An Algorithmic Approach to Perineal Reconstruction After ... · An Algorithmic Approach to Perineal...
7
An Algorithmic Approach to Perineal Reconstruction After Cancer ResectionVExperience From Two International Centers Hannah Eliza John, MBBS, MRCS,* Zita Maria Jessop, MA (Cantab), MRCS,Þ Michele Di Candia, MD,* Jeremy Simcock, MD (Melb), FRCS (Plast),*þ Amer J Durrani, MSc (Dist), FRCS (Plast),* and Charles M. Malata, FRCS (Plast)* Aim: This paper aims to simplify the approach to reconstruction of the peri- neum after resection of malignancies of the anal canal, lower rectum, vulva, and vagina. Materials and Methods: The data were collected from 2 centers, namely, Addenbrooke’s Hospital, University of Cambridge, United Kingdom and Christchurch Hospital, University of Otago, New Zealand. All patients who underwent perineal reconstruction from 1997 to 2009 at Christchurch Hospital (13 years) and 2001 to 2009 at Addenbrooke’s Hospital (9 years) were included. The diagnosis (indication), primary surgery, reconstructive surgery, compli- cations, tumor outcomes (recurrence and survival), and follow-up were entered into a database (Microsoft Excel; Redmond, Wash). The incidence of previous radiotherapy, requirement for adjuvant radiotherapy, and length of inpatient stay were also recorded. Results: Forty-six patients were identified for this studyV13 in New Zealand and 33 in Cambridge. Indications for perineal reconstruction included resec- tion of anal and rectal malignancies (24), vulval and vaginal malignancy (19), perineal sarcoma (1), and perineal squamous cell carcinoma arising in an enterocutaneous fistula (Table 1). The reconstructive strategies adopted included rectus abdominis myocutaneous flaps (26), gluteal fold flaps (9), gracilis V-Yor advancement flaps (7) and others (4), gluteal rotation flaps (1), local flap (2), and free latissimus dorsi flaps (1). Conclusions: Although various surgeons performed the reconstructive sur- geries at 2 different centers, the essential approach remained the same. Smaller defects were best treated by local flaps, whereas the rectus abdominis flap remained the standard option for larger defects that additionally required clo- sure of dead space. On the basis of our 2 center experience, we propose a simple algorithm to facilitate the planning of reconstructive surgery for the perineum. Key Words: perineum, vulva, algorithm for perineal reconstruction, anal canal, vaginal malignancy, pedicled flap, advanced perineal malignancy, vertical rectus abdominis muscle flap, transverse rectus abdominis muscle flap, gluteal fold flap, gracilis myocutaneous flap (Ann Plast Surg 2013;71: 96Y102) I rrespective of geographical location, plastic surgeons around the globe are faced with the ever-increasing challenge of reconstructing the perineum after wide local excisions of malignancies arising from the anal canal, rectum, vulva, and vagina. In the past, the vulvoper- ineal area was thought to heal poorly because of poor blood supply, although in reality, this region has a rich blood supply almost com- parable to that of the face. The widely anastomotic vascular network allows the perineal area to be a versatile donor site for local pedicled flaps. Recent trends in the surgical management of patients with vulval and perineal cancer have emphasized the value of conservative and less aggressive operations, which help to preserve function and appearance of the affected area as much as possible. On the other hand, radical operations for advanced perineal cancers are required to remove both primary and recurrent malignancy. Patients are also psychologically affected by bulky reconstructions in the vulvoper- ineal area; hence, the need for adequate morphofunctional recon- struction must be recognized. 1 Reconstructive options range from local advancement flaps for smaller defects, to pedicled flaps harvested from the inner thigh, gluteal fold and the abdomen for larger defects. Free flaps are used less commonly because of the limited access to and availability of vessels of suitable caliber for microvascular anastomosis. Currently, there is no consensus as to which reconstructive approach should be adopted for perineal defects. Cordeiro et al 2 suggested a classifi- cation system and reconstructive algorithm for vaginal defects. In 2005, Salgarello et al 3 proposed a flap algorithm for vulval recon- struction after radical vulvectomy. We therefore decided to review our experience with immediate perineal reconstruction at 2 interna- tional centers with the aim of creating a comprehensive algorithm to include all perineal defects and the reconstructive options available to provide a guiding framework for any reconstructive surgeon working in this area. PATIENTS AND METHODS All 46 patients who underwent perineal reconstruction after cancer resection at Addenbrooke’s University Hospital, Cambridge, in TABLE 1. Patient Demographics and Tumor Characteristics Cambridge (n = 33) New Zealand (n = 13) Total (N = 46) Sex distribution Males 8 6 14 Females 25 7 32 Tumor location Anal/rectal malignancy 14 10 24 Vulval/vaginal malignancy 18 2 20 Sacral chondroma with perineal ulcer 0 1 1 Perineal enterocutaneous fistula 1 0 1 Recurrent malignancy 19 6 25 96 www.annalsplasticsurgery.com Annals of Plastic Surgery & Volume 71, Number 1, July 2013 RECONSTRUCTIVE SURGERY Received June 13, 2011, and accepted for publication, after revision, November 7, 2011. From the *Department of Plastic and Reconstructive Surgery, Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust; †School of Clinical Medicine, University of Cambridge, Cambridge, United Kingdom; and ‡Department of Plastic and Reconstructive Surgery, Christchurch Hospital, University of Otago, Christchurch, New Zealand. Presented at the 44th Congress of the European Society for Surgical Research, May 23, 2009, Nimes, France, and at the Summer Meeting, British Association of Plastic, Reconstructive and Aesthetic Surgeons, June 30, 2010, Sheffield, UK. Conflicts of interest and sources of funding: none declared. Reprints: Charles M. Malata, FRCS (Plast), Department of Plastic and Recon- structive Surgery, Box 186, Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation Trust, Hills Rd, CB2 2QQ Cambridge, United Kingdom. E-mail: [email protected] Copyright * 2012 by Lippincott Williams & Wilkins ISSN: 0148-7043/13/7101-0096 DOI: 10.1097/SAP.0b013e3182414485 Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of An Algorithmic Approach to Perineal Reconstruction After ... · An Algorithmic Approach to Perineal...

An Algorithmic Approach to Perineal Reconstruction After CancerResectionVExperience From Two International Centers
Hannah Eliza John, MBBS, MRCS,* Zita Maria Jessop, MA (Cantab), MRCS,Þ Michele Di Candia, MD,*Jeremy Simcock, MD (Melb), FRCS (Plast),*þ Amer J Durrani, MSc (Dist), FRCS (Plast),*
and Charles M. Malata, FRCS (Plast)*
Aim: This paper aims to simplify the approach to reconstruction of the peri-neum after resection of malignancies of the anal canal, lower rectum, vulva, andvagina.Materials and Methods: The data were collected from 2 centers, namely,Addenbrooke’s Hospital, University of Cambridge, United Kingdom andChristchurch Hospital, University of Otago, New Zealand. All patients whounderwent perineal reconstruction from 1997 to 2009 at Christchurch Hospital(13 years) and 2001 to 2009 at Addenbrooke’s Hospital (9 years) were included.The diagnosis (indication), primary surgery, reconstructive surgery, compli-cations, tumor outcomes (recurrence and survival), and follow-up were enteredinto a database (Microsoft Excel; Redmond, Wash). The incidence of previousradiotherapy, requirement for adjuvant radiotherapy, and length of inpatient staywere also recorded.Results: Forty-six patients were identified for this studyV13 in New Zealandand 33 in Cambridge. Indications for perineal reconstruction included resec-tion of anal and rectal malignancies (24), vulval and vaginal malignancy (19),perineal sarcoma (1), and perineal squamous cell carcinoma arising in anenterocutaneous fistula (Table 1). The reconstructive strategies adopted includedrectus abdominis myocutaneous flaps (26), gluteal fold flaps (9), gracilis V-Yoradvancement flaps (7) and others (4), gluteal rotation flaps (1), local flap (2), andfree latissimus dorsi flaps (1).Conclusions: Although various surgeons performed the reconstructive sur-geries at 2 different centers, the essential approach remained the same. Smallerdefects were best treated by local flaps, whereas the rectus abdominis flapremained the standard option for larger defects that additionally required clo-sure of dead space. On the basis of our 2 center experience, we propose a simplealgorithm to facilitate the planning of reconstructive surgery for the perineum.
Key Words: perineum, vulva, algorithm for perineal reconstruction, analcanal, vaginal malignancy, pedicled flap, advanced perineal malignancy,vertical rectus abdominis muscle flap, transverse rectus abdominis muscle flap,gluteal fold flap, gracilis myocutaneous flap
(Ann Plast Surg 2013;71: 96Y102)
I rrespective of geographical location, plastic surgeons around theglobe are faced with the ever-increasing challenge of reconstructing
the perineum after wide local excisions of malignancies arising fromthe anal canal, rectum, vulva, and vagina. In the past, the vulvoper-ineal area was thought to heal poorly because of poor blood supply,although in reality, this region has a rich blood supply almost com-parable to that of the face. The widely anastomotic vascular networkallows the perineal area to be a versatile donor site for local pedicledflaps. Recent trends in the surgical management of patients withvulval and perineal cancer have emphasized the value of conservativeand less aggressive operations, which help to preserve function andappearance of the affected area as much as possible. On the otherhand, radical operations for advanced perineal cancers are required toremove both primary and recurrent malignancy. Patients are alsopsychologically affected by bulky reconstructions in the vulvoper-ineal area; hence, the need for adequate morphofunctional recon-struction must be recognized.1
Reconstructive options range from local advancement flapsfor smaller defects, to pedicled flaps harvested from the inner thigh,gluteal fold and the abdomen for larger defects. Free flaps are usedless commonly because of the limited access to and availability ofvessels of suitable caliber for microvascular anastomosis. Currently,there is no consensus as to which reconstructive approach shouldbe adopted for perineal defects. Cordeiro et al2 suggested a classifi-cation system and reconstructive algorithm for vaginal defects. In2005, Salgarello et al3 proposed a flap algorithm for vulval recon-struction after radical vulvectomy. We therefore decided to reviewour experience with immediate perineal reconstruction at 2 interna-tional centers with the aim of creating a comprehensive algorithm toinclude all perineal defects and the reconstructive options available toprovide a guiding framework for any reconstructive surgeon workingin this area.
PATIENTS AND METHODSAll 46 patients who underwent perineal reconstruction after
cancer resection at Addenbrooke’s University Hospital, Cambridge, in
TABLE 1. Patient Demographics and Tumor Characteristics
Cambridge(n = 33)
New Zealand(n = 13)
Total(N = 46)
Sex distribution
Males 8 6 14
Females 25 7 32
Tumor location
Anal/rectal malignancy 14 10 24
Vulval/vaginal malignancy 18 2 20
Sacral chondroma withperineal ulcer
0 1 1
Perineal enterocutaneousfistula
1 0 1
Recurrent malignancy 19 6 25
96 www.annalsplasticsurgery.com Annals of Plastic Surgery & Volume 71, Number 1, July 2013
RECONSTRUCTIVE SURGERY
Received June 13, 2011, and accepted for publication, after revision, November 7,2011.
From the *Department of Plastic and Reconstructive Surgery, Addenbrooke’sHospital, Cambridge University Hospitals NHS Foundation Trust; †School ofClinical Medicine, University of Cambridge, Cambridge, United Kingdom; and‡Department of Plastic and Reconstructive Surgery, Christchurch Hospital,University of Otago, Christchurch, New Zealand.
Presented at the 44th Congress of the European Society for Surgical Research, May23, 2009, Nimes, France, and at the Summer Meeting, British Association ofPlastic, Reconstructive and Aesthetic Surgeons, June 30, 2010, Sheffield, UK.
Conflicts of interest and sources of funding: none declared.Reprints: Charles M. Malata, FRCS (Plast), Department of Plastic and Recon-
structive Surgery, Box 186, Addenbrooke’s Hospital, Cambridge UniversityHospitals NHSFoundationTrust,HillsRd,CB22QQCambridge,UnitedKingdom.E-mail: [email protected]
Copyright * 2012 by Lippincott Williams & WilkinsISSN: 0148-7043/13/7101-0096DOI: 10.1097/SAP.0b013e3182414485
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
the United Kingdom (June 2001YJune 2009) and ChristchurchHospital in New Zealand (June 1997YJune 2009) were retrospectivelyreviewed. The raw data used in this study were collected from the
2 centers using the same proforma, resulting in 33 patients fromCambridge and 13 from Christchurch. The following data were col-lected from the clinical notes and the histology reports: patient’s age
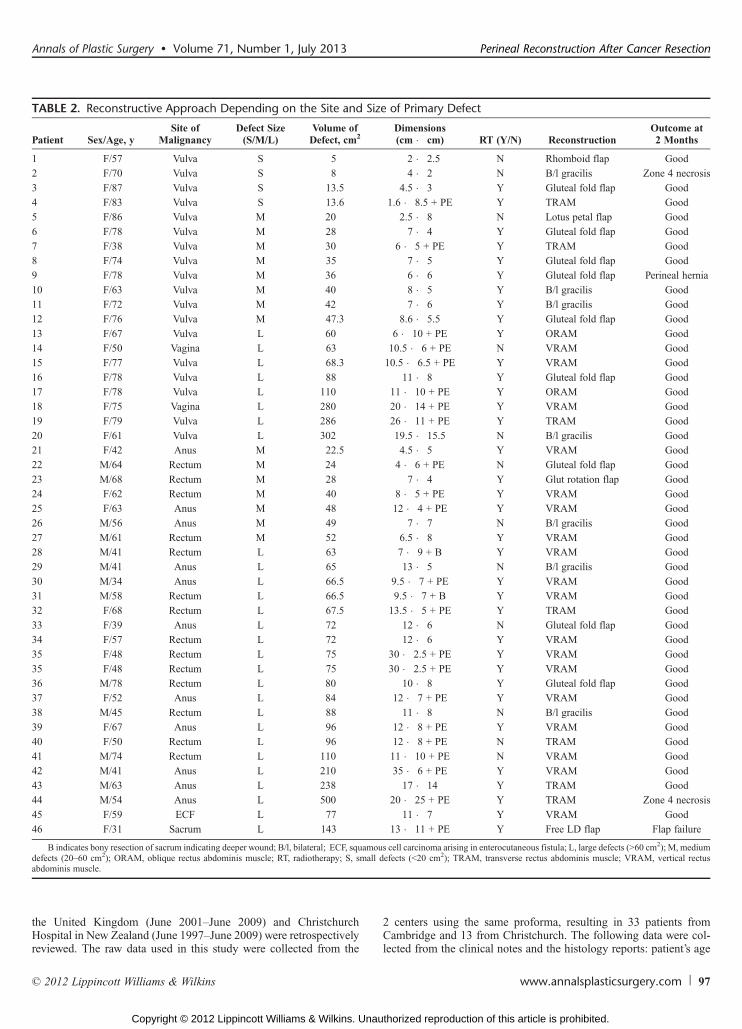
TABLE 2. Reconstructive Approach Depending on the Site and Size of Primary Defect
Patient Sex/Age, ySite of
MalignancyDefect Size(S/M/L)
Volume ofDefect, cm2
Dimensions(cm � cm) RT (Y/N) Reconstruction
Outcome at2 Months
1 F/57 Vulva S 5 2 � 2.5 N Rhomboid flap Good
2 F/70 Vulva S 8 4 � 2 N B/l gracilis Zone 4 necrosis
3 F/87 Vulva S 13.5 4.5 � 3 Y Gluteal fold flap Good
4 F/83 Vulva S 13.6 1.6 � 8.5 + PE Y TRAM Good
5 F/86 Vulva M 20 2.5 � 8 N Lotus petal flap Good
6 F/78 Vulva M 28 7 � 4 Y Gluteal fold flap Good
7 F/38 Vulva M 30 6 � 5 + PE Y TRAM Good
8 F/74 Vulva M 35 7 � 5 Y Gluteal fold flap Good
9 F/78 Vulva M 36 6 � 6 Y Gluteal fold flap Perineal hernia
10 F/63 Vulva M 40 8 � 5 Y B/l gracilis Good
11 F/72 Vulva M 42 7 � 6 Y B/l gracilis Good
12 F/76 Vulva M 47.3 8.6 � 5.5 Y Gluteal fold flap Good
13 F/67 Vulva L 60 6 � 10 + PE Y ORAM Good
14 F/50 Vagina L 63 10.5 � 6 + PE N VRAM Good
15 F/77 Vulva L 68.3 10.5 � 6.5 + PE Y VRAM Good
16 F/78 Vulva L 88 11 � 8 Y Gluteal fold flap Good
17 F/78 Vulva L 110 11 � 10 + PE Y ORAM Good
18 F/75 Vagina L 280 20 � 14 + PE Y VRAM Good
19 F/79 Vulva L 286 26 � 11 + PE Y TRAM Good
20 F/61 Vulva L 302 19.5 � 15.5 N B/l gracilis Good
21 F/42 Anus M 22.5 4.5 � 5 Y VRAM Good
22 M/64 Rectum M 24 4 � 6 + PE N Gluteal fold flap Good
23 M/68 Rectum M 28 7 � 4 Y Glut rotation flap Good
24 F/62 Rectum M 40 8 � 5 + PE Y VRAM Good
25 F/63 Anus M 48 12 � 4 + PE Y VRAM Good
26 M/56 Anus M 49 7 � 7 N B/l gracilis Good
27 M/61 Rectum M 52 6.5 � 8 Y VRAM Good
28 M/41 Rectum L 63 7 � 9 + B Y VRAM Good
29 M/41 Anus L 65 13 � 5 N B/l gracilis Good
30 M/34 Anus L 66.5 9.5 � 7 + PE Y VRAM Good
31 M/58 Rectum L 66.5 9.5 � 7 + B Y VRAM Good
32 F/68 Rectum L 67.5 13.5 � 5 + PE Y TRAM Good
33 F/39 Anus L 72 12 � 6 N Gluteal fold flap Good
34 F/57 Rectum L 72 12 � 6 Y VRAM Good
35 F/48 Rectum L 75 30 � 2.5 + PE Y VRAM Good
35 F/48 Rectum L 75 30 � 2.5 + PE Y VRAM Good
36 M/78 Rectum L 80 10 � 8 Y Gluteal fold flap Good
37 F/52 Anus L 84 12 � 7 + PE Y VRAM Good
38 M/45 Rectum L 88 11 � 8 N B/l gracilis Good
39 F/67 Anus L 96 12 � 8 + PE Y VRAM Good
40 F/50 Rectum L 96 12 � 8 + PE N TRAM Good
41 M/74 Rectum L 110 11 � 10 + PE N VRAM Good
42 M/41 Anus L 210 35 � 6 + PE Y VRAM Good
43 M/63 Anus L 238 17 � 14 Y TRAM Good
44 M/54 Anus L 500 20 � 25 + PE Y TRAM Zone 4 necrosis
45 F/59 ECF L 77 11 � 7 Y VRAM Good
46 F/31 Sacrum L 143 13 � 11 + PE Y Free LD flap Flap failure
B indicates bony resection of sacrum indicating deeper wound; B/l, bilateral; ECF, squamous cell carcinoma arising in enterocutaneous fistula; L, large defects (960 cm2); M, mediumdefects (20Y60 cm2); ORAM, oblique rectus abdominis muscle; RT, radiotherapy; S, small defects (G20 cm2); TRAM, transverse rectus abdominis muscle; VRAM, vertical rectusabdominis muscle.
Annals of Plastic Surgery & Volume 71, Number 1, July 2013 Perineal Reconstruction After Cancer Resection
* 2012 Lippincott Williams & Wilkins www.annalsplasticsurgery.com 97
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
and sex, site and type of tumor, tumor size and stage, the ablativesurgical procedure performed (vulvectomy, proctectomy, abdomi-noperineal resection (APR), pelvic exenteration (PE), sacrectomy,coccygectomy, and concomitant groin dissection), the reconstruc-tive procedure and its timing, and the surgical teams involved(colorectal, gyneoncology, urologists, and plastic surgeons). Thehospital stay, plastic surgical outcomes (primary healing, woundbreakdown, subsequent surgical procedures or operations, and othertreatment such as vacuum-assisted therapy), and oncology outcomes(recurrence, survival, and follow-up) were recorded. Patientswere followed up in the plastic surgical clinic for wound related/healing problems and thereafter by the primary surgical teams and
oncologists in the colorectal or gyne-oncological clinics. The me-dian follow-up was 12 months (range, 3Y48 months). Functionalrehabilitation for mobility, return to work, driving, and resumptionof intercourse (where relevant) was noted.
RESULTS
Demographic Data and Tumor CharacteristicsDuring the study period, 46 patients were treated in the
2 centers, comprising 33 in the United Kingdom and 13 in NewZealand. The mean patient age was 62.5 years (range, 31Y87) and themale to female ratio was 1:2.5. Table 1 summarizes patient demo-graphics and tumor characteristics. The most common malignancyrequiring immediate perineal reconstruction in our study wassquamous cell carcinoma of the anorectal region, followed by tumorsof the vulva and vagina. Of the 46 patients, 34 (975%) had undergonepreoperative radiotherapy (RT) as part of neoadjuvant treatment toreduce the tumor load, 27 (58%) had also received preoperative che-motherapy, and 25 (54%) underwent surgery for recurrent tumors. Thedefect size ranged from 5 to 500 cm2.
Reconstructive TechniquesTable 2 outlines the different reconstructive techniques used
according to the site and size of perineal defects after primary excision.The choice of reconstructive technique generally conformed to astandard pattern. After a simple wide local excision of a vulval ma-lignancy, the reconstruction of choice was the local flap. Withan increase in the volume of tissue resected, the next choice wasbilateral V-Y medial thigh advancement flaps with or without incor-poration of the gracilis muscle. When operating on patients who hadbeen previously irradiated there was a need to resect greater amountsof tissue to reach a well-vascularized bed outside the radiation field(patient 4, Table 2). Hence, a greater volume of tissue was required
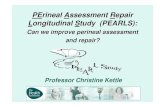
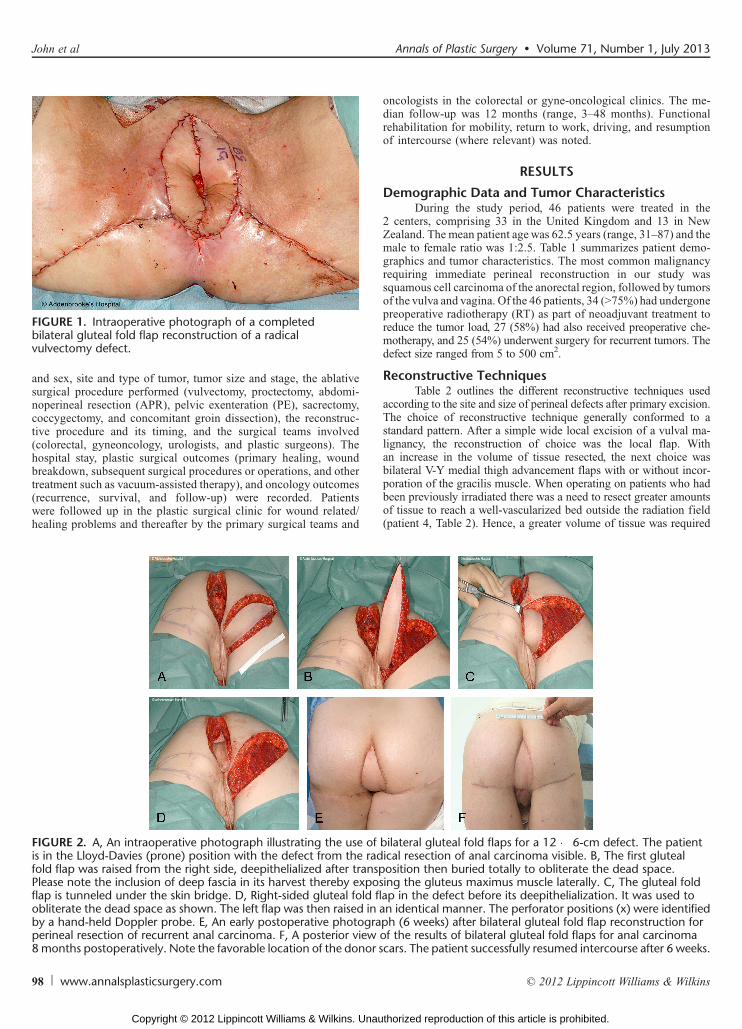
FIGURE 2. A, An intraoperative photograph illustrating the use of bilateral gluteal fold flaps for a 12 � 6-cm defect. The patientis in the Lloyd-Davies (prone) position with the defect from the radical resection of anal carcinoma visible. B, The first glutealfold flap was raised from the right side, deepithelialized after transposition then buried totally to obliterate the dead space.Please note the inclusion of deep fascia in its harvest thereby exposing the gluteus maximus muscle laterally. C, The gluteal foldflap is tunneled under the skin bridge. D, Right-sided gluteal fold flap in the defect before its deepithelialization. It was used toobliterate the dead space as shown. The left flap was then raised in an identical manner. The perforator positions (x) were identifiedby a hand-held Doppler probe. E, An early postoperative photograph (6 weeks) after bilateral gluteal fold flap reconstruction forperineal resection of recurrent anal carcinoma. F, A posterior view of the results of bilateral gluteal fold flaps for anal carcinoma8months postoperatively. Note the favorable location of the donor scars. The patient successfully resumed intercourse after 6 weeks.
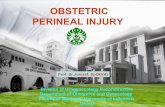
FIGURE 1. Intraoperative photograph of a completedbilateral gluteal fold flap reconstruction of a radicalvulvectomy defect.
98 www.annalsplasticsurgery.com * 2012 Lippincott Williams & Wilkins
John et al Annals of Plastic Surgery & Volume 71, Number 1, July 2013
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
to obliterate the dead space, at which point many surgeons pre-ferred bilateral gluteal fold flaps as it gave an aesthetically appeal-ing appearance of the neovulva and the donor site was cosmeticallyacceptable (Fig. 1). In cases where wide local excision of the malig-nancy was associated with PE and hence had a greater amount ofpelvic dead space which required filling, the rectus abdominis myo-cutaneous (RAM) flaps were the most popular, even when initialvolumes of cancer resected were small (patient 3, Table 2).
Similarly, considering malignancies arising from rectum andanal canal, the smaller resections were reconstructed with bilateralgracilis flaps associated with V-Y advancement of skin (patients 26and 29, Table 2), whereas larger areas required gluteal fold flaps(patients 33 and 36, Table 2) (Figs. 2AYF). Although 1 large volumedefect (88 cm2) without PE was successfully closed using bilateralgracilis flaps (patient 38, Table 2), the most common method ofreconstruction after APR used pedicled rectus abdominis flaps(Figs. 3AYE). This was especially true for those patients with largevolume defects (960 cm2), those who underwent PE, and those withresection of bony sacrum suggesting larger volumes of dead space.Other methods such as superior gluteal artery perforator rotationflaps, although used occasionally, were noted to be associated withgreater incidence of complications such as wound dehiscence, whichrequired multiple trips back to theater for debridement and closure(patient 23, Table 2). This may have been related to the postoperativenursing position or proximity to the field of radiation. A free latis-simus dorsi flap was used to reconstruct a defect after a sacrectomyperformed for resection of a sacral chondroma and perineal ulcer(patient 46, Table 2). However, this failed because of anastomotic
venous thrombosis, and the patient subsequently died of respiratoryand cardiac complications while awaiting further definitive surgery.
Plastic Surgical OutcomesOverall flap success rate was 97.8%, with the 1 free flap used
being the only case that failed. Wound dehiscence was the mostcommon problem affecting more than a third of the patients (37%,17 patients) of whom 13 (28%) required some form of surgicalrevision (Table 3). Distal necrosis of the flap requiring debridementoccurred in 2 patients who had reconstruction using vertical rec-tus abdominis muscle flaps. Of the patients who had wound dehis-cence, all of them had previously undergone radiation and 70% ofthem, chemotherapy.
Oncology OutcomesAlthough immediate reconstruction after primary surgery was
performed with curative intent, 18 (39%) patients have since diedeither because of distant metastases (8 patients) or unrelated causes
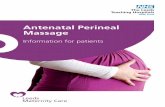
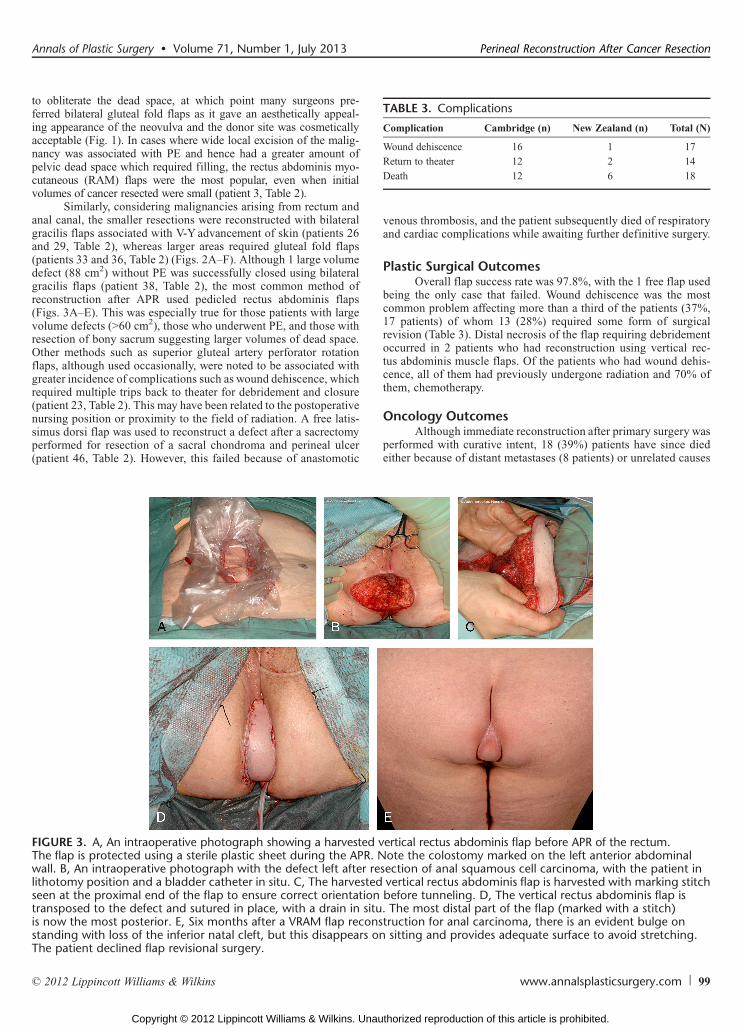
FIGURE 3. A, An intraoperative photograph showing a harvested vertical rectus abdominis flap before APR of the rectum.The flap is protected using a sterile plastic sheet during the APR. Note the colostomy marked on the left anterior abdominalwall. B, An intraoperative photograph with the defect left after resection of anal squamous cell carcinoma, with the patient inlithotomy position and a bladder catheter in situ. C, The harvested vertical rectus abdominis flap is harvested with marking stitchseen at the proximal end of the flap to ensure correct orientation before tunneling. D, The vertical rectus abdominis flap istransposed to the defect and sutured in place, with a drain in situ. The most distal part of the flap (marked with a stitch)is now the most posterior. E, Six months after a VRAM flap reconstruction for anal carcinoma, there is an evident bulge onstanding with loss of the inferior natal cleft, but this disappears on sitting and provides adequate surface to avoid stretching.The patient declined flap revisional surgery.
TABLE 3. Complications
Complication Cambridge (n) New Zealand (n) Total (N)
Wound dehiscence 16 1 17
Return to theater 12 2 14
Death 12 6 18
Annals of Plastic Surgery & Volume 71, Number 1, July 2013 Perineal Reconstruction After Cancer Resection
* 2012 Lippincott Williams & Wilkins www.annalsplasticsurgery.com 99
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
such as respiratory infections, cardiac failure, or myocardial infarc-tion (after the 6-month period after surgery).
DISCUSSIONDespite advances in neoadjuvant therapy for perineal malig-
nancies, surgical resection of the tumor remains the treatment ofchoice. Adverse conditions such as locally advanced disease (oftenrecurrent), prior surgery, and the presence of irradiated tissue oftencombine to make surgical management a challenging problem. Thesurgeon is faced with a large defect within inelastic tissue whereprimary closure cannot be performed. Historically, the wounds wereleft to heal by secondary intention, a slow process requiring multiple(often painful) dressing changes during a period of 3 to 12 months.Studies have shown that using a flap after primary resection decreasesthe incidence of complications for patients subsequently undergoingpostoperative RT.4
Over the years, many techniques of reconstruction of the peri-neum have been developed with the goals of reducing morbidity bylimiting the volume of tissue resected, providing aesthetically appeal-ing tissue cover, as well as restoring function. Methods have evolvedfrom split skin grafting to various flaps like gracilis (myocutaneous),gluteal fold (fasciocutaneous), andmost commonly now, RAM flaps.5Y8
Each procedure is associated with its own unique set of complicationsand the surgeon has to be versatile in tailoring the technique used tothe patient’s need. This paper aims to recommend a basic guideline oftime-tested techniques used for perineal reconstructions, based on thesite of malignancy and the size of primary defect.
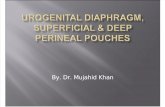
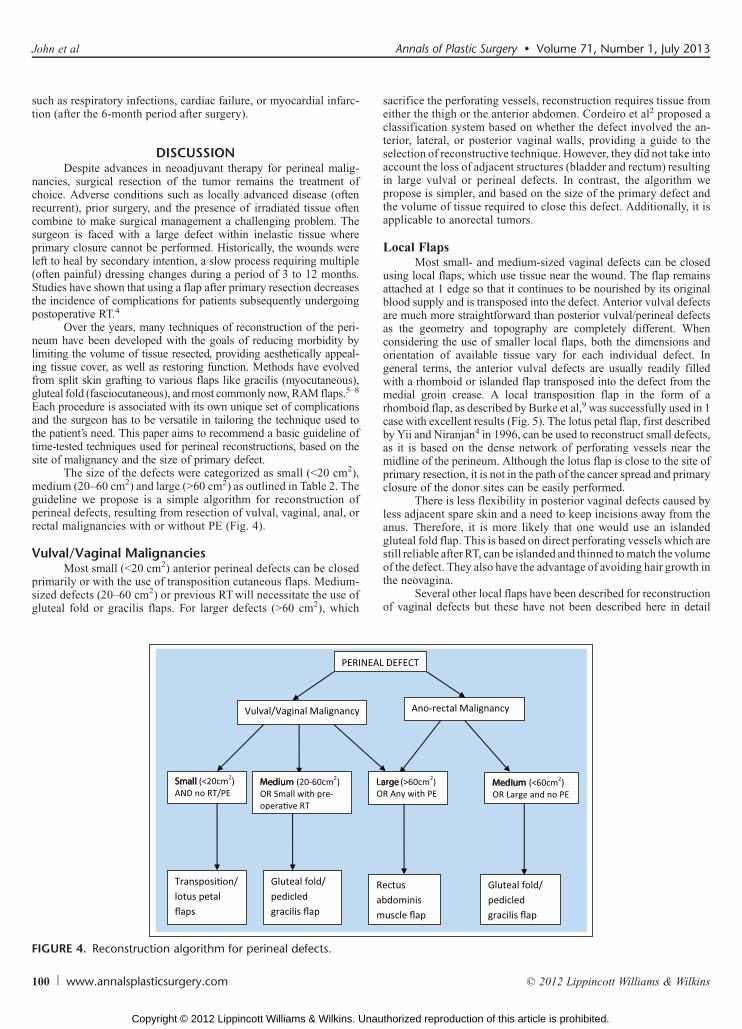
The size of the defects were categorized as small (G20 cm2),medium (20Y60 cm2) and large (960 cm2) as outlined in Table 2. Theguideline we propose is a simple algorithm for reconstruction ofperineal defects, resulting from resection of vulval, vaginal, anal, orrectal malignancies with or without PE (Fig. 4).
Vulval/Vaginal MalignanciesMost small (G20 cm2) anterior perineal defects can be closed
primarily or with the use of transposition cutaneous flaps. Medium-sized defects (20Y60 cm2) or previous RTwill necessitate the use ofgluteal fold or gracilis flaps. For larger defects (960 cm2), which
sacrifice the perforating vessels, reconstruction requires tissue fromeither the thigh or the anterior abdomen. Cordeiro et al2 proposed aclassification system based on whether the defect involved the an-terior, lateral, or posterior vaginal walls, providing a guide to theselection of reconstructive technique. However, they did not take intoaccount the loss of adjacent structures (bladder and rectum) resultingin large vulval or perineal defects. In contrast, the algorithm wepropose is simpler, and based on the size of the primary defect andthe volume of tissue required to close this defect. Additionally, it isapplicable to anorectal tumors.
Local FlapsMost small- and medium-sized vaginal defects can be closed
using local flaps, which use tissue near the wound. The flap remainsattached at 1 edge so that it continues to be nourished by its originalblood supply and is transposed into the defect. Anterior vulval defectsare much more straightforward than posterior vulval/perineal defectsas the geometry and topography are completely different. Whenconsidering the use of smaller local flaps, both the dimensions andorientation of available tissue vary for each individual defect. Ingeneral terms, the anterior vulval defects are usually readily filledwith a rhomboid or islanded flap transposed into the defect from themedial groin crease. A local transposition flap in the form of arhomboid flap, as described by Burke et al,9 was successfully used in 1case with excellent results (Fig. 5). The lotus petal flap, first describedby Yii and Niranjan4 in 1996, can be used to reconstruct small defects,as it is based on the dense network of perforating vessels near themidline of the perineum. Although the lotus flap is close to the site ofprimary resection, it is not in the path of the cancer spread and primaryclosure of the donor sites can be easily performed.
There is less flexibility in posterior vaginal defects caused byless adjacent spare skin and a need to keep incisions away from theanus. Therefore, it is more likely that one would use an islandedgluteal fold flap. This is based on direct perforating vessels which arestill reliable after RT, can be islanded and thinned tomatch the volumeof the defect. They also have the advantage of avoiding hair growth inthe neovagina.
Several other local flaps have been described for reconstructionof vaginal defects but these have not been described here in detail
FIGURE 4. Reconstruction algorithm for perineal defects.
100 www.annalsplasticsurgery.com * 2012 Lippincott Williams & Wilkins
John et al Annals of Plastic Surgery & Volume 71, Number 1, July 2013
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
simply because we have not used them in our practice. These includethe perineal artery axial flap (for small defects),10 fasciocutaneouspudendal thigh flap, also known as the Singapore flap (for small-and medium-sized defects),11,12 and the anterolateral thigh flaps(for medium to large defects). The anterolateral thigh flap may bereliably pedicled into perineal defects, does not require an intrao-perative change of patient’s position,13 and has been successfullyused for reconstruction after PE with good effect and low donor-sitemorbidity.14,15 With further experience, these can be slotted into theperineal reconstruction algorithm based on the volume of tissue theyprovide to close defects.
Pedicled Gracilis FlapBilateral gracilis flaps can provide cover for large defects and
are such as those resulting from total circumferential vaginectomies,first described byMcCraw et al7 in 1975. In our experience, where thedefect was complex, bilateral flaps were harvested. The flaps can alsobe tubularized to form a neovagina and then anchored either to theperiosteum of the sacrum or pubis to prevent prolapse. The advantageof gracilis muscle flaps is the wide arc of rotation and proximity tothe introitus. The gracilis V-Y advancement provides tissue over abroad front especially useful for anterior perineal reconstruction, asillustrated in Figure 6.
RAM FlapsFor defects resulting from PE where there was substantial dead
space that required filling, the rectus abdominis flap was the recon-struction of choice. This was harvested as a transverse or vertical flapor in 2 cases obliquely oriented flaps with an ellipse of skin, as de-scribed by Taylor et al.16 For circumferential vaginal defects, the skinisland was folded and tubularized to form the neovagina. Advantagesof the RAM flap include the reliability or robustness of the deepinferior epigastric vascular pedicle (even after pelvic RT), and therelative ease bywhich it can be harvestedwithout position change. Theflap is bulky and hence suitable to fill dead space and there is minimaldonor-site morbidity.
Anorectal MalignanciesResection of all the anorectal malignancies in our study resulted
in defects greater than 20 cm2 in volume. Those of smaller volumewere classed under medium-sized defects as their management is thesame and except for gluteal fold flaps, other local flaps have not beenconsidered for defects from anorectal malignancies because the pri-mary resection is in the form of APR resulting in a deeper wound anddead space that requires filling. Medium-sized defects (G60 cm2) orlarge defects, without PE necessitated the use of gluteal fold orpedicled gracilis flaps. These flaps are also suitable for patients whoundergo the primary resection laparoscopically. The rectus abdominisflap is, however, ideal for defects with large amount of dead space afterresection of anorectal malignancies and PE (Fig. 4).
Gluteal Fold FlapsAfter APR, a popular option for reconstruction of the perineum
is harvesting a gluteal fold flap.8 The gluteal fold flap, although a localflap, combines the advantages of a distant flap (such as reliability afterpelvic or perineal RT) with those of being locally available andamenable to harvest without moving the patient from the lithotomyposition. It has a long reach and 2 are available for bulk (Figs. 2AYF),or if one is damaged during tumor resection or flap harvest. Althoughnot included in our algorithm for reconstruction of perineal defectswith PE, bilateral gluteal fold flaps did provide enough tissue volumefor 1 such case (patient 22, Table 2) and can be considered if patientanatomy allows. When bilateral gluteal fold flaps are harvested, thenatal cleft can be recreated for a more natural look and the scar is wellhidden.17 However, the disadvantage of a gluteal fold flap is thediscomfort patients experience on sitting down in the initial period.Our experience recommends that they do not sit for more than a fewminutes for the first 3 weeks.
RAM FlapThe most popular choice of reconstructive surgery after an
APRwith or without PE is the rectus abdominis flap. The right rectus
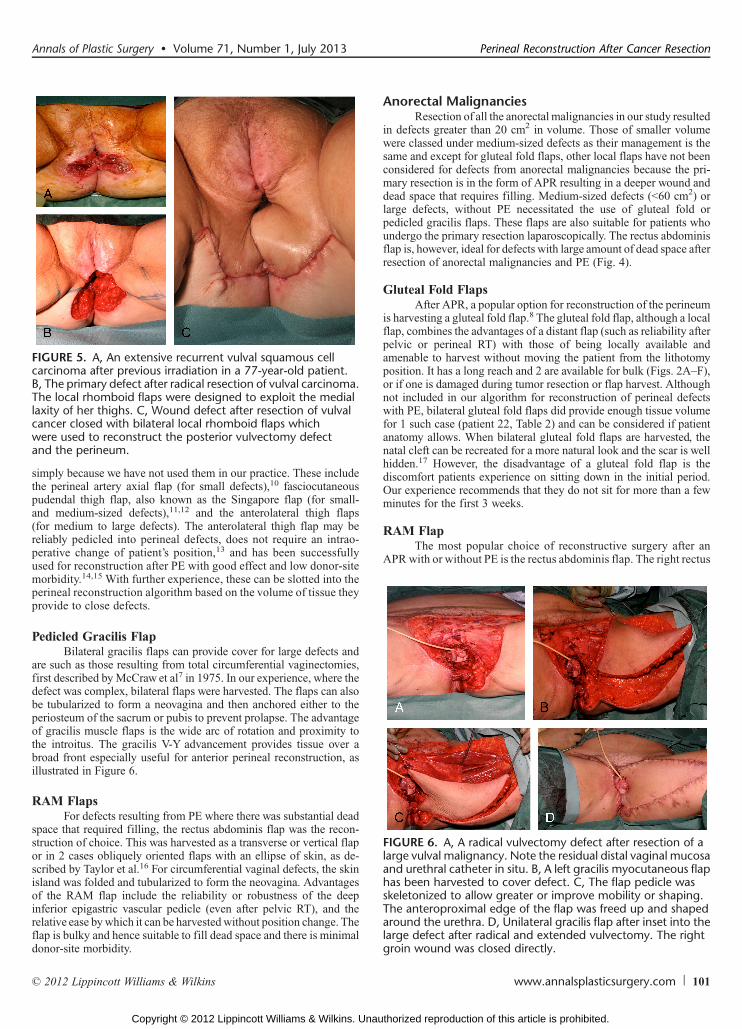
FIGURE 5. A, An extensive recurrent vulval squamous cellcarcinoma after previous irradiation in a 77-year-old patient.B, The primary defect after radical resection of vulval carcinoma.The local rhomboid flaps were designed to exploit the mediallaxity of her thighs. C, Wound defect after resection of vulvalcancer closed with bilateral local rhomboid flaps whichwere used to reconstruct the posterior vulvectomy defectand the perineum.
FIGURE 6. A, A radical vulvectomy defect after resection of alarge vulval malignancy. Note the residual distal vaginal mucosaand urethral catheter in situ. B, A left gracilis myocutaneous flaphas been harvested to cover defect. C, The flap pedicle wasskeletonized to allow greater or improve mobility or shaping.The anteroproximal edge of the flap was freed up and shapedaround the urethra. D, Unilateral gracilis flap after inset into thelarge defect after radical and extended vulvectomy. The rightgroin wound was closed directly.
Annals of Plastic Surgery & Volume 71, Number 1, July 2013 Perineal Reconstruction After Cancer Resection
* 2012 Lippincott Williams & Wilkins www.annalsplasticsurgery.com 101
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
muscle is preferentially chosen as the colostomy is usually sitedthrough the left rectus (Fig. 7). Nelson and Butler18 compared133 patients who underwent PE surgery after APR and found thatrectus abdominis flaps were associated with a significant decrease incomplications as compared with various thigh flaps.
CONCLUSIONSResection of malignancies involving structures in the peri-
neum often requires a multidisciplinary team approach, not only in theoperating theater but also starting with preoperative planning with thepatient. Staging investigations are necessary to establish whethersurgery will be curative or just debulking. Preoperative chemotherapyand particularly RT may successfully decrease tumor load but RTin particular, significantly affects the wound bed and therefore choiceof flap.19 It is pertinent to excise all the irradiated areas back to healthytissue to enable wound healing once the flap is in place. Because eachpatient has different complicating factors, the reconstructive sur-geon needs to be versatile and tailor each procedure according to thepatient’s needs. However, in areas such as the perineum, which is
known for its higher-than-average complication rates and whereseveral different techniques have been proposed by surgeons all overthe world, it is useful to have a simplified logical process for decisionmaking. This study has not focused on assimilating all the availablemethods of perineal reconstruction, rather it is an analysis of a 2 centerexperience in this field and a proposal for a simplified algorithm toprovide a framework for surgeons involved in this process.
REFERENCES1. Corney RH, Crowther ME, Everett H et al. Psychosexual dysfunction in wo-
men with gynaecological cancer following radical pelvic surgery. Br J ObstetGynaecol. 1993;100:73Y78.
2. Cordeiro PG, Pusic AL, Disa JJ. A classification system and reconstructivealgorithm for acquired vaginal defects. Plast Reconstr Surg. 2002;110:1058Y1065.
3. Salgarello M, Farallo E, Barone-Adesi L, et al. Flap algorithm in vulvar re-construction after radical, extensive vulvectomy. Ann Plast Surg. 2005;54:184Y190.
4. Yii NW, Niranjan NS. Lotus petal flaps in vulvo-vaginal reconstruction. Br JPlast Surg. 1996;49:547Y554.
5. Sadove RC, Horton CE. Utilizing full-thickness skin grafts for vaginal re-construction. Clin Plast Surg. 1988;15:443Y448.
6. Woods JE, Alter G, Meland B, et al. Experience with vaginal reconstructionutilizing the modified Singapore flap. Plast Reconstr Surg. 1992;90:270Y274.
7. McCraw JB, Massey FM, Shanklin KD, et al. Vaginal reconstruction withgracilis myocutaneous flaps. Plast Reconstr Surg. 1975;58:76Y83.
8. Hashimoto I, Nakanishi H, Nagae H, et al. Gluteal-fold flap for vulvar andbuttock reconstruction: anatomic study and adjustment of flap volume. PlastReconstr Surg. 2001;108:1998Y2005.
9. Burke TW, Morris M, Levenback C, et al. Closure of complex vulvar defectsusing local rhomboid flaps. Obstet Gynecol. 1994;84:1043Y1047.
10. Hagerty RC, Vaughn TR, Lutz MH. The perineal artery axial flap in recon-struction of the vagina. Plast Reconstr Surg. 1988;82:344Y345.
11. Wee JT, Joseph VT. A new technique of vaginal reconstruction using neuro-vascular pudendal-thigh flaps: a preliminary report. Plast Reconstr Surg.1989;83:701Y709.
12. Monstrey S, Blondeel P, Van Landuyt K, et al. The versatility of the puden-dal thigh fasciocutaneous flap used as an island flap. Plast Reconstr Surg.2001;107:719Y725.
13. Wang X, Qiao Q, Burd A, et al. Perineum reconstruction with pedicled ante-rolateral thigh fasciocutaneous flap. Ann Plast Surg. 2006;56:151Y155.
14. Wong S, Garvey P, Skibber J, et al. Reconstruction of pelvic exenteration defectswith anterolateral thigh-vastus lateralis muscle flaps. Plast Reconstr Surg.2009;124:1177Y1185.
15. Kuo YR, Yeh MC, Shih HS, et al. Versatility of the anterolateral thigh flap withvascularized fascia lata for reconstruction of complex soft-tissue defects:clinical experience and functional assessment of the donor site. Plast ReconstrSurg. 2009;124:171Y180.
16. Taylor GI, Corlett R, Boyd JB. The extended deep inferior epigastric flap: aclinical technique. Plast Reconstr Surg. 1983;72:751Y765.
17. Ragoowansi R, Yii N, Niranjan N. Immediate vulvar and vaginal reconstructionusing the gluteal-fold flap: long-term results.Br J Plast Surg. 2004;57:406Y410.
18. Nelson RA, Butler CE. Surgical outcomes of VRAM versus thigh flaps forimmediate reconstruction of pelvic and perineal cancer resection defects. PlastReconstr Surg. 2009;123:175Y183.
19. Chessin DB, Hartley J, Cohen AM, et al. Rectus flap reconstruction decreasesperinealwound complications after pelvic chemoradiation and surgery: a cohortstudy. Ann Surg Oncol. 2005;12:104Y110.
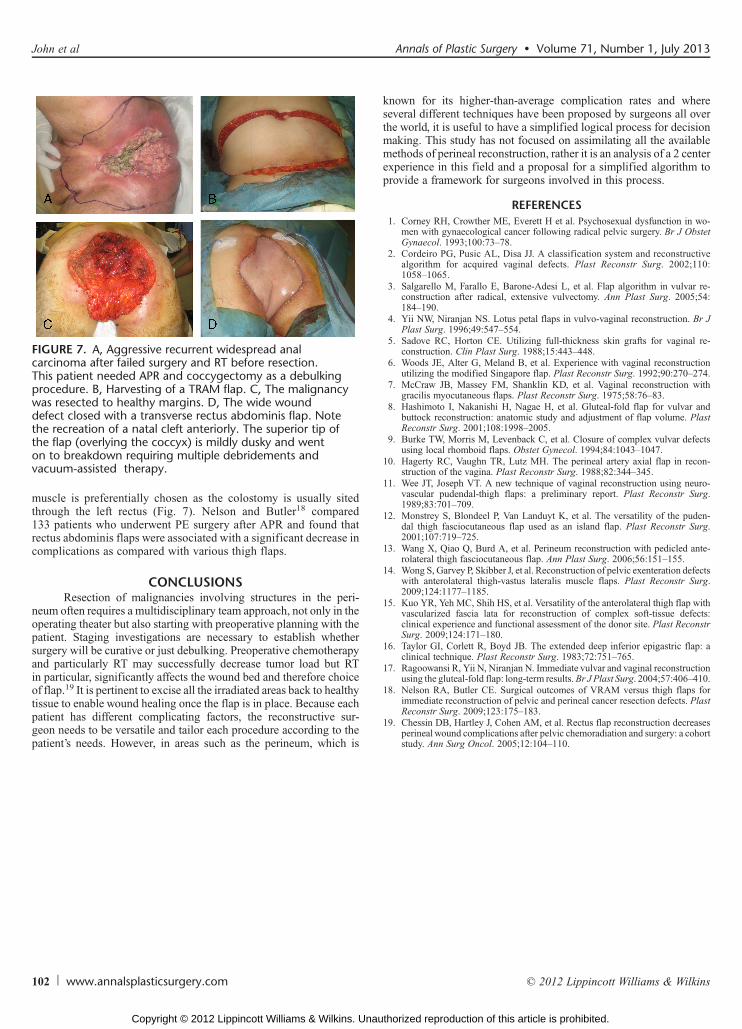
FIGURE 7. A, Aggressive recurrent widespread analcarcinoma after failed surgery and RT before resection.This patient needed APR and coccygectomy as a debulkingprocedure. B, Harvesting of a TRAM flap. C, The malignancywas resected to healthy margins. D, The wide wounddefect closed with a transverse rectus abdominis flap. Notethe recreation of a natal cleft anteriorly. The superior tip ofthe flap (overlying the coccyx) is mildly dusky and wenton to breakdown requiring multiple debridements andvacuum-assisted therapy.
102 www.annalsplasticsurgery.com * 2012 Lippincott Williams & Wilkins
John et al Annals of Plastic Surgery & Volume 71, Number 1, July 2013
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.