

An Introduction to the Care-Seeking & Referral Community ...
22
Transcript of An Introduction to the Care-Seeking & Referral Community ...

Outline of Presentation
• Overview of the aims of the COP
• Why we suggest a focus on referral & emergency transport
• Ways to think about referral & emergency transport
• How we hope to run the community of practice
• Ideas about future seminars
• Your views, questions, examples and exchange across countries
30
Why We Are Doing This
• A great deal of work remains if we are to reach the SDG targets by 2030
• Universal access to services and emergency transport for those who need it essential if we are to reach SDG goals
• Inequality is a major challenge
• Need to focus on quality
• Challenges in getting the right women and newborns to the right place at the right time.
• We currently know very little about what is happening
31
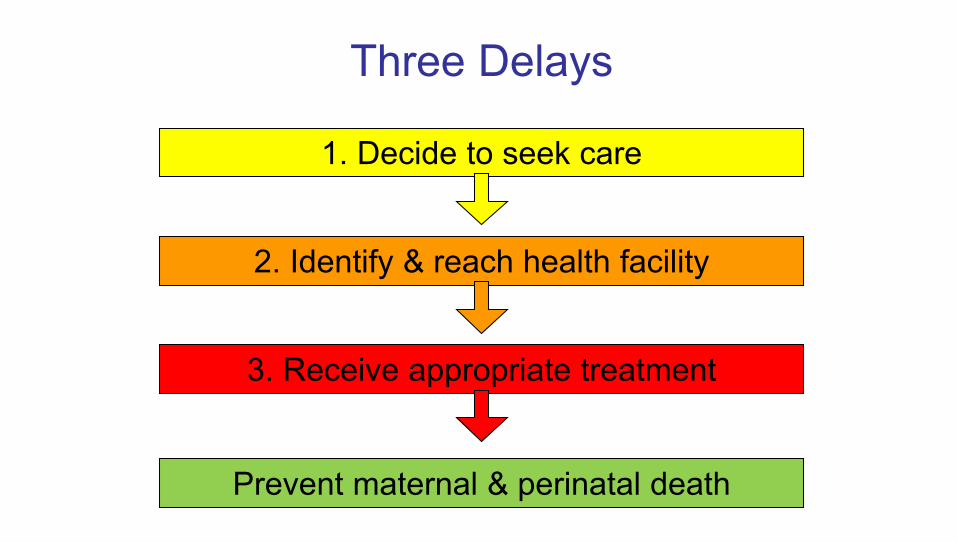
Three Delays
1. Decide to seek care
2. Identify & reach health facility
3. Receive appropriate treatment
Prevent maternal & perinatal death
• Lassi ZS, Bhutta ZA. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database of Systematic Reviews 2015
• World Health Organization and International Initiative for Impact Evaluation. An evidence map of social, behavioural and community engagement interventions for reproductive, maternal, newborn and child health. Geneva: World Health Organization; 2017.
• Active CoP & other activities on Community Health Workers
33
1. Decide to seek care

• High-quality health systems in the SDG era: time for a revolution– https://www.hqsscommission.org
• WHO– Quality framework & new guidelines
• Respectful Care Community
34
3. Receive appropriate treatment

5/21/2019 35
2. Identify & reach health facility

Campbell OMR, Calvert C, Testa A, Strehlow M, Benova L, Keyes E, Donnay F, Macleod D, Gabrysch S, Rong L, Ronsmans C, Sadruddin S, Koblinsky M & Bailey P. The scale, scope, coverage & capability of childbirth care. Lancet 2016
4 3 Emergency transport pathways
Emergency Strategy
Facility with routine care only
Facility with routine care &
Facility with routine care
BEmOCCEmOC
(or alongside midwifery unit) &
Home

Campbell OMR, Calvert C, Testa A, Strehlow M, Benova L, Keyes E, Donnay F, Macleod D, Gabrysch S, Rong L, Ronsmans C, Sadruddin S, Koblinsky M & Bailey P. The scale, scope, coverage & capability of childbirth care. Lancet 2016
4 3 2
1
2
3
4
Emergency transport pathways
Skilled birth attendant strategies
Facility with routine care only
Facility with routine care &
Facility with routine care
BEmOCCEmOC
(or alongside midwifery unit) &
Home Maternity WaitingHome
Go to maternity waiting home ahead of labor 0
Routine transport pathways
1

• Attend routine ANC (can be from multiple providers)
• Attend 6 week post-natal care
• Babies to well baby clinic
• During the day
• Can be planned for
• Not too far
• Free or low cost
• Public transport might be available
• Woman and baby well
• Doesn’t need accompanying
Easy Journeys
38
• Woman referred in ANC (but generally well)
• Baby referred (but generally well)
• Baby referred to other services (but generally well)
• Early post-natal visit
• During the day
• Can be planned for
• Likely to be further away and cost more
• Public transport might be available
• Other costs incurred
• Woman and baby generally well
• Doesn’t necessarily need accompanying
Not So Easy Journeys
39
• Woman in normal labour to a facility to deliver
• Woman home from the hospital after delivering
• Unwell baby to facility
• Can be any time of the day or night
• If at night – possible security issues
• Might need to arrange or hire private transport – so more expensive
• Body fluids
• Urgency
• Companion needed
• Ergonomics
• Women / Baby in pain
Uncomfortable Journeys
40

• Pregnant woman seriously ill
• Woman in a labor with complications home to facility
• Woman in labor with complications facility to facility
• Sick & small newborn facility to facility
• Can be any time of the day or night
• If at night – possible security issues
• Might need to arrange or hire private transport – so more expensive
• Body fluids
• Urgency
• Companion needed
• Ergonomics
• Woman/ Baby In Pain
• Everyone extremely stressed
Emergency Journeys
41

Key Components of a Successful Referral System
• Knowledge of population needs and health system capabilities
• An adequately resourced referral center
• Active collaboration between referral levels and across sectors
• Formalized communication and transport arrangements
• Agreed setting-specific protocols for referrer and receiver
• Supervision and accountability for providers performance
• Affordable service costs
• Capacity to monitor effectiveness
• Policy support
Murray S, Pearson S (2006) Maternity referral systems in developing countries: Current knowledge and future research needs. Social Science and Medicine 62 (2006) 2205-2215
42

43

Insights From Qualitative Studies
• Long amount of time often took to organize transport
• Limited transport options in some areas, some times of year
• Different experiences of local support
• Who will look after other children
• Drivers refusing to transport women in labor because of fear of soilage or concerns women might die in transit
• Cost
• Embarrassment , “shameful”
• Pain
• Uncomfortable positions
Wilson et al. A Systematic review and thematic synthesis of qualitative studies on maternal emergency transport in low and middle income countries. IJOG. 122 (2013)
44

Reasons to re-look at the issue of emergency transport & referral
• Quality and respectful care emphasis
• Rights approach
• Technological advances
• Sick and small newborns
• Increased recognitions of inter- and intra-country inequality
• The role of the nonprofit and private sector
• Cash transfers
45

Hopes for This Community of Practice
• Involvement of a range of people working in different areas in a range of countries
• Implementation focus
– Context
– Processes
– Scale
• Always thinking about access for the poor and vulnerable
• Respectful, kind safe space to admit challenges and mistakes
46

Future Seminars
• How can we better measure to inform practice
– Bangladesh DHS, Record Reviews in Nigeria, Referral Audits
• What does respectful referral look like? What would a rights approach to referral look like?
• Challenges in managing an ambulance fleet
– Do you have specialized ambulances, where are ambulances stations, how to you run a call canter?
47

What Are Your Views?
• What are your questions about the presentation? • Do you agree this is a good area to focus on? • What important work/issues have we forgotten?
• What relevant work would you like to share?• Are there other relevant networks we should link into ? (Emergency
medicine) • What would you like to know about others working in different settings?
• What are you suggestions for future presentations?
48
Next Steps
Please send suggestions on :
• Names of people to invite to join this community of practice
• Resources (documents or links) of interest to members of this community of practice
• Focus of the COP
• Any issues raised in the webinar that have not been addressed
To: Loveday [email protected]
5/21/2019 FOOTER GOES HERE 49
THANK YOU.
This presentation was made possible by the support of the American People through the United States Agency for International Development (USAID) under the terms of the Coordinating Implementation Research to Communicate Learning and Evidence (CIRCLE) contract AID-OAA-M-16-00006. CIRCLE is implemented by Social Solutions International, Inc., in partnership with Forum One. Views expressed are not necessarily of USAID or other affiliated institutions.
5/21/2019 FOOTER GOES HERE

















