
An Intro to the World of Forensics · (HBO‐ Autopsy), Dr. Henry Lee, Dead Men ... 1. Peden M,...
29
An Intro to the World of Forensics MayJen Amolat‐Apiado, MD, MFM, MPH Forensic Pathologist, Forensic Science Adjunct
Transcript of An Intro to the World of Forensics · (HBO‐ Autopsy), Dr. Henry Lee, Dead Men ... 1. Peden M,...
AnIntrototheWorldofForensics
MayJenAmolat‐Apiado,MD,MFM,MPHForensicPathologist,ForensicScienceAdjunct
FORENSICSDEFINED• Forensic‐fromforensis‐todebate/argue,relatedtothelaw,akaforum
• Forensicscience‐anyscienceappliedtolegalissues
• Forensicmedicine‐medicalknowledgeappliedtolegalissues(appliedtotheliving;forensicnursing;forensicpathology;forensicpsychiatry)
• Differentdisciplineswithintheforensicssciences‐criminalisOcs(hair,fiber,physical/biologicalevidence),quesOoneddocuments,anthropology,pathology,odontology,profiling,digitalmedia,engineering,wildlifeforensics

VALUEOFFORENSICSCIENCE

CRIMESCENERECONSTRUCTION FORENSICSCIENTIST(S)
MEDICALEXAMINER
INVESTIGATOR/POLICE

GENERALEDUCATIONALTRACK
• Bachelors• (Masters• PhD/terminaldegree• Postgradwork/forensicsubspecializaOon)• MembershipsinsocieOes• (Board‐cerOficaOoninparOcularfield• RelevantpublicaOons)• Onthejobexperience

FORENSIC‐RELATEDCAREERS• INSCHOOLSForensiceducators‐K‐12teachers,college/gradschool
• WITHPOLICE:Evidence/crimescenetechnicians,police(policeacademy)
• INCRIMELABS:BS;orMSinForensicScienceorPhDwww.aafs.org,www.criminalists.org
• INCOURT:lawyers:JD,passingthebar

CAREERS2• InMEDICALEXAMINERSOFFICEHAS:MDtrainedinanatomicpathologyandforensicpathology(medicalexaminer)
• PhD‐levelandboard‐cerOfiedforensictoxicologists‐detecOonofchemicalsubstancesinpostmortemorlivingsample
• Morguetechnicians‐anatomy(biology/funeraldirectorbackground)furthertraininginphotography,radiology
• Supportstaff‐secretaries/administrators‐asset;BA/BS/AA/AS
• InvesOgators‐nursing,EMS,Physicianassistant,morgue/funeraldirectorslatertrainedandcerOfiedbyAMERICANBOARDOFMEDICOLEGALDEATHINVESTIGATORS– OPTIONALBUTMOSTWELCOME:Counselors‐PsyD,PhDorMSWforbereaved/PTSD/violent;EPIDEMIOLOGISTS;MS,PHDorMPH
CAREERS3• INHOSPITALS:Forensicnurses;RNwithSANE+forensicmedicine
training(www.iafne.org);forensicphysicians(inUKcalledpolicesurgeons,employedbypolice)
• FORENSICODONTOLOGY‐bitemark,ID,DDSdegree,www.abfo.org
• FORENSICBIOLOGISTS/ENTOMOLOGISTS/DNASCIENTISTS‐BS,MA,PhD
• CRIMINALPROFILING‐FBIbehavioralscienceunit;forensicpsychologists,MA,PhD,alsowww.forensic‐science.org
• WILDLIFEFORENSICS‐USFishandWildlife,criminalistsalsovetswithforensictraining/experiencewww.lab.fws.gov
CAREERS4
• INNGOsvsWARCRIMES:Forensicanthropology(BS(4),MA(2),PhD(4‐6)pluspostgraduatework)www.theabfa.org
• INOWNCOMPANIES:Digital/computerforensics,quesOoneddocuments‐‐AmericanSocietyofQuesOonedExaminerswww.asqde.org,AmericanBoardofForensicDocumentExaminerswww.abfde.org
• INACADEMIAorGovtorNGOsefng,alsoPRIVATEPRACTICE:alloftheabove
BEETHICALASANEXPERTWITNESS;DONOTFALSIFYORCONFOUNDJURYJUSTBECAUSEYOUARE“BELIEVABLE”TOTHEJURY
• MEDIAPERSONALITY:Dr.G(DiscoveryChannel),Dr.Baden(HBO‐Autopsy),Dr.HenryLee,DeadMenTalking,aCBSshow;alsoCSIshowconsultants

TRUTV.COMTRUTVLIBRARY

WHATNEXT?CHECKOUT—AAFS.ORG,
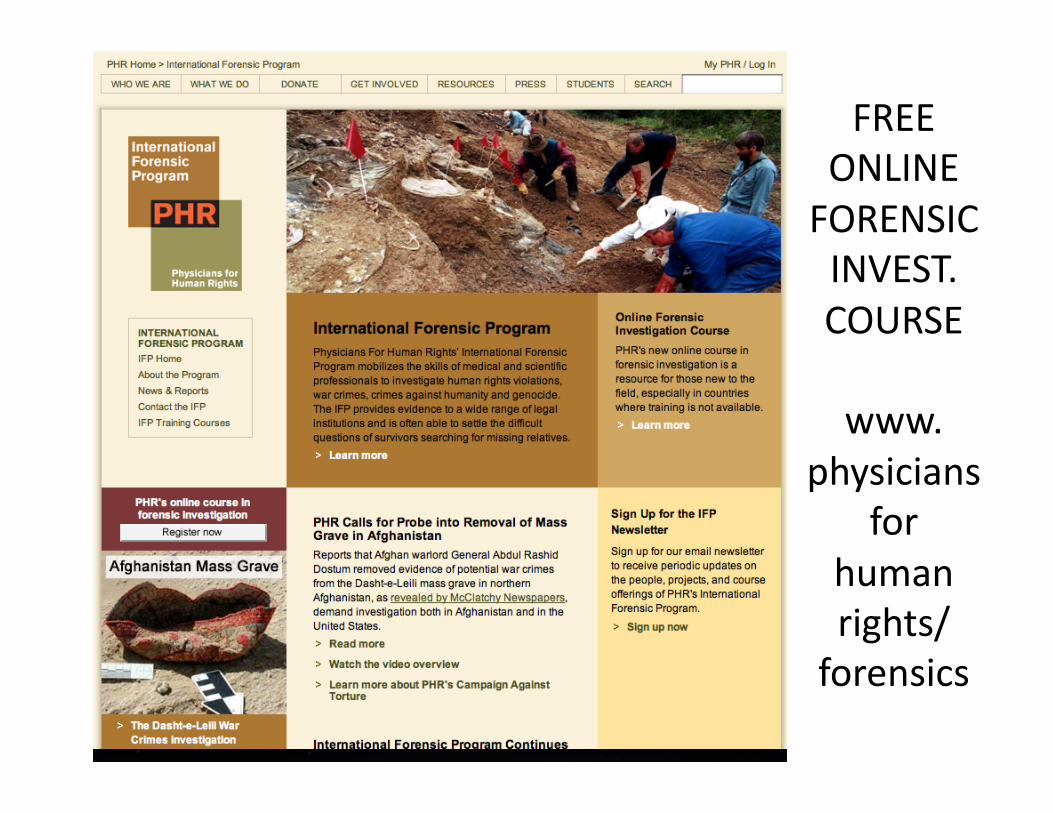
FREEONLINEFORENSICINVEST.COURSE
www.physicians
forhumanrights/forensics
NEXTFRONTIER• Morepeople,morestudentsinbekerschools(CSIeffect‐inTVcrimesissolvedsomuchfaster,BUTrealityismorecolorfulormorebizarrethanficOon)
• Improvedscienceandtechnology(fasterDNAthroughputsonobackloginpropertyandpersonalcrimes),moreandbekerresearch
• Bekerstandardsinlawandforensics,sotherewillbenowrongfulconvicOons(ex.Innocenceproject)
• OUTCOMES:LESSCRIME,SAFERCOMMUNITIES,LESSPEOPLEDYINGBEFORETHEIRTIME

MayJenniferAmolat‐Apiado,MD,MFM,MPHAmericanAcademyofForensicSciencesAnnualMeeOng
ACauseforForensicPublicHealth:Preven7onandPublicHealthContentinTwoU.SForensicJournals
GLOBALINJURYBURDEN
• Injuryresultsin9%oftheworld’smortality
– mostlyfromlow‐andmiddle‐incomecountries
– 5Mdieannuallyfrominjury– Thenumberofhomicides(500,000)orthenumberofsuicides(860,000)ishigherthanthenumberofdeathsfromHIV,malariaandtuberculosiscombined(1)
1.PedenM,McGeeK,SharmaGTheInjuryChartbook:AGraphicalOverviewoftheGlobalBurdenofInjuries.Geneva:WorldHealthOrganizaOon;2002.
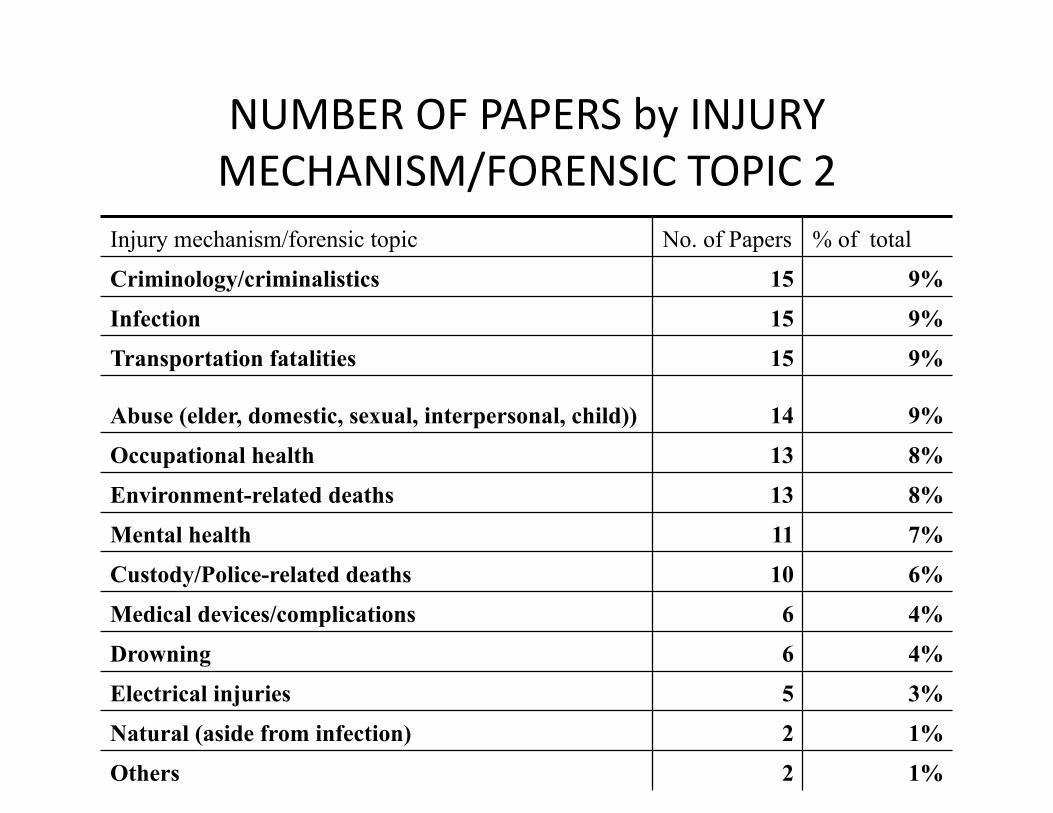
NUMBEROFPAPERSbyINJURYMECHANISM/FORENSICTOPIC2
Injury mechanism/forensic topic No. of Papers % of total
Criminology/criminalistics 15 9%
Infection 15 9%
Transportation fatalities 15 9%
Abuse (elder, domestic, sexual, interpersonal, child)) 14 9%
Occupational health 13 8%
Environment-related deaths 13 8%
Mental health 11 7%
Custody/Police-related deaths 10 6%
Medical devices/complications 6 4%
Drowning 6 4%
Electrical injuries 5 3%
Natural (aside from infection) 2 1%
Others 2 1%

NO.OFPAPERSbyMANNEROFDEATH
Manner of death Number of Papers
Percentages of total
Accidents 61 37%
Suicide 30 19%
Homicide 29 18%
Natural 24 15%
Therapeutic complication/misadventure
7 4%
Other/not applicable 36 22%

NUMBEROFPAPERSBYPRIMARYAUTHOR’SSPECIFICAFFILIATION1
Specific affiliation of 1st author No.of Papers % of total Medical examiners’ offices 34 21%
Academic forensic medicine department 18 11%
Hospital department, pathology 18 11%
Other government public health agencies 16 10%
Hospital departments, psychiatry 14 9%
Medical school/med center/hospitals 12 7%
University department/university 11 7%
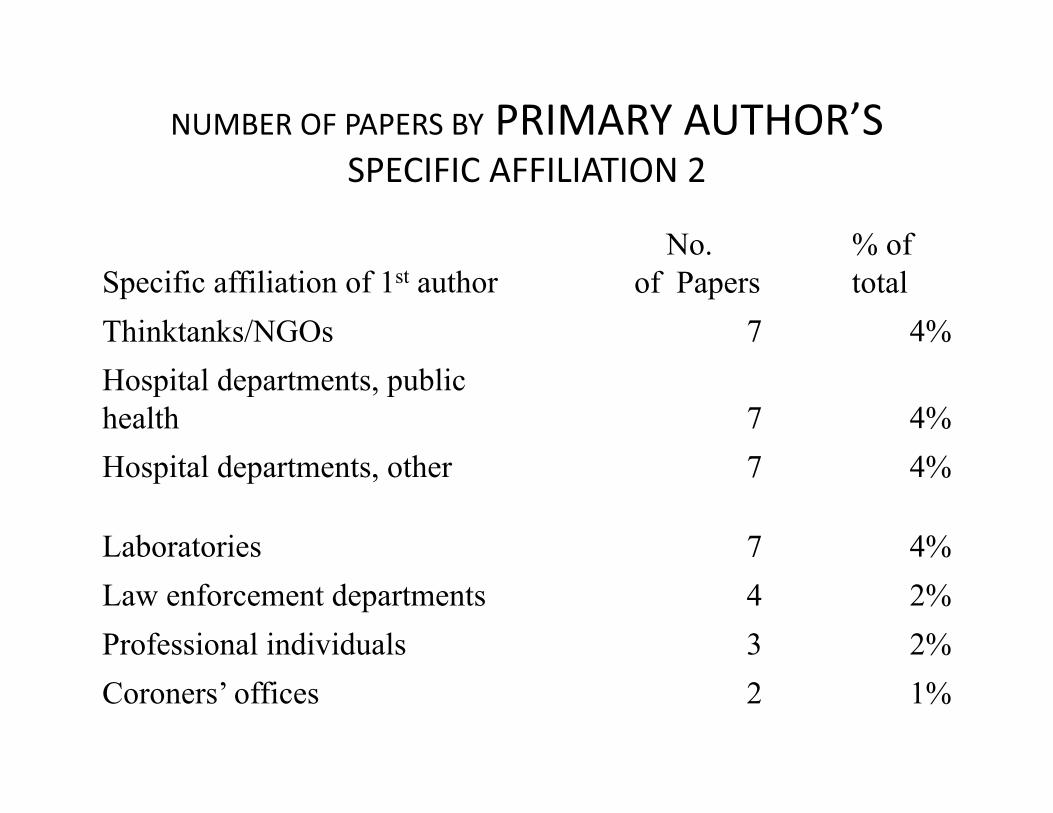
NUMBEROFPAPERSBYPRIMARYAUTHOR’SSPECIFICAFFILIATION2
Specific affiliation of 1st author No.
of Papers % of total
Thinktanks/NGOs 7 4%
Hospital departments, public health 7 4%
Hospital departments, other 7 4%
Laboratories 7 4%
Law enforcement departments 4 2%
Professional individuals 3 2%
Coroners’ offices 2 1%
AREWEDOINGENOUGH?
PublichealthpracOcecanbenefitfromincreasedparOcipaOonofmedicalexaminersandotherforensicdisciplinesastheyareinherentlyinvolvedincasesofinjuryandviolence
THEBESTFORENSICSISNOTENOUGH!WENEED
SOCIALWORK/MENTALHEALTHREFERRALS,PARTICIPATIONINCOMMUNITY,IMPROVESCHOOLS,PARENTINGPRACTICES/PEERQUALITY,ANTI‐CRIMELAWS(ex.firearms),JOBSANDBETTERSURROUNDINGS(environmentalpolicing)

ECOLOGICALMODELFrameworkfordeterminingrisksandintervenOons
age,educaOon,income,substanceandalcoholabuse,psychiatricorpersonalitydisordersandhistoryofviolentbehaviororabuse
poorparenOngpracOces,conflictinthehome(marriageorfamily)andassociaOonwithdelinquentorviolentfriends
drugtrade,highratesoftransients(residenOalmobility),poverty,unemployment,socialisolaOonandweakorineffecOveinsOtuOons.
normsthatsupporttheuseofviolence,availabilityofweapons,weakcriminaljusOcesystems,policiesthatperpetuateorincreasesocioeconomicinequaliOes

YES,YOUCAN!
WECANALLCONTRIBUTEINHELPINGSAVELIVES.
ADDRESSINDIVIDUAL,FAMILY,COMMUNITYANDSOCIETALRISKFACTORSTHROUGHABROAD‐BASEDFORUMOR(PUBLICHEALTH)GROUP.
USEINTERVENTIONSTHATAREPROVENTOWORK!(SEEHANDOUTorblog)

VIOLENCEINTERVENTIONSECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE INFANT AND TODDLER (AGED 0–3) CHILDHOOD (AGED 3–11)
Individual • Reduce unintended pregnancies • Increase access to prenatal/postnatal services • Treatment programmes for victims of maltreatment to reduce consequences • Services for children who witness violence
• Social-development training • Pre-school enrichment
• School-based child maltreatment prevention programmes
• Drug-resistance education • Gun-safety training
Relationship (for example, family, peers)
• Home-visitation services • Parenting training • Therapeutic foster care
• Mentoring • Home-school partnership programmes to promote parental involvement
Community • Lead monitoring and toxin removal • Screening by health-care providers for maltreatment
• Safe havens for children on high-risk routes to and from school • After-school programmes to extend adult supervision • Recreational programmes
• Community policing • Improving emergency response and trauma care • Training for health-care providers in the detection and reporting of child maltreatment • Promotion of safe storage of firearms and other lethal weapons • Prevention and educational campaigns to increase awareness of child maltreatment • Child-protection service programmes • Services for incarcerated perpetrators
• Gun buy backs
Societal • Reduce media violence • Public information campaigns to promote pro-social norms
• Strengthen police and judicial systems • De-concentrate poverty • Reduce income inequality
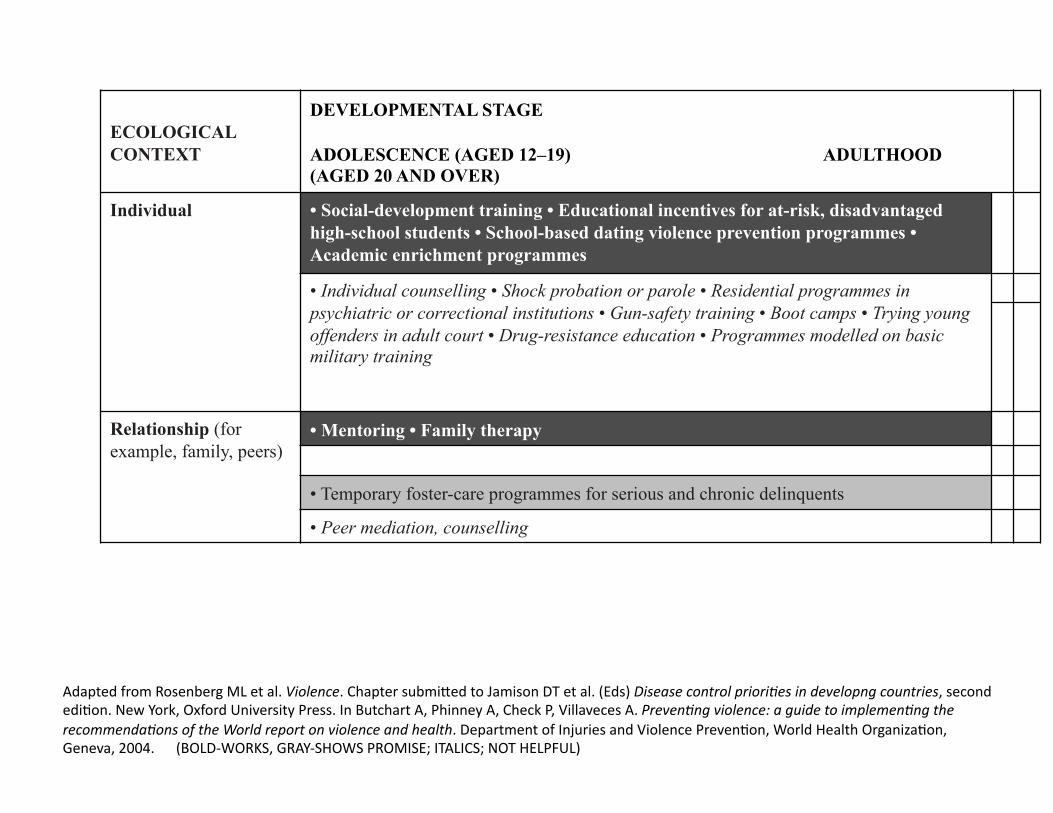
ECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE
ADOLESCENCE (AGED 12–19) ADULTHOOD (AGED 20 AND OVER)
Individual • Social-development training • Educational incentives for at-risk, disadvantaged high-school students • School-based dating violence prevention programmes • Academic enrichment programmes
• Individual counselling • Shock probation or parole • Residential programmes in psychiatric or correctional institutions • Gun-safety training • Boot camps • Trying young offenders in adult court • Drug-resistance education • Programmes modelled on basic military training
Relationship (for example, family, peers)
• Mentoring • Family therapy
• Temporary foster-care programmes for serious and chronic delinquents
• Peer mediation, counselling
AdaptedfromRosenbergMLetal.Violence.ChaptersubmikedtoJamisonDTetal.(Eds)DiseasecontrolprioriBesindevelopngcountries,secondediOon.NewYork,OxfordUniversityPress.InButchartA,PhinneyA,CheckP,VillavecesA.PrevenBngviolence:aguidetoimplemenBngtherecommendaBonsoftheWorldreportonviolenceandhealth.DepartmentofInjuriesandViolencePrevenOon,WorldHealthOrganizaOon,Geneva,2004.(BOLD‐WORKS,GRAY‐SHOWSPROMISE;ITALICS;NOTHELPFUL)
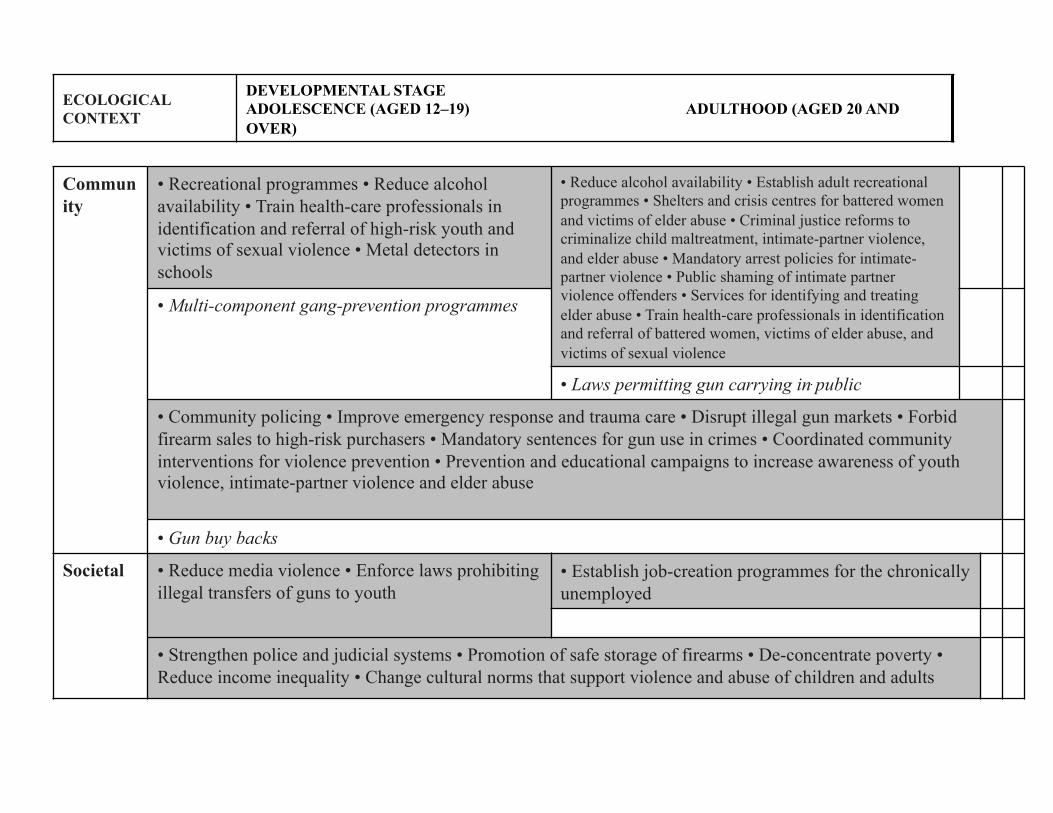
Community
• Recreational programmes • Reduce alcohol availability • Train health-care professionals in identification and referral of high-risk youth and victims of sexual violence • Metal detectors in schools
• Reduce alcohol availability • Establish adult recreational programmes • Shelters and crisis centres for battered women and victims of elder abuse • Criminal justice reforms to criminalize child maltreatment, intimate-partner violence, and elder abuse • Mandatory arrest policies for intimate-partner violence • Public shaming of intimate partner violence offenders • Services for identifying and treating elder abuse • Train health-care professionals in identification and referral of battered women, victims of elder abuse, and victims of sexual violence
• Multi-component gang-prevention programmes
• Laws permitting gun carrying in public
• Community policing • Improve emergency response and trauma care • Disrupt illegal gun markets • Forbid firearm sales to high-risk purchasers • Mandatory sentences for gun use in crimes • Coordinated community interventions for violence prevention • Prevention and educational campaigns to increase awareness of youth violence, intimate-partner violence and elder abuse
• Gun buy backs
Societal • Reduce media violence • Enforce laws prohibiting illegal transfers of guns to youth
• Establish job-creation programmes for the chronically unemployed
• Strengthen police and judicial systems • Promotion of safe storage of firearms • De-concentrate poverty • Reduce income inequality • Change cultural norms that support violence and abuse of children and adults
ECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE ADOLESCENCE (AGED 12–19) ADULTHOOD (AGED 20 AND OVER)
WHO‐VIPwebsite
hkp://www.who.int/violence_injury_prevenOon/violence/en/
CDC

THANKYOU!
• Dr.AMOLAT‐APIADO’sCONTACTANDHANDOUTS:
Blog:
theautographer.wordpress.com
Email:


![Here in, you will find the generations of Tom Riley ... · 2. Pressie Jamison Jr. married Janette Issac-Jamison [5] childen A. James Alton Jamison married Elizabeth Willis-Jamison](https://static.fdocuments.in/doc/165x107/5fbd9c48cb905b04f4672401/here-in-you-will-find-the-generations-of-tom-riley-2-pressie-jamison-jr-married.jpg)















