of patients with the operative mortality and early and mid-term outcomes.
CONCLUSIONSEndovascular treatment is still successfully performed
in cases whose open surgery has high risks [21]. A good preoperative preparation and an experienced cardiovascular surgery and anesthesiology team are required. However, when the long term outcomes will be available, it will be possible to use the procedure also in young patients more safely.
REFERENCES1. Çil BE, Canyigit M, Çiftçi TT, Peynircioglu B, Hazirolan T, Pamuk AG,
et al. Endovascular treatment of aortic lesions using the Medtronic Talent system: single center experience with mid-term follow-up. Anadolu Kardiyol Derg. 2008; 8: 134-138.
2. Ouriel K, Clair DG, Greenberg RK, Lyden SP, O’Hara PJ, Sarac TP, et al. Endovascular repair of abdominal aortic aneurysms: device-specific outcome. J Vasc Surg. 2003; 37: 991-998.
3. Carpenter JP, Baum RA, Barker CF, Golden MA, Velazquez OC, Mitchell ME, et al. Durability of benefits of endovascular versus conventional abdominal aortic aneurysm repair. J Vasc Surg. 2002; 35: 222-228.
4. Buth J, Laheij RJ. Early complications and endoleaks after endovascular abdominal aortic aneurysm repair: report of a multicenter study. J Vasc Surg. 2000; 31: 134-146.
5. White GH, Yu W, May J, Chaufour X, Stephen MS. Endoleak as a complication of endoluminal grafting of abdominal aortic aneurysms: classification, incidence, diagnosis, and management. J Endovasc Surg 1997; 4: 152-168.
6. Johnston KW, Rutherford RB, Tilson MD, Shah DM, Hollier L, Stanley JC. Suggested standards for reporting on arterial aneurysms. Subcommittee on Reporting Standards for Arterial Aneurysms, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery
Mean
Aneurysm diameter 58 ± 3.5cm
Infrarenal non-aneurysmatic segment diameter 1.97 ± 0.37cm
Common femoral artery diameter 8.7 ± 0.82cm
Vertical angle of aneurysm 48 ± 12 degree
Table 2: Measurements with CT Angiography.

Central
Ozcaliskan et al. (2015)Email:
Ann Vasc Med Res 2(2): 1016 (2015) 5/5
Erdogan MB, Zor H, Ozcaliskan O, Erdogmus O (2015) Anaconda Experiment in Endovascular Stent Therapy of Abdominal Aortic Aneurysms: Early Results of a Single Center. Ann Vasc Med Res 2(2): 1016.
Cite this article
and North American Chapter, International Society for Cardiovascular Surgery. J Vasc Surg. 1991; 13: 452.
7. Therasse E, Soulez G, Giroux MF, Perreault P, Bouchard L, Blair JF, et al. Stent-graft placement for the treatment of thoracic aortic diseases. Radiographics. 2005; 25: 157-173.
8. Santilli SM, Littooy FN, Cambria RA, Rapp JH, Tretinyak AS, d’Audiffret AC, et al. Expansion rates and outcomes for the 3.0-cm to the 3.9-cm infrarenal abdominal aortic aneurysm. J Vasc Surg. 2002; 35: 666-671.
9. Palmaz JC. Review of polymeric graft materials for endovascular applications. J Vasc Interv Radiol. 1998; 9: 7-13.
10. Rozenblit A, Rozenblit G, Meddineni S. The role of helical CT-angiography in endovascular grafting procedures. In: Endovascular Grafting Techniques, Parodi, JC, Veith, F, Marin, M (Eds), Williams and Wilkins, Philadelphia 1999; 15.
11. Mohan IV, Laheij RJ, Harris PL. Eurostar Collaborators. Risk factors for endoleak and the evidence for stent-graft oversizing in patients undergoing endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2001; 21: 344-349.
12. Peppelenbosch N, Buth J, Harris PL, van Marrewijk C, Fransen G. EUROSTAR Collaborators. Diameter of abdominal aortic aneurysm and outcome of endovascular aneurysm repair: does size matter? A report from EUROSTAR. J Vasc Surg. 2004; 39: 288-297.
13. Abu-Ghaida AM, Clair DG, Greenberg RK, Srivastava S, O’hara PJ, Ouriel K. Broadening the applicability of endovascular aneurysm repair: the use of iliac conduits. J Vasc Surg. 2002; 36: 111-117.
14. Chaikof EL, Blankensteijn JD, Harris PL, White GH, Zarins CK, Bernhard VM, et al. Reporting standards for endovascular aortic aneurysm repair. J Vasc Surg. 2002; 35: 1048-1060.
15. Golzarian J, Maes EB, Sun S. Endoleak: treatment options. Tech Vasc Interv Radiol. 2005; 8: 41-49.
16. Powell JT, Greenhalgh RM. Clinical practice. Small abdominal aortic aneurysms. N Engl J Med. 2003; 348: 1895-1901.
17. Blum U, Voshage G, Lammer J, Beyersdorf F, Töllner D, Kretschmer G, et al. Endoluminal stent-grafts for infrarenal abdominal aortic aneurysms. N Engl J Med. 1997; 336: 13-20.
18. Velázquez OC, Carpenter JP, Baum RA, Barker CF, Golden M, Criado F, et al. Perigraft air, fever, and leukocytosis after endovascular repair of abdominal aortic aneurysms. Am J Surg. 1999; 178: 185-189.
19. Bölke E, Jehle PM, Storck M, Braun C, Schams S, Steinbach G, et al. Endovascular stent-graft placement versus conventional open surgery in infrarenal aortic aneurysm: a prospective study on acute phase response and clinical outcome. Clin Chim Acta. 2001; 314: 203.
20. Odegård A, Lundbom J, Myhre HO, Hatlinghus S, Bergh K, Waage A, et al. The inflammatory response following treatment of abdominal aortic aneurysms: a comparison between open surgery and endovascular repair. Eur J Vasc Endovasc Surg. 2000; 19: 536-544.
21. EVAR trial participants. Endovascular aneurysm repair and outcome in patients unfit for open repair of abdominal aortic aneurysm (EVAR trial 2): randomised controlled trial. Lancet. 2005; 365: 2187-2192.
22. United Kingdom EVAR Trial Investigators, Greenhalgh RM, Brown LC, Powell JT, Thompson SG, Epstein D. Endovascular repair of aortic aneurysm in patients physically ineligible for open repair. N Engl J Med. 2010; 362: 1872-1880.
23. Gouëffic Y, Becquemin JP, Desgranges P, Kobeiter H. Midterm survival after endovascular versus open repair of infrarenal aortic aneurysms. J Endovasc Ther. 2005; 12: 47-57.