An Unforeseeable Diagnosis in a Pregnant Woman with a ... · suspicious adnexal mass. CASE...
2
Central JSM Clinical Case Reports Cite this article: Telli E, Yalcin OT, Oge T, Kabukcuoglu S (2015) An Unforeseeable Diagnosis in a Pregnant Woman with a Suspicious Adnexal Mass. JSM Clin Case Rep 3(2): 1079. *Corresponding author Elcin Telli, Osmangazi University, School of Medicine, Department of Obstetrics and Gynecology, Eskisehir, Turkey, Tel: +905054422395; Fax: +902222392979; E-mail: Submitted: 24 October 2014 Accepted: 09 June 2015 Published: 11 June 2015 Copyright © 2015 Telli et al. OPEN ACCESS Keywords • Adnexal mass • Leiomyomatosis peritonealis disseminate • Peritoneal leiomyomatosis Case Report An Unforeseeable Diagnosis in a Pregnant Woman with a Suspicious Adnexal Mass Elcin Telli 1 *, Omer Tarık Yalcin 1 , Tufan Oge 1 , and Sare Kabukcuoglu 2 1 Department of Obstetrics and Gynecology, Osmangazi University, Turkey 2 Sare Kabukcuoglu, Department of Pathology, Osmangazi University, Turkey Abstract Hereby, we present a rare case of 22 year-old pregnant woman with a suspicious adnexal mass coexisting multiple nodules on ovary, peritoneum and omentum diagnosed as disseminated peritoneal leiomyomatosis. ABBREVIATIONS Disseminated peritoneal leiomyomatosis (DPL) INTRODUCTION Disseminated peritoneal leiomyomatosis(DPL) in the name of leiomyomatosis peritonealis disseminata is a rare disease that usually occurs in the reproductive aged women [1]. Hormonal, genetic and iatrogenic theories were defined as possible mechanisms in etiology [2]. An animal study revealed that, the influence of estrogen or both estrogen and progesterone promotes the differentiation of subcoelomic mesenchyme to smooth muscle-like and decidua-like cells and these cells were observed as subperitoneals nodules in macroscopic view [3]. Because of the prolonged elevation of estrogen and progesterone levels in pregnancy, pregnancy was suggested as a causation of DPL and this entity was identified in case reports in the literature [4,5]. Although the name of the disease connotes malignancy, it acts as benign except some cases developing malignancy [6]. Because of the rarity of disease and coexistence of DPL with other gynaecological conditions, we aimed to present a case of DPL in a pregnant woman with leiomyomatosis uteri and a suspicious adnexal mass. CASE PRESENTATION A 22 year-old pregnant woman with a complaint of persistent adnexal mass admitted to our outpatient clinic. She had no complaint in terms of abdominal swelling, abdominal pain or acute abdomen. In her history, an adnexal mass had been diagnosed at the sixth weeks of gestation and sonographic follow- up had been performed until the 13th weeks of gestation. On physical examination an enlarged uterus and a right sided adnexal mass measuring 6 centimeters in diameter were palpated. Transvaginal ultrasonography revealed, a 13 weeks aged live fetus, a heterogenous adnexal mass on the right adnexa measuring 66x38x44 millimeters in diameter and a fundal leiomyoma measuring 42x32 millimeters in diameter were revealed. The mass was suspicious of malignancy because of the morphology and the low resistance blood flow on Doppler sonography. There were no ascites in the pelvic cavity. Hemotological, biochemical and tumor marker analysis were all in normal range. Patient was advised to have magnetic resonance imaging examination but she declined and wished to learn the definite diagnosis as soon as possible. Therefore, the patient underwent a laparotomy with midline incision because of an adnexal mass that is suspicious for malignancy. During the exploration, the uterus was enlarged a size of a 14 weeks aged gestation. There were multiple of uterine nodules measuring nearly two centimeters in diameter in the biggest one. On the right ovary, 6 centimeters cyst with well surrounded multiple nodules above the cyst capsule was identified. The right pelvic peritoneum was also containing multiple nodules similar to the ones on the cyst capsule. These nodules were smooth surfaced and egg-shaped and the biggest one was measured 7 millimeters in diameter. There were no presence of free fluid in the pelvic cavity and the omentum was in normal appearance except adhesions. Peritoneal washings, a right salpingo-oophorectomy, removal of the peritoneal nodules on the right pelvic cavity and partial omentectomy were performed. On macroscopic view after removal, the cyst was containing a 3x2 centimeters in diameter solid nodule and on frozen section analysis, no malignant findings were found. On final microscopic view, there were well-defined smooth muscle nodules on peritoneum, ovary and omentum. All of the nodules were stained by desmin. The final pathology of the nodules on ovary, peritoneum and omentum revealed DPL. The cyst was diagnosed to be a folliculer cyst. The patient had an uneventful
Transcript of An Unforeseeable Diagnosis in a Pregnant Woman with a ... · suspicious adnexal mass. CASE...

Central JSM Clinical Case Reports
Cite this article: Telli E, Yalcin OT, Oge T, Kabukcuoglu S (2015) An Unforeseeable Diagnosis in a Pregnant Woman with a Suspicious Adnexal Mass. JSM Clin Case Rep 3(2): 1079.
*Corresponding authorElcin Telli, Osmangazi University, School of Medicine, Department of Obstetrics and Gynecology, Eskisehir, Turkey, Tel: +905054422395; Fax: +902222392979; E-mail:
Submitted: 24 October 2014
Accepted: 09 June 2015
Published: 11 June 2015
Copyright© 2015 Telli et al.
OPEN ACCESS
Keywords•Adnexal mass•Leiomyomatosis peritonealis disseminate•Peritoneal leiomyomatosis
Case Report
An Unforeseeable Diagnosis in a Pregnant Woman with a Suspicious Adnexal MassElcin Telli1*, Omer Tarık Yalcin1, Tufan Oge1, and Sare Kabukcuoglu2
1Department of Obstetrics and Gynecology, Osmangazi University, Turkey2Sare Kabukcuoglu, Department of Pathology, Osmangazi University, Turkey
Abstract
Hereby, we present a rare case of 22 year-old pregnant woman with a suspicious adnexal mass coexisting multiple nodules on ovary, peritoneum and omentum diagnosed as disseminated peritoneal leiomyomatosis.
ABBREVIATIONSDisseminated peritoneal leiomyomatosis (DPL)
INTRODUCTIONDisseminated peritoneal leiomyomatosis(DPL) in the
name of leiomyomatosis peritonealis disseminata is a rare disease that usually occurs in the reproductive aged women [1]. Hormonal, genetic and iatrogenic theories were defined as possible mechanisms in etiology [2]. An animal study revealed that, the influence of estrogen or both estrogen and progesterone promotes the differentiation of subcoelomic mesenchyme to smooth muscle-like and decidua-like cells and these cells were observed as subperitoneals nodules in macroscopic view [3]. Because of the prolonged elevation of estrogen and progesterone levels in pregnancy, pregnancy was suggested as a causation of DPL and this entity was identified in case reports in the literature [4,5]. Although the name of the disease connotes malignancy, it acts as benign except some cases developing malignancy [6].
Because of the rarity of disease and coexistence of DPL with other gynaecological conditions, we aimed to present a case of DPL in a pregnant woman with leiomyomatosis uteri and a suspicious adnexal mass.
CASE PRESENTATIONA 22 year-old pregnant woman with a complaint of persistent
adnexal mass admitted to our outpatient clinic. She had no complaint in terms of abdominal swelling, abdominal pain or acute abdomen. In her history, an adnexal mass had been diagnosed at the sixth weeks of gestation and sonographic follow-up had been performed until the 13th weeks of gestation.
On physical examination an enlarged uterus and a right sided adnexal mass measuring 6 centimeters in diameter were
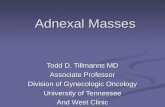
palpated. Transvaginal ultrasonography revealed, a 13 weeks aged live fetus, a heterogenous adnexal mass on the right adnexa measuring 66x38x44 millimeters in diameter and a fundal leiomyoma measuring 42x32 millimeters in diameter were revealed. The mass was suspicious of malignancy because of the morphology and the low resistance blood flow on Doppler sonography. There were no ascites in the pelvic cavity. Hemotological, biochemical and tumor marker analysis were all in normal range.
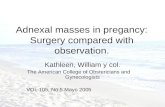
Patient was advised to have magnetic resonance imaging examination but she declined and wished to learn the definite diagnosis as soon as possible. Therefore, the patient underwent a laparotomy with midline incision because of an adnexal mass that is suspicious for malignancy. During the exploration, the uterus was enlarged a size of a 14 weeks aged gestation. There were multiple of uterine nodules measuring nearly two centimeters in diameter in the biggest one. On the right ovary, 6 centimeters cyst with well surrounded multiple nodules above the cyst capsule was identified. The right pelvic peritoneum was also containing multiple nodules similar to the ones on the cyst capsule. These nodules were smooth surfaced and egg-shaped and the biggest one was measured 7 millimeters in diameter. There were no presence of free fluid in the pelvic cavity and the omentum was in normal appearance except adhesions. Peritoneal washings, a right salpingo-oophorectomy, removal of the peritoneal nodules on the right pelvic cavity and partial omentectomy were performed. On macroscopic view after removal, the cyst was containing a 3x2 centimeters in diameter solid nodule and on frozen section analysis, no malignant findings were found. On final microscopic view, there were well-defined smooth muscle nodules on peritoneum, ovary and omentum. All of the nodules were stained by desmin. The final pathology of the nodules on ovary, peritoneum and omentum revealed DPL. The cyst was diagnosed to be a folliculer cyst. The patient had an uneventful

Central
Telli et al. (2015)Email:
JSM Clin Case Rep 3(2): 1079 (2015) 2/2
Telli E, Yalcin OT, Oge T, Kabukcuoglu S (2015) An Unforeseeable Diagnosis in a Pregnant Woman with a Suspicious Adnexal Mass. JSM Clin Case Rep 3(2): 1079.
Cite this article
recovery and was discharged on the second day of the operation. The follow-up was uneventful and after birth the patient and newborn were both healthy.
DISCUSSION The gynaecological problems appearing in pregnancy cause
trouble both for the pregnant and the clinician. Because of the enlarging uterus and in order to not to harm the fetus preserving the safety of the fetus, most of the clinicians may postpone the surgical interventions to dates after delivery. It is important to distinguish malignant lesions from benign ones before making a decision about a surgical intervention [7]. Because of the rarity of the disease and information confirmed by case reports, there is a challenge about management and follow-up of DPL in pregnancy.
There is not a perfect imaging modality to distinguish DPL from peritoneal carcinomatosis or benign conditions especially for the pregnant women. Therefore, the definitive prognosis should be confirmed by pathology [8].
In the previously reported papers, the proper treatment for reproductive aged patients was defined as removel of the nodules and omentectomy followed by cessation of the hormonal exposure [2]. Because of the lack of data for pregnants, the management remains unclear. Although there is data confirming spontaneous regression of disease after pregnancy, the development of malignancy in DPL has also been identified [6,9,10]. For the follow-up, the suggested technics after curative resection were computed tomography imaging and tumor marker testing annually for three years [11]. The influence of alteration in estrogen and progesterone levels during pregnancy on DPL was not shown and the follow-up during pregnancy was not defined.
In conclusion, clinicians should keep in mind the possibility of rare benign conditions coexisting with adnexal masses. Benign conditions may act as malignants and the use of frozen section analysis avoids unnecessary interventions during surgery.
REFERENCES1. Quade BJ, McLachlin CM, Soto-Wright V, Zuckerman J, Mutter GL,
Morton CC. Disseminated peritoneal leiomyomatosis. Clonality analysis by X chromosome inactivation and cytogenetics of a clinically benign smooth muscle proliferation. Am J Pathol. 1997; 150: 2153-2166.
2. Al-Talib A, Tulandi T. Pathophysiology and possible iatrogenic cause of leiomyomatosis peritonealis disseminata. Gynecol Obstet Invest. 2010; 69: 239-244.
3. Fujii S. Experimental approach to leiomyomatosis peritonealis disseminata--progesterone-induced smooth muscle-like cells in the subperitoneal nodules produced by estrogen (author’s transl). Acta Obstet Gynaecol Jpn. 1981; 33: 671-680.
4. Lim OW, Segal A, Ziel HK. Leiomyomatosis peritonealis disseminata associated with pregnancy. Obstet Gynecol. 1980; 55: 122-125.
5. Tripathi M, Singh PA, Tripathi A. Disseminated peritoneal leiomyomatosis: a case report. Indian J Pathol Microbiol. 2007; 50: 342-344.
6. Sharma P, Chaturvedi KU, Gupta R, Nigam S. Leiomyomatosis peritonealis disseminata with malignant change in a post-menopausal woman. Gynecol Oncol. 2004; 95: 742-745.
7. Telli E, Yalcin OT, Ozalp SS, Hassa H. Surgical intervention for adnexal masses during pregnancy. BMJ Case Rep. 2013; 2013.
8. Cohen DT, Oliva E, Hahn PF, Fuller AF Jr, Lee SI. Uterine smooth-muscle tumors with unusual growth patterns: imaging with pathologic correlation. AJR Am J Roentgenol. 2007; 188: 246-255.
9. Hoynck van Papendrecht HP, Gratama S. Leiomyomatosis peritonealis disseminata. Eur J Obstet Gynecol Reprod Biol. 1983; 14: 251-259.
10. Büttner A, Bässler R, Theele C. Pregnancy-associated ectopic deciduas (deciduosis) of the greater omentum. An analysis of 60 biopsies with cases of fibrosing deciduosis and leiomyomatosis peritonealis disseminata. Pathol Res Pract. 1993; 189: 352-359.
11. Jeyarajah S, Chow A, Lloyd J, Zacharakis E, Purkayastha S, Tekkis P. Follow-up in patients with disseminated peritoneal leiomyomatosis: a report of an unusual, high-risk case. BMJ Case Rep. 2009; 2009.
Figure 1 A right sided heterogenous adnexal mass.
Figure 2 Well-defined smooth muscle nodules on omentum (hematoxylin and eosin X80).