An exploration of substance use in rural Ontario Kathy Hardill, RNEC Doing the Work North Bay, July...
24
Rural Harm Reduction: “Below the Radar” An exploration of substance use in rural Ontario Kathy Hardill, RNEC Doing the Work North Bay, July 2012
-
Upload
harry-glenn -
Category
Documents
-
view
213 -
download
0
Transcript of An exploration of substance use in rural Ontario Kathy Hardill, RNEC Doing the Work North Bay, July...

Rural Harm Reduction: “Below the Radar”
An exploration of substance use in rural Ontario
Kathy Hardill, RNECDoing the Work
North Bay, July 2012
North Hastings
Town of Bancroft population 3,500 250 km NE Toronto Just south of Algonquin Park Mineral capital of Canada Mining – uranium, iron, corundum Logging
North Hastings
More likely to have low income, low education than rest of Ontario
High unemployment “dry” town until 1970s – bootlegging Religious fundamentalism Political conservatism Back to the landers Visible drug culture
› Where to go for drugs› Cannabis cultivation

“Below the Radar” - 2010
• Advanced Clinical Practice Fellowship RNAO and The Bancroft Medical Clinic› Literature review› Key informant interviews› Interviews with substance using individuals
3 nurses developed q’aire 2 administered survey Flyers, postings, snowball sampling 10 respondents 4 more 1:1 interviews later

Rural substance use
More substance use Fewer services (of all kinds) More barriers to service More stigma Poverty, unemployment, class selective
migration generational poverty, similar risks as inner city neighbourhoods
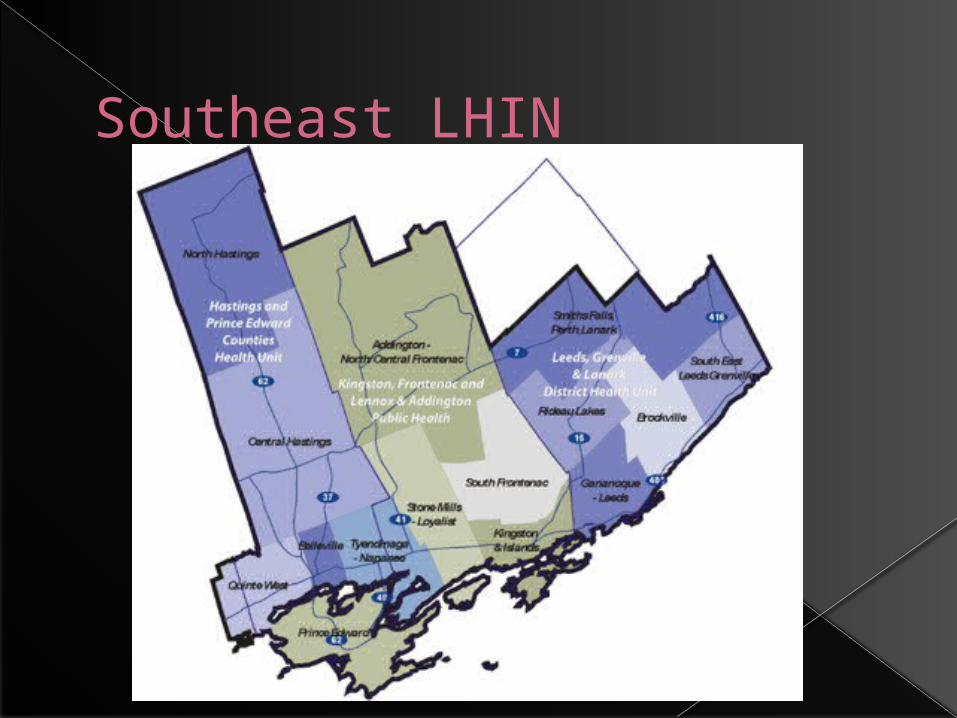
Southeast LHIN

Ontario Student Drug Use and Health Study- SE LHIN
70,000 Ontario students since 1977, CAMH
SE LHIN highest of all LHINs for: student use of opioid pain relievers without
a prescription (23.7% vs 18% Ont) student drinking and driving(17.6% vs 12%
Ont) ecstasy use by high school students (7.9%)

North Hastings
Cluster 5 suicide deaths 2010 Male, 18-55 Ongoing substance use Minimal contact with health care system
ongoing overdoses, suicides 2011, 2012
“ as (people’s) addiction increases, so does their isolation and their ability to access mainstream services becomes really limited”

Local data: interviews, KIs
Younger age – median age 40 Child rearing age Low incomes/precarious employment
Seasonal, part time, social assistance 6/10 < $999/mo
Precarious housing 7/10 renting, 1/10 homeless
Local data
Early drug use 9-15 years 6/10 alcohol, 4/10 cannabis
Polydrug use – marijuana, percocet, benzos
100% tobacco use Top three drugs of choice? “Oxycontin, Oxycontin, Oxycontin”
Local data
7/10 named an opiate as drug of choice 9/10 had been unable to obtain their DOC:
“It was horrible – I wanted to cut my legs off”
“I went through hell for a week – I thought I was dying”
Local data
Mental health – 6/10 depression/anxiety, 2/10 PTSD, 1/10 hx child abuse, 1/10 self injury, 1/10 hospitalized for suicidality
Pervasive low self esteem “Low self esteem takes on a life of its
own – there is just a hopelessness, a sense of not being able to accomplish anything, just an awful hopelessness”

Needle use, NEP
Bancroft NEP located in pharmacy Long hours of being open Lack of confidentiality, data, teaching Exponential increase but why?
› More aware of NEP? more trusting?› More drug use? use of drugs requiring
more frequent injections?› NO ONE KNOWS!!!!!

Increased NEP use – why?
Year # needles distributed
# needles/month
2009 3168 264
2010 12592 1049
2011 31620 2635(608/week)
Needle use
Needles found in several parks by public works employees - town liability issue
Lack of education? Lack of material resources? Stigma?
Outdoor drug use inherently unsafe Need to know who is using what,
where, how Lobby PHU to conduct research

Barriers and gaps - KIs
Diverse lack of services (72%) – addictions, counselling, primary care, residential treatment, crisis, child care, methadone
“It is our responsibility as a community to provide what people need, so they can get the help they need”

Barriers and gaps
Call for proactive, innovative collaboration between agencies
“We’ve got to stop being territorial about our clients and start thinking outside the box to reach people who will not be picking up the phone and calling to say they have a problem”

Barriers and gaps
Transportation To counselling, detox, primary care, NEP,
methadone Price of gasoline, insurance, unreliable
vehicles Gas pumps - $7!!!

Barriers and gaps
Stigma/isolation“I kept my addiction very hush hush”
“It’s harder in rural areas because labels stick, there is usually a small pool of providers, and some labels are even generational. The ‘mental memory’ of people and their family connections never fades”

Barriers and gaps
Lack of awareness/understanding by providers
9/10 had primary care provider, only 1 could think of anyone to go to for help re drug use
“We have to remove the sense of being punished for revealing a health condition to your provider”

Barriers and gaps
Methadone maintenance therapy (MMT) Replace opiate with prescribed
methadone to stabilize people Prohibitive zoning by-laws
“I used to hitchhike from Pembroke to Peterborough every week to go to clinic” (260 km one way)

Barriers and gaps
Lack of woman safe space – being “thirteen stepped” When women attending 12 step
programs are repeatedly approached sexually even after rebuffing advances and this is accepted in the culture of the group
“it becomes a balancing act to choose between your sobriety and your safety”

Challenges
distance and travel poverty lack of anonymity – not wanting to
“out” oneself as a drug user Lack of understanding of substance
use, harm reduction by service providers
Lack of services
Below the radar…….
Questions?
Report available:
http://www.substanceusestrategynetwork.org/resources.html