An Update in Geriatric Medicine - British Society of ... · PDF fileAn Update in Geriatric...
27
An Update in Geriatric Medicine Dr Cathryn Mainwaring BMedSci BM BS MRCP(UK) ST4 in Geriatrics Kings College Hospital NHS Foundation Trust
-
Upload
phunghuong -
Category
Documents
-
view
218 -
download
2
Transcript of An Update in Geriatric Medicine - British Society of ... · PDF fileAn Update in Geriatric...

An Update in Geriatric Medicine
Dr Cathryn Mainwaring BMedSci BM BS MRCP(UK)
ST4 in Geriatrics Kings College Hospital NHS Foundation Trust

A little bit about me…


Aims
1) Present a case of recurrent aspiration pneumonia
1) Examine the literature on aspiration pneumonia
1) Use this as a springboard to discuss pertinent issues such as DNACPRs and Advanced Care Planning

JE 79 year old male. Admitted 23/12/2015 PC - Fall HPC - Walking in bedroom - Slipped and fell - Hit his head - Lie approximately 1 hour - Feeling generally weak - Reports dizziness and swallowing
difficulties
PMHx - Pulmonary Embolism - Paroxysmal Atrial Fibrillation - Stroke - Castleman’s Disease - Chronic Inflammatory Demyelinating
Polyneuropathy
DHx - Senna, laxido, sodium docusate - Solifenacin - Vitamin B co-strong - Irbesartan - Omeprazole - Paracetamol - Warfarin - Ferrous fumarate - Adcal D3 - Alendronic Acid - Prednisolone
SHx - Mobile with stick - Wheelchair for outdoor use - Lives in residential home - Assistance with personal care - Known to community SALT team - Cognitively good; AMT 7/10

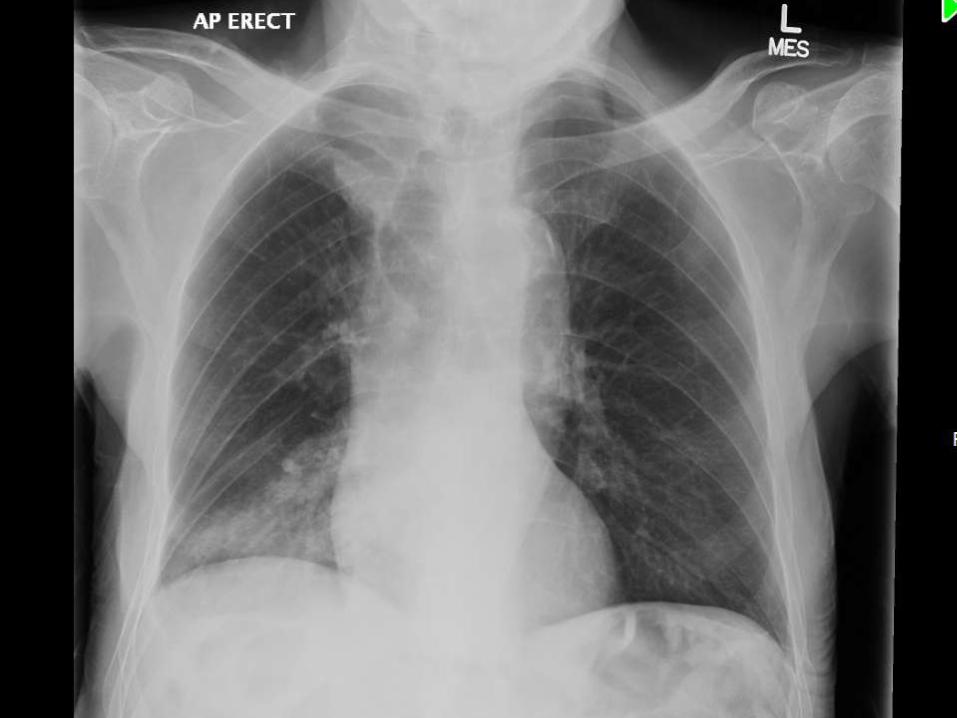
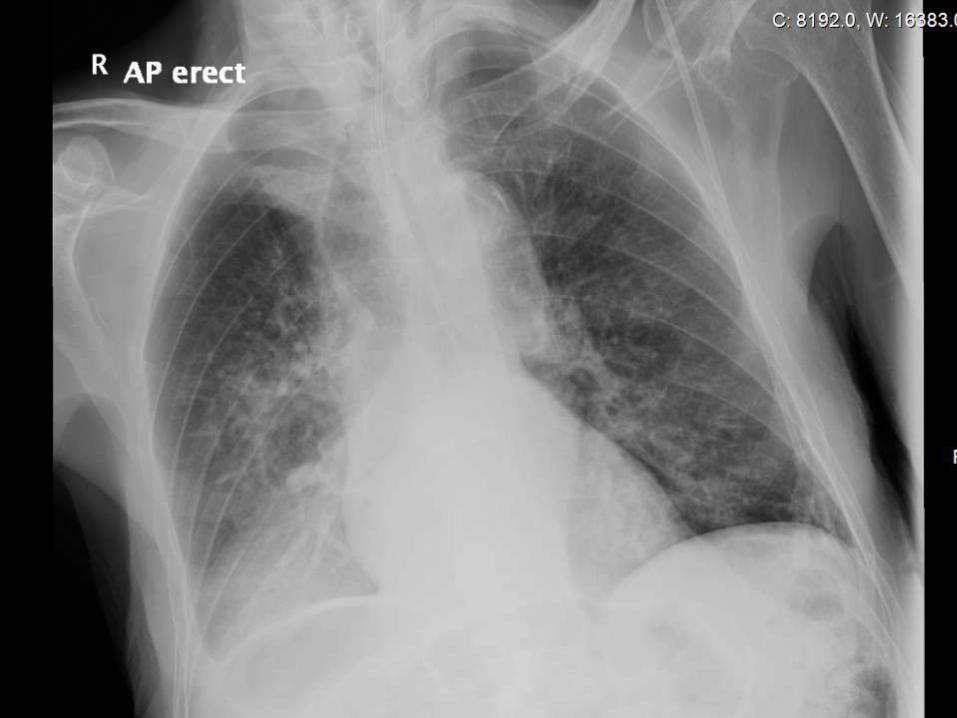
O/E - Frail - Distal weakness and wasting - Crackles at right lung base Ix - Bloods unremarkable - CT head; no intracranial haemorrhage, small vessel disease IMP - Fall secondary to postural hypotension and neuromuscular weakness - Oropharyngeal Dysphagia; likely decompensated old stroke Plan - Postural blood pressure - ECG - Physiotherapy - Dietician review - CXR - DNACPR discussed with patient - SALT Assessment Mild to moderate oropharnygeal dysphagia Stage 1 fluids and soft moist diet


Could this have been predicted?
Was there anything that could have been done to prevent this man’s recurrent aspiration?
How could communication between all the stake holder’s in this gentleman’s care have been
improved?
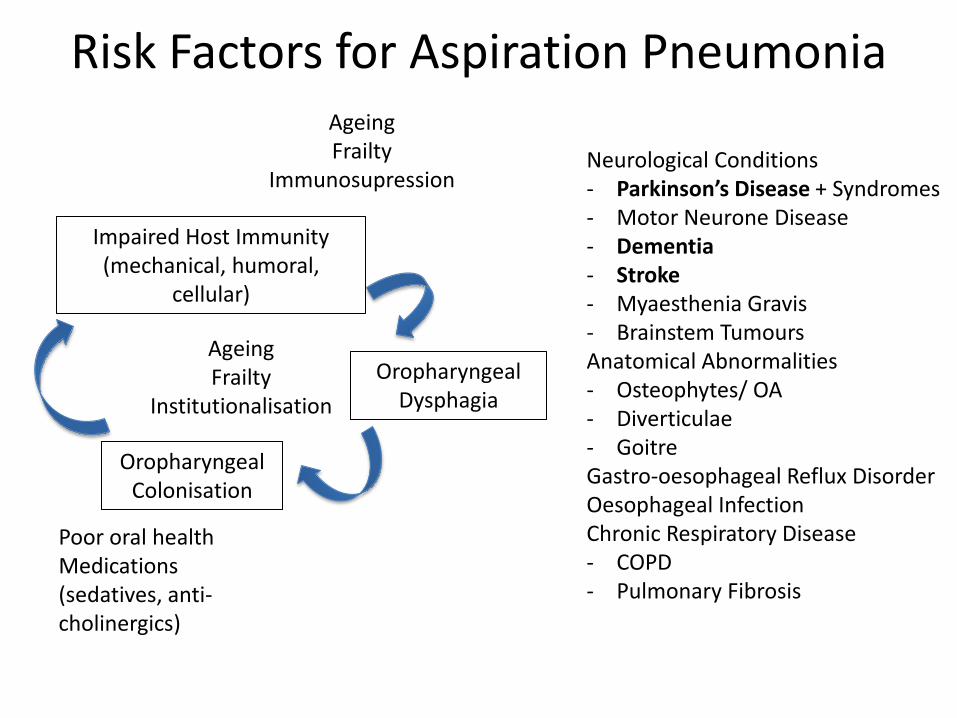
Risk Factors for Aspiration Pneumonia
Oropharyngeal Colonisation
Oropharyngeal Dysphagia
Impaired Host Immunity (mechanical, humoral,
cellular)
Neurological Conditions - Parkinson’s Disease + Syndromes - Motor Neurone Disease - Dementia - Stroke - Myaesthenia Gravis - Brainstem Tumours Anatomical Abnormalities - Osteophytes/ OA - Diverticulae - Goitre Gastro-oesophageal Reflux Disorder Oesophageal Infection Chronic Respiratory Disease - COPD - Pulmonary Fibrosis
Poor oral health Medications (sedatives, anti-cholinergics)
Ageing Frailty
Immunosupression
Ageing Frailty
Institutionalisation
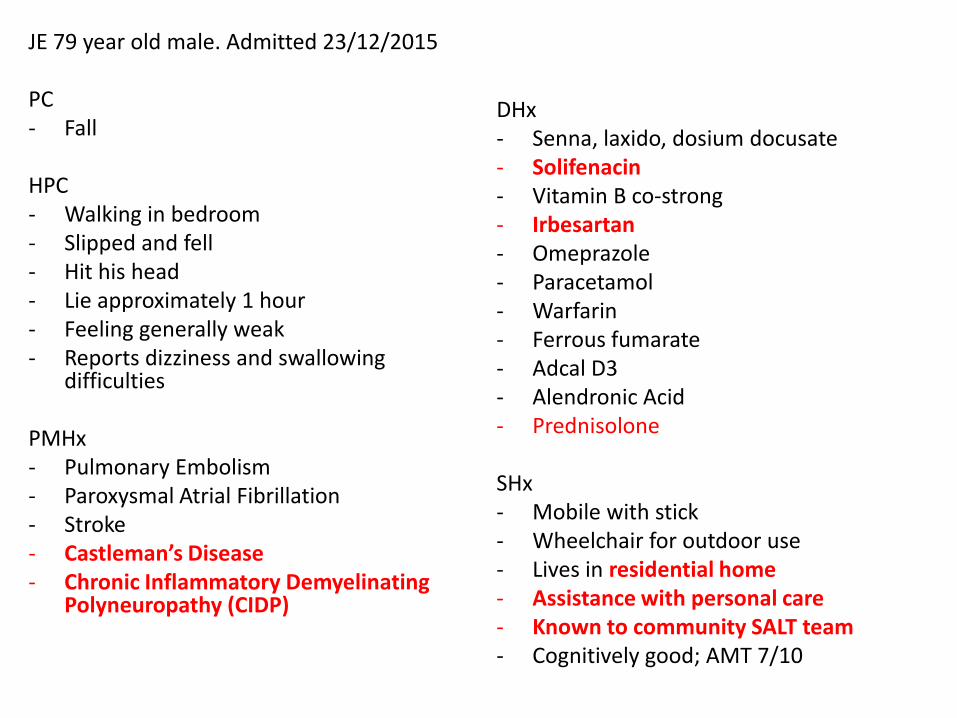
JE 79 year old male. Admitted 23/12/2015 PC - Fall HPC - Walking in bedroom - Slipped and fell - Hit his head - Lie approximately 1 hour - Feeling generally weak - Reports dizziness and swallowing
difficulties
PMHx - Pulmonary Embolism - Paroxysmal Atrial Fibrillation - Stroke - Castleman’s Disease - Chronic Inflammatory Demyelinating
Polyneuropathy (CIDP)
DHx - Senna, laxido, dosium docusate - Solifenacin - Vitamin B co-strong - Irbesartan - Omeprazole - Paracetamol - Warfarin - Ferrous fumarate - Adcal D3 - Alendronic Acid - Prednisolone
SHx - Mobile with stick - Wheelchair for outdoor use - Lives in residential home - Assistance with personal care - Known to community SALT team - Cognitively good; AMT 7/10

Prevention of Aspiration Pneumonia
? Pharmacological
Amantadine
Cilostazol
ACE inhibitors
? Dietary Modification
? Positioning
? Oral Care
Chlorhexidine
? Tube Feeding

Treatment of Aspiration Pneumonia
Antibiotics, Oxygen, Nil By Mouth, ?Palliative Care

DNACPRs

Decisions relating to cardiopulmonary resuscitation - new statement 2015 The British Medical Association, Resuscitation Council (UK) and Royal College of Nursing note the judgment in the High Court in the case of Winspear v City Hospitals Sunderland NHS Foundation Trust [2015] EWHC 3250 (QB). The wording of the guidance in Decisions relating to cardiopulmonary resuscitation is under review. We will make any necessary changes to ensure that it is compliant with this most recent decision. For the present, we wish to emphasise the following points for attention when health professionals consider making an anticipatory decision about CPR for a person who does not have capacity to participate in the decision-making process: In order to make a fully informed decision, where it is both practicable and appropriate, they must discuss the patient’s situation and the decision with those close to the patient (subject to any confidentiality restrictions expressed if, and when, the patient had capacity). Where both practicable and appropriate, they should not delay contacting those close to the patient in order to do this. Of note, in the recent judgment it was stated by the judge that “a telephone call at 3.00 am may be less than convenient or desirable than a meeting in working hours, but that is not the same as whether it is practicable”. When it is not possible to contact those close to the patient immediately and an anticipatory decision about CPR is needed in order to deliver high-quality care, that decision should be made in accordance with the relevant legislation.

DNACPRs in the context of surgery…
Is anaesthesia and surgery appropriate?
If surgery is appropriate;
- Is the patient medically optimised?
- What resuscitation measures are appropriate?
1) Discontinuation
2) Modification
3) Laissez Faire

“Message in a Bottle”


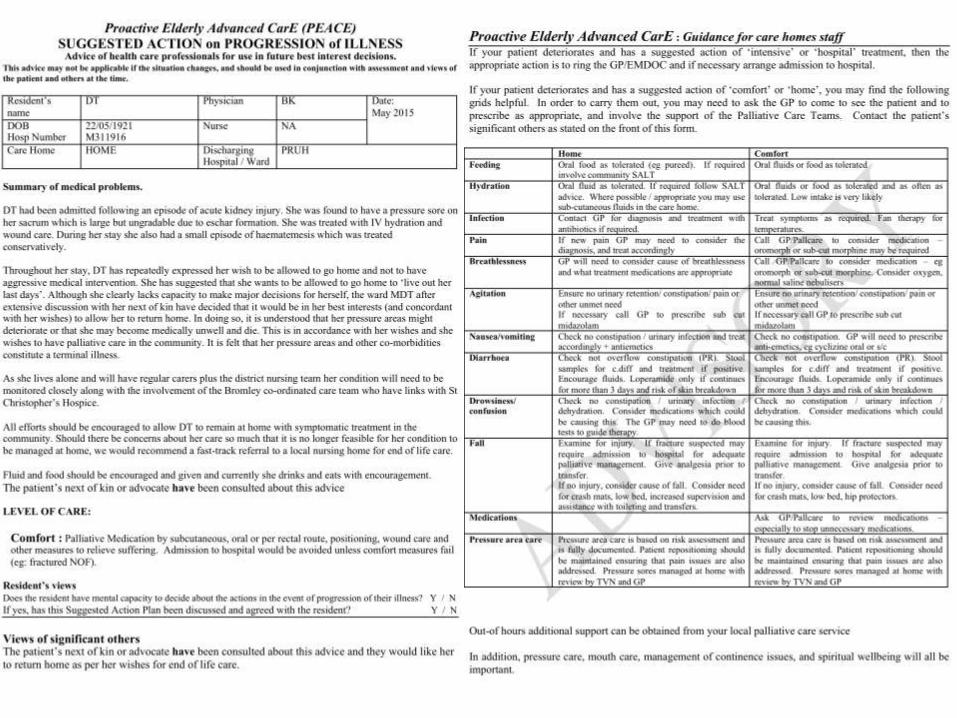
Advanced Care Planning
“formal decision making to establish decisions about future care that take effect when a patient loses capacity”
Electronic urgent care plan record
Bridging the communication gap between hospital and community services
Diagnoses, Key Contacts, Allergies, Resuscitation status, Wishes & Preferences
Ambulance control staff, 111, GPs, OOH GP, Hospitals, Care homes, Community nurses,
Hospices

Bromley Care Coordination

In Summary
There are a number of factors that increase the risk of aspiration pneumonia. Various approaches to reduce this risk have been proposed, but the quality of evidence is low. A multi-factorial approach to this problem is likely to be beneficial, including the use of ACE-inhibitors DNACPRs; communication is key. Advanced care planning may be a useful tool to plan the care of those at high risk of recurrent aspiration pneumonia. Advanced care plans should be shared with all stakeholders. PEACE documents or electronic records may help.

Any Questions?
References Aspiration Pneumonia Loeb, M.B., Becker, M., Eady, A. and Walker‐Dilks, C., 2003. Interventions to prevent aspiration pneumonia in older adults: a systematic review. Journal of the American Geriatrics Society, 51(7), pp.1018-1022. Marik, P.E. and Kaplan, D., 2003. Aspiration pneumonia and dysphagia in the elderly. CHEST Journal, 124(1), pp.328-336. Ortega, O., Parra, C., Zarcero, S., Nart, J., Sakwinska, O. and Clavé, P., 2014. Oral health in older patients with oropharyngeal dysphagia. Age and ageing, 43(1), pp.132-137. Marik, P.E., 2001. Aspiration pneumonitis and aspiration pneumonia. New England Journal of Medicine, 344(9), pp.665-671. Manabe, T., Teramoto, S., Tamiya, N., Okochi, J. and Hizawa, N., 2015. Risk Factors for Aspiration Pneumonia in Older Adults. PloS one, 10(10), p.e0140060. Ward, K.T., Nam, S. and Cook, E.A., 2015. Aspiration Pneumonia in the Geriatric Population. Current Geriatrics Reports, 4(2), pp. 202-209. Caldeira, D., Alarcão, J., Vaz-Carneiro, A. and Costa, J., 2012. Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: systematic review and meta-analysis. Sharif-Abdullah, S.S., Chong, M.C., Surindar-Kaur, S.S., Kamaruzzaman, S.B. and Ng, K.H., 2016. The effect of chlorhexidine in reducing oral colonisation in geriatric patients: a randomised controlled trial. Singapore medical journal, 57(5), pp.262-266. Cabre, M., Serra-Prat, M., Palomera, E., Almirall, J., Pallares, R. and Clavé, P., 2010. Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age and ageing, 39(1), pp.39-45. Clinical, P. and Models of Care Committee, 2014. American Geriatrics Society feeding tubes in advanced dementia position statement. Journal of the American Geriatrics Society, 62(8), p.1590. NICE Guidance. 2006. Dementia: Supporting people with dementia and their carers in health and social care (CG 42) NICE Guidance. 2006. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition (CG32) DNACPR British Medical Assiociation & The Resuscitation Council (UK) & the Royal College of Nursing2014. Decisions relating to cardiopulmonary resuscitation Association of Anaesthetists of Great Britain and Ireland. 2009. DNAR decisions in the perioperative period. Advanced Care Planning Mullick, A., Martin, J. and Sallnow, L., 2013. An introduction to advance care planning in practice. BMJ, 347(f6064), pp.1-12. Hayes, N., Kalsi, T., Steves, C., Martin, F., Evans, J., Schiff, R. and Briant, L., 2011. Advance Care Planning (PEACE) for care home residents in an acute hospital setting: impact on ongoing advance care planning and readmissions. BMJ supportive & palliative care, 1(1), pp.99-99. Message in a bottle http://www.lions105ea.com/specialist_officer/miab.html Coordinate my care http://coordinatemycare.co.uk