R3 030340(tr25.891 v030 improvement of rrm across rns and rns bss)-rev
Upload
bonnie-payneCategory
view
213download
0
An Innovative Support Group For Graduate RNs Working in Long Term Care
Jeanne Delicata RN, MSN, APRN, BC, Allyson Koenig RN BSN; & Patricia Morgan PhD, RN, CNE
Addresses Nurse of the Future Core Competencies©• Evidenced-Based Practice • Professionalism• Leadership• Safety • Quality• Communication • Teamwork & Collaboration
A New Collaboration between Nursing Practice and Education

Issues common among new graduate nurses in long-term care identified (May 2010)
• Unrealistic expectations for practice
• Interactions with older experienced RNs
• Charge Nurse responsibilities
• Safety
• Attrition
• Documentation
• Lack of familiarity with Nurse Practice Act or Standards of Practice

Literature Confirmed Problem
– Transition into practice stressful time for new graduate nurses (Calhoun, 2010).
– New graduates cite lack of support (Boswell, Lowry & Wilhoit, 2004).
– New graduates have difficulty with time management, inter-professional interactions, and lack skills to communicate with CNAs and older RNs (MPNEP, 2011).

– Long-term care is especially difficult for new RNs because they assume charge positions quickly after orientation.
– Charge positions in LTC can be stressful, feel overwhelming and contribute to high attrition rates for new nurses (Aaron, 2011).

PROJECT DESIGN
• Innovative interventions aimed at improving the transition to practice into long term care for new graduate nurses at the Maine Veterans Home (MVH)
• New collaboration among University of New England Nursing Faculty, MVH Nurse Educator & Millennial Charge Nurse

GOALS
1. Increase participation in the Benner Group.2. Secure educational materials for each new RN
hired starting in 2011.3. Evaluate impact and outcomes for the
participating nurses around identified issues.4. Introduce the concept of the Benner Group to
another LTC facility within MVH system.

ACTIVITIES
• Monthly support group meetings• Discussions included scope of practice, State Board of Nursing
rules and regulations, documentation for LTC, communicating with CNAs
• Issued a ‘Documentation Pocket Guide’• Issued BON Rules & Regulations and ANA Principles of
Documentation • Issued MVH ‘Nursing Pearls’ and Quick Flip Notes• “Know it before you call” cards placed on all units• Ordered: Benner’s (2001) From Novice to Expert & A Charge
Nurse’s Guide ( )

OUTCOMES
• Benner Group sessions increased to twice/month at request of new graduate nurses
• Attendance rate 50% initially, recently declined
• 8 new grads hired in fall of 2010 and 7 still working*.
OUTPUTS
• Study to evaluate impact of support group on nurses pending IRB approval
• Plan to implement Benner Group with 5 new grads hired in 2012
• Intend to introduce Benner Group Model to another LTC facility
External Factors:-Down Economy-Lack of open positions for
new grads-New grads turning to LTC
for work but not their first choice
Practicum Exploring Patient Safety During Transitions in
Surgical Care Gloria Neault, MSN, RN, CNOR
Staff Development EducatorSouthern Maine Medical Center

Competency Gaps
• Patient-centered care • Safety • Communication • Teamwork and collaboration
• Systems-based practice • Quality improvement • Safety • Communication• Teamwork and collaboration
New Graduates Rated Top 4 in Importance as a Nurse
Preceptors’ Assessments of Lowest Scoring Competencies
Nurse of the Future Competencies
• Safety
• Collegial Communication
• Teamwork & Collaboration

Comparison
• 154 hrs • One preceptor• One unit • Most Med-Surg, SCU and ED • Only 4% surgical!
• 154 hrs • Multiple preceptors• Multiple Surgical Services areas
(systems-based) • “Interdisciplinary Days” • Focus: Safety
Traditional Practicum Innovative Practicum

Clinical Days: Systems-Based
• Pre-Admission Testing • Ambulatory Care • Operating Room • Post-Anesthesia Care • Endoscopy • Radiology • Cardiac Cath Lab

Interdisciplinary Days: Focus on Safety
• Infection Control • Quality Management • Case Management • Risk Management • Clinical Nurse Specialist • Surgeon
– Office – Preoperative and postoperative care – Hospital rounds – Procedures
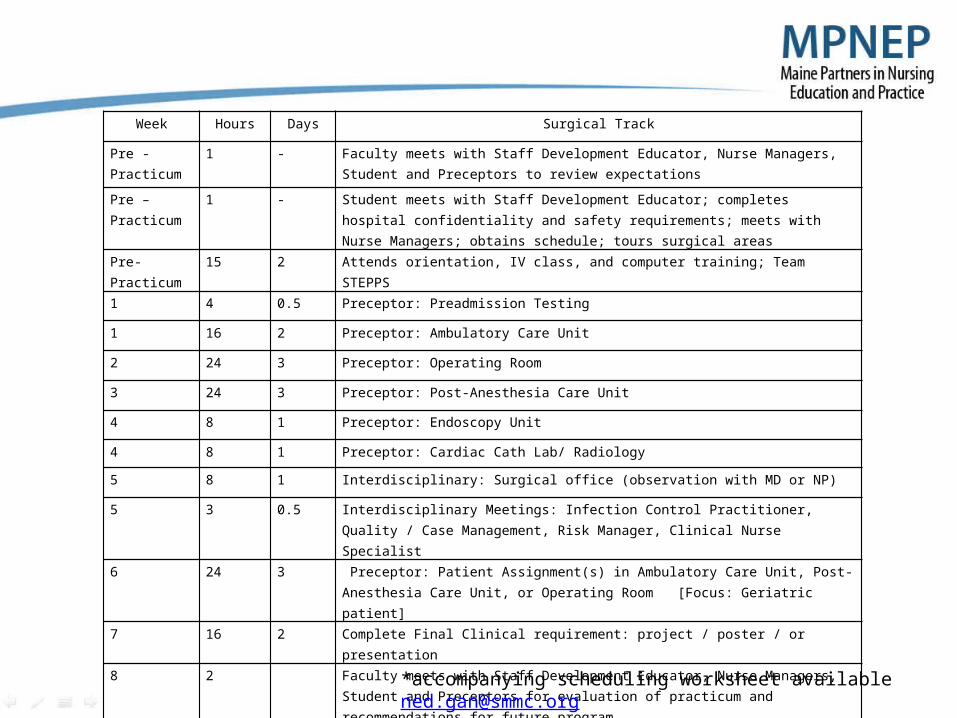
Week Hours Days Surgical Track
Pre -Practicum 1 - Faculty meets with Staff Development Educator, Nurse Managers, Student and Preceptors to review expectations
Pre –Practicum 1 - Student meets with Staff Development Educator; completes hospital confidentiality and safety requirements; meets with Nurse Managers; obtains schedule; tours surgical areas
Pre-Practicum 15 2 Attends orientation, IV class, and computer training; Team STEPPS
1 4 0.5 Preceptor: Preadmission Testing
1 16 2 Preceptor: Ambulatory Care Unit
2 24 3 Preceptor: Operating Room
3 24 3 Preceptor: Post-Anesthesia Care Unit
4 8 1 Preceptor: Endoscopy Unit
4 8 1 Preceptor: Cardiac Cath Lab/ Radiology
5 8 1 Interdisciplinary: Surgical office (observation with MD or NP)
5 3 0.5 Interdisciplinary Meetings: Infection Control Practitioner, Quality / Case Management, Risk Manager, Clinical Nurse Specialist
6 24 3 Preceptor: Patient Assignment(s) in Ambulatory Care Unit, Post-Anesthesia Care Unit, or Operating Room [Focus: Geriatric patient]
7 16 2 Complete Final Clinical requirement: project / poster / or presentation
8 2 Faculty meets with Staff Development Educator, Nurse Managers, Student and Preceptors for evaluation of practicum and recommendations for future program
Total 154 20 approx
*accompanying scheduling worksheet available [email protected]

Outcomes
• Practicum academic objectives met • Safety, communication, teamwork and collaboration project objectives met • Increased knowledge and appreciation for the complex nature of safety:
– Systems-based: seeing the whole patient experience – Role of interdisciplinary team members on patient safety – Interdisciplinary Days value-added – Collaborative poster presentation at Maine Nursing Summit
• Communication – Increased communication between education and practice – Formal group meetings held
• Planning and evaluation • Included student, preceptor, managers, staff development, and faculty
– Important role of hand-off communication – Incorporation of Team STEPPS principles

Outcomes
• Teamwork and collaboration – Surgery viewed as a systems-based continuum – Interdisciplinary nature of healthcare – Appreciation for the contributions of all disciplines
• Professional development of student – Student participation in planning and evaluation meetings – Maine Nursing Summit
• Collaborative poster by student and educator • Attendance of student with preceptor and most planning team members
• Critical role of preceptor identified • Outputs: tools developed
– Surgical Practicum Track – Scheduling Worksheet

Future of Project
• Adjustments to track – Decrease time in preadmission testing – Addition of initial patient observation
• Through whole system • Prior to work in individual areas • Faculty recommendation
– Increase focus on geriatric patient
• Recommendations to other health care organizations
– Replication – May use in other clinical areas – Surgical practicum being requested
by students for next semester – Positive learning experience for
student, preceptors, managers, educators, and faculty
– Tools developed to organize the flow and scheduling of practicum experiences
• Student schedule / expectations • Preceptor and manager guidance • Faculty communication • Setting interdisciplinary days • Assuring pre and post meetings

Millennial Preceptor Program: Preparing for the Future
Gloria Neault, MSN, RN Staff Development Educator
Southern Maine Medical Center

Preceptor Demographics in Maine
• Current preceptor demographics– 31% 24-35 years old – 31% 1-5 yrs as RN – 46% 1-5 yrs precepting – 54% less than 5 new graduates precepted
• Preceptor demands increasing (G. Neault, MSN) – Practicum students - traditional, second-career, second-degree – New employees - new graduates, experienced nurses from multiple
generations – Nurse Residency Programs
Preparation as a Preceptor
• Maine preceptor “perception of preparedness”
– 20% well-prepared – 39% prepared – 36% somewhat prepared – 6% poorly prepared
• 57% of preceptors have received no formal preceptor education!
Millennial Preceptor Program: Preparing for the Future
• Goal:
to deliver a preceptor program that meets the needs of the Millennial nurse preceptor
Millennial (Generation Y / Net Generation) born about 1980-2000 (Ulrich, 2012)

Nurse of the Future Competencies
• Teaching / Learning • Professionalism
Millennial Preceptor Program
• Based on – Preceptor demographics in Maine – How adults and millennial adults prefer to learn
– Self-direction (adults) – Immediate application to real-life work (adults)– Increased technology use (Millennial)– Small group work (Millennial)
• Blended methodology – Technology use: online preceptor course – Technology use: links, email list – Interactive, small group work: ½ day workshop

Outcomes
• One published research study on blended preceptor program using online course and workshop (Bradley, et. al, 2007)
• Evaluation of learner and instructor satisfaction with blended preceptor program
• Survey questionnaires – Preceptor satisfaction – Instructor satisfaction
• IRB approval • Replication study following workshop 3/2/12• Preliminary poster presentation at Maine Nursing Summit 3/21/12 • Statistical analysis in progress
– Kristiina Hyrkas, Ph.D., Maine Medical Center, Center for Nursing Research and Quality Outcomes
Outcomes
• Comparison to Maine Partners in Nursing Education and Practice Preceptor Survey Data (2011) – Selected questions from MPNEP Preceptor Survey – Preceptor demographics – Included in IRB approval
• Data collected following workshop 3/2/12 • Preliminary poster presentation Maine Nursing Summit 3/21/12 • Statistical analysis in progress
– Kristiina Hyrkas, Ph.D., Maine Medical Center, Center for Nursing Research and Quality Outcomes

Initial Findings
• n = 15
• 100% completed online course • 100% completed workshop • 100% completed questionnaire
• Learners and educators satisfied with blended method
• Success due to lessons learned from Bradley et. al (2007): – Frequent communication – Address computer issues proactively

Initial Findings
Maine Preceptors Millennial Preceptors
(MPNEP, 2011) (Neault, 2012)
• 48% 93% BS/BSN• 31% 60% 1-5 yrs practicing • 31% 87% 24-35 years old • 43% 53% 1-5 yrs precepting • 54% 100% less than 5 new graduates precepted • 57% 87% no preceptor education • 42% 80% somewhat/poorly prepared
Future of Project
Health care organization use
• Plans to continue • Educator benefits
– Decreased workshop prep time – Learners arrive with basic knowledge– Learners prepared to participate in
workshop – Collaboration with faculty
• Learner benefits – Convenient – Own pace – Millennial learning methods
• Maintains face-to-face contact
Recommendations
• Consider use for Millennial and Gen X preceptor development
• Cost-effective – Decreased educator time – ½ day workshop vs full-day – Offsets cost of online program
selected
– Increased retention rates • Collaboration among multiple
health care organizations in Maine being discussed
MEPNEP-Dirigo Pines
Modified Gerontology Dedicated Education UnitIn Retirement Community Assisted Living
Lisa Harvey-McPherson, Executive SponsorProject leaders:
Maggie Michaud, RN, Executive Director, Dirigo PinesBeth Clark, PhD, Director of Undergraduate programs, Husson University
Elisa Giaquinto, Assistant Professor, Husson UniversityValerie Sauda, Geriatric Nurse Service Instructor, Rosscare
• Project goals– Identify and align Husson University clinical and
course objectives with AACN gerontology nursing competencies for healthy older adults
– Develop and deliver staff nurse preceptor program– Establish gerontology nurse educator
collaborations at Dirigo Pines
• Geriatric Nurse service Instructor provided training modules for staff to coach students– Staff engaged in collaborative opportunity
• Husson faculty provided 6 week clinical experience onsite – Focus on topics like medication reviews, functional
assessments, culture and aging, and economic issues in aging

• Lessons learned-Staff education– Staff training
• “Coaching” model effective for this level of care• Staff enjoyed coaching training program
“teaching college”• Staff turnover can be challenging for continuity• Low number of RN staff onsite

• Lessons Learned-Student clinical experience
– Conflict between accreditation bodies for school and clinical preceptor type model (MS required)
– Experience valuable for interprofessional communication
• There were non-caring behaviors observed-Labeling, stereotyping
-Identified as lack of education by faculty• Students able to see economic disparity in aging
between two different assisted living (one high income, one low income) and were able to identify trend in nursing models of care/system of healthcare for aging at this level of care

• Students reflections recorded in their journals were powerful about gerontology
• Faculty/staff relationship building important and valuable

• Overall, staff, faculty and students satisfied with the experience– Inclusive communication was key to resolving
issues and challenges that developed during the project.
– Project leadership team also communicated regularly regarding implementation of the pilot project.

• For the future– Increase student involvement in continuum of
care in this setting– Develop more delegation exercises for students in
the clinical experience– Increase faculty involvement on site to increase
staff education and mentoring– Potential for a faculty mentorship program
development to help mentor upcoming faculty in area of gerontology nursing education

Collaborative Immersion Model: Daring to Imagine, Listen, and Create
Carla E. Randall, PhD, RN, Principle Investigator
Research team:Allison Haynes, BS, RN
Kristiina Hyrkas, PhD, LicNSc, MNSc, RNKrista Meinersmann, PhD, RN
Jennifer Kelley, BS, RNHelen Peake-Godin, MN, RN
MPNEP 22 May 2012

Maine Medical CenterUniversity of Southern Maine

Shared vision statement
Through academic and practice partnership, we develop innovative, high quality and sustainable models of nursing education and practice to meet the community’s need for nursing.

Work teams
Marketing and information Curriculum developmentResearchFaculty & clinical developmentUnit/staff development

What we had to listen … and learn about
Administrative clarityWork loadUnion academic workforce and non-
union hospital nursing staffFull-time nursing staff become part- time
clinical teachers and continue to work as staff RNs
Educational differencesCurrent practices
Proposal
Create a project that develops a collaborative learning and teaching model of clinical nursing
Increase admission (24 students/yr) o first group admitted January 2011o second group admitted May 2012
Conduct a 3 year longitudinal studyo Quantitative and qualitative research methods

Education transformation: What was different?
Teaching teams MMC practice and SON facultyKnowledge, Know-how, and Formation focusDeliberate clinical/classroom connection
Clinical faculty embedded in classroomClinical immersion began in Physical Assessment and
Fundamentals coursesEarlier entry into acute care setting
Cohort groups—same clinical groups throughout
Increased use of simulation

Focus group
What was it like teaching in the pilot last semester? Tell us a story about your experience.
What contributions or hindrances did you find with the students coming to the course as a CNA?
Tell the group about a challenge you had in teaching last semester.
Describe a moment of inspiration from the past semester.
What was different this semester from other semesters you’ve taught (not in the pilot program)?

Team
It was a great team, and I know we started off crazy, and trying to figure things out but I admire how you all came together, the clinical folks. Thank you, you really did a great job!

Teamwork
I was thinking…about teamwork, I think that it’s more fun and I can do more work actually…with a team. In other words, we encourage each other, bounce ideas off each other. When someone with creative ideas…says, well let’s do it this way…I think what happens is that it enhances where I might stop, they would continue. My reaction [was] “oh dear, that sounds like a lot of work”… or how [are] we were going to do it, there’s that relationship of “yea we can do this.” And they have new ideas, so that was the fun part of it. So the work felt less heavy…but knowing that you have a team with you makes you a little more adventurous. It did for me.
Classroom/Clinical
What’s being taught may vary from what’s being practiced, so to kind of re-learn or continue learning, or refresh from the lecture portion,…it was great being in the classroom to know what the students are learning versus just being out there in the clinical field, you never have that connection. And having that connection was I think a huge benefit.

Doing well
For the first time doing it with this clinical group, usually this group has a large difference in their capabilities in being able to do certain tasks and their confidence was a lot more than students I’ve dealt with in the past. I found that they were taking on 2 patients by the middle of the semester if not a little bit more, and they were able to accomplish those tasks before the end of the day and they did really well.

—beyond expectationsFor instance, we did a lot of work on using SBAR and physician calling, and that’s usually something where new nurses struggle, calling the physician. I sat down with a student, and handed [her] the phone, and said, you tell me your concerns. They’re very good concerns, now let’s call the doctor, and [she was] like “uhhh…” so [she] took a moment and pulled [herself] together, but she called, and she called more beautifully than even an experienced nurse I’ve heard, and it was just like “Yes! That was great!” I had never been able to see a student do something that well before, communicating with a physician over the phone…
Inspirational
There’s a transgendered person who started on medications to become a woman. And she called me over, she said, “do you know how long it will take, now that I’ve started getting the medications, until I start feeling different”. And I said I have no idea. I asked [a] student, to talk with her…he got down on his knee in front of her and said, “I can look this up if you can wait just a few minutes, and she said okay”…then he sat down with her…she gave him the names …he found out what the onset would be…and I just kind of backed out of the situation…for some students, if they haven’t encountered somebody who’s transgendered or thinking about it…that could be very intimidating. It wasn’t at all for him. He was lovely with her.
FormationThe question on that last journal was about the notion of formation…we had structured the class [using] knowledge, know-how, and formation, and [I] asked them how their learning had advanced in those ways… and they talked about…the fact that they just thought they were going to come in, bing-bong, and walk out, and they’d be nurses. And then they realized that this was a process that would take them years to become a nurse….And so that was pretty profound, to hear that from students in their first semester.

Recommendations
CNA requirement. oAdmit to SON summer semester, take CNA, Pharm,
Patho, and transition courses. Pedagogical and curriculum changes Strong team development across content areas & semesters Faculty/nursing staff & unit orientation and development
oMasters prepared clinical teaching faculty requirement Project manager—faculty member
oRelease time Expand collaboration to include other practice agencies
oNeed to develop blueprint for replication

The qualitative research team

SON/MMC Collaborative Team Members
Maine Medical CenterMarjorie Wiggins Andria MoorePaula White Marty RiehleKristiina Hyrkas Geri Tamborelli Allie Haynes
University of Southern Maine School of NursingKrista Meinersmann Carla RandallLiz Elliott Helen Peake-GodinSu Sepples Janis Childs
New Graduate Nurse Orientation Utilizing H-Works Program
Maine General Rehabilitation & Nursing CareMary DiMascio RN,MSDirector of Nursing ServicesMay 22,2012

New Graduate Nurse Orientation Utilizing H-Works Program
• The goal was to identify missing information in our Gary Birch orientation and formalize the current system of new graduate orientation by February using the MGH evidence based H-Works program.
• We sought to enhance the current in-house orientation for our new graduate R N’s transitioning from student to nurse, knowing that learning multiple new responsibilities can be stressful.
• Our 5 new RN’s were signed up with a partner over several months to attend the 2 day hospital orientation with other new RN’s within the MGH system.

PROJECT GOALS
• Goal #1 To include Gray Birch new RN’s into the appropriate topics on given dates in a classroom setting at MGH –IV’s, anticoagulant therapy - goal met
• Goal #2 To hold regular support group meetings –goal met
• To have regular meetings with the nurse manager checking in on “how is it going?” – goal met; ongoing
• To have the new RN graduates meet each other in the classroom and share their experiences - goal met
• Goal #3 Adopt the MGH preceptor certification course an evidence based practice and develop the program to be specific for Gary Birch to meet our cultures specific needs - This goal is in process
• Goal #4 Ongoing evaluations for the preceptor program at 6 months and 1 year – goal will follow #3

Nurse of the Future core competencies –Maine Gerontological Nursing Competencies
#3 Leadership – KNOWLEDGE: Recognize the leadership principles that support the older adult within a variety of healthcare environments – SKILLS: Apply principles of group process and team communication in working with older adult and/or caregiver – Apply leadership and management skills to improve safety for older adults including , but not limited to polypharmacy, fall reduction, elder abuse, and home safety – ATTITUDES: Value the older adults as a contributing member of society.
#7 Teamwork and Collaboration – KNOWLEDGE: Identify importance of interdisciplinary team in caring for older adult. SKILLS: Demonstrate ability to provide supportive communication for an older adult during transitions of care. ATTITUDES: Value the importance of the interdisciplinary team in helping an older adult or their caregiver

New RN feedback & change recommendations
• As a new grad, it was terrifying yet exciting to work on my own
• Making the transition was a big step, not knowing what to expect
• How would I handle all these patients when in school I only had 3 it was scary
• Thankfully everyone was very welcoming, not one person told me “no” when I asked for help, this put me at ease
• With my schooling and MGRNC my skills have become more developed ,now I feel comfortable maintaining IV’s,trach care, dressings, wound vacs, pic line blood draws, feeding tubes and many other things.
• I heard about places where “nurses eat their young” but at MGRNC the “ nurses nurture their young”
• The 2 day of hospital orientation gave me some good ideas one was to implement at Gray Birch a C N A handoff with a paper tool
• Changes to orientation could be eliminating watching videos for 2 days, sticking to the orientation checklist some nurses were too busy to sign off.
• It was a good experience• I hope other new nurses can benefit
from working a MGRNC
• CHANGES: Hospital implemented a new orientation process. Gray Birch will revisit the orientation checklist process

New RN feedback & change recommendations
• The learning curve for a new grad is something unique, special and personal for each grad depending on schooling, C N A experience and life learning
• I will always remember that key phrase “ You don’t know what you don’t know” and opportunities to learn come up every shift and with every patient.
• I have unconditional support• Every nurse manager, nurse, C N A,
supervisor was willing to step in and assist my in my journey
• I feel I have the confidence to be that patient advocate
• Answer questions, perform tasks as a functioning nurse and provide complete care.


CONCLUSION
• New graduate RN’s were willing to be open and share honestly during the support group meetings
• They voiced that there was value in the meetings and a safe place to express feelings
• They also found value in attending the 2 day MGH class/hands on sessions. Some information was new and some topics provided reinforcement of skills
• 2 of the 5 new graduate RN’s moved on, one relocation closer to their home and one stayed within the MGH system taking a position in acute care.

Next Steps
• We will continue on with sending new graduate RN’s to the 2 day orientation utilizing H-Works
• Suggested adjustments would be to incorporate the Maine Gerontological Nursing Competencies into the H-Works program

Maine General Rehabilitation & Nursing Care at Gary Birch
We thank you for this opportunity !
Central Maine Medical Center
CENTRAL MAINE MEDICAL CENTER NEW GRADUATE NURSE ORIENTATION PROGRAM FOR ICU
Mary Philbrick BSN, RN,CCRNCentral Maine Medical Center, Lewiston, Maine

Brief overview
• After reviewing in 2011 the new graduate orientation process at CMMC, there was a need for improvement and we identified many of the same gaps that are listed in the competencies mentioned from the MPNEP
• CMMC was excited for the opportunity to create a more effective program that utilizes a novice to expert model and mentor philosophy that can help shape our newly hired ICU graduate nurses into future nurse leaders.

Goal
• To standardize orientation process through phases and to establish this program throughout the corporation for all new graduate nurses and utilize the best methods of training that are needed to help nurses practice at the highest standard of quality, safe and holistic patient care.
Core Competencies
• Improve communication skills
• Augment critical thinking skills towards clinical reasoning
• Focus on patient quality and safety
• Gain knowledge and skills in phases
• Collaboration in the healthcare team
• Partnership = Shared responsibility in orientating new staff
• Encourage new staff to be engaged and accountable
• Reduce turnover & enhance job satisfaction
Other key activities
• Focus on novice to expert model• Standardized preceptor training• Mentoring from other disciplines - partnerships• Improve efficiency of training – road map• Decrease length of orientation

ICU New Grad Phased Orientation for assignments:
Phase Time for each Phase - estimated
Assignment for the orientee
Examples of goals and focus
1 4 weeks 1 ICU patient in stable condition Basic patient care, assessment skills charting, unit organization and time management, prioritization and communication. Work with a CCT if applicable. SEE GOAL SHEET.
2 4 weeks 1 ICU patient in stable condition and one non - ICU patient
Review rhythms, monitors, crash carts, plums, pacemakers, level one and other equipment. Rounds presentation and case reviews with educator. SEE GOAL SHEET
3 4 weeks 2 ICU patients one unstable and one stable
Review drips, hemodynamic, ICP, ventilator and VAC equipment. Review assessment skills & ABG’s. Work with RT, Intensivists or Cardiologist. Focus on other tools for communication and safety. SEE GOAL SHEET
4 4 weeks 1 highest acuity ICU patient Review Hypothermia CCO/SVO2, Intubation CRRT, IABP equipment waveform analysis. Work with RT, Intensivists or Cardiologist. as well as continue the focus on communication with PI, best practice etc. hypothermia. SEE GOAL SHEET
5 4-6 weeks 1 high acuity and one ICU patient Review Organ Donation, Pediatrics, time management, organizational skills and critical thinking. Work with Intensivists or Cardiologist if not done earlier. Work with Coordinator & Pediatric RN. SEE GOAL SHEET
Outcomes
• 5 new graduate ICU RN’s– All 5 completed orientation in 6-8 months– Prior 2 years orientation this was 8-10 months– Mixed results with preceptors in utilizing new
tools– 5 ICU staff received preceptor training – Standardized preceptor program developed

Outcomes continued
• New graduate nurse survey:– All 5 new staff felt the program phases were
beneficial in moving them through orientation– 2 - 3 new staff felt the preceptors utilized the
phases through the orientation– 4 - 5 new staff believed their orientation brought
them to a proficient/competent level– Over all program rating “good” on a scale of poor,
fair, good excellent)

Recommendations
– ICU leadership and preceptors survey pending– Job satisfaction survey pending
• Need leadership & preceptor buy in• Needed more education on the process for
those who make assignments

Summary
• New staff felt it created a solid foundation in application of concepts and clinical experience.
• Improved time management skills • Small successes – new staff satisfaction• Change is hard – seasoned preceptors
resistant
Strengthening the Preparation of Psychiatric Charge Nurses
Beth Clark, PhD, RNCLisa Hussey, BAGwyneth Mattingly, BSN, RNCConnie Sprague, MSN, RN

Problem Statement: Undergraduate leadership courses are usually based on a medical rather than a psychiatric model of care. They do not address the unique issues faced by psychiatric charge nurses such as milieu management and working closely with the interdisciplinary team. With a focus on process and relationship rather than skills, the psychiatric role is often ambiguous for students. They may not be aware of the unique challenges and rewards of psychiatric nursing.

Goals of the ProjectPrimary Goals:
• Strengthen the skills, role, and identity of psychiatric charge nurses
• Promote excellence in nursing care
• Provide a positive and effective learning environment for nursing students.
Secondary Goals:• Develop new leaders who will
promote a positive image of psychiatric nursing
• Improve psychiatric nurse satisfactions and retention
• Promote stronger collaboration between education and service
• Encourage students to consider psychiatric nursing as a challenging and rewarding career option

Nurse of the Future Competencies:
• Leadership• Teamwork and
Collaboration• Quality Improvement • Professionalism

Project Design• Needs assessment with nurse managers and
members of leadership team• Literature review• Create curriculum• Develop pre and post assessment• Implement training• Evaluate• Extend training to other leaders• Group mentoring and support

Outcomes• All participants either agreed or strongly agreed that:
– the faculty were knowledgeable– the stated educational objectives were met– the program met their personal objectives
• Participants were able to identify key ideas that they will use in their practices
• Post-test scores went up on 87% of the items and went down on just one item (2%)
• 50 % of eligible nurses have now received training

Reported Areas of Greatest Growth in Pre and Post-test Scores:
• giving timely, relevant, and objective feedback• participating in strategic planning and quality initiatives• utilizing research findings to establish standards,
practices, and patient care models• creating environment of open communication & sharing• applying components of crucial conversations• eliminating workplace violence & sexual abuse• Monitoring clinical activities to identify both expected
and unexpected risks.

Participant Comments“The Charge Nurse role challenges each of us daily and with this training we are better able to provide stability, leadership, and guidance to the staff providing exceptional patient care”
“This is a program with long life and will benefit many”
“Outstanding!!!”
“I found the Charge Nurse Leadership Orientation to reinforce my previous knowledge as well as motivate me to be a better leader.”

Nursing Student and Faculty Comments
• Student site evaluations for Acadia are highly positive
• Students felt welcomed and supported during their rotation
• Faculty appreciated the opportunity to work closely with the staff at Acadia and hope this kind of collaboration will continue.

Themes of Follow-upMentor/Support Meeting:
• Challenge of managing the milieu-particularly around staffing issues and sick calls
• Appreciation for an hour off the unit to share concerns and frustrations. “Sometimes we feel isolated in our own little silos." It is good to feel the peer support.
• How to supervise without being drawn into staffing or patient problems that staff should be addressing
• How to best support each other and know what is happening on other units
• How to manage charge nurse responsibilities with everything else that needs to be done

Future Plans
• Permanent charge nurses will complete the full two days of training; all inpatient and outpatient RNs will complete the one day leadership section – 50% complete – target completion for July 1, 2012
• Revise curriculum based on feedback from participants
• Continue mentoring and support group in the fall• Complete 6 month and 1 year follow-up evaluations