An Inherited Molecular Lesion of Erythrocyte Pyruvate...
18
An Inherited Molecular Lesion of Erythrocyte Pyruvate Kinase IDENTIFICATION OF A KINETICALLY ABERRANT ISOZYME ASSOCIATED WITH PREMATURE HEMOLYSIS DONALD E. PAGLIA, WILLIAM N. VALENIrNE, MARjoRIE A. BAUGHAN, DENs R. MEILR, CLAUDE F. REED, and 0. Ross McINTymE From the Departments of Medicine and Pathology, University of California Los Angeles School of Medicine, Los Angeles, California 90024, and the Veterans Administration Center, Los Angeles, California 90073; the Depart- ments of Pediatrics and Internal Medicine, University of Rochester School of Medicine and Strong Memorial Hospital, Rochester, New York 14620; and the Department of Medicine, Dartmouth Medical School, Hanover, New Hampshire 03755 A B S T RA C T Atypical cases of heritable hemo- lytic anemia have been noted that conform clini- cally and biochemically to anemias of the pyruvate- kinase (PK)-deficient type, except for the presence of apparently adequate quantities of erythrocyte-PK activity by the usual assay pro- cedure. Investigations of four such anomalous cases, occurring in two unrelated families, are presented. Erythrocytes contained a kinetically aberrant isozyme of pyruvate kinase (PK2). Michaelis constants for the pathologic isozyme relative to phosphoenolpyruvate were over 10-fold greater than control values, but no kinetic abnor- mality was evident for the second substrate, adeno- sine diphosphate. PK2 exhibited a pH optimum almost 1 U lower than the wild enzyme form (PK1). Significant differences were also evident in the functional stabilities of the isozymes. Leuko- cytes were unaffected. Family studies revealed paternal heterozygosity for quantitative PK deficiency of the usual type. Clinically normal maternal relatives and some This study was abstracted in Blood, December 1967, 30: 881. Dr. 0. Ross\ McIntyre is a Markle scholar in aca- demic medicine. Received for publication 29 January 1968 and in re- 7Ased form 15 April 1968. siblings demonstrated intermediate deviations in erythrocyte-PK kinetics and reaction character- istics compatible with coexistence of normal PK1 and kinetically abnormal PK2. Hemolytic anemia in the propositi appeared to require simultaneous inheritance of the gene governing PK2 production and its presumed allele resulting in quantitative PK deficiency. Both genetic defects were traced through three generations, the defective gene in both instances apparently resident on autosomes. A revision of the PK assay technique is sug- gested, since catalytic inefficiency of PK2 was manifested only at low substrate concentrations and was therefore undetectable at the relatively high phosphoenolpyruvate levels employed in the conventional assay. INTRODUCTION Over 100 documented cases (1, 2) of hemolytic anemia associated with hereditary deficiency of erythrocyte pyruvate kinase (PK) have appeared in the world literature since the original descrip- tion in 1961 (3). A pattern of clinical and labora- tory features has evolved from these studies which partially characterizes this inborn error of erythro- cyte metabolism (4, 5). The Journal of Clinical Investigation Volume 47 1968 1929
Transcript of An Inherited Molecular Lesion of Erythrocyte Pyruvate...

An Inherited Molecular Lesion
of Erythrocyte Pyruvate Kinase
IDENTIFICATION OF A KINETICALLY ABERRANT
ISOZYME ASSOCIATEDWITH PREMATUREHEMOLYSIS
DONALDE. PAGLIA, WILLIAM N. VALENIrNE, MARjoRIE A. BAUGHAN,DENsR. MEILR, CLAUDEF. REED, and 0. Ross McINTymE
From the Departments of Medicine and Pathology, University of CaliforniaLos Angeles School of Medicine, Los Angeles, California 90024, and theVeterans Administration Center, Los Angeles, California 90073; the Depart-ments of Pediatrics and Internal Medicine, University of Rochester Schoolof Medicine and Strong Memorial Hospital, Rochester, NewYork 14620;and the Department of Medicine, Dartmouth Medical School,Hanover, NewHampshire 03755
A B S T RAC T Atypical cases of heritable hemo-lytic anemia have been noted that conform clini-cally and biochemically to anemias of the pyruvate-kinase (PK)-deficient type, except for thepresence of apparently adequate quantities oferythrocyte-PK activity by the usual assay pro-cedure. Investigations of four such anomalouscases, occurring in two unrelated families, arepresented. Erythrocytes contained a kineticallyaberrant isozyme of pyruvate kinase (PK2).Michaelis constants for the pathologic isozymerelative to phosphoenolpyruvate were over 10-foldgreater than control values, but no kinetic abnor-mality was evident for the second substrate, adeno-sine diphosphate. PK2 exhibited a pH optimumalmost 1 U lower than the wild enzyme form(PK1). Significant differences were also evidentin the functional stabilities of the isozymes. Leuko-cytes were unaffected.
Family studies revealed paternal heterozygosityfor quantitative PK deficiency of the usual type.Clinically normal maternal relatives and some
This study was abstracted in Blood, December 1967, 30:881.
Dr. 0. Ross\ McIntyre is a Markle scholar in aca-
demic medicine.Received for publication 29 January 1968 and in re-
7Ased form 15 April 1968.
siblings demonstrated intermediate deviations inerythrocyte-PK kinetics and reaction character-istics compatible with coexistence of normal PK1and kinetically abnormal PK2. Hemolytic anemiain the propositi appeared to require simultaneousinheritance of the gene governing PK2 productionand its presumed allele resulting in quantitativePK deficiency. Both genetic defects were tracedthrough three generations, the defective gene inboth instances apparently resident on autosomes.
A revision of the PK assay technique is sug-gested, since catalytic inefficiency of PK2 wasmanifested only at low substrate concentrationsand was therefore undetectable at the relativelyhigh phosphoenolpyruvate levels employed in theconventional assay.
INTRODUCTION
Over 100 documented cases (1, 2) of hemolyticanemia associated with hereditary deficiency oferythrocyte pyruvate kinase (PK) have appearedin the world literature since the original descrip-tion in 1961 (3). A pattern of clinical and labora-tory features has evolved from these studies whichpartially characterizes this inborn error of erythro-cyte metabolism (4, 5).
The Journal of Clinical Investigation Volume 47 1968 1929

A closely related group of patients has beenobserved in this laboratory and elsewhere whichpresents a diagnostic dilemma. Because they sowell conform to the accepted criteria, they are sus-pect as PK-deficiency problems, yet quantitativeassays by conventional methods consistently fail todetect significant reductions in erythrocyte enzymelevels and, indeed, PK activity is occasionallygreater than in normal cells. These findings havesuggested the possible existence of an anomalouskinetic form of PK.
The present report describes four such atypicalcases of severe hemolytic anemia occurring in twounrelated families. Erythrocyte PK activity in thepropositi, adequate by the usual laboratory assaytechniques, was found to, have anomalous kineticswith markedly reduced catalytic rates at low -con-centrations of its substrate, phosphoenolpyruvate(PEP). Inhibitors were not demonstrable, andkinetics dependent upon the second substrate,adenosine diphosphate (ADP), were normal.Clinical expression appeared to be contingent uponsimultaneous inheritance of a gene causing defi-ciency of the usual molecular species of PK (heredesignated PK1), and a gene governing productionof the pathologic isozyme (here designated PK2).Both genetic defects were traced through threegenerations, the defective genes apparently re-siding on autosomes. Qualitative studies estab-lished further distinctions between the isozymes,most notably in regard to pH dependency andfunctional stabilities.
METHODS
SubjectsKindred G included three affected siblings. 11-yr old
propositus 1, a Caucasian male and the eldest child,was noted to be jaundiced shortly after birth withoutevidence of fetomaternal incompatibilities. Jaundice per-sisted for 1 1 months, but exchange transfusion was notdeemed necessary. Intermittent episodes of icterus, pal-lor, and dark urine that lasted 1-3 wk were noted at age 6months and recurred every 2 wk-2 months. Upper res-piratory infections were associated with symptom exacer-bations. He was hospitalized initially in January 1960,at 414, yr of age, with marked pallor, icterus, and hepato-splenomegaly. Laboratory studies included a reticulocytecount of 11.41%, negative antiglobulin, acid-hemolysis,and Donath-Landsteiner tests, normal levels of red-cellglutathione, and glucose-6-phosphate dehydrogenase ac-tivity, normal erythrocyte' osmotic fragility, and aDacie type-II autohemolysis pattern.
A diagnosis of congenital nonspherocytic hemolyticanemia was made, and during the next 3 yr transfusionswere required every 4-6 months. In January 1964, sple-nectomy was performed after "chromium cell-survivalstudies demonstrated splenic sequestration and a to of20 days (normal, 27-36 days). The gall bladder containednumerous small stones, but a liver biopsy was normal.The spleen was enlarged (340 g) but microscopicallyshowed only dilated congested sinusoids. Since surgery,the patient has not required further transfusions and hasmaintained hemoglobin between 9 and 10 g/100 ml withreticulocytosis of 10-25%o. He has remained fully activeand asymptomatic.
Propositus 2, a 7 yr old female, was not jaundicedduring the neonatal period but has always been pale withminimally icteric sclerae. She never required transfusionand has maintained hemoglobin levels between 9 and 10g/100 ml with reticulocytosis of 5-12%. The spleen wasenlarged, extending 3-4 cm below the costal margin.
Except for slight pallor, 3-yr old female propositus 3was well until 17 months of age, when icterus, lethargy,fever, and splenomegaly were noted. The packed cell vol-ume at that time was 15%, and results of autohemolysis,osmotic fragility and other peripheral blood studies weresimilar to those of her older brother. Transfusions every4-6 months have maintained her packed cell volume be-tween 21 and 31%.
The fourth sibling, a 9 yr old female, and the parentsand grandparents have been clinically and hematologicallynormal. There is no known consanguinity. The father isof English-Welsh descent, although the surname mayhave Norman origins. The mother is of northern Ger-man and English ancestry. The family has lived in up-per New Yprk State since the early 19th century, andall living members reside within a radius of 50 miles.
Kindred D contained one affected child. Propositus 4,a 16 yr old Caucasian male, was the product of a normalpregnancy and delivery but was jaundiced at birth. Al-though investigations for blood-group incompatibilitieswere negative, an exchange transfusion was performed.The patient remained chronically anemic thereafter withsplenomegaly, reticulocytosis, and elevated serum bili-rubin. Spherocytes were not evident in peripheral bloodsmears, and the incubated red-cell fragility test wasnormal. Jaundice fluctuated, being transiently worse withviral infections, but transfusions were never required.
For several years he had occasional bouts of vagueright upper abdominal pain lasting several days. Initialcholecystograms were negative, but gallstones were notedon films taken in October 1966. Elective cholecystectomyand splenectomy were performed 2' months later. Pre-operative physical examination was unremarkable ex-cept for jaundice and a firm spleen palpable 6 cm belowthe costal margin. Total serum bilirubin was 8.6 mg/100ml (normal, 0-1.0 mg/100 ml) of which 0.7 mg/100 mlwas direct reacting (normal, 04.25 mg/100 ml), and thereticulocyte count was 9.3%. Gallstones were presentin the cystic duct and gall bladder. Commonduct explora-tion was carried out, and a 973 g spleen was removed.
There was a pronounced postoperative drop in total
1930 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

serum bilirubin to 1.2 mg/100 ml (0.4 mg/100 ml directreacting) and a rise in the reticulocyte count to a maxi-mum of 25%. Reticulocytes gradually declined to pre-operative levels, and hemoglobin values rose to 13 g/100ml 2-3 months after surgery. This was not sustained andby the 6th postoperative month, serum bilirubin hadagain risen to values approaching preoperative levels.His condition has since remained stable and transfusionshave not been necessary.
The parents, both of English extraction, and two malesiblings were clinically normal. None of the maternalor paternal relatives was known to be affected. There wasno consanguinity nor known relationship to kindred G.
ProceduresRoutine hematologic studies were performed by stand-
ard methods (6). Autohemolysis of sterile defibrinatedblood incubated at 370C was determined by the Selwyn-Dacie technique (7) as modified by Young, Izzo, Altman,and Swisher (8). Osmotic fragility was measured bythe method of Shen, Ham, and Fleming (9) accordingto the modification of Young et al. (8). Determinationof erythrocyte 2,3-diphosphoglycerate (2,3-DPG) wasperformed according to Bartlett (10). Methods for themeasurement of glucose utilization, lactate production,and ATP stability have been detailed in a previous re-port (11).
Enzyme activities in erythrocytes and leukocytes weredetermined on homogenates of saline-washed cells sepa-rated by sedimentation in polyvinylpyrrolidone-citrateand counted in quadruplicate as described previously (12).Pyruvate kinase was assayed by a modification of themethod of Bucher and Pfleiderer (13), which has beendetailed in earlier reports (12, 14). All values forerythrocyte PK were corrected for reagent-blank ac-tivities as well as for PK contributions by contaminatingleukocytes on the basis of simultaneous assays per-formed on washed leukocyte suspensions. In all experi-ments white-cell corrections were less than 10% of ob-served activity maxima. Reagent-blank activities havebeen found to be virtually negligible when the assay sys-tem exclusively employed crystalline rabbit-muscle lac-tate dehydrogenase 1 with less than 0.003% contaminatingPK activity.
Assay procedures as reported elsewhere were also per-formed for hexokinase, glucosephosphate isomerase, phos-phofructokinase, fructosediphosphate aldolase, glyceral-dehyde-3-phosphate dehydrogenase, triosephosphate iso-merase, phosphoglycerate kinase, phosphoglyceromu-tase, phosphopyruvate hydratase (enolase), lactatedehydrogenase, glucose-6-phosphate dehydrogenase (G-6-PD), phosphogluconic dehydrogenase, glutathione sta-bility, glutathione reductase, glutathione peroxidase,glyoxalase, and other combined enzymes of the terminalpentose-phosphate pathway (15-19).
Excepting glyoxalase determinations and the 20°C as-
say temperature for glutathione peroxidase, all spectro-photometric assays were performed at 370C by following
1 A grade. Calbiochem, Los Angeles, Calif.
pyridine nucleotide absorbance changes at 340 mu in aBeckman DU Spectrophotometer, model 2400, coupled toa model 2000 Gilford Multiple-Sample absorbance re-corder. Enzyme units (EU) were defined as the num-ber of micromoles of pyridine nucleotide converted perminute by 1010 cells and were calculated on the basis ofa molar absorptivity of 6.22 X 10-3 at that wave length(20).
Michaelis constants (Kin) were determined by simul-taneous analyses of erythrocyte and leukocyte PK ac-tivities in the standard assay systems at 12-16 concen-trations of substrate varying between 0.01 and 9.0 mmoles/liter for PEP and between 0.05 and 2.0 mmoles/liter forADP. Final pH in the reaction system was 6.9 ± 0.1.Variations in PEP levels were performed at a constantADP concentration, 0.4 mmole/liter, whereas studies onthe effect of ADP variations were conducted at 1.5 mMPEP. Potassium and magnesium concentrations wereheld constant at 75.0 and 8.0 mmoles/liter, respectively,and Km for these ions was not determined. Correctionswere always made for reagent-blank activities deter-mined at each substrate concentration. These were foundto be relatively independent of substrate levels, varyingby no more than plus or minus 50% of the very smallstandard-assay reagent-blank correction. Additionally,erythrocyte PK activities were corrected for contamina-tion with leukocyte PK on the basis of concurrent white-cell assays at each concentration of PEP and ADP.Substrate concentrations coinciding with half-maximalPK activities were taken directly from best-fit linearcoordinate curves, which defined Km with greater re-producibility than did extrapolations of double-reciprocalLineweaver-Burk plots.
RESULTS
Hematologic studies. Table I presents resultsof standard hematologic measurements on immedi-ate family members obtained at times of enzymeanalyses and averaged over the 1 yr study period.Whereas the propositi exhibited moderate tomarked anemia, at least one sibling and bothparents in each family appeared normal by con-ventional criteria, excepting perhaps the motherin kindred G who showed progressive signs ofmild anemia as she entered the third trimester ofher 5th pregnancy. Leukocyte values ranged withinnormal limits in all family members studied.
Red-cell morphologic abnormalities were quali-tatively comparable among all four propositi anddid not vary significantly from the nonspecificchanges usually seen in congenital nonspherocytichemolytic anemias. Slight anisocytosis and poi-kilocytosis with moderate polychromatophilia andmacrocytosis were common features. The latterwas reflected by slight alterations in red-cell
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase ].931

Kindred GPropositus I
(III-6)*
Propositus 2(111-4)
Propositfus 31(111-3)Repeat
Sister(III-5)
Mother(11-12)
Father(II-11)
Kindred DPropositus 4
(111-1)Brother
(111-2)Brother
(111-3)Mother
(11-3)Father
(11-2)Normal meanNormal range
TABLE I
Mean Peripheral Red-Cell Values and Autohemolysis Data
Autohemolysis
Additive
Reticulo- Glucose, Adenosine. ATP,Hb PCV RBC cytes None 0.026 M 0.018 M 0.021 M
g/1OO ml % X 10/ % %cmm
8.8 28 2.67
9.4 30 3.21
9.6 31 3.74
6.8
14.3
11.4
15.6
21
44
2.60
35 3.79
48 5.18
11.1 34 3.14
17.8 6.0 3.5 2.0 1.0
6.8 3.5 3.0 2.0 0.7
4.4 6.5 5.5 2.0
11.4
0.5 0.8 0.1 0.2
1.4 2.3 0.3 0.3
0.3 1.0 0.2 0.3
18.9 6.9 3.2 0.7
13.1 39 4.51 1.2
13.2
13.5
40 4.63
41 4.30
14.1 43 4.74
0.5
1.1 0.9 0.2 0.4
0.7
1.7 0.2 0.2 0.20-3.5 0-0.5 0-1.0 0-1.0
* Genealogic designation according to Fig. 6.1 Specimen obtained 10 days after transfusion. Repeat specimen obtained 2.5 months later.
indices. Variable numbers of irregularly con-tracted and fragmented cells were present alongwith occasional target cells. Spherocytes were notevident, and platelets always appeared adequate inquantity. Stained films of peripheral blood anderythrocyte indices from the parents and unaffectedsiblings appeared normal, again with the exceptionof the pregnant mother in kindred G, who showedchanges compatible with slight hypochromic, nor-mocytic anemia.
Osmotic fragility of fresh erythrocytes was
either normal or slightly decreased in all casesstudied, and the propositi were indistinguishableon this basis from other family members. Pre-incubation of blood for 24 hr at 370C effectedsome deviation from normal fragility patterns.Onset of propositus-cell hemolysis was either nor-mal (two cases) or occurred at saline concentra-tions slightly higher than usual (two cases), butthe majority of these cell populations showed sub-stantial resistance to osmotic lysis, a characteristicshared by the mother in kindred G. In other family
1932 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

members the patterns of incubated-cell osmoticfragilities were either normal or indicative ofslightly increased resistance to osmotic disruption.
Studies on the effectiveness of erythrocyte gly-colysis. Autohemolysis of sterile defibrinatedblood from the propositi was slightly or moder-ately increased after 48-hr incubation at 370C.Table I shows the extent of this in vitro abnor-mality and the relative ineffectiveness of glucoseand adenosine as corrective agents. In the presenceof neutralized ATP, autohemolysis was restoredto normal levels in the three cases tested. Thesefindings conformed to the Selwyn-Dacie type-IIdesignation (7), the autohemolysis pattern com-monly noted in quantitative PK deficiencies.
Measurements of glucose utilization and lactateproduction by red cells of kindred G are presented
in Table II. The proband generally showed varia-ble increases in both parameters, most likely re-flecting the increased metabolic rates of young cellpopulations. The ratio of lactate production toglucose consumption, more reliable for compara-tive purposes than either value alone, was in eachcase within the range of normals.
Erythrocyte ATP stabilities over a 3 hr incuba-tion period are also recorded in Table II for threepropositi and their close relatives. Except for thesplenectomized patient, propositus 1, who showeda 37% loss of ATP (over a 4 hr period), all wereconsidered to be within normal limits. Additionalstudies on propositus 3 were expanded to includeincubations up to 6 hr. Under these circumstances,intracellular ATP decreased 9.5, 23.5, and 36.3%oafter 2, 4, and 6 hr, respectively, indicating that
TABLE I IMetabolic Studies on Erythrocytes of the Propositi and Various Relatives
ATP levelsGlucose Lactate Lactate/
utilization production glucose ratio Initial Final* %7 Change 2, 3-DPG
jumoles/ml RBC/hr pmoles/ml RBC pmoies P/miRBC
Kindred GPropositus 1 2.61 4.87 1.86 1.67 1.05 -37 16.6
(II1-6)$Propositus 2 3.47 4.15 1.46 0.98 0.98 0 11.3
(III-4)
Propositus 3 4.96 6.83 1.38 1.37 1.32 - 3.6 18.2(I 11-3)
Sister 2.66 5.17 1.94 1.60 1.48 - 7.1 8.9(1III-5)
Mother 2.60 3.30 1.27 0.91 0.87 - 4.8 12.5(II-12)
Father 2.57 5.01 1.95 1.21 1.26 + 4.1 10.9(II-11)
Maternal Grandmother 2.66 5.06 1.90 1.44 1.48 + 2.4 11.8(1-6)
Maternal Grandfather 1.95 2.63 1.38 0.89 0.97 + 9.1 11.9(I-5)
Paternal Grandmother 2.60 4.02 1.42 1.63 1.50 - 7.8 8.8(1-4)
Kindred DPropositus 4 20.2
(III-1)
Normal range 1.57-2.23 2.37-3.91 1.49-2.11 1.15-1.67 1.28-1.50 ±i10.0 7.0-11.0
* Incubation time was 3 hr for all cases except propositus 1, which was 4 hr.t Genealogic designation according to Fig. 6.
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase 1933

TABLE II ISummary of PK Determinations on Propositi and Immedsate Families by Standard Assay Technique
Employing 1.5 mMPEP
Mean PK activity (EU)*
RBC WBC Reticulocytes
Normal mean and SDHeterozygous PK-deficiency rangeHomozygous PK-deficiency range
Kindred GPropositus 1
(I11-6)-Propositus 2
(III-4)Propositus 3§
(I1--3)Repeat
Sister(I11-5)
Mother(11-12)
Father(II-11)
Kindred DPropositus 4
(111-1)Brother
(111-2)Brother
(III-3)
Mother(11-3)
Father(11-2)
2.74 (0.47)0.6-1.750.0-0.47
3.14
1.69
1.44
1.25
2.73
2.27
1.68
2.60
1.79
2.06
1.96
1.75
1,373 (222)
1,197
1,217
22.6
5.5
713 4.4
11.40.4878
1,256 1.1
1,342
1,521
869
0.5
21.3
1.2
928 1.2
1,079 1.1
1,251 0.7
* Each PK value reported for erythrocytes is the mean of two to five determinations on each of two to four separatespecimens. Leukocyte values are single determinations.t Genealogic designation according to Fig. 6.§ Specimen obtained 10 days after transfusion. Repeat specimen obtained 2.5 months later.
ATP instability might be manifested only afterprolonged incubations.
Absolute amounts of cellular ATP were dimin-ished in one propositus and perhaps in the othersas well, when compared with the values usuallyfound in reticulocytes and young cells. Threepropositi showed prominent elevations in erythro-cyte 2,3-DPG, which suggested a metabolic im-pairment in terminal glycolysis.
Cellular enzyme assays. In no instance was anerythrocyte or leukocyte enzyme other than PK
found to be quantitatively deficient in the pro-positi or their families. Assay values of the glyco-lytic, pentose-shunt, and other erythrocyte en-zymes enumerated in the Procedures section, inMethods, were uniformly normal or elevated com-mensurate with the degree of reticulocytosis.Erythrocyte G-6-PD levels in all propositi werealmost twice those of normal control values.
Repetitive erythrocyte-PK assays in these kin-dreds over a 1 yr period have been averaged inTable III. Even considering the increases sec-
1934 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

TABLE IVErythrocyte and Leukocyte PK Michaelis Constants for PEPand ADP
Michaelis-Menton constants
Erythrocyte PK Leukocyte PKGenealogic
Group Patient designation* PEP ADP PEP ADP
mmoles/liierKindred G
Propositus 1Repeat
Propositus 2Propositus 3t
Repeat
MotherMaternal UncleMaternal Grandfather
SisterFatherPaternal GrandmotherMaternal UncleMaternal AuntMaternal Grandmother
Kindred DPropositus 4
BrotherBrotherMotherMaternal UncleMaternal GrandfatherMaternal CousinMaternal Cousin
FatherMaternal GrandmotherMaternal CousinMaternal Cousin
Normal Controls
111-6
111-4111-3
11-1211-15
I-5
111-5II-11
1-411-1411-13
1-6
III-1
111-2111-3
11-311-4
1-3111-4111-6
II-21-4
111-5111-7
1.251.301.230.591.60
0.480.710.83
0.090.180.160.190.160.13
0.100.090.150.15
0.14
0.10
1.31 0.18
0.530.830.340.550.500.700.75
0.090.180.270.27
0.090.100.090.090.150.150.21
0.16
0.20
0.200.230.10
0.100.110.190.11
0.070.070.05
0.050.050.050.100.080.08
0.170.180.20
0.20
0.19
0.08 0.18
0.080.150.080.100.10
0.050.09
0.080.090.070.05
0.18
0.24
0.220.23
* According to Fig. 6.$ Specimen obtained 10 days after transfusion. Repeat specimen obtained 2.5 months later.
ondary to reticulocytosis, no propositus had PKactivities consistent with the usual homozygousdeficiency state, although two appeared to havevalues compatible with heterozygosity. Comparisonwith our laboratory norms indicated that the
father in each. kindred was heterozygous for theusual quantitative PK deficiency, an observation
supported by erythrocyte assays conducted onpaternal relatives in kindred G which revealedseven additional instances of heterozygosity ex-tending through three generations.
PK kinetic studies. Results.of Km determina-tions, summarized in Table IV, established threeclear patterns of erythrocyte-PK kinetic behavior.
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase
1
2
3
1
2
3
1935

Whereas there were no significant individualdeviations from normal controls in red-cell orleukocyte PK Km relative to ADP, marked differ-ences in Km for PEP were found in erythrocytesfrom the propositi and certain family members.These ranged from 1.2 to 1.6 mmoles/liter forproband cells (Table IV, group 1), reflecting atleast a 10-fold elevation over normal values.Studies with white-cell suspensions establishedthat this enzyme aberration was not shared byleukocytes.
Segregation into two distinct molecular speciesof erythrocyte PK on the basis of kinetic behaviorwas further supported by the occurrence in 10family members (Table IV, group 2) of kineticpatterns intermediate between the propositi andnormal controls, a finding postulated to representcoexistence of normal (PK1) and kineticallyabnormal (PK2) enzymes. In each kindred,the mother, maternal grandfather, and a mater-nal uncle demonstrated intermediate red-cell PKkinetics.
All paternal family members, in addition tosome maternal relatives, displayed normal PKkinetics whether or not the individual had absoluteerythrocyte activities indicative of a heterozygousPK-deficiency state on a quantitative basis (TableIV, group 3).
In Fig. 1, PK activity in propositus hemolysatesis shown as a function of PEP concentration, dem-onstrating markedly reduced catalysis at low sub-strate levels. At the PEP concentration usuallyemployed in PK assays (in this laboratory, 1.5mmoles/liter), erythrocyte PK activity of all pro-positi was normal or slightly subnormal. Km. cal-culations from these data, however, revealedmarked differences in kinetic behavior betweennormal and propositus enzyme.
To provide a common scale for comparativepurposes, the data in Fig. 1 were converted fromabsolute values to rate-of-change curves in Fig. 2describing the celerity of approach to maximumPK activities as substrate levels increased. Thesecurves designated the PEP concentrations atwhich varying fractions of maximal PK activityoccurred. Prominent slope differences, most pro-nounced in the initial segments, reflected the widevariations between the two isozymes in their de-pendencies upon substrate availability. For exam-ple, 75% maximal activity of the wild enzyme
-PROPOSITUS NO.
IUS-
TERH OZYGOUSPK-DEFICIENCY RANGE
OZYGOUS PK-DEFICIENCY RANGE
0 1, 3 4 5 6PEP CONCEN7TRAT7ON (mmoles/lifer)
FIGURE 1 Erythrocyte-PK kinetic curves for the pro-positi. Points on the reaction-velocity plateau are notshown for PEP concentrations above 6.0 mmoles/liter.The cross-hatched area describes typical kinetics fornormal-control erythrocyte PK. The abscissa arrow in-dicates the substrate level usually employed in the stand-ard PK assay system. The broken curve for propositus 3was derived from a posttransfusion specimen as noted inthe text.
form (PK1) occurred at PEP levels approximat-ing 0.2-0.3 mmole/liter, whereas 2.0-3.0 mmPEP was required to effect comparable activitywith the anomalous isozyme (PK2) presumablypresent in propositus cells. Similarly, PK1 cata-lyzed at over 70%o' of maximum capacity at aPEP concentration of 0.3 mmole/liter, whereasPK2 activity was less than 10% at the same sub-strate level. Substrate saturation of PK1 generallyoccurred between 0.5 and 1.5 mmPEP. WithPK2, concentrations of 4-9 mmPEP were re-quired for complete saturation. Comparison withthe kinetic curve of a control reticulocyte-richspecimen indicated that observed abnormalitieswere not simply a function of young cell popula-tions per se.
In Figs. 1 and 2, two curves are shown forpropositus 3, and similarly two Kmvalues for thispatient are recorded in Table IV. The first, re-flecting kinetic behavior directly intermediate be-tween normals and other propositi, were derivedfrom assays of a specimen obtained 10 days after
1936 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

..3......m~MPP~
PEP CONCENTRAF/ON (mmoles//if er)J
FIGURE 2 Propositus-PK kinetic curves normalized on the basis of maximumapparent activities. The shaded control range contains the mean of six repre-sentative normal controls, plus or minus two standard deviations. RC desig-nates the curve derived from a specimen obtained from an unrelated patientwith 31% reticulocytosis from another cause. At the half-maximal level,Michaelis constants may be read directly off the abscissa, and the value rangesare so noted. The broken curve for propositus 3 again represents kinetics ofthe posttransfusion specimen.
transfusion of normal whole blood. The patientpresented clinically as the most severely affectedof the proband yet displayed PK kinetics whichin 10 other subjects were known to be pheno-typically benign. Assays 2%2 months later, aftervirtually complete attrition of the transfused cells,yielded the second curve and Km. indicating thatthe original findings resulted from admixture ofpropositus and transfused normal erythrocytes.
Comparable in vitro studies were performed onmixtures of normal cells with equal numbers ofcells from propositus 1. Results of these experi-ments, shown in Fig. 3, indicated not only thatartificial cell mixtures could yield intermediatekinetic characteristics, but further that enzymeinhibition was not a primary mechanism in modi-fying the kinetics, since cell combinations behavedessentially as the sum of the isolated componentswithout apparent influence upon one another.
Rate-change curves derived in the same mannerfor other members of kindreds G and D are pre-sented in Figs. 4 and 5, respectively. Erythrocytesfrom paternal relatives yielded normal kinetic pat-terns whether or not the individual was hetero-zygous for quantitative PK deficiency. Directly
intermediate curves, similar to those noted forin vitro and transfusion mixtures of normal andproband cells, were demonstrated by the samesiblings and maternal relatives who had inter-mediate Km values (Table IV)., supporting thehypothesis that both PK1 and PK2 isozymes werepresent in these erythrocytes.
In view of the relative lability of PK prepara-tions and the sensitivity of Km (PEP) measure-ments to assay parameters, direct comparison withKm (PEP) values reported in the literature seemstenuous. Such constants for human erythrocytePK have been shown to vary with environmentalconcentrations of magnesium (21), monovalentcations (21), ATP (21), ADP (22), and withpH, and partial purification (23). Under com-parable conditions, however, there is good agree-ment among reported values and our determina-tions on normals (21, 23-25). Considerably lessvariation exists for reported Kmvalues relative toADP (22-28), and no distinction among our casescould be made on this basis.
With incidental exceptions (21, 22), kineticstudies on partially purified PK, usually fromrabbit skeletal muscle, have indicated that Km for
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase 1937

0_.8
0.7
0.6 701062:: 1.30 K E
CONTROL CELLS0.3 1 / ,/ *-. MIXED CELLS
g/-. PROPOSITUS CELLS
R 0,1, X .... .... \ XXv0 0.5 1.0 1.5 2.0 2.5
PEP CONCENTRATION (mmoles/li/er)
FIGuRE 3 PK kinetic curve for mixture of normal erythrocytes with equalnumbers from propositus 1. Solid curves describe the kinetics for the individualcomponents of the cell mixture.
either PEP or ADP was independent of concen-tration of the other substrate (24, 27, 28). Thathuman erythrocyte PK may be unique in thisregard was suggested by the findings of Campos,
...
( 0.89~O. 8
0.6 7sf
.0.5 .09-0.21 0.48-0.83
W~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.. ...... ........0.4 I E-12 U-15 I-50.3 ,t fo.~~~~~~~~~~~~~~~~~~~~ ~~~~~~~~~~....... ...............
Zt / a ....... . . ..,,.
202
TtF / ...:PROPOSITUS RANGE
O I '-',,
<~~~~~~~~~~~~~~~~~~..oo . .. . .. ..
Koler, and Bigley (22), who demonstrated thateach Km was apparently a dependent variable ofthe second substrate's concentration. While thismay have been a function of the concentration
1.0 1.5 2.0
PEP CONCENTRATION(mmo/es//,ler)FIGURE 4 Erythrocyte-PK kinetic curves for kindred G. The range of all proposi-tus values from Fig. 2 is included in the heavily stippled area. Relatives are indi-vidually designated according to genealogic position as shown in Fig. 6. Normaland intermediate kinetic patterns are shown by solid and broken curves, re-spectively.
1938 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

GUN..ULMA..... ..... ...... :--:-.:..nD~CONTR(L.' "a:====_
08~~~~~~~~~~~~~~00.97 -i.g.......0.5 0.090.27 0.340.83 123.60 Km (mM P.EP
/ /7 f/-//f/
k 0~~~~~~~~~~~~~~~~~~~~~~~~~~........> ctw~
g 1 ~~~.../ ........o''W
I Si }/;i iS'o' ,,, ~~~~~~~~~~~~~~~~~~~~~...~04 I 1aZ /1/
8..8.wHe /B v ..........................................................
0.3 Ah ........
? ......%O. 2 2/ v/> ......~~~~~~~~~~~~~~~.. ... ..............
K 02o n{/. ..... -.PROPOSiTUS RANGE KINDRED~h.................
._, .................................................t~~~~~~~~~~~~~~0.4 ..::''.. \~~~~~~~......^ -an,~~~~~~~~~~.t................s0 0.5 1.0 1.5 2.0 2.5
PEP CONCENTfRATION(mmo/es/I,/er)FIGURE 5 Erythrocyte-P'K kinetic curves for kindred D. Value ranges and desig-
nations are the same as those indicated in Figs. 2 and 4.
ranges studied or the high magnesium-ion levelsemployed (21), these findings, if confirmed, wouldsuggest a mechanism of enzymatic conversion pos-sibly different from that suspected to prevail withPK from leukocvtes and other sources (24, 29).As suggested by the investigators, it would be ofparticular pertinence to consider this phenomenonin relation to studies with mutant enzyme formssuch as PK2. As yet, we have not been able toestablish whether this effect is demonstrable witheither PK1 or PK2 isozymes under our assayconditions.
Modification of the standard PK assay method.For the patient in each kindred initially studied(propositi 1 and 4), intersection of normal andpropositus activity curves in Fig. 1 occurred atPEP concentrations very close to that employedin the routine PK assay system, i.e., 1.5 mmPEP.Because of this fortuitous crossover, the in vitrotest for PK activity as performed in our laboratorywas unable to differentiate PK1 from PK2. Thetest procedure was subsequently modified by assay-ing hemolysates simultaneously at high and lowPEP concentrations, e.g., 1.5, or 2.0 and 0.3 or 0.4
TABLE VRatio of PK Activity at 0.4 mMPEP To That at 2.0 mAI PEP
Ratio of PK activities at 0.4 and 2.0 mMPEP
No. ofProposed determi-
Subject group genotype Mean Range nations
Propositi PKIAPK2 0.16 0-0.23 8
Relatives with intermediate PKLPK2 0.39 0.22-0.55 15PK kinetics
Relatives with heterozygous PK1PK1A 0.78 0.67-0.89 3PK deficiency
Relatives with normal PKLPKt 0.82 0.75-0.86 8PK kinetics
Normal controls PK1PK1 0.80 0.69-0.96 16
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase 1939

TABLE VIPK Activities in Mixtures of Propositus and
Normal-Control Erythrocytes
Relative proportions of PK activitycells in mixture (AA340 mM/10 min)*
Propositus Control 1.5 mM 0.3 mMcells cells PEP PEP
All 0 0.150 0.0305 1 0.150 0.0402 1 0.150 0.0501 1 0.150 0.0601 2 0.150 0.0701 5 0.140 0.0800 All 0.150 0.090
* Accuracy of reported values is + 10-1 5%.
mMPEP. With this revision, the distinction be-tween PK1 and PK2 was readily apparent. This isexemplified by data in Table V, showing resultsof modified PK assays on normal control andproband erythrocytes along with those from otherfamily members. Ratios of enzymatic reaction ratesat two substrate concentrations appeared to be adistinctive feature of the isozyme involved and in-dependent of absolute PK levels which variedwidely. Segregation of cases on the basis of differ-ences in these ratios, except for an occasionalequivocal value, correlated exactly with groupingsobtained by more elaborate Km determinations.PK activity ratios for different combinations ofPEP concentrations, viz., 0.3:1.5, 0.4:1.5, and0.4: 2.0 mmoles/liter yielded identical case group-ings.
The sensitivity of the modified assay methodwas demonstrated by data recorded in Table VI.Hemolysates of normal control and proposituscells were mixed in varying proportions and theirresultant PK activities were determined at 1.5and 0.3 mm PEP. Measurable activity at thehigher substrate concentration was constant for allcombinations. At 0.3 mmPEP, however, varia-tions in hemolysate proportions as little as 16%produced detectable alterations in observed PKreaction rates. This is approximately the resolu-tion limit of the spectrophotometric assay methodper se.
With the modified assay technique, other avail-able family members were screened for erythro-cyte PK activities. Findings suggestive of alteredPK kinetics or low absolute activity levels were
investigated further by Kmdeterminations. Resultsof family surveys are incorporated in the pedigreesshown in Fig. 6.
PK inhibition studies. Experiments cited pre-viously, in which normal and proband erythrocyteswere mixed in varying proportions, failed to detectany inhibitors in propositus cells to account for theobserved alterations in PK kinetics. In each in-stance, PK activities in hemolysate mixtures wereequivalent to the sums of activities contributed bythe isolated components. These findings were inde-pendent of varying cell proportions up to 5: 1 infavor of either normal or proband cells, and theywere unaffected by preincubation of the mixtures,either as intact cells or lysates, up to 30 min at25 or 370C.
Preparatory to attempts to separate the iso-zymes chromatographically, lysates of mixed nor-mal and proband erythrocytes, as well as hemoly-sates from relatives with intermediate PK kinetics,were deionized by dialysis or gel filtration in 25
KINDRED_aI
I
N
KINDRED_@I
II
N
FIGURE 6 Genealogies for kindreds Gand D. Generationsare designated by Roman numerals with individual posi-tions numbered consecutively from left to right. Malesand females are shown as squares and circles, respec-tively. The propositi are indicated by numbered arrows.Deceased individuals and those not studied are noted bydiagonal lines and question marks, respectively. A par-tially blackened symbol indicates heterozygous deficiencyfor the usual molecular form of erythrocyte pyruvatekinase, PK1. Heterozygosity for the anomalous isozyme,PK2, indicated by partial shading, is isolated to the pro-band and their siblings and maternal relatives. PositionIII-2 in kindred G has been filled by the recent birth ofa male infant whose cord-blood PK assayed at 1.79 EUwith a Km (PEP) of 1.1 mmoles/liter.
1940 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

separate procedures. Lysates were prepared bydilution of saline-washed erythrocytes in 4-9 vol-umes of 0.005 M phosphate buffer, varying indifferent experiments from pH 6.6 to 7.6, followedby triplicate freezing and thawing in a Dowanoland dry-ice mixture. Hemolysates (approximately20 ml) were equilibrated at 40C either by dialysisagainst large volumes of the appropriate buffer(3-5 liters changed three times over 8 to 12 hr)
or by passage through a 1.5 X 25.0-cm column ofSephadex G-25 previously equilibrated with thesame buffer. Without exception, PK kinetics inthe hemolysates were unaltered by such deioniza-tion procedures. Some decrease in total PK activ-ity was occasionally observed after the more
prolonged dialyses, but again activities in mixtureswere equal to the sums of activities in the unmixedcomponents identically treated.
Studies on pH effects. Erythrocytes from twopropositi were studied for pH dependency of theirPK activities. Cells from four normal controls andthree family members with intermediate kineticswere similarly studied. The assay system was pre-
pared using triethanolamine-HCl (TEA) buffersof identical molarity but varying pH, and pH was
determined in each cuvette solution with a Beck-man Expandomatic pH meter, both before andafter initiation of the enzymatic reaction withhemolysate.
Prevailing pH was found invariably to be lowerthan that of the primary buffer. It was apparentthat the standard assay system, containing TEAin a final concentration of 8.3 mmoles/liter, pos-
sessed insufficient buffering capacity to maintainpH at 7.5 as supposed. Actual values ranged be-tween 6.8 and 7.1, the variations occasioned bydifferent batches of PEP.
Results of pH dependency studies, presented inFig. 7, indicated that a pH range of 6.8 to 7.1was still optimal for normal PK1, but PK2 frompropositus cells reached peak efficiency between 6.1and 6.4. Rapid decrescence of PK, activity abovepH 6.5 possibly accounted for the several lowvalues noted for some propositi and maternal rela-tives on the basis of standard PK assays (TableIII and Fig. 1), some of which would normallybe considered indicative of heterozygous PK-deficiency states.
All hemolysates behaved similarly at low pHbut showed divergent characteristics above pH 6.0,
Q.0
o 0.5
K
RO
.0
.
(.3
PK, PK2 INTERMEDIATESPK2 PROPOSITI
5.0 6.0pH
70
FIGURE 7 pH optimum curves. The shaded area con-
tains the range of values from four representative nor-
mal controls. Values shown in the upper graph were de-termined at the PEP concentration usually employed inroutine PK assays; those in the lower graph were de-termined simultaneously at a low substrate level. ThepH reported is a mean of values determined beforeinitiation and after completion of reaction measurementsin each cuvette, a value range of less than 0.05 pH U.
when PEP concentration was 1.5 mmoles/liter.The distinct differences between pH-dependencycurves derived for propositus and normal red-cellPK were accompanied again by intermediatecurves in three cases postulated to representcoexistence of PK1 and PK2. These distinctionswere clear whether or not PK activities were de-termined at high or low substrate levels. As shownin the lower half of Fig. 7, differences among thethree groups (propositi, intermediates, and nor-
mals) at 0.4 mMPEP were apparent over theentire pH range explored.
Comparison of curves in Fig. 7 indicated furtherthat the ratio of activities at these two concentra-tions was also a dependent variable of pH. Segre-gation of cases on the basis of activity ratios athigh and low PEP levels, as proposed for themodified PK screening test, therefore requiredcritical control of pH to ensure reproducibility as
well as validity.
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase
I/5IMM PEPI PKI CONTROL RANGE
5.0 6 H 05.0 6.0 oH 7.0 8.0
pn~~~~~~~~~~~~~~~~~~
1941

t: loo
k sot 80
70
E 60
Z 50
b 40
k 30
w 20
Q. 0cx:
5 10 15 20 25 30
STORAGEPERIOD (DAYS)
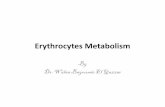
PK stability studies. In view of relativelyrapid degradation of PK activity in stored erythro-cytes, and especially in hemolysates, Attempts weremade to detect differences in stability character-istics of PK1 relative to PK2. Saline-washed redcells from normal controls, propositi, and somerelatives with intermediate kinetics were storedintact or as phosphate-buffered hemolysates at 22,4, and - 200C. Intact erythrocytes at the lattertemperature were frozen rapidly in dry-ice andDowanol mixtures before storage. PK assays athigh and low substrate concentrations were con-ducted over a 1 month period. Magnesium inconjunction with mercaptoethanol (MCE) wasalso tested for ability to retard PK inactivation.
Generally, PK2 stability was found to be lessthan half that of PK, under all comparable storageconditions. Washed-cell preparations showed iden-tical activity losses whether preserved at 4 or- 200C. Mean curves presented in Fig. 8 com-bined the values determined for both temperaturesand indicated a twofold or greater decay rate forpropositus enzyme. At room temperature, decayrates were considerably accelerated, but a similarrelative difference existed between PK1 (ti, 6days) and PK2 (ti, 2 days) for the initial decayslopes.
Propositus and normal hemolysates equivalentto 105 cells/,Ml in 0.005 M phosphate buffer, pH7.2, also showed pronounced differences in PKdegradation at 4VC, as shown in the first part ofFig. 9. Interestingly, the rate of activity loss in
1942 Paglia, Valentine, Baughan, Miller, Reed,
FIGURE 8 PK stability curves for saline-washed erythrocytes. Each point is the meanof four determinations on two separate cellpreparations. Storage temperature was either4VC or -20'C with no significant differ-ence apparent between results at the twotemperatures.
propositus cells was virtually identical to thatdetermined for the patient's mother, even thoughan intermediate decay curve might be expected for
K
(3
'4.-
'14J
141
1 2 3 4 5 6 7
STORAGEPERIOD (DAYS)FIGURE 9 PK stability curves for buffered hemolysates.Each point is the mean of four determinations on twohemolysate preparations. Storage temperature was 40C.Values in the lower graph were determined on identicalhemolysates wnhich additionally contained 0.01 M MgCl2and 0.001 M mercaptoethanol. Zero-time assays were per-formed approximately 48 hr after venipuncture.
and McIntyre

the latter. This may have resulted from shipmentdelays between venipuncture and zero-time assays,which generally approximated 48 hr.
Whereas the presence of 0.001 M MCEand0.01 M MgCl2 did not effectively alter PK decayrates in intact erythrocytes, hemolysate activitieswere significantly affected in all instances. Theextent of PK protection by these additives isshown by comparison of the two graphs in Fig. 9,which also indicated a greater stabilizing effectby the additives on PK1 than on PK2.
DISCUSSION
Preliminary attempts to obtain isozyme separationby gel filtration, starch-gel electrophoresis, andcolumn chromatography yielded equivocal resultsat least partially due to instability of this enzymeover the periods required for shipment and proc-essing. Electrophoretic separations were addition-ally complicated by the lack of a suitable positivestain for PK. Nevertheless, proband erythrocytePK was found to differ distinctly from the usualenzyme form on the basis of kinetic properties, pHdependency, and functional stability. In the ab-sence of demonstrable inhibitors, these variations,virtually identical in propositi from two unrelatedfamilies, seemed sufficient in magnitude to justifythe supposition that a pathologic PK isozyme(PK2) was operative in erythrocytes of affectedsubjects. This supposition was supported by thefrequent occurrence of intermediate degrees ofvariation in phenotypically normal relatives inwhom erythrocyte studies indicated coexistence ofboth isozymes.
The diverse findings in these studies may bereconciled within the framework of a simple uni-fying hypothesis regarding the patterns of geneticexpression in erythrocyte PK deficiency. Thishypothesis presumes that erythrocyte-PK activi-ties and kinetics common to most individuals inthe population at large should occur when bothcontributed genes are normal, resulting in a geno-type designated PK1PKR.
A gene, here designated PK1A, which produceskinetically normal but quantitatively deficient ac-tivity, when inherited in company with a normalPK1 gene, would then effect the common hetero-zygous deficiency state with normal kinetics butapproximately half-normal activity levels, a geno-type of PK1PKA. Similarly, the usual homozy-
gous PK deficiency with genotype PK1APKRAshould behave normally by kinetic standards if thepaucity of enzyme protein permits experimentaldeterminations. Wehave found this to be true inseveral cases so studied, as have other investi-gators (22, 23, 29).
Nearly pure production of the kinetically anoma-lous isozyme (PK2) could occur when this geneis inherited along with one causing quantitativedeficiency, i.e., a genotype of PK1APK2. Occur-rence of kinetic patterns which are directly inter-mediate between pure PK1 and PK2 would thenbe contingent upon concomitant inheritance of both(genotype PK1PK2), which should be distinguish-able biochemically, but not clinically, from eitherPK1PK, or PKPKA. Even though results ofpresent studies conform to an allelic hypothesis,this terminology is used only for simplicity ofdiscussion and should not imply that allelism doesin fact exist.
In normal erythrocytes, PK activity has beenshown to depend directly upon PEP availability,and generally this enzyme operates far below itspotential maximum (21). In PK-deficient cells ofthe usual variety, the enzyme may be more nearlysaturated as PEP concentrations increase due tothe partial metabolic block. Concurrently, the fallin intracellular levels of ATP, which partiallycompetes with PEP for a common binding locus(27, 30), may actually increase rates of PKcatalysis in the deficient cell with a consequentKm (PEP) depression (21). In the case of PK2,however, inefficiency of catalytic conversion isdemonstrable in vitro even in the absence of ATP.Intracellular PEP levels would therefore be ex-pected to elevate appreciably before effectivecatalysis could occur. Presumably this would havethe same consequences of intermediate accumula-tion, such as 2,3-DPG, and altered ADP/ATPratios as those which obtain when quantitativelyexiguous PK1 is operative at full saturation. Inthese propositi, then, the enzymopathy conceivablycould present a significant metabolic handicap tothe red cells by virtue of profound catalytic ineffi-ciency at the low intracellular PEP concentrationsnormally prevalent (31, 32).
In the present study, as in many instances ofquantitative PK deficiency, glycolysis and ATPmaintenance in the cells assayed appeared reasona-bly adequate. It should be emphasized, however,
A Pathologic Isozyme of Erythrocyte Pyruvate Kinase 1943

that in such subjects only select reticulocyte-richpopulations of young cells still capable of survivalare available for study. In view of the ancillarymetabolic pathways available to reticulocytes, thegreatly enhanced glycolytic capacities of youngerythrocytes compared with older cells, and thefact that all assays yield mean values, such observa-tions fail to answer the crucial question, i.e., howwill these same cells glycolyze and maintain ATPat some later stage of existence?
It is clear that capacity for erythrocyte survivalin extreme cell youth cannot be extrapolated toolder cells, and hemolytic anemia by definition willbe the result of diminished survival. Ultimatemetabolic aberrations preceding cell destructionmay be demonstrable only in moribund cells whichare not selectively available for study. Measure-ments of glycolytic activity, ATP levels and ATPmaintenance in cells a priori still capable of sur-vival can only provide hints of metabolic eventsimmediately proximal to cell destruction.
Adequate erythrocyte survival measurementswere not available in the present cases, but life-span shortening may be gauged clinically and interms of measured elevations in G-6-PD activitiesand reticulocytes. The etiologic basis of the meta-bolic findings reported in Table II is thus open tosome speculation, and equal argument might bemade for an increase in ATP utilization as op-posed to impaired formation. Such considerationsaside, one point remains clear: the patterns ofmetabolic changes in propositus erythrocytes, aswell as the clinical features presented by the pro-band, conformed well to those demonstrable inhomozygous PKdeficiency of the quantitative type.
Chronic hemolytic anemia, then, has been foundto be associated both with severe quantitative de-pression of PK activity and with active enzymecatalytically inefficient at low substrate concentra-
-tions. This essential identity in phenotypic ex-pression resulting from two separate aberrationsin erythrocyte PK renders it unlikely that anymechanism other than deficient PK catalysis' isprimary in causing the observed syndrome.
Just as the general category of congenital non-spherocytic hemolytic anemias has been shown tobe a heterogeneous group frequently associatedwith one of several erythroenzymopathies, similarheterogeneity appears to be evolving within thesubcategory of PK-deficiency hemolytic anemias.
Some cases reported as atypical PK deficienciesmay in fact represent kinetic anomalies similar,if not identical, to those in the present study,e.g., case 6 of Loder and de Gruchy (33), casesE. H. and M. C. of Koler, Bigley, Jones, Rigas,Vanbellinghen, and Thompson (29), and the casereports of Fusco, Busch, Negrini, and Azzolini(34) and Sachs, Wicker, Gilcher, Conrad, andCohen (35).
Unpublished studies by Miwa, Ohyama, andKumatori 2 and by Tanaka 3 have also indicatedthat abnormal PK kinetics rather than a quanti-tative enzyme deficit may underlie some instancesof the syndrome. Tanaka has noted an occasionalpatient with intermediate levels of red-cell PKactivity whose apparent Km(PEP) was over twicenormal. In the case investigated by Miwa et al.,a child with nonspherocytic hemolytic anemia wasfound to have elevated erythrocyte levels of PEPand monophosphoglycerates, as well as increasedPK activity. The Km(PEP) was five times greaterthan that of controls, and the pH optimum wasalso shifted to the acidic region.
There has been justifiable controversy regardingthe relative importance of mutant structural-genevs. control-gene effects in PK-deficiency anemias.The extensive work of Koler et al. (29), whichestablished the molecular distinction between leu-kocyte and erythrocyte PK, additionally demon-strated apparent molecular homogeneity of thisenzyme within erythrocytes, whether normal,heterozygous, or homozygous for quantitative PKdeficiency. In support of the latter findings, kineticstudies of homozygotes by Wiesmann and T6nz(23) and Campos et al. (22) failed to demonstratesignificant deviations from normal.
The possibility of mutant structural genes alsooperating in PK-deficiency states received prelimi-nary support from Waller and L6hr (36, 37) andfrom Boivin and Galand (38). Waller and L6hr'stwo cases had Km (PEP) values in crude hemoly-sates two to four times higher than normals, butwith less than 8%o of the usual measurable activity,in contrast to our observations of 10-fold higherKmassociated with borderline normal or elevatedactivity rates when assayed with 1.5 mmPEP assubstrate. Boivin and Galand, working with PKpartially purified by diethylaminoethyl (DEAE)
2 Personal communication.3 Personal communication.
1944 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre

extraction and ammonium sulfate precipitation,found Km (PEP) five times lower than normalsin red cells having some 20% of the usual activitylevels at full enzyme saturation, indicating that intheir case, enhanced catalytic efficiency might bepossible at low PEP concentrations.
Such diverse observations make it difficult toincriminate either a control-gene or structural-genemutation alone as the sole genetic determinant ofPK-deficiency hemolytic anemia. It would seemmore appropriate to postulate that the syndromemay result from a mutant regulator or mutantstructural gene, or both in combination, with agreater probability being associated with control-gene defects.
Certainly such conjectures must be consid-ered speculative, not only because alternative ex-planations exist, but also because some of thepublished information remains unconfirmed andwas reported originally with incomplete specifica-tion of assay conditions. Nonetheless, two blocksof reliable data now indicate that familial hemo-lytic anemia, conforming in virtually all respectsto the PK-deficient type, may be associated witheither a quantitative or a qualitative enzyme defect,lending a priori support to a basic pathogeneticrole for the enzymopathy per se in the inductionof premature hemolysis.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the technical con-tributions of Julie Wittenberg, Klaus Kfirschner, MaryLu Wilson, Agnes Halasz, Ernesto Guereque, MaryluMattson, Thea Gabor, Vaudeen Abel, Martha Benson,Marion Murphy, and Geraldine Roberts. Assistance inpreparation of the manuscript was provided by RuthExley. Dr. John Ellis kindly referred the patients inkindred G. We also wish to thank Dr. Kouichi Tanakafor his review of the manuscript and helpful suggestions.
This work was supported in part by U. S. PublicHealth Service Grants HE-01069, FR 05403-06, HE-6234, and AM-02992; U. S. Army Medical and ResearchDevelopment Command Contract DA-49-193 MD 2656;and contributions from the Louis B. Mayer FoundationFund for Medical Education and Research, Los Angeles;and the Pediatric Blood Research Fund, Strong MemorialHospital, Rochester, N. Y.
REFERENCES
1. Tanaka, K. R., and W. N. Valentine. 1968. Pyruvatekinase deficiency. In Hereditary Disorders of Erythro-cyte Metabolism. Proceedings of a Symposium, Cityof Hope Medical Center, Calif. 1967. E. Beutler, edi-tor. Grune and Stratton, Inc., New York. 1: 229.
2. Tanaka, K. R. Pyruvate kinase. 1968. In BiochemicalMethods in Red Cell Genetics. J. J. Yunis, editor.Academic Press Inc., New York. In press.
3. Valentine, W. N., K. R. Tanaka, and S. Miwa. 1961.A specific erythrocyte glycolytic enzyme defect (py-ruvate kinase) in three subjects with congenital non-spherocytic hemolytic anemia. Trans. Assoc. Am.Physicians. 74: 100.
4. Valentine, W. N., and K. R.' Tanaka. 1966. Pyruvatekinase deficiency hereditary hemolytic anemia. In TheMetabolic Basis of Inherited Disease. J. B. Stanbury,J. B. Wyngaarden, and D. S. Fredrickson, editors.McGraw-Hill Book Co., New York. 1051.
5. Keitt, A. S. 1966. Pyruvate kinase deficiency andrelated disorders of red cell glycolysis. Am. J. Med.41: 762.
6. Cartwright, G. E. 1958. Diagnostic Laboratory Hema-tology. Grune and Stratton, Inc., New York. 2ndedition.
7. Selwyn, J. G., and J. V. Dacie. 1954. Autohemolysisand other changes resulting from incubation in vitroof red cells from patients with congenital hemolyticanemia. Blood. 9: 414.
8. Young, L. E., M. J. Izzo, K. I. Altman, and S. N.Swisher. 1956. Studies on spontaneous in vitro auto-hemolysis in hemolytic disorders. Blood. 11: 977.
9. Shen, S. C., T. H. Ham, and E. M. Fleming. 1943.Studies on the destruction of red blood cells. III.Mechanism and complications of hemoglobinuria inpatients with thermal burns; spherocytosis and in-creased osmotic fragility of red blood cells. NewEngl. J. Med. 229: 701.
10. Bartlett, G. R. 1959. Human red cell glycolytic inter-mediates. J. Biol. Chem. 234: 449.
11. Miller, D. R., R. L. Baehner, and L. K. Diamond.1967. Paroxysmal nocturnal hemoglobinuria in child-hood and adolescence. Clinical and erythrocyte meta-bolic studies in two cases. Pediatrics. 39: 675.
12. Tanaka, K. R., W. N. Valentine, and S. Miwa. 1962.Pyruvate kinase (PK) deficiency hereditary non-spherocytic hemolytic anemia. Blood. 19: 267.
13. Biucher, T., and G. Pfleiderer. 1955. Pyruvate kinasefrom muscle. In Methods in Enzymology. S. P. Colo-wick and N. 0. Kaplan, editors. Academic Press,Inc., New York. 1: 435.
14. Valentine, W. N., and K. R. Tanaka. 1966. Pyruvatekinase: clinical aspects. In Methods in Enzymology.S. P. Colowick, N. 0. Kaplan, and W. A. Wood,editors. Academic Press Inc., New York. 9: 468.
15. Koutras, G. A., M. Hattori, A. S. Schneider, F. G.Ebaugh, Jr., and W. N. Valentine. 1964. Studies onchromated erythrocytes: effect of sodium chromateon erythrocyte glutathione reductase. f. Clin. Invest.43: 323.
16. Valentine, W. N., F. A. Oski, D. E. Paglia, M. A.Baughan, A. S. Schneider, and J. L. Naiman. 1967.Hereditary hemolytic anemia with hexokinase defi-ciency. Role of hexokinase in erythrocyte aging. NewEngl. J. Med. 276: 1.
A Pathologic Isozyme of Erythrocyte Pyruvate KinaTse 1945

17. Schneider, A. S., W. N. Valentine, M. Hattori, andH. L. Heins, Jr. 1965. Hereditary hemolytic anemiawith triosephosphate isomerase deficiency. New Engl.J. Mled. 272: 229.
18. Paglia, D. E., and W. N. Valentine. 1967. Studies onthe quantitative and qualitative characterization oferythrocyte glutathione peroxidase. J. Lab. Clin. Med.70: 158.
19. Baughan, M. A., W. N. Valentine, D. E. Paglia,P. 0. Ways, E. R. Simon, and Q. B. DeMarsh. 1968.Hereditary hemolytic anemia associated with glucose-phosphate isomerase (GPI) deficiency-a new enzymedefect of human erythrocytes. Blood. (In press.)
20. Horecker, B. L., and A. Kornberg. 1948. The extinc-tion coefficients of the reduced band of pyridinenucleotides. J. Biol. Chem. 175: 385.
21. Rose, I. A., and J. V. B. Warms. 1966. Control ofglycolysis in the human red blood cell. J. Biol. Chem.241: 4848.
22. Campos, J. O., R. D. Koler, and R. H. Bigley. 1965.Kinetic differences between human red cell and leuko-cyte pyruvate kinase. Nature. 208: 194.
23. Wiesmann, U., and 0. Tonz. 1966. Investigations ofthe kinetics of red cell pyruvate kinase in normalindividuals *and in a patient with pyruvate kinasedeficiency. Nature. 209: 612.
24. Boyer, P. D. 1962. Pyruvate kinase. In The Enzymes.P. D. Boyer, H. Lardy, and K. Myrbach, editors.Academic Press Inc., New York. 2nd edition. 6: 95.
25. McQuate, J. T., and M. F. Utter. 1959. Equilibriumand kinetic studies of the pyruvic kinase reaction.J. Biol. Chem. 234: 2151.
26. Whigham, W. R. 1965. Purification of pyruvatekinase from human red cells. Ph.D. Thesis. BaylorUniversity, Dallas.
27. Reynard, A. M., L. F. Hass, D. D. Jacobsen, andP. D. Boyer. 1961. The correlation of reactionkinetics and substrate binding with the mechanism ofpyruvate kinase. J. Biol. Chem. 236: 2277.
28. Mildvan, A. S., and M. Cohn. 1966. Kinetic and mag-netic resonance studies of the pyruvate kinase reac-
tion. II. Complexes of enzyme, metal, and substrates.J. Biol. Chem. 241: 1178.
29. Koler, R. D., R. H. Bigley, R. T. Jones, D. A. Rigas,P. Vanbellinghen, and P. Thompson. 1964. Pyruvatekinase: molecular differences between human red celland leukocyte enzyme. Cold Spring Harbor Symp.Quant. Biol. 29: 213.
30. Kerson, L. A., D. Garfinkel, and A. S. Mildvan.1967. Computer simulation studies of mammalianpyruvate kinase. J. Biol. Chem. 242: 2124.
31. Busch, D., and K. Schmuck. 1965. Probleme desErythrozytenstoffwechsels bei Anamien mit Pyruvat-kinasemangel. Folia Haematol. 83: 395.
32. Jacobasch, G., I. Syllm-Rapoport, H. Scharfschwerdt,F. M. G. Otto, and H. Pester. 1965. Pyruvatkinase-mangel und einige Probleme der Glykolyseregulierung.Folia Haematol. 83: 407.
33. Loder, P. B., and G. C. de Gruchy. 1965. Red-cellenzymes and co-enzymes in non-spherocytic congenitalhaemolytic anaemias. Brit. J. Haematol, 11: 21.
34. Fusco, F. A., D. Busch, A. C. Negrini, and A. Azzo-lini. 1966. Anemia emolitica congenita non sferociticada anomalie della pyruvatochinasi. Haematol. Arch.51: 836.
35. Sachs, J. R., D. J. Wicker, R. 0. Gilcher, M. E.Conrad, and R. J. Cohen. 1967. PK deficient hemo-lytic anemia inherited as an autosomal dominant.Blood. 30: 881. (Abstr.)
36. Waller, H. D., and G. W. Lohr. 1962. Hereditarynonspherocytic enzymopenic hemolytic anemia withpyruvate kinase deficiency. Proc. 9th Congr. Intern.Sor. Hematol. Mexico City. 257.
37. Waller, H. D., and G. W. Lohr. 1963. Hereditary non-spherocytic enzymopenic hemolytic anemias with py-ruvate kinase or 2,3-diphosphoglycerate mutase defi-ciency. Proc. 9th Congr. Europ. Soc. Hematol. Lisbon.74.
38. Boivin, P., and C. Galand. 1967. Constante deMichaelis anormale pour le phospho-enol-pyruvate aucours d'un deficit en pyruvate-kinase erythrocytaire.Rev. FranC. Etudes Clin. Biol. 12: 372.
1946 Paglia, Valentine, Baughan, Miller, Reed, and McIntyre