An ECMO Primer
109
VA- and VV-ECMO A tutorial… Alain Combes Service de Réanimation iCAN, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
Transcript of An ECMO Primer

VA- and VV-ECMO
A tutorial…
Alain Combes
Service de Réanimation
iCAN, Institute of Cardiometabolism and Nutrition
Hôpital Pitié-Salpêtrière, AP-HP, Paris
Université Pierre et Marie Curie, Paris 6www.reamedpitie.com

Conflict of interest
Principal Investigator: HEROICS trial HVHF after complicated heart surgery NCT01077349 Sponsored by GAMBRO
Principal Investigator: EOLIA trial VV ECMO in ARDS NCT01470703 Sponsored MAQUET, Getinge Group
Received honoraria from MAQUET, Getinge Group

The ECMO
extracorporeal circuit
Centrifugal pump
Membrane oxygenator
Controller
Cannulas
Tubing

The ECMO circuit:
Centrifugal pump
Electrical
Centrifugal pump
0->4000 RPM
Can deliver flows up to 8 L/min
Very reliable
Up to 21 days

The ECMO circuit:
Membrane Oxygenator
Hollow fiber membrane oxygenator
Polymethylpentene
Heparin-coated
High performance
CO2 elimination
Blood oxygenation
Low pressure drop
Long duration 15-21 d
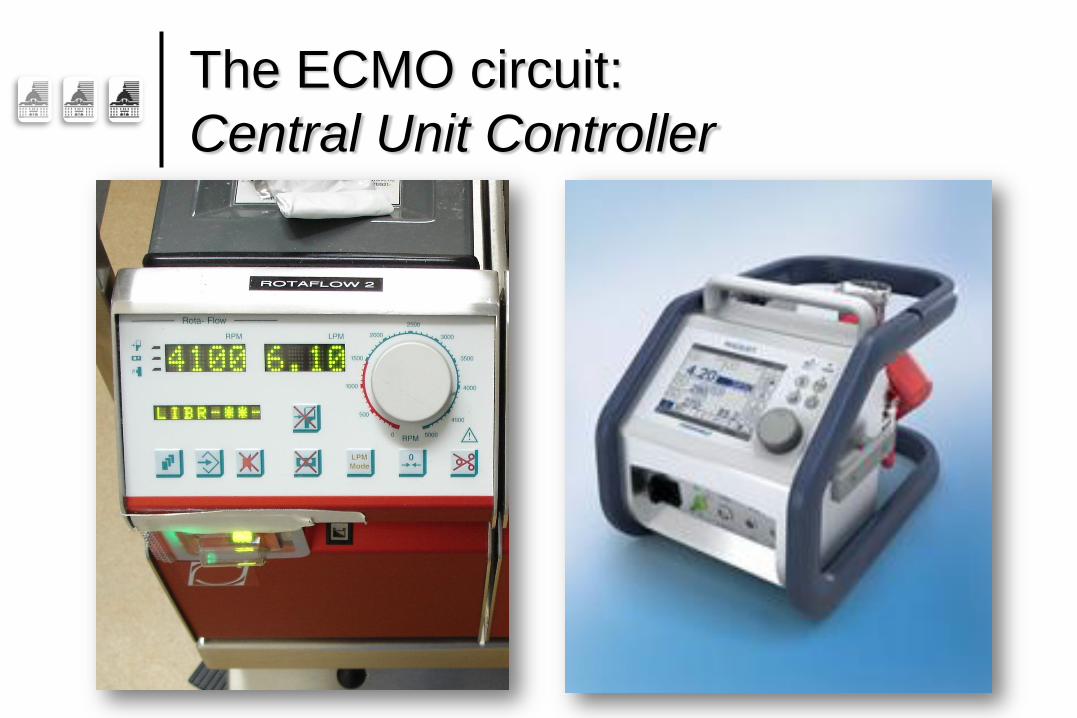
The ECMO circuit:
Central Unit Controller
Flow alarms

The ECMO circuit:
Cannulas
Percutaneous insertion of the Cannulas (Seldinger) Drainage Cannula:
• Femoral Vein
• Long cannula: up to 60 cm
Return Cannula:
• Oxygenated blood
• Femoral artery
• Shorter cannula: 20-25 cm
Cannulas Diameter+++ 22 – 30 Fr for drainage 15 – 23 Fr for return

Poiseuille’s Law…
Flow function of the 4th power of cannula diameter
Maximize drainage cannula diameter
25-30 Fr
To decrease pump speed, pressure and blood trauma

VA-ECMO for refractory
cardiogenic shock…

ECMO is now the
first line device…
In the context of acute refractory cardiac failure

Extracorporeal Membrane
Oxygenation: ECMO/ECLS
ECMO = ExtraCorporeal Membrane Oxygenation:
Centrifugal Pump + Oxygenator: Heart-Lung support
Peripheral vascular access:
Femoral site (cannulas), Seldinger technique, limited cut-down
Advantages
Easy and rapid implantation if peripheral ECMO
• No sterno/cardiotomy, local anesthesia, Emergency situations
Provides high and stable output flow
Simultaneous cardiac and pulmonary assistance: ECMO
Bridge to: Recovery, Bridge, Transplantation, Withdrawal
“Low cost” (2 - 40 times cheaper / other devices)

ECMO program at La Pitié, Paris
020406080
100120140160180200220240260280
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Total
Post CPB
Medical
Portable ECMO
Program

ECMO: Cannulas

Therapeutic Strategy:
When to initiate mechanical assistance?
Parameters to evaluate: Etiology/Time course of the disease Treatments administered Clinical status, in particular neurological status:
• Is it futile to insert a device?
Other clinical signs associated with rapid deterioration of cardiac function: Nausea, abdominal pain, Alteration of
consciousness Tachycardia, rhythm disturbances Ionic disturbances, Acidosis Hepatic / Renal failure
Doppler-Echocardiography +++ LVEF <20% Signs of low cardiac output, Ao VTI <8cm

Independent predictors of ICU death

The classical indications of
mechanical assistance…
4 types of indications:
« Bridge to recovery »
« Bridge to bridge »
« Bridge to transplantation »
« Destination therapy »
But now… In the acute setting…
Bridge to whatever seems reasonable
Including “withdrawal” after a few days• If refractory MOF…

ECMO vs. BiVAD?

P = ns


Creatinine mol/dlT bilirubin mol/dl

Results of ECMO…
In the context of acute refractory cardiac failure

1993-2002 2002-2009


Long term survival: 68%, 4 (10%) patients had heart transplantation
Independent predictors of ICU death determined at admission:
SAPS II >56 (OR, 10.23) and troponin Ic >12 g/L (OR, 7.49)

ECMO after cardiac
arrest

3-year prospective observational study
ECMO for 59 patients
Aged 18–75 years
With witnessed in-hospital cardiac arrest of cardiac origin
Undergoing CPR of more than 10 min
Compared with patients
Receiving conventional CPR
Matching process based
On a propensity-score

ECMO

60 min


This poor outcome suggests that the use of ECLS should be more restricted following OH refractory cardiac arrest

The Mobile ECMO
rescue team at La Pitié

The Mobile ECMO rescue team at La Pitié:
2005-2009 experience for refractory cardiac failure…

The mobile ECMO rescue team
Centres Patients N (%)
Median distance (range), Km
Median time (range), min
Paris urban agglomeration (7 centres) 25 (29) 4 (4-18) 4 (4-26) Paris region (26 centres) 54 (62) 13 (4-53) 19 (7-46) Outside Paris region (4 centres) 8 (9) 88 (87-243) 60 (64-134) Total (37 centres) 87 17 (4-243) 20 (4-134)

The mobile ECMO rescue team
87 patients 2005-2009
57 males, 28 females
Mean age: 46.1 [13-76]
Etiologies
AMI 46%
Chronic DCM 16%
Other Acute HF= 38%
• Myocarditis 14
• Intoxication 5
• Rythmic 4
• Post-Partum 3
• Hypoxemia 2
• Takotsubo 3
• Anaphylactic 1
• Septic 1

One year survival = 35%

Comparison with in-house patients
In the multivariate analysis
Adjusted for the inotrope score
Stratified for diagnosis and CPR at ECMO start
Mortality at hospital discharge in the
Cardiac-RESCUE Program group was
not statistically different between groups
OR 1.48, 95% CI 0.72–3.00, p=0.29

ICU management of
VA-ECMO

ECMO limitations
Time limitation: 15 – 21 days for femoral ECMO
>2 months using central ECMO
Patient must remain supine
If femoral ECMO
Local Complications :
Hemorrhage, embolism, acute leg ischemia, infection
Stroke: ischemic, hemorrhagic
Pump highly pre- and afterload dependent
Non-pulsatile flow?
Pulmonary edema

Management of pulmonary
edema under peripheral ECMO
ECMO increases LV afterload+++ Solutions to decrease LVEDP
Dobutamine for improving LV ejection Decrease ECMO flow? Intra aortic balloon pump Atrial Septostomy Transeptal LA drainage Impella® 5.0 Switch from femoral to central ECMO
• With a LA, PA or LV drainage cannula…• Use 2 ECMO systems, as for a BiVAD

Driving Lines Surveillance
Frequent surveillance
No folding
No tension• May precipitate pump failure
Maintain lines along leg axis • For >40 cm
• To prevent vessel tear
Special attention when moving the patient…

Patient’s Surveillance
Watch for Leg Ischemia…
Especially if no reperfusion line inserted

Lines “kicking” hard…
Check for hypovolemia
TTE/TEE
CVP
Frequent in case of vasoplegia due to Multiple Organ Failure
Fluid challenge if patent hypovolemia
Check tip of drainage cannula
Should be placed in the RA

Fibrin deposition

The “Harlequin” syndrome…
Flow competition in the aorta
Recovering Heart vs. ECMO pump
If pulmonary function is impaired
“Blue head”: deoxygenated blood directed to the upper part of the body
“Red legs”: oxygenated blood in the lower part of the body
SpO2 probe, blood gases on Right hand/right ear lobe/Right radial artery
Switch to VV ECMO if persistent lung failure

Biological Surveillance

Anticoagulation
Heparin
aPTT: 45-60 sec, 1.5 x control
Aspirin
Stop if Platelets < 50 G/L
Initiate if Platelets > 75-100 G/L
Aspirin + Clopidogrel
When Platelets > 400 G/L
When early/massive fibrin deposition

Anticoagulation problems…
Massive bleeding… In case of MOF
• Massive hepatic failure• Consumption
Stop aspirin, clopidogrel Possible to stop heparin for a few hours… or days…
• The whole circuit is heparin-coated…
Transfusion thresholds • 7-8 g/dl for RBC• <20 G/L for platelets
Clotting Membrane/Cannulas Check for clotting if
• Decrased blood flow, PaO2, Hemolysis• LA/PA/LV drainage

Hemolysis
May occur due to Membrane failure
• Fibrin, Clot formation
Pump with highly turbulent flow Clotting in the cannulas High energy blood suction
• Hypovolemia• Pulmonary artery/Left atrium drainage cannula
• Recovery of native heart function
Bloody diuresis Check regularly serum free hemoglobin

Echocardiography
Flow : Aortic TVI TDI : Ea / Sa
Diastolic filling (E)
Systolic : Parameter (LVEF)
Parasternal short
axis

Echo is fundamental
At the time of cannula insertion
To verify correct positioning of the venous cannula
For daily surveillance
Heart recovery
• Evaluation of weaning success
Complications
• Pericardial effusion
• Tamponnade
• Intracardiac clotting

Weaning from
ECMO…
Echocardiographic criteria

Parameters at minimal ECMO flow
0
40
60
80
100
120
E,
cm
/s
Weaned Not Weaned
0
40
60
80
100
120
E,
cm
/s
Weaned Not Weaned
33 hemodynamically stable patients who tolerated an ECMO
weaning trial the day before successful/unsuccessful weaning

Parameters at minimal ECMO flow
0
10
20
30
40
50
60
70
80
Puls
e p
ressure
, m
mH
g
0
10
20
30
40
50
60
70
Eje
ction fra
ction,
%0
40
60
80
100
120
E,
cm
/s
Weaned Not Weaned
0
40
60
80
100
120
E,
cm
/s
Weaned Not Weaned
33 hemodynamically stable patients who tolerated an ECMO
weaning trial the day before successful/unsuccessful weaning

Parameters at minimal ECMO flow
0
5
10
15
20
25
E/E
a
Weaned Not Weaned
0
40
60
80
100
120
E,
cm
/s
Weaned Not Weaned
33 hemodynamically stable patients who tolerated an ECMO
weaning trial the day before successful/unsuccessful weaning
“Heavy” and/or
Expensive Devices
Not for the acute phase…

VV-ECMO for refractory
respiratory failure…

ELSO registry from 1986–2006
1,473 patients with severe respiratoryfailure
50% survived to hospital discharge
Median age was 34 years
Most patients (78%) supported withvenovenous ECMO

Multivariate logistic regression model
Pre-ECMO factors associated with increasedodds of death were
Increasing age
Decreased weight
Days on mechanical ventilation beforeECMO
Arterial blood pH < 7.18
Hispanic and Asian race vs. white race
VA ECMO vs. VV ECMO

The CESAR trial

Time from randomization to death
Log rank p = 0.03

Influenza A
(H1N1)v09 …




17 (25%)

Et al…

Et al…
Trauma patients

In lung tranplant
patients…


In the case of massive
pulmonary emboli


Can we rely on
guidelines???…
When to decide on the initiation of ECMO?


SDRA lié à la grippe H1N1
Recommandations pour la ventilation
A. Mercat, J-C.M. Richard, A. Combes, J. Chastre, J.D. Ricard, D. Dreyfuss, L. Brochard
Réseau de Recherche en Ventilation Artificielle
(REVA)

ECMO : potential indications
• Refractory hypoxemia: PaO2/FiO2 < 50, persistent *
Despite: FiO2 > 80 %, PEEP (≤ 20 cmH2O)
Targeting Pplat = 32 cmH2O, prone position +/- NOi
• Plateau Pressure ≥ 35 cmH2O
despite reducing PEEP to 5 cmH2O
AND Vt to 4 ml/kg with pH remaining ≥ 7,15
* : Should also account for disease’s type and evolution

Where to perform ECMO?
• Experienced centers:
• With Heart surgeons, intensivists, perfusionists, nurses….
• All experienced in the management of ECMO devices
• ECMO programs should include a
mobile ECMO retrieval team
• Available 24H/7D
• Nationwide or regional EMCO networks necessary

Management of
Venovenous ECMO

ECMO Circuit
configuration for acute
respiratory failure
Venoarterial vs. Venovenous?

Comparison of VV and VA
configurations
VV configuration
Only lung support
Minor cardiac effects
Closed loop
RV/LV pre and afterload mostly unaffected
RV afterload may decrease
Improved oxygenation
VA configuration
Heart and Lung support
Decreases RV preload and pulmonary blood flow
Increases LV afterload
May cause LV stunning
Decreases arterial pulse pressure

ECMO configuration for
acute respiratory failure
Should always be venovenous…
…Except in the case of severe
associated cardiogenic shock

Peripheral VA ECMO is not
indicated for ARF because…
Flow competition in the aorta
Heart vs. ECMO pump
If pulmonary function is impaired
The “Harlequin” syndrome
• “Blue head”: deoxygenated blood directed to the upper part of the body
• “Red legs”: hyperoxygenated blood in the lower part of the body
Not possible to rest the lungs
Vt, Pplat and FiO2 cannot be reduced

Peripheral VA ECMO is not
indicated for ARF because…
VA ECMO increases LV afterload
Risk of myocardial damage/stunning
Complications associated with the arterial line in VA femoro-femoral ECMO
Leg ischemia
Arterial embolism
Massive arterial hemorrhage
ELSO registry from 1986–2006
1,473 patients with severe ARF
50% survived to hospital discharge
Most patients (78%) supported with venovenous ECMO
2009
68 H1N1 patients who received ECMO
77% survived
Most patients (93%) supported with venovenous ECMO

Determinants of arterial blood
oxygenation and
decarboxylation on VV ECMO

Most important determinants of
arterial oygenation during VV ECMO
ECMO Blood flow
Should match cardiac output
Oxygen demand
SvO2
Hemoglobin concentration
Recirculation
Cannula position/cannula type
Pulmonary shunt volume

How to optimize blood oxygenation?
Minimize recirculation Cannulas adequately (re)positionned Fluid loading to correct hypovolemia Adjust pump flow
ECMO flow objective: Pump flow: the major determinant of oxygenation
• >5 - 6 l/min or >3 L/m² or >60% of CO
USE LARGE DRAINAGE CANNULAS!!!
Other parameters Red cells transfusion:
• Increased transfusion threshold to Hb >10 g/dl• Only if persistent low SaO2

VV ECMO Circuit
configuration for acute
respiratory failure
ECMO cannulas
Jugulo-femoral… Femoro-jugular?
One… Two… Three…???

Poiseuille’s Law…
Flow function of the 4th power of cannula diameter
Maximize inflow cannula diameter
25-30 Fr
To decrease pump speed and blood trauma

Flow required to maintain equivalent SvO2
Significantly less flow was required
during Femoro-Atrial VV ECMO

Femoro-Jugular configuration
27 Fr drainage cannula
19 Fr return cannula

Avalon Cannula:
Solution to recirculation???
Mechanical Ventilation of
the patient on
VV ECMO
Allow the lungs to REST!!!

Mechanical Ventilation of the
patient under VV ECMO
Main objective: Minimize VILI Plateau Pressure 20-24 cm H2O Vt set at 1-4 ml/kg of ideal body weight
• If assist controlled mode used
BiPAP or APRV mode possible
Other MV settings PEEP increased to recruit the lungs
• 10-15 cm H2O
FiO2 < 50% Resp Rate 30-35
Patient often deeply sedated and paralyzed at the initial phase

Cohorte REVA Grippe ECMO

Biological Surveillance
Same as for VA ECMO…

Weaning from VV ECMO

VV ECMO Weaning Protocol
Weaning test: Sweep gas flow set at 0 L/min
• FiO2 set at 0.21 on the membrane • Pump flow not modified
Adjust FiO2 and Vt on the respirator
The device may be withdrawn if PaO2 >60 mmHg, SaO2 >90% FiO2 on the respirator <60% Inspiratory plateau pressure <30 cm H2O and if echocardiography reveals no signs of
acute cor pulmonale For at least 1-2 hours and up to 12 hours

Should ECMO be used
for all severe ARDS
patients?
Are there still skeptics????

Hubmayr, Rolf D., [email protected]
At this time, we do not
support the position that as
a nation we should invest in
the development of
additional ECMO centers

Designing
a new trial…
EOLIA:
ECMO to rescue Lung Injury in severe ARDS

EOLIA: ECMO to rescue Lung Injury
in severe ARDS
Multicenter international randomized controlled trial
Best care possible in the ECMO arm
ECMO initiated asap for every patient randomized• Using the most recent ECMO technology
• CardioHelp, from Maquet
Inclusion of some non-ECMO centers with a mobile ECMO rescue team available from the referral center in less than 1 hour
• Transport of randomized patients to the referral center UNDER ECMO
• ECMO managed only in highly experienced centers
“Highly protective” MV• Plateau pressure limited to ≤ 20 cm H2O

EOLIA: ECMO to rescue Lung Injury
in severe ARDS
Best care possible in the control arm
MV protocolized using the “high PEEP – high recruitment” strategy of the EXPRESS trial
To limit plateau pressure <28-30 cm H2O
• Vt limited to 6 ml/kg IBW
“Ethical” cross-over option to ECMO if the patient develops refractory hypoxemia

EOLIA: ECMO to rescue Lung
Injury in severe ARDS

EOLIA: ECMO to rescue Lung
Injury in severe ARDS

Conclusion
Early and rapid recognition of refractory cardiogenic shock
VA-ECMO can save the life of up to 70% of the patients
Poor outcomes if MOF at the time of ECMO institution
For the most severe forms of ARDS, VV-ECMO:
Replaces pulmonary function, Allows ultraprotective MV
Should allow facilitated lung healing
Only experienced centers should run these programs
With a mobile ECMO retrieval team available 24H/7D
Still a controversy on the use of VV-ECMO
Need for a confirmation trial…

La Pitié: 1612 to 2012…