AMS AND SURGICAL PROPHYLAXIS
31
AMS AND SURGICAL PROPHYLAXIS Dr Mushira Enani
Transcript of AMS AND SURGICAL PROPHYLAXIS

AMS AND SURGICAL PROPHYLAXIS
Dr Mushira Enani

Improving Surgical Antibiotic Prophylaxis: Using the PDSA
Model Mushira Enani, MbChB, FRCPE, FACP, FIDSA
Assistant Professor of MedicineConsultant, Infectious Diseases
King Fahad Medical City, Riyadh, Saudi Arabia


Outline
Background
Quality Improvement ModelKFMC experience applying the PDSA model to improve SAP

Background
Surgical site infections (SSIs) are a major contributor to patient injury, mortality, and health care costs.
The goal of SAP is to prevent SSI by reducing the burden of bacteria at the surgical site throughout the operative procedure.
Despite evidence of effectiveness of antimicrobials to prevent SSIs, studies have demonstrated errors in selection, timing, dosing, and duration of surgical antimicrobial prophylaxis (SAP).



Key Performance Indicators (KPI)
Choice: First generation cephalosporins
Dose: should be administered in doses sufficient to achieve adequate serum and tissue drug levels from skin incision to closure.
- Cefazolin 2 grams for non-obese
- Cefazolin 3 grams for obese patientsRe-dosing: repeat intraoperative dosing is warranted for procedures that exceed two half-lives of the drug and for procedures in which there is excessive blood loss (>1500 mL), and extensive burns*Redosing of SAP following closure of the surgical incision is not warrantedfor patients undergoing clean and clean-contaminated procedures, even in the presence of a drains.

Medicine. 96(29):e6903, JULY 2017


JAMA Surg. 2019; 154 (7): 590
Duration: SAP should be stopped Within 24 hours.
In a study of more than 79,000 patients, length of antibiotic
prophylaxis was independently associated with increasing odds of both AKI and CDI infection. This risk increased with each additional day of antibiotics.

o 74 years old lady with DM/ HTN who was admitted on Dec 28th 2009. Jan 9th, She
underwent emergency CABG with MVR/ TVR @2 AM, she was out from OR @ 10:56
AM. Bypass time was 177 min.
o Jan 25th, she developed deep sternal SSI/ mediastinitis requiring vac machine.
o Jan 27th: Re-operated for wound debridement, sternal wires were removed, 3 pockets of
pus were found, debridement was done, wound closure with tension sutures and
mediastinal drain, pleura drain and hemovac drains left in place.
Case Scenario

First Do No Harm
Real patient!


Plan-Do-Check-Act (PDSA Cycle)
• Quality improvement model aimed at making positive changes in health care processes to achieving favorable outcomes.
• This is a method that has been widely used by the Institute for Healthcare Improvement for rapid cycle improvement.
• One of the unique features of this model is the cyclical nature of impacting and assessing change, accomplished through small and frequent PDSAs rather than big and slow ones.

(1) What is the goal of the project?
(2) How will it be known whether the goal was reached?
(3) What will be done to reach the goal?



KFMC Experience, 2016 - 2018
In 2016, SAP was chosen as a quality improvement project when it was identified that lack of awareness on best practices and variation in process of antimicrobial prophylaxis was administered in surgery was major factors for poor compliance. Timing and duration of prophylactic antibiotic were major gaps. The project continued until 2017, where it has shown that improving communication between surgeons, anesthesia, and nursing staff resulted in a outstanding improvement in compliance with proper timing and duration of SAP.Therefore, as part of the sustainability plan, we decided to continue the project in 2018 to persistently improve compliance on SAP wherein new indicators are included such as the compliance to the preset order sheet and the reduction of Surgical Site Infection (SSI) rate post Coronary Artery Bypass Grafting (CABG).

FOCUS-PDCA
F: Find an opportunity
O: organize a team
C: Clarify the process
U: Understand the reasons of variation (root-cause analysis)
S: Strategy for change

Organize a team
Project Team Leader: Dr.
Mushira Enani, Consultant, Infectious Diseases,
Medical Dept.
Project Coordinator: Ms.
Fe Faustino, Quality Nurse, Main Hospital
Consultant, Clinical Audit Department
Clinical Audit Reviewer, Clinical
Audit Department
Nursing Director of OR
Department
Quality Nurse, QMD
Clinical Pharmacy
Department
Director & The
Chairperson of IPC
Medical Secretary, MH
Members
Chairperson, Clinical Audit

Clarify the process

Understand the problem

S: Strategy for change
Select the desired OutcomesTo improve compliance to the following KPIs by 2nd quarter of 2018:
- Selection of SAP as per guidelines: 95%- Timing of SAP within 60 min of surgical incision: 100%- Stopping SAP within 24 hours of surgery end time: 80%- Reduce SSI post CABG by 10%
Establish a baseline compliance to the use of Preset Order Sheet

Plan
Task Responsible person
Role Timeline
Baseline dataQuarterly monitoringData analysisEducation/ awareness

Do
1. Baseline Data was collected and compared to 2018.2. Quarterly monitoring of compliance of :
- Selection of SAP as per guidelines- Timing of SAP within 60 min of surgical incision- Stopping SAP within 24 hours of surgery end time
3. Monitoring of SSI incidence post CABG4. Monitoring compliance on using the Preset Order Sheet5. Staff Policy awareness on the Prevention of SSI6. Conduct regular multidisciplinary meetings

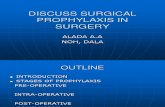
Check

8995
68
9994
81
0
20
40
60
80
100
120
Selection Timing 60 m Stop
SAP KPI
2017 2018

Sustainability plan
Strict compliance on the use of SAP preset order sheet. Continuous education and awareness campaign to staff. Spread improvement across KFMC and monitor SSI rate. Continuous audit and feedback of the results of the SAP data to
surgeons and other concerned departments can help improve performance.

Conclusion
• Effective communication, continuous education and awareness
among surgeons, nurses, anesthesia staff, infection control, and
clinical auditors resulted in behavioral change toward best
practices in process measures related to SSI prevention.

Thank you