
An unusual cause for Persistent Pneumoniaold.criticalcare.org.za/images/presentations/Dr...
28
An unusual cause for Persistent Pneumonia Dr Visva Naidoo Paediatric Pulmonology Fellow Department of Paediatrics, UKZN
Transcript of An unusual cause for Persistent Pneumoniaold.criticalcare.org.za/images/presentations/Dr...
An unusual cause for Persistent Pneumonia
Dr Visva Naidoo
Paediatric Pulmonology Fellow
Department of Paediatrics, UKZN
Case presentation
• 3 year old male with a persistent / non resolving multilobar left sided pneumonia despite stepwise escalation of antimicrobial cover
• Initial presentation : Cough, fever, loss of appetite and weight for one month
• No prior illnesses requiring admission
• No TB contact
• HIV negative

Examination
• Wasted but not stunted
• Non-Toxic, Chronically ill
• Generalised lymphadenopathy
• Early digital clubbing
• Saturations 99% in room air
• Chest : moderate respiratory distress, RR 40,
volume loss on left
signs of left sided consolidation
• CVS : no pulmonary hypertension
• Abdomen : hepatomegaly 2cm, spleen nil
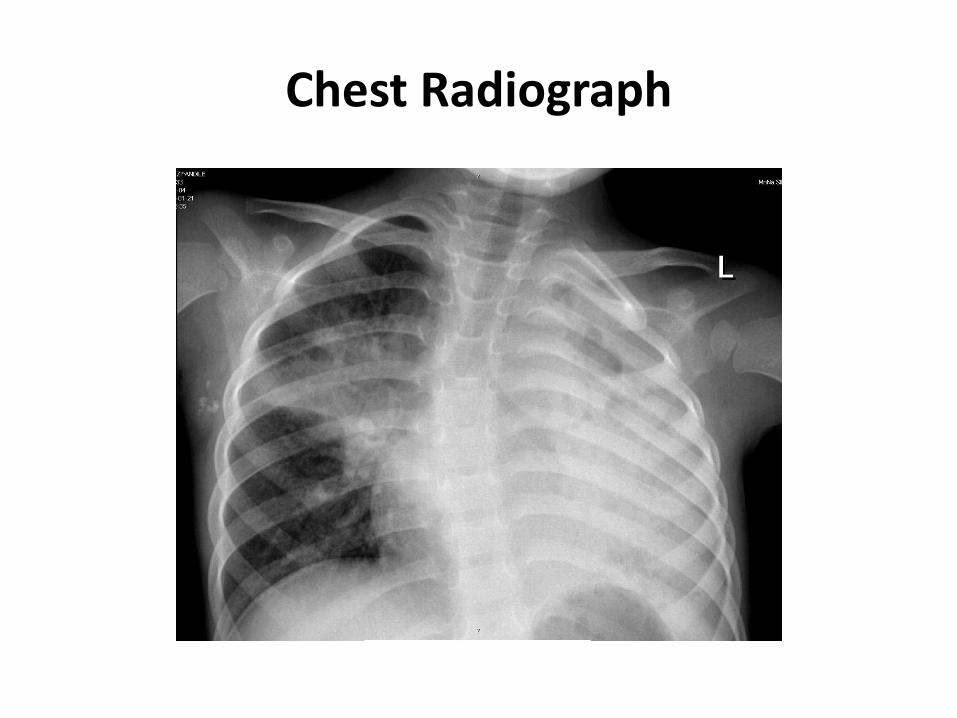
Chest Radiograph

Chest Radiograph
Approach to problem
HOST FACTORS
• Immunity
• Lung defense mechanisms
• Anatomical abnormalities
- lung
- airway – extrinsic intrinsic
• Aspiration
• Allergic lung diseases
• Non-infectious diseases
PATHOGENS
• Bacterial
• TB / NTM
• Fungal
• Atypical
ENVIRONMENTAL

Persistent pneumonia
• Untreated infection
• Unresolved infection
• Complicated infection – abscess / empyema
• Sanctuary infection
• Tuberculosis / atypical / fungal

Investigations
HOST
• HIV ELISA negative
• Contrast swallow normal
• CT Chest : consolidation,
no foreign body,
no structural disease
• Bronchoscopy normal
PATHOGEN
• Elevated WCC with neutrophillia
• Elevated acute phase reactants
• ESR 108
• TST negative
• Sputums MCS / TB / Fungi negative
• BAL negative

Initial Therapy
• Ciprofloxacin / Amikacin
• 4 drug anti-Tuberculous therapy
• Fluconazole
• Chest physiotherapy
• Nutritional support
Progress
• Remained apyrexial with persistent respiratory signs of mild-moderate distress
• TB treatment continued
• 3 weeks later – developed fever, generalised lymphadenopathy – 0.5- 1.0 cm and a fluctuant parasternal mass with surrounding crepitus.
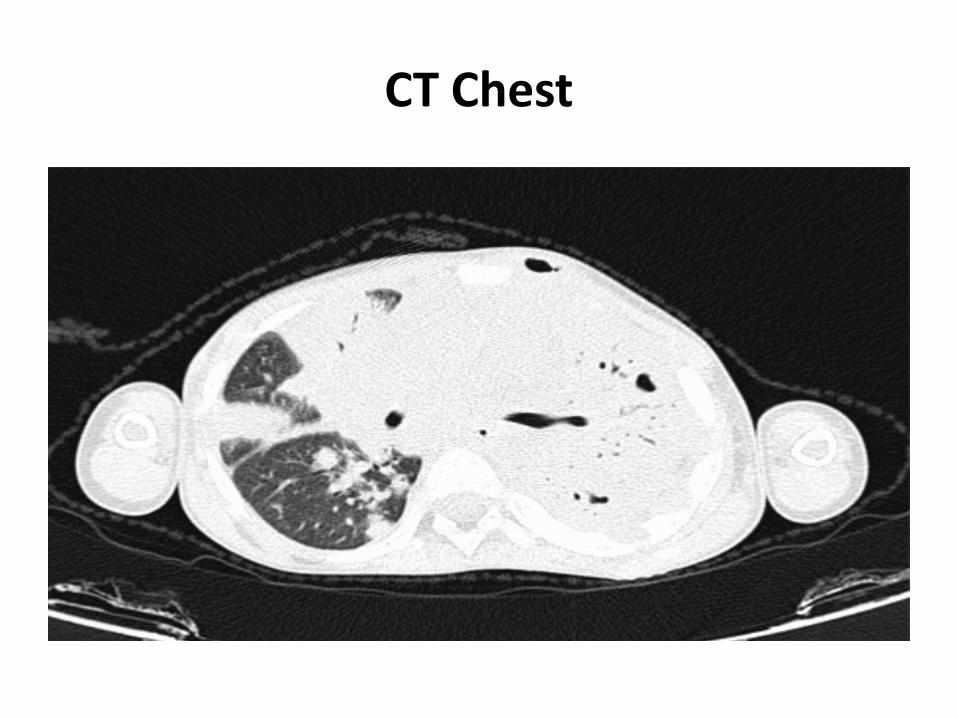
CT Chest

CT Chest

Bone scan
Diffuse increased uptake in the left posterolateral chest wall, which is likely to suggest extension into soft tissue
Persistent pneumonia with soft tissue extension & lymphadenopathy
• Differential ???
• Fungal histoplasmosis
• MDR TB
• NTM
• Staphylococcal
• Empiric treatment with Fluconazole MDR TB therapy, Vancomycin
Further investigations
• Serial CRP, ESR remained elevated
• Beta – Glycans 73 (normal < 60)
• Fine needle aspirate of sternal mass
• Bone Marrow Aspirate and Trephine
• Fine needle aspirate of Lymph Node
• Transthoracic Lung Aspirate
Pus cells, AFB negative, no fungal elements,
no organisms, no growth

Deterioration
Deterioration
• Further respiratory deterioration requiring supportive ventilation
• 4cm Right sided cervical mass – yielded 4 mls thick, non-offensive, green pus
• Axillary lymph node abscess
• Differential ??? – chronic illness with persistent / non resolving pneumonia / abscesses / soft tissue involvement
Diagnosis
• Abscess Fluid Aspirate / Endotracheal aspirate
Streptomyces / Nocardia
• No CNS dissemination – CT brain normal
• Commenced on high dose Co-Trimoxazole and Amikacin
• Worsening lung picture – escalated support

Diagnosis
Pulmonary Nocardiosis
Nocardia Pseudobrasiliensis
Sensitive
Cotrimoxazole
Amikacin
Meropenem
Ciprofloxacin
Linezolid
Nocardiosis
• Rare opportunistic infection that affects patients with deficient cell mediated immunity
• In immunocompetent hosts chronic infection
• Ubiquitous - soil and decaying vegetable matter
• Emerging disease due to transplant surgery and HIV
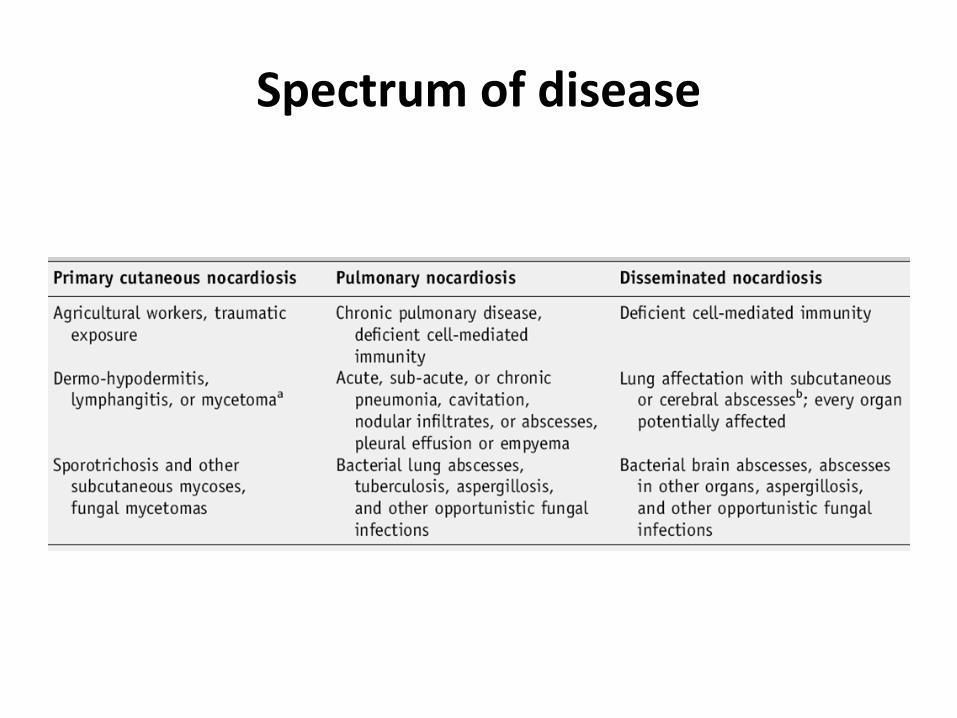
Spectrum of disease
Pulmonary Nocardiosis
• Acute / Subacute / Chronic
• Respiratory tract portal of entry in 50-70% of cases
• Similar clinical picture to TB – delay in diagnosis
• More frequently encountered in those with structural lung disease
• Clinical features - Weight loss, persistent cough, low grade fever, dyspnea, night sweats, fatigue, anorexia, hemoptysis, and pleuritic chest pain
• Imaging - lobar infiltrates, abscesses, cavities, pleural effusions, pulmonary nodules
When to suspect Nocardia ??
• Immunocompromised
• Structural Lung Disease
• Acute / Subacute / Chronic pneumonia
• - not responding to standard therapy
• Skin and Soft Tissue Abscesses / Brain abscess
• Chest X-ray : confluent pneumonia, cavitation, pleural and chest wall involvement
• ability to disseminate to virtually any organ, and its tendency to relapse or progress despite appropriate therapy.
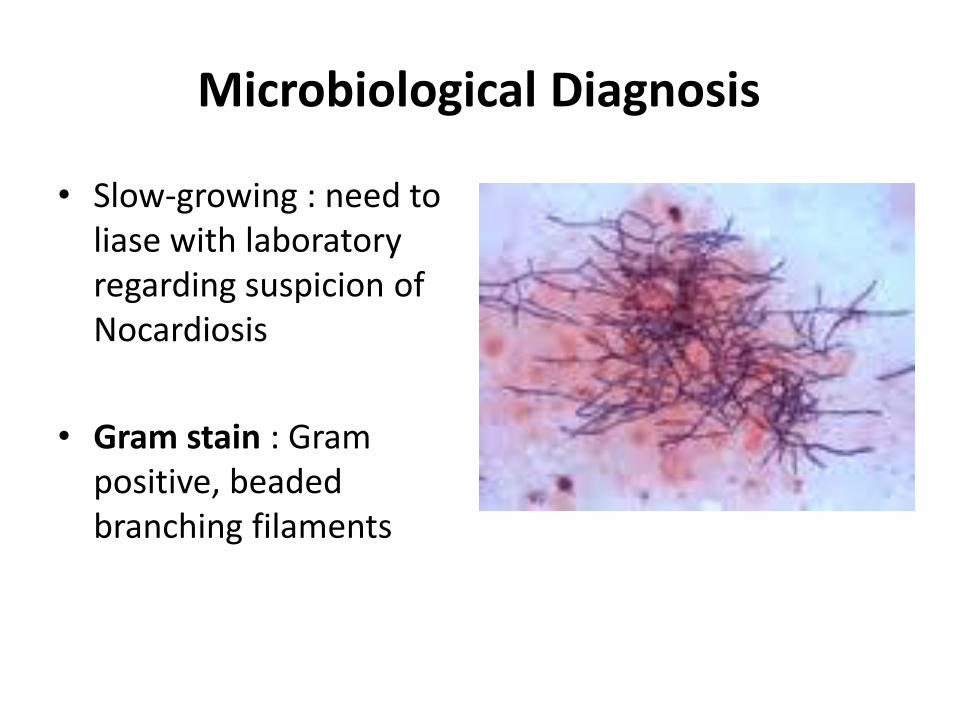
Microbiological Diagnosis
• Slow-growing : need to liase with laboratory regarding suspicion of Nocardiosis
• Gram stain : Gram positive, beaded branching filaments
Diagnosis
• Modified acid fast stains• Blood & Chocolate Agar / Selective media• Plates are incubated in air at 370C for up to 4 weeks
• Colonies that grow – Lysosyme test -nocardias are resistant to lysosyme– Urea test– Casein hydrolysis– Tyrosine hydrolysis– Xanthine hydrolysis– PCR and 16S rRNA sequencing

Treatment
• Combination therapy / Prolonged therapy
• Sulphonamides / Co-Trimoxazole
• Severe disease / Invasive infection
• - Intravenous treatment 2-3 agents for at least six weeks or until improvement noted
• Imipenem, Amikacin, Cephalosporins, Linezolid
• Oral treatment for 6 to 12 months – co-trimoxazole, minocycline, amoxycilin/clavunate
Learning points
• Prototype of chronic pneumonia with soft tissue and/or lymph node abscesses –Nocardia is a differential
• Nocardia is slow-growing and can mimic many other conditions, therefore diagnosis is difficult
• Good outcomes require prompt therapy, prolonged courses and combination therapy

References
1. Pediatric Nocardiosis Barbara J. Law and Melvin I. Marks Pediatrics 1982;70;560
2. Nocardiosis: Updated Clinical Review and Experience at a Tertiary Center J. Ambrosioni, D. Lew, J. Garbino Infection Volume 38 Number 20 89-97
3. Bacteria That Masquerade as Fungi Actinomycosis/Nocardia Donna C. Sullivan1 and Stanley W. Chapman1 Proc Am Thorac Soc Vol 7. pp 216–221, 2010
4. Nocardia brasiliensis primary pulmonary nocardiosis with subcutaneous involvement in immunocompetent patient R Amatya1, R Koirala2, B Khanal3, SS Dhakal4 Indian Journal of Medical Microbiology, Vol. 29, No. 1, January-March, 2011, pp. 68-70
5. Evaluation of Recurrent Pneumonia Howard B. Panitch The Padiatric Infectious Disease Journal Vol 24, Number 3, March 2005


















